
Abstract
The Coronavirus Disease 2019 (COVID-19) pandemic has resulted in significant morbidity and mortality worldwide. Although initial reports concentrated on severe respiratory illness, emerging literature has indicated a substantially elevated risk of thromboembolic events in patients with COVID-19 disease. Pro-inflammatory cytokine release has been linked to endothelial dysfunction and activation of coagulation pathways, as evident by elevated D-dimer levels and deranged coagulation parameters. Both macrovascular and microvascular thromboses have been described in observational cohort and post-mortem studies. Concurrently, preliminary data have suggested the role of therapeutic anticoagulation in preventing major thromboembolic complications in moderately but not critically ill patients. However, pending results from randomized controlled trials, clear guidance is lacking regarding the intensity and duration of anticoagulation in such patients. Herein, we review the existing evidence on incidence and pathophysiology of COVID-19 related thromboembolic complications and guide anticoagulation therapy based on current literature and societal consensus statements.
Keywords
Introduction
Since the end of 2019, the spread of a novel coronavirus SARS-CoV2 has been reported, first in the Chinese mainland, followed by several European countries, and since early March 2020 in the USA. Shortly after, the World health organization (WHO) declared the fast spread of SARS-CoV2 infection as a pandemic. 1 Despite the high likelihood of a mild or asymptomatic clinical course, SARS-CoV2 infection called “COVID-19” can be associated with more severe manifestations such as severe pneumonia, acute respiratory distress syndrome (ARDS), hepatic, cardiac, and renal injury.2–4 Fortunately, vaccinations for SARS-CoV2 are underway throughout most of the world. Unfortunately, slow public participation and emerging variants with increased transmissibility such as the “Delta Variant” keep this serious disease at the forefront of worldwide attention, thus, necessitating focus on understanding the full pathophysiology of its disease process. 5
COVID-19 has a known correlation with the disruption of the coagulation cascade consequently resulting in cases of pulmonary microthrombi, arterial and/or venous thrombotic related events. 6 These events can result in the aggravation of one's hospital course leading to prolonged inpatient hospitalizations, exaggerated stays in intensive care units (ICU) or even death. Concerningly, these factors may result in exhaustion or even a collapse of health care systems. A high proportion of COVID-19 patients, especially if treated in ICUs, suffer from thrombotic or thromboembolic complications in addition to more traditional associated illnesses such as pneumonia.7–14 Initial reports hypothesized a disseminated intravascular like coagulopathy (DIC) in patients with severe COVID-19 infection.10,15 Those studies displayed consistently elevated D-dimer and fibrin degradation products (FDP). Prolongation of prothrombin time (PT) activated partial thromboplastin time (aPTT), and thrombocytopenia were also noted.15–17
Although more recent studies have indicated the coagulopathy associated with COVID-19 infection is distinct from classic DIC,10,18 other studies, have not shown ample difference between COVID-19 and other pathogens inducing DIC.9,14,19,20 Recent publications for a pro-coagulant mechanism include the proof of a generalized coagulopathy21,22 which may include variables such as increased Factor V, 23 lupus anticoagulant, 24 or reduction of the von Willebrand factor inhibitor ADAMST13. 25 Elevation of these markers is associated with amplification of thrombin generation and thereby thrombus formation (Figure 1).26–29 Furthermore, increased levels of plasminogen activator inhibitor type 1 (PAI-1), as well as tissue type plasminogen activator (t-PA) were also found to be elevated in severe COVID-19 infection adding traction to the theory of an overall disrupted coagulation cascade similarly seen in DIC.28,30,31

Graphical illustration of SARS-CoV 2 entry into human cells and development of thrombosis on the basis of the Virchow triad. CRP: C-reactive protein; EC: endothelial cell; FVIII: Factor VIII; IL-6 and IL-1B: Interleukin 6 and 1B; PAI-1: plasminogen activator inhibitor type 1; SARS-CoV 2: Coronavirus 19; t-PA: tissue type plasminogen activator; TNF-alpha: tumor necrosis factor alpha; vWF: von Willenbrand factor; u-PA: urikinase type plasminogen activator.
Epidemiology of Thrombosis in COVID-19
Venous Thromboses and Emboli:
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and/or pulmonary embolism (PE), frequently occur in patients with severe COVID-19 infection and as with most venous thrombotic events, is related to Virchow's triad of immobility, endothelial infection, and immune dysfunction resulting in hypercoagulability (Figure 1)3,32,33 Initial reports show an incidence of VTE between 20 to 43% mainly in the form of PE (Table 1). Among 184 consecutively investigated severe COVID-19 patients, VTE's cumulative incidence was 27%, again mostly from PE. 10 In another report of 150 patients with severe COVID-19 infection, VTE occurred in 43% of patients. Also reported was a higher frequency of extra corporal circuit clotting (hemodialysis and extra corporal membrane oxygenator lines). 9 In another study from France, 21% of severe COVID-19 patients were diagnosed with PE. 34 Similar rates were observed in smaller studies.11,13 Interestingly, in all reported studies, almost all patients were at least on prophylactic dose AC therapy.9–11,13
Studies investigating thrombotic and thromboembolic complication of patients with COVID-19 infection.

AC: anticoagulation; ACS acute coronary syndrome; ALI acute limb ischemia, ASA: aspirin; CVA cerebrovascular accident; DAD diffuse alveolar damage; ICA: internal carotid artery, ICU intensive care unit; MI: myocardial infarction; PE: pulmonary embolism; VTE: venous thromboembolism
Another concerning phenomenon involving the pulmonary circulation in COVID-19 patients has been observed in the form of microvascular thombi. These thrombi were found more frequently than large-vessel clots indicating a local pulmonary hypercoagulable process leading to the observed clinical presentation. 46–45 A post-mortem autopsy study revealed small to medium-sized pulmonary artery thrombi in all investigated patients. 47 The authors hypothesized that COVID-19 infection results in a direct pulmonary thrombosis rather than thromboembolism. 47 Such a manifestation can cause hemorrhagic necrosis, fibrosis, cessation of the pulmonary circulation, acute pulmonary hypertension, and ultimately death. 47 Another post-mortem autopsy study revealed severe endothelial injury with disruption of cell membranes, widespread vascular thrombosis, alveolar-capillary occlusion, and significant angiogenesis. 48 Such microthrombi were found in other organs but at a lower frequency.49,50
Arterial Thromboses and Emboli:
Arterial thromboses were less frequently reported (Table 1) in patients diagnosed with COVID-19. In an early report from Klok et al. the cumulative incidence of arterial thromboses was 3.7%. 10 Similarly, Lodigiani et al. found stroke present in 2.5% of cases while acute coronary syndromes and myocardial infarctions were present in 1.1% of cases among 388 COVID-19 infected patients. 14 A study from Italy showed an increase of patients presenting with acute limb ischemia (ALI) by comparing the first three months of 2020 with those of 2019 (16.3% vs 1.8%, respectively). 38 The patients’ mean age was 75 years, and 25% and 20% had a history of atrial fibrillation and peripheral arterial disease, respectively. 38 Alarmingly, the presentation of arterial thrombosis does not seem to be isolated to patients at higher age and advanced comorbidities. Recent case series have raised concerns about the presentation of young and generally healthy people with large-vessel strokes or ALI.39–51 In a single-center study from Spain, the incidence of arterial thromboses among 1419 admitted patients with COVID-19 was 14 (1%), including acute coronary syndromes, acute ischemic stroke, transient ischemic attack, and limb thrombotic events, respectively. 52
Furthermore, an increased risk of stroke and acute myocardial infarctions (MI), especially stent thromboses, were reported.39,53 Nevertheless, in recently published data from large health care systems involving a large sample size, the incidence of arterial thromboses/emboli was much lower than reported in earlier studies.7,8,35 A report from a large health care system in New York City identified a stroke incidence of 0.9% (32/3556). 51 However, compared to contemporary stroke patients, those with COVID-19 infection were younger, had higher D-dimer levels, were more frequently of the cryptogenic subtype, and had higher inpatient mortality. 51 Similarly, in a retrospective cohort of 1114 patients with COVID-19 diagnosed through Massachusetts General Brigham's integrated health network with independently adjudicated thrombotic/embolic events, stroke and MI incidence were 0.1% (1/1114) and 1.3% (14/1114). 8 Several reasons were postulated for the lower incidence of stroke compared to Chinese patients. 37 Besides the difference in patient characteristics, stroke detection in severely ill COVID-19 patients is challenging, especially in those intubated and sedated. 51 Of note, strokes in patients with COVID-19 more frequently affected large-vessels in younger patients compared to strokes in non-COVID patients. 39 Finally, an independent adjudication of events might have also contributed to the lower rates of arterial thromboses.8,35
Authors of the same health care system in New York presented a series of patients with COVID-19 infection presenting with ST-segment elevation MI (STEMI). 54 Those patients were also characterized by elevated D-dimer and abysmal prognosis (mortality of 72%). 54 Half of those patients underwent angiography, and two-thirds had obstructive disease. 54 Interestingly, in MI patients without COVID-19, the infection has declined in several countries during the first pandemic peak.55,56 Such a decline may have reflected fear of COVID-19 exposure while being evaluated for MI in the hospital. Additionally, delays in the management of STEMI patients during the pandemic's early days were reported.57,58 Such delays were associated with higher rates of short-term complications (eg, cardiogenic shock, congestive heart failure, sustained ventricular tachycardia/fibrillation, use of mechanical circulatory devices, and in-hospital death).57–59 In general, COVID-19 seems to be associated with a myocardial injury related to coronary thrombosis and other non-coronary pathologic mechanisms.49,60,61
Pathophysiology of Thrombosis in COVID-19 Patients
The pathophysiology of COVID-19 associated thrombotic/embolic complications, as stated before, can be highlighted based on Virchow's triad: stasis of blood flow, vessel injury, and hypercoagulability (Figure 1).
SARS-CoV-2 enters the human cells via angiotensin-converting enzyme receptor type 2 (ACE2).62–64 This receptor type is expressed on many human cell types, eg, alveolar cells, cardiac myocytes, podocytes, and endothelial cells (EC).63,65 Consequently, the direct impact of SARS-CoV-2 on the vascular system including veins and arteries is not surprising. EC injury results in tissue factor release, stimulation of the coagulation cascade, triggering of an inflammatory response called “cytokine storm” and activation of the complement system.66,67 Cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) rise dramatically in patients with severe COVID-19 infection. A similar pattern is seen in severe infections caused by other pathogens and are known to be associated with activation of the coagulation system.68–70 Both cytokines promote their prothrombotic features via interaction with EC.68,70,71
Interleukin-6 is an interesting inflammatory marker in its relationship with COVID-19. Several studies suggest elevated IL-6 serum levels positively correlate with worsened disease severity.72–74 A retrospective study by Ruan et al. showed an almost two-fold increase in serum IL-6 level in patients dying from COVID-19 versus those who were discharged from the hospital. 75 Whether this represents a correlation with an overall sicker patient population leading to a more general inflammatory state, versus correlation with a unique inflammatory cascade, is still not fully understood.
Additionally, TNF-α activates the complement system, which stimulates the coagulation system.69,76,77 The enhanced thrombosis is partially mediated by an increase in plasminogen activator inhibitor type 1 (PAI-1), a natural inhibitor of fibrinolysis.78,79 The imbalance between coagulation and fibrinolysis in patients with severe COVID-19 infection “COVID-19 associated coagulopathy (CAC)” is reflected by several markers. A systemic EC insult at the respiratory system level, the gateway of COVID-19 infection, results in dysfunctional haemostasis, fibrinolysis, and vessel permeability,47,48 leading to pulmonary intravascular coagulopathy with prominent capillary thrombosis, vessel wall edema, and hemorrhagic infarction.47,48,79 Once the virus affects EC in other organs, more systemic thromboses and emboli can emerge, including large arterial thromboses.38,39,54
CAC shares features of DIC as well as thrombotic microangiopathy.18,47 In early observations from China, over 71.4% of COVID-19 non-survivors developed DIC according to the international society of thrombosis and haemostasis (ISTH). 15 However, such an observation was not reported in subsequent studies. One must make several distinctions between DIC and CAC. While DIC is primarily characterized by bleeding due to coagulation markers and thrombocytes’ consumption, CAC's hallmark is thrombosis reflected by elevated D-dimer and fibrinogen, a prolonged aPTT, and mild thrombocytopenia.10,13,15,19 Nevertheless, in some late-stage severe COVID-19 infections, overt DIC might occur. 79
Biomarkers of Thrombosis, Risk Stratification and Monitoring
D-dimer and fibrin degradation products (FDP) have emerged as the most robust clinical applied marker to distinguish the risk of thromboembolic complications. They correlate with disease severity and predict outcome.13,15 D-dimer has a high negative predictive value and is recommended to rule out VTE in the general population. 80 In Patients with COVID-19 infection, D-dimer was independently associated with poor prognosis with D-dimer levels > 1 μg/mL being associated with an 18-times increased risk for mortality. 81 More importantly, COVID-19 infection non-survivors showed a progressive increase in D-dimer and FDP compared to survivors.15,81 Furthermore, a continuous elevation of fibrinogen, ferritin, and C-reactive protein may reflect a more deleterious clinical course.79,81,82 PT, aPTT, and thrombocytopenia are also found in patients with COVID-19 infection but do not correlate with disease severity or outcome.13,15,81 Of note, the mild increase in aPTT might be influenced by the development of antiphospholipid antibodies in some patients with severe COVID-19 infection. 9 Although less investigated, von Willebrand factor (vWF) and factor VIII may evolve as markers of activated endothelium.9,34
Like in sepsis and septic shock, thrombocytopenia, and dynamic changes in platelet count in patients with COVID-19 are predictive of outcomes.83,84 The pathology responsible for thrombocytopenia in COVID-19 is not fully understood. However, the alveolar inflammation and thrombosis result in platelet activation and consumption and, more importantly, extramedullary megakaryocytes, leading to exhaustion of the platelet system.83,85 Extramedullary “pulmonary or intravascular” megakaryocytes were found in all major organs of patients with COVID-19 infection, which actively produce platelets. 61 Additionally, direct infection of the bone marrow by the coronavirus with subsequent inhibition of hematopoiesis has been postulated as causative of thrombocytopenia.86,87
Even with the absence of high-quality evidence, the use of these biomarkers’ to monitor coagulation is recommended but should not be used to guide treatment with anticoagulants or antiplatelet agents. 2 Frankly, elevated D-dimer levels without other clinical correlates should not trigger the utilization of therapeutic anticoagulation.2,21,88,89
There is emerging evidence evaluating the role of the neutrophile-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) in predicting COVID-19 infections with a more aggressive course. Existing data retrospectively reviewed hospitalized patients with COVID-19 and found an elevated NLR or PLR at admission correlated with increased morbidity and mortality.90–92 Further data is needed to better understand the predictive accuracy of these markers, as well as understand their relationship to the pathophysiology of COVID-19 infections.
Antithrombotic Therapy in COVID-19 Positive Patients
Antithrombotic therapy in COVID-19 patients can be challenging. Over the last year, several societies and medical associations published recommendations for antithrombotic management of patients with COVID-19.2,21,88,89,93 Currently, the National Institute of Health (NIH) does not recommend routine intermediate or full dose anticoagulation but does recommend all hospitalized non-pregnant adults with COVID-19 be placed on prophylactic dose anticoagulation. 2 Detailed dosing parameters for these various strengths among commonly used inpatient anticoagulants can be found in Table 2. Screening for DVT can be neither recommended nor discouraged based on the current evidence. 2 However, according to the recommendation of the American Society of Echocardiography (ASE), in critically ill patients with COVID-19 admitted to the ICU, DVT assessment may be reasonable by using a two-point compression point of care ultrasound technique. 94 While the treatment of arterial or venous thrombotic or thromboembolic events underlies recent international guidelines95–97 and is summarized in antithrombotic recommendations of institutions and associations,2,21,88,89,93 venous or arterial thromboprophylaxis is still the aim of ongoing studies and clinical experience (Table 3 and Figure 2).

Algorithm for the utilization of antithrombotic prophylaxis and therapy in patients with coronavirus 19 infection.
Commonly used doses of anticoagulation medications in the inpatient setting. 98

aPTT: activated partial thromboplastin time; ACT: activated clotting time; CKD: chronic kidney disease; IV intravenous; SC: subcutaneous; TID: three time per day.
Recommendations of international societies for thrombosis prophylaxis in patients with COVID-19 infection.
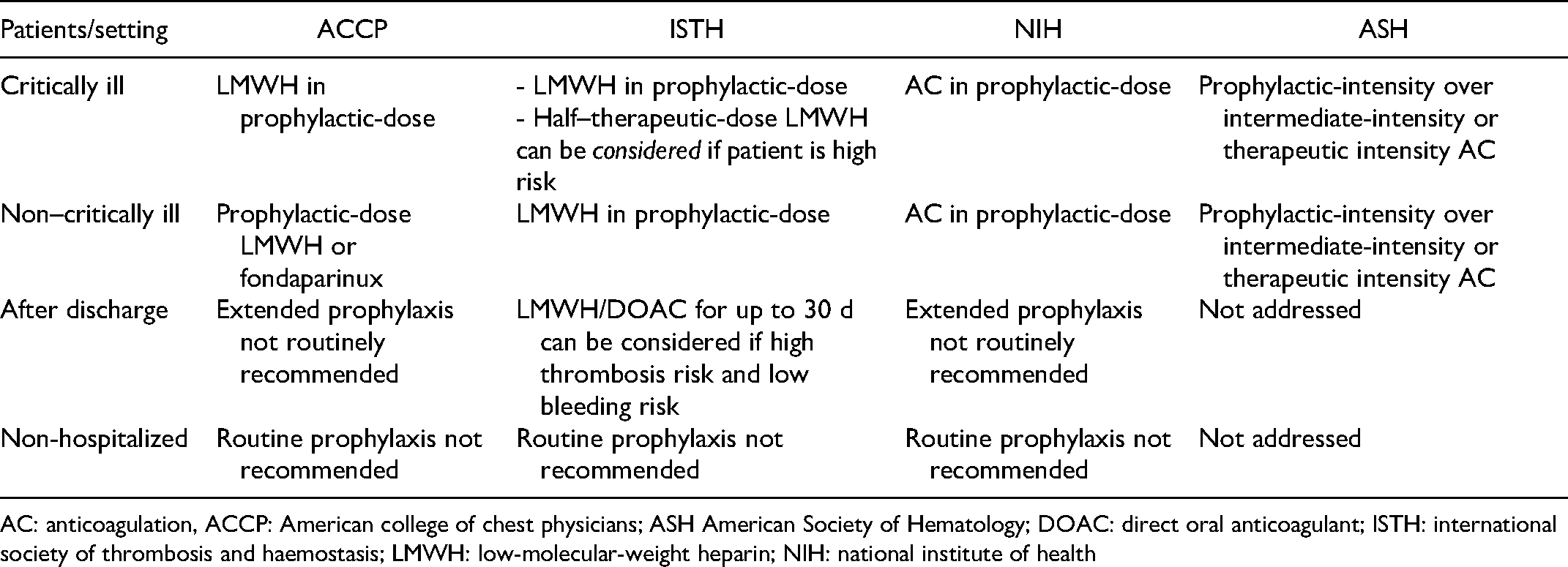
AC: anticoagulation, ACCP: American college of chest physicians; ASH American Society of Hematology; DOAC: direct oral anticoagulant; ISTH: international society of thrombosis and haemostasis; LMWH: low-molecular-weight heparin; NIH: national institute of health
Management of Venous Thromboprophylaxis
The NIH COVID-19 treatment guideline suggests treating hospitalized COVID-19 patients with VTE prophylaxis per the standard of care for other hospitalized patients. 2 However, anecdotally some centers are using doubled antithrombotic dose (ie, intermediate dose) or even therapeutic dose (in high-risk patients or those admitted to the ICU) strategies given the higher incidence of thrombotic complications in COVID-patients requiring mechanical ventilation. 99 Table 2 depicts commonly used doses of unfractionated heparin (UFH) and low molecular weight heparin (LMWH).
Lemos et al. published the first randomized study comparing therapeutic versus prophylactic dose of either LMWH or UFH in COVID-19 patients requiring mechanical ventilation. 100 The primary endpoint was a variation of gas exchange over time (between baseline, 7, and 14 days after randomization) and the secondary endpoint was time to liberation from mechanical ventilation. 100 The authors reported a significant improvement in the gas exchange and higher ratio of liberation from mechanical ventilation and more ventilator-free days in the group treated by therapeutic dose than those treated by a prophylactic dose of anticoagulants. 100 Despite adding reassurance for clinicians, one must stress this study had a low sample size, used surrogate rather than hard clinical endpoints, and was conducted in a single center, reducing the reported findings’ generalizability.
In a retrospective study of 449 individuals with COVID-19, the administration of enoxaparin 40 or 60 mg once daily was associated with a lower mortality rate in patients with high sepsis-induced coagulopathy (SIC) score or elevated D-dimer, but not in the whole cohort, when compared with nonusers. 101 More recently, another retrospective large-sample size study of 4389 patients with proven COVID-19 infection, prophylactic and therapeutic anticoagulation were both associated with lower in-hospital mortality and a lower intubation rate in comparison to patients who did not receive anticoagulation. 35 In adjusted analyzes, a trend towards reducing in-hospital mortality was detected for therapeutic anticoagulation compared to prophylactic anticoagulation; however, this must be interpreted with caution as they are largely hypothesis generating given the inherit biases that exist within observational studies.
Several larger scale randomized trials are currently awaited to shed more light on the risks and benefits of prophylactic, intermediate, or therapeutic dose AC for patients with COVID-19 infection. 102 On December 22nd, 2020, the NIH announced a pause on enrollment of patients with critically ill COVID-19 in the Anti-thrombotics for Adults Hospitalized With COVID-19 (ACTIV-4) trial1 103 due to potential harm and futility of the therapeutic AC regimen as described by the independent overseeing board. Nevertheless, enrollment of moderately ill COVID-19 patients continued. 104
Additional trials are currently ongoing to investigate the ideal antithrombotic management for patients with COVID-19. An interim analysis of a multiplatform randomized controlled trials (ACTIV-4, REMAP-CAP and ATTACC) has been published online on January 28th 2021. 105 The analysis indicates that in patients with moderate COVID-19 (hospitalized but not initially requiring ICU therapies/level of care) therapeutic AC with UFH or LMWH is superior to prophylactic dose AC regarding the reduction of the primary endpoint of organ support-free days (to day 21). 105 The superiority of such strategy was evident regardless of D-dimer levels at randomization. Nevertheless, the very same strategy was shown to be futile and potentially harmful when applied on patients with severe COVID-19 infection (receiving organ support/ICU level care). Several issues remain to be discussed regarding the interpretation of this analysis. First, most of the data was provided by one trial, the Randomised, Embedded, Multi-factorial, Adaptive Platform Trial for Community-Acquired Pneumoniatrial (REMAP-CAP) (84%). Second, the majority of the enrolled patients were from the United Kingdom where intermediate dose was applied as standard of care for thrombosis prophylaxis. 106
More evidence suggests little benefit with potential harm in therapeutic-dose versus prophylactic-dose anticoagulation. A randomized controlled trial by Lopes et al. compared these two arms in patients hospitalized with COVID-19 symptoms. The authors found a statistically non-significant difference in the primary endpoint, a composite of death, duration of hospitalization, or duration of supplemental oxygen use through 30 days when comparing therapeutic with prophylactic anticoagulation (34.8% vs 41.3%; P = .40). 107 However, more aggressive anticoagulation was associated with higher risk of major bleeding and/or clinically significant non-major bleeding was statistically worse in the therapeutic dose anticoagulation arm (8% vs 2%; P = .001). 107
Another randomized clinical trial, Intermediate-dose versus Standard Prophylactic Anticoagulation and Statin versus Placebo in ICU Patients With COVID-19 (INSPIRATION) showed no difference in the primary endpoint of composite of venous or arterial thrombosis, treatment with extracorporeal membrane oxygenation, or mortality within 30 days comparing intermediate with standard prophylactic dose of AC in patients with COVID-19 infection admitted to ICU (45.7% vs 44.1%; P = .70). 108 The findings from those randomized control trials are also supported by reports from observational studies. 109 It appears that patients with moderate or severe COVID-19 infection do not derive benefits from dose escalation of antithrombotic therapy. However, it is not clear how to change thromboprophylaxis in a patient with moderate COVID-19 who progresses to severe illness..105,106
The evidence is sparse but there is recent data to help guide anticoagulation management in outpatients suffering from COVID-19. Conners at al recently published a paper in JAMA evaluating outcomes in symptomatic COVID-19 outpatients randomized to aspirin, apixaban 2.5 mg twice daily, apixaban 5 mg twice daily, and placebo. They found no significant difference in composite outcomes after 45 days of therapy between the active groups and the placebo group. 110 It should be noted the trial was stopped early due to an unanticipated overall low event rate.
Alternative AC for Patients with Heparin Induced Thrombocytopenia (HIT):
Generally there is an overall low incidence of HIT with UFH and LMWH, 3% and 0.2% respectively. 111 Nevertheless, fondaparinux, bivalirudin or argatroban might be a considerable option in patients with heparin induced thrombocytopenia. 112 Two clinical trials are being conducted to investigate the safety and efficacy of these drugs in patients with COVID-19.113,114 The use of direct oral anticoagulants (DOAC) in patients with COVID-19 is a matter of great debate. While proponents advocate its use in moderate COVID-19 patients to protect health care worker form exposure to the patients one must stress that using DOACs in critically ill patients in ICU settings cannot be recommended as the bioavailability and gastrointestinal absorption of these drugs are uncertain. 115 Additionally, several drug-drug interactions between anticoagulants and antiviral medicines have been reported.89,115 A study in 32 patients on chronic DOACs and COVID-19 infection treated with antiviral drugs showed alarmingly high plasma levels of the anticoagulant. 115 Several trials are currently being conducted to elucidate the role of DOAC in patients with moderate COVID-19 infection. 113 Furthermore the role of DOAC in the post-discharge period is also an important niche. 113 Currently, data on the antithrombotic management of patients with COVID-19 after hospital discharge is scarce. A study investigating the rate of post-discharge VTE in patients after COVID-19 admission showed no increased risk of VTE compared to discharges of other medicine patients. 116 Most experts recommend using thromboprophylaxis if immobilization persists after discharge and stopping it if the patient returns to daily life (Table 3) (Figure 2). Nevertheless, several randomized clinical trials are currently being conducted to investigate the impact of AC in the post-discharge phase. 113 However, in the absence of clinical evidence of VTE or a thrombotic event, therapeutic anticoagulation cannot be recommended outside the setting of clinical trials. 2
Monitoring AC in Patients with COVID-19 Receiving Thromboprophylaxis:
In general monitoring anticoagulation in patients undergoing thromboprophylaxis dose of AC is not necessary. Nevertheless, in the elderly, patients with chronic kidney disease, and those with the extremes of body weight (especially those who are underweight) might profit from monitoring AC levels. In patients with COVID-19, increased plasma levels of fibrinogen and Factor VIII can result in shortening of the aPTT. 117 Alternatively, Anti-Factor Xa activity measured 4 h after the third dose of UFH/LMWH can be considered.
Antiplatelet Agents for Thromboprophylaxis
A recent in-vitro study elucidated the fundamental role of platelet activation in the process of cytokine storm in COVID-19 infection. Platelet activation and tissue factor release by COVID-19 could be blunted by the interleukin-6 inhibitor Tocilizumab or aspirin. 118 Furthermore experimental data in mice indicate that aspirin can reduce intravascular thrombin activity and microvascular occlusion in staphylococcus aureus-induced sepsis. 119 This finding is in line with the results of a contemporary meta-analysis of cohort studies that found that antiplatelet therapy, particularly aspirin, was associated with decreased mortality in patients with sepsis. 120 However, it remains unclear whether this applies to patients suffering from COVID-19. Retrospective studies have indicated that patients on chronic aspirin treatment were associated with lower risks of mechanical ventilation, ICU admission, and in-hospital mortality. 121
There is limited information about the effect of antiplatelet drugs in critically ill patients with COVID-19 patients. A small-sample study showed that a combination of anticoagulant and antiplatelet therapy could reduce the pro-coagulant pattern of the blood measured by viscoelastic tests (clot stiffness and clot time). 26 Recently Meizlish et al. performed a propensity-matched analysis of patients with COVID-19. 122 The authors found a mortality benefit for intermediate-dose anticoagulation and aspirin compared to prophylactic-dose anticoagulation and no aspirin. 122 Another small sample-size randomized study investigated the clinical outcome of COVID-19 patients treated with dipyridamole versus placebo. 123 Patients in the dipyridamole arm had a significant reduction of D-dimer levels, as well as increased lymphocyte and platelet counts, as well as an overall beneficial clinical outcome. 123
Ticagrelor has been shown to reduce circulating platelet-leucocyte aggregates, interleukin-6 levels and improve oxygen requirements in patients admitted with pneumonia. 124 The effect of ticagrelor in patients with severe COVID-19 infection with or without thrombosis has not been investigated yet.
The CHEST Guideline, Expert Panel Report and NIH COVID-19 treatment guidelines discourage using antiplatelet agents to prevent arterial thromboses.2,88 Additionally, it is essential to avoid antiplatelet therapy 24 h after thrombolysis or mechanical thrombectomy in stroke patients. 125 It is critical to mention the risks and benefits of thrombolysis or mechanical thrombectomy. Several randomized controlled trials (RCTs) are currently underway to elucidate the role of antiplatelet therapy alone or in combination with other antithrombotic agents in patients with COVID-19 and are summarized by Talasaz et al.. 102
Considerations for Vulnerable Patients and Subgroups:
Several vulnerable populations and subgroups such as children, pregnant women, and the immune compromised should be mentioned. The amount of evidence for might be limited since these patients are mostly excluded from clinical trials. In children with COVID-19 infection, the same thromboprophylaxis should be applied as for those without COVID-19 infection according to the NIH. 2 Similarly pregnant women with severe COVID-19 infection should receive prophylactic dose of AC. 2 Anticoagulation therapy use during labor and delivery requires specialized care and planning and should be managed in pregnant patients with COVID-19 in a similar way as in pregnant patients with other conditions that require anticoagulation in pregnancy. 2 COVID-19 patients may be placed in an immune compromised state as suggested by an increased risk of mucormycosis infection identified in a recent met-analysis. 126 This relationship and its association with the morbidity and mortality of COVID-19 infected patients will require further study.
Conclusion
In summary, infection with SARS-Cov2 may result in serious illness requiring admission to ICU. Those patients are at risk of developing ARDS and thrombotic complications associated with a higher risk of mortality. Several biomarkers have been introduced and investigated, which may support more aggressive medical management of the infection, including anticoagulation therapy. Prophylactic antithrombotic strategies to avoid venous or arterial thrombotic/thromboembolic events are still in discussion and/or evaluation.
Prophylactic dose anticoagulation appears to be associated with the best efficacy and safety ratio as compared to regimen using intermediate or therapeutic doses of anticoagulation in patients hospitalized with COVID-19.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because there is no patient protected information in the article.