
Abstract
Background
Cases of thrombosis with thrombocytopenia syndrome (TTS) have been reported following vaccination with AZD1222 or Ad26.COV2.S. This review aimed to explore the pathophysiology, epidemiology, diagnosis, management, and prognosis of TTS.
Methods
A systematic review was conducted to identify evidence on TTS till 4th September 2021. Case reports and series reporting patient-level data were included. Descriptive statistics were reported and compared across patients with different sexes, age groups, vaccines, types of thrombosis, and outcomes.
Findings
Sixty-two studies reporting 160 cases were included from 16 countries. Patients were predominantly females with a median age of 42.50 (22) years. AZD1222 was administered to 140 patients (87·5%). TTS onset occurred in a median of 9 (4) days after vaccination. Venous thrombosis was most common (61.0%). Most patients developed cerebral venous sinus thrombosis (CVST; 66.3%). CVST was significantly more common in female vs male patients (p = 0·001) and in patients aged <45 years vs ≥45 years (p = 0·004). The mortality rate was 36.2%, and patients with suspected TTS, venous thrombosis, CVST, pulmonary embolism, or intraneural complications, patients not managed with non-heparin anticoagulants or IVIG, patients receiving platelet transfusions, and patients requiring intensive care unit admission, mechanical ventilation, or inpatient neurosurgery were more likely to expire than recover.
Interpretation
These findings help to understand the pathophysiology of TTS while also recommending diagnostic and management approaches to improve prognosis in patients.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Keywords
Introduction
Having exerted widespread effects over all spheres of society, the coronavirus disease 2019 (COVID-19) pandemic has forced government and healthcare institutions to divert resources and develop methods to curtail it. Vaccines have been put under extreme emphasis as the prime method of halting transmission, with over one billion doses administered worldwide.
Among these vaccines, the Oxford-AstraZeneca (AZD1222) and the Johnson & Johnson (Ad26.COV2.S) have recently been implicated in an extremely rare prothrombotic disorder comprising of thrombosis in uncommon sites with concurrent thrombocytopenia and development of anti-platelet factor 4 (anti-PF4) antibodies.1,2 This disorder has been termed as thrombosis with thrombocytopenia syndrome (TTS).
Owing to its atypical presentations, TTS can present as a diagnostic challenge for healthcare workers. The common manifestations range from routine constitutional changes to visual defects, severe headaches, leg and back pains, easy bruising, or petechiae. Unchecked, TTS may lead to cerebral hemorrhages and fatality.1,3 As reports of TTS came to light, administration of both vaccines was temporarily restricted, with Denmark and Norway permanently halting the AZD1222 vaccine.
Similar to its rare occurrence, current evidence on TTS is also limited, existing in the form of case reports and series. Further hampering this issue, a large proportion of available data is centered around pharmacovigilance programs, such as Vaccine Adverse Event Reporting System (VAERS) and Medicines and Healthcare products Regulatory Agency (MHRA).4,5 While these systems are excellent at providing early warnings for pharmacological adverse events, their capacity to inform clinical decision-making is limited, owing to their reliance on non-standardized patient-reported outcomes.
We conducted a systematic review of patient-level data with the aim of summarizing the limited data available and explore the pathogenesis, epidemiology, clinical features, diagnoses, management, and prognoses in TTS patients.
Methods
The protocol of this review is registered with PROSPERO CRD42021252688, and this review has been reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Electronic Searches
An exhaustive literature search was conducted on PubMed, Embase, CINAHL, Scopus, LILACS, Global Index Medicus, World Health Organization (WHO) COVID-19 Database, Europe PMC, ScienceDirect, Preprints, medRxiv, Open Science Framework (OSF), and Research Square to identify all scientific literature available till 4th September 2021. No language restrictions were applied. The strategies employed for searching these databases are documented in Supplementary Appendix (p3-7).
In addition, reference lists of all identified review articles and included studies were checked for additional references. To identify potentially relevant gray literature, reports and guidelines published by several hematological and pharmacovigilance organizations were hand searched (appendix p8).
Selection Strategy
Case reports and series providing patient-level data on TTS cases were included in this review. Patients with radiologically confirmed venous or arterial thrombosis and associated thrombocytopenia (platelet count <150 000/mm3) occurring within 4 to 30 days of administration of AZD1222 or Ad26.COV2.S vaccine were classified as confirmed TTS cases if their enzyme-linked immunosorbent assay (ELISA) heparin-PF4 antibodies were positive. 3 Patients meeting the above criteria but with missing ELISA results were considered suspected cases.
EndNote x9 by Clarivate Analytics was used to remove duplicate records. Title and abstracts of deduplicated records were screened by UW and SA independently using Rayyan QCRI. 6 Full-text review was independently performed by MST and AH. All discrepancies were resolved through discussion and consensus.
Data Extraction
Data extraction from the included studies was performed by SMG, MST, ZA, and AH using a structured Microsoft Excel 2016 worksheet. The worksheet was piloted prior to data extraction on two studies randomly selected from the included studies.
The extracted variables included: study characteristics (country, setting, type); patient demographics (age, sex, ethnicity, comorbidities, current medications, SARS-CoV-2 infection status, SARS-CoV-2 serology, vaccine administered, number of doses administered); clinical manifestations (time of onset of TTS after vaccination, presenting signs and symptoms); radiological characteristics (imaging modalities, venous/arterial thrombosis, blood vessel(s) involved); laboratory parameters (platelet count, hemoglobin, leukocytes, fibrinogen, aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyltransferase (GGT), lactate dehydrogenase (LDH), serum creatinine, lactate, C-reactive protein, D-dimers, activated partial thromboplastin time (APTT), prothrombin time (PT), thrombin time (TT), international normalized ratio (INR), blood film, antiphospholipid antibodies, anti-PF4 antibodies); therapeutic management (heparin, steroids, intravenous immunoglobulins (IVIGs), platelet transfusions, non-heparin anticoagulants, thrombectomy, intensive care unit (ICU) admission, mechanical ventilation); and outcomes (complications, recovery, mortality).
Comorbidities, current medications, SARS-CoV-2 infection status, recent exposure to heparin prior to TTS onset, and complications were assumed negative unless otherwise specified in included studies. However, these characteristics were marked unknown when studies reported aggregated data and it was not possible to disaggregate data to individual patients. Management options were marked unknown for studies reporting aggregated data and for studies not documenting at least one of the following management options: heparin, steroids, intravenous immunoglobulins (IVIGs), platelet transfusions, and non-heparin anticoagulants. For remaining studies, management options were assumed negative unless otherwise specified.
TTS onset was defined as the time of the first symptom occurring on or after the fourth day of vaccination. For all laboratory parameters, we extracted the first-available and most abnormal results. Severe thrombocytopenia was defined as a platelet count ≤25 000/mm3. The final dataset was rechecked thrice for accuracy by SMG, MST, and ZA by referring to original studies, and all discrepancies were resolved accordingly.
Statistical Analyses
Analyses were performed on IBM SPSS Statistics version 24. Descriptive statistics were reported. Shapiro-Wilk tests for normality were performed to assess the distributions of continuous variables (Table S1, appendix p9-10), and they were presented as means ± standard deviations or medians (interquartile ranges [IQRs]) as appropriate. Categorical variables were summarized using frequencies and percentages.
Clinicodemographic characteristics were compared across patients with different sexes, age groups, vaccines, types of thrombosis, and outcomes. For these comparisons, continuous variables, such as age, days from vaccination to TTS onset, and days from vaccination to hospitalization, were converted to categorical variables. These comparisons were performed using chi-squared tests or Fisher's exact tests, when assumptions for the former were not met. Missing data were included in analyses, allowing denominators to remain consistent. For sensitivity analyses, clinicodemographic characteristics were compared across patients with different outcomes after excluding suspected TTS cases. All analyses were two-sided with p <0·05 considered threshold for statistical significance.
Quality Assessment
Quality assessment of included studies was independently conducted by UW and SA using the National Institute of Health Quality Assessment Tool for Case Series Studies. 7 Each case series was scored out of nine, based on clarity of study objectives, case definition, consecutive subject recruitment, comparability of subjects, clarity of intervention, definition and measurement of outcomes, length of follow-up, statistical methods, and results. A case series scoring seven to nine was considered good quality, four to six fair considered quality, and less than four considered poor quality. Consecutive subject recruitment, comparability of subjects, and statistical methods were excluded from the scoring criteria for case reports, which were consequently scored out of six. Case reports scoring six were considered good quality, three to five considered fair quality, and less than three considered poor quality.
Results
The literature search yielded 36 734 studies after deduplication (Figure 1). Out of these, 92 studies were reviewed as full text and 62 studies were included according to our inclusion criteria (Table S2, appendix p11-26).1,2,8-67 The remaining 30 studies were excluded (Table S3, appendix p27-28).

PRISMA flow diagram of study selection process
Among the included studies, 21 studies were case series while 41 were case reports. Most studies were published at the time of reporting of this review, except for three which were preprints.14,23,28 Majority of the studies (N = 59) originated from high-income countries (HICs), with most being reported from United Kingdom (Table 1).
Distribution of studies (N = 62) and TTS cases (N = 160) according to country of origin
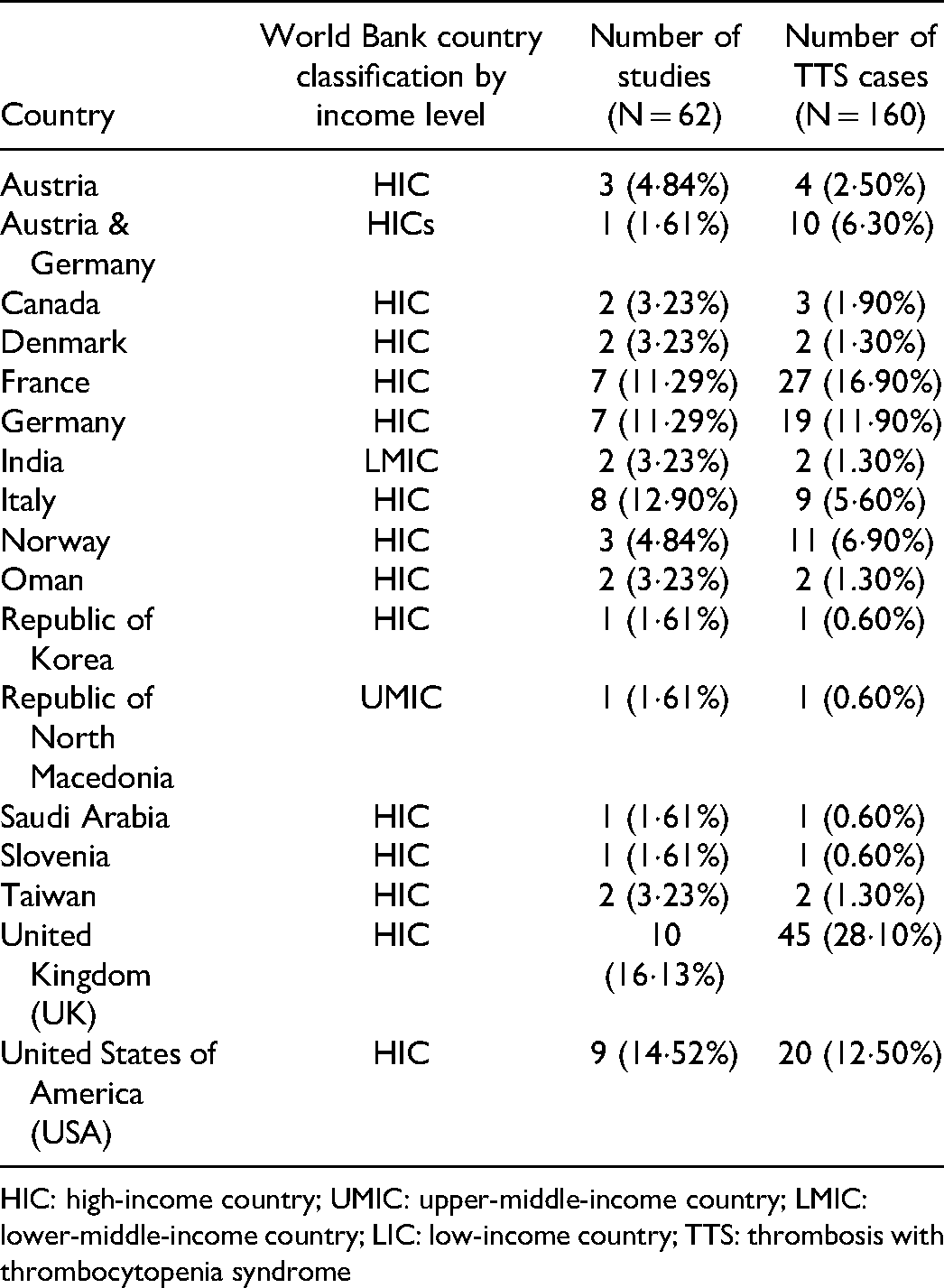
HIC: high-income country; UMIC: upper-middle-income country; LMIC: lower-middle-income country; LIC: low-income country; TTS: thrombosis with thrombocytopenia syndrome
Patient Demographics
From the included studies, 160 patients (120 confirmed and 40 suspected) were included in this review after excluding 21 ineligible patients (Table S4, appendix p29). The patients were predominantly females with a median age of 42·50 years (IQR 22, range 21–77 years; N = 132). Most patients were from the United Kingdom and France (28·1% [45 of 160] and 16·9% [27 of 160], respectively). Ethnicity was documented for only 29 patients, out of which, 26 were Caucasians and 3 Asians.
At the time of vaccination, most patients had insignificant preexisting comorbidities, active medications, exposure to heparin, and pregnancy status. Only two patients (1.3% [2 of 160] had documented history of prior SARS-CoV-2 infection, while another patient (0·6% [1 of 160]) had COVID-19 at presentation. COVID-19 serology was positive in 38 of 59 patients (64·4%), with all patients developing antibodies against the spike glycoprotein (Table 2). Among patients who had received Ad26.COV2.S vaccine, COVID-19 serology was insignificant in 5 (100% [5 of 5]) and unknown in the remaining 15 patients (Table S6; appendix p33–35).
Clinicodemographic characteristics of all patients (N = 160)

TTS: thrombosis with thrombocytopenia syndrome; CVST: cerebral venous sinus thrombosis; LMWH: low-molecular-weight-heparin; IVIG: intravenous immunoglobulin; ICU: intensive care unit
Clinical Manifestations
A total of 140 of 160 patients (87·5%) were administered AZD1222 while the rest had received Ad26.COV2.S vaccine. For patients receiving AZD1222 vaccine, onset of TTS predominantly occurred after the first dose (76/77, 98.7%), while dosages were unknown for the remaining 63 patients. The median number of days from vaccination to TTS onset and hospitalization were 9 (4; N = 131) and 11 (5; N = 113), respectively. Patients who were hospitalized within 15 days of vaccination were more likely to have received AZD1222 vaccine than Ad26.COV2.S vaccine (p <0.0010); Table S6, appendix p33–35). Patients had a median length of hospital stay of 7 (11; N = 40) days.
Venous thrombosis was most common among patients, followed by combined arterial and venous thrombosis and isolated arterial thrombosis. Most patients developed cerebral venous sinus thrombosis (CVST), predominantly affecting the transverse, sigmoid, and sagittal sinuses. CVST was significantly more common in in female vs male patients (p = 0·001; Table S7, p36–38) and in patients aged <45 years vs ≥45 years (p = 0·004; Table S8, p39-41). Splanchnic vein thrombosis (SVT) and pulmonary embolism (PE) were also documented in a subset of patients. Other relatively common locations of thrombosis were deep veins, internal jugular vein, and portal vein (14·4% [23 of 160], 11·3% [18 of 160], and 10.6% [17 of 160]], respectively).
Presenting symptoms commonly included severe headache or neurologic changes in patients with CVST; abdominal pain or backache in patients with SVT; chest pain or shortness of breath in patients with PE; and leg pain or swelling in patients with deep vein thrombosis (DVT). Symptoms of thrombocytopenia, such as petechiae or mucosal bleeding, were often present as well. Computed tomography (CT), magnetic resonance imaging (MRI), ultrasound, and digital subtraction angiography were the most common imaging modalities employed to visualize thrombosis and associated complications.
Laboratory Parameters
ELISA for PF4 antibodies was positive in 120 patients (100% [120 of 120]), while 15.6% patients (25 of 160) were tested with unspecified assays and 5·6% patients (9 of 160) were not tested for anti-PF4 antibodies. Serotonin release assays (SRAs) were used in six confirmed patients and yielded positive results. Among the rapid HIT assays, chemiluminescence immunoassays (CLIAs) were negative in four confirmed patients, latex-enhanced immunoassays negative in three confirmed and two suspected patients, and lateral flow immunoassays negative in one confirmed and one suspected patient.
All patients had a significant decline in platelet count at diagnosis, but the exact platelet counts were missing for 28 patients. Among the remaining patients, 45.5% (60 of 132]) developed severe thrombocytopenia. Additionally, many patients had elevated levels of D-dimers, PT, TT, and INR with low levels of fibrinogen. Blood films results were documented for 12 of 160 patients (7.5%), revealing schistocytes and platelet anisocytosis in 16.7% patients each (2 of 12). Antiphospholipid antibodies were assessed in 71 (44·4% [71 of 160]) and were positive in 4 patients (5·6% [4 of 71]).
Therapeutic Management
Heparin was administered to 35 patients (37.2% [35 of 94]), with majority receiving low-molecular-weight-heparins (LMWHs). Most patients were administered steroids, IVIG, and non-heparin anticoagulants. A subset of patients was also managed with platelet transfusions, endovascular thrombectomy, ICU admission, and mechanical ventilation.
Complications and Outcomes
A significant proportion of patients developed hemorrhages (60 of 160 patients, 37·5%), with intracranial hemorrhages being more common than extracranial hemorrhages. Subtypes of intracranial hemorrhage included intracerebral (56.8% patients [21 of 37]), subarachnoid (32.4% [12 of 37]), combined intracerebral and subdural (2.7% [1 of 37]), and combined intracerebral and subarachnoid hemorrhages (8.1% [3 of 37]). Subtypes of intracranial hemorrhage were unknown for 21 patients. Extracranial hemorrhages involved the gastrointestinal system (GIT), adrenal glands, conjunctiva, and surgical site (33·3% [2 of 6], 33·3% [2 of 6], 16·7% [1 of 6], and 16·7% [1 of 6] patients, respectively).
Other intraneural complications commonly included brain herniation (18 of 160 patients, 11·3%) and cerebral edema (11 of 160 patients, 6.9%). These complications were significantly more common in patients who were administered AZD1222 vaccine vs Ad26.COV2.S vaccine (p = 0·046; Table S6, appendix p33-35).
Extra-neural complications were relatively uncommon, primarily manifesting as edema, ischemia, or infarction of the bowel wall, cardiac arrest, myocardial infarction, severe acute respiratory syndrome, or toe infarction. The incidence of extra-neural complications was higher in patients with combined arterial and venous thrombosis vs isolated arterial or venous thrombosis (p = 0·017; Table S9, appendix p42-44).
The mortality rate in this review was 36·2% (47 of 130), while outcomes were unknown for 30 patients. Compared to recovery, mortality was more common among suspected TTS patients, patients with venous thrombosis, CVST, pulmonary embolism, or intraneural complications, patients not managed with non-heparin anticoagulants or IVIG, patients receiving platelet transfusions, and patients requiring ICU admission, mechanical ventilation, or neurosurgery (Table S10, appendix p45-47).
On sensitivity analysis, treatment with IVIG was not significantly associated with mortality or recovery. Additionally, mortality was found to be more common compared to recovery in patients receiving oral contraceptives (p = 0·0090) and those developing intracranial hemorrhages (p = 0.0080). The validity of other findings remained unchanged (Table S11, appendix p48-50).
Quality Assessment of Included Studies
A total of 37 studies were determined to be of good quality while the remaining 25 studies were of fair quality (Table S5, appendix p30-32). Studies were primarily downgraded for unclear study population,9,10,12,15,16,20,25,26,35,37,38,42,45,46,50-53,57-59,62,64-66 non-consecutive subject recruitment,1,2,8,9,11,20-23,28,29,31,35,37,65,67 incomparable subjects,20,35,37 unclear intervention,2,8,9,16,21,22 inadequate length of follow-up,1,2,9,19,22,28,32,67 inadequate description of statistical methods,20,35,42 and inadequate description of results. 20 Common causes for downgrading studies were unclear study population and non-consecutive subject recruitment, raising concerns that the included sample could be biased towards severer presentations.
Discussion
Manifesting with atypical thrombosis, thrombocytopenia, and anti-PF4 antibodies, TTS is an extremely rare but serious platelet-activating prothrombotic disorder that clinically resembles spontaneous HIT.68-70 The concurrence of thrombosis and thrombocytopenia in TTS indicates an immunological etiology contributing to the hypercoagulable state. 71 In the case of HIT, the prothrombotic state has been associated with IgG-specific antibodies, capable of recognizing multimolecular complexes between the cationic PF4 and the anionic heparin. 69 However, the unique aspect of TTS is that there is no prior exposure to heparin that can explain the subsequent development of thrombosis and thrombocytopenia. While existing theories have proposed that one or more anionic components of the vaccines could be triggering the formation of anti-PF4 antibodies, the exact pathophysiology of TTS remains an active area of investigation globally. 1
Implicated in the development of TTS, AZD1222 and Ad26.COV2.S are adenoviral vector-based vaccines encoding the spike glycoprotein. Our review identified more cases of TTS patients who were administered AZD1222 compared to patients who received Ad26.COV2.S. While the exact reason for this pattern is unknown, we propose several hypotheses that could explain this difference.
First, AZD1222 uses a chimpanzee vector while Ad26.COV2.S utilizes the human Ad26-based vector, engaging different host cell receptors. Additionally, Ad26.COV2.S vaccine transgene encodes for a membrane-bound SARS-CoV-2 spike glycoprotein that does not shed S1, which is substantially different from the unmodified spike glycoprotein coded by AZD1222. These differences can lead to different phylogenetic and biological characteristics, potentially resulting in different vaccine safety with regards to TTS. 72 However, another adenoviral vaccine, Sputnik V, also utilizes the human Ad26 serotype along with Ad5 serotype in two separate doses, 73 and despite being administered in multiple countries, there are no reported cases of TTS following vaccination with Sputnik V till date. 74
Second, TTS is an extremely rare disorder with an incidence rate ranging from 1 in 125 000–1,000,000 individuals vaccinated for SARS-CoV-2. 75 Across 31 countries with data available, AZD1222 has been administered to approximately 48 million individuals compared to 19 million who received Ad26.COV2.S till 25th June 2021. 76 Additionally, both vaccines are being administered in different parts of the world, with AZD1222 being more common in Europe and Ad26.COV2.S being more common in the United States. Pharmacovigilance capacities differ significantly between Europe and the United States, which could potentially lead to differences in reporting of TTS. 77 Regardless, these hypotheses cannot be confirmed in the absence of reliable epidemiological data originating from high-quality and uniform pharmacovigilance systems.
In our review, a majority of TTS patients were females, those aged 30–49 years, and those without any known comorbidities. These gendered trends could be attributed to the clinical and pathophysiological resemblance of TTS with HIT, considering that females have twice the risk of developing HIT compared to males. 78 Existing theories explaining these trends in HIT are based upon sex-dependent immune responses to heparin-PF4 multimolecular complexes. 78 However, the extent to which these theories can be extrapolated to TTS is currently unknown, owing to the absence of heparin exposure in TTS patients. On the other hand, TTS patients in our review exhibited contradictory age trends compared to HIT, which is rare in patients aged <40 and has a higher incidence in older patients. 79
Among all patients, venous thrombi were more common compared to arterial thrombi, another feature that TTS shares with HIT. 80 However, while statistically insignificant, male patients more often developed arterial thrombosis compared to female patients in this review. Generally, risk factors contributing to stasis and hypercoagulability components of the Virchow's triad are most significant for venous thrombosis, while those contributing to vessel wall changes relatively stand out more in arterial thrombosis. 81 Most of the female patients included in this review were 21–49 years of age, and hence, are expected to have protective effects of estrogen on blood vessel walls. 82
Additionally, existing literature had hypothesized that, compared to younger patients, older TTS patients might be more likely to present with arterial thrombosis. 83 This could be attributed to the post-menopausal loss of protective effects of estrogen, considering that most patients with TTS were females. Our review also identified the incidence of arterial thrombosis to be higher in patients aged ≥45 vs <45 years, but this difference was not statistically significant.
When compared with HIT, another contradictory characteristic of TTS is that a majority of patients develop CVST more so than elsewhere in the body, as highlighted in our review. On the other hand, CVST is extremely rare in patients with HIT, with very limited number of cases documented in literature. 84 While the pathophysiology of CVST in the setting of TTS warrants further investigations, our findings indicate that CVST is significantly more common in female patients and patients aged <45 years. Intracranial hemorrhages have traditionally been common in CVST patients, developing in nearly one-third of cases. 85 This can explain the high proportion of TTS patients with intracranial hemorrhages observed in our review.
For diagnostic purposes, existing guidelines recommend testing suspected TTS patients for anti-PF4 antibodies prior to initiation of therapy, particularly using the ELISA assay. 3 Individuals with TTS often have high optical density (OD) readings, ranging from 2·00 to 3·00 or even higher, which are sufficient to inform diagnosis in the setting of thrombosis and thrombocytopenia following recent COVID-19 vaccination without any exposure to heparin.1,31 Despite being the gold-standard for diagnosing HIT, SRAs are often not required in suspected TTS patients with strongly positive ELISA results, with our review only identifying six patients tested with SRAs. This can be attributed to the higher cost, turnaround time, and resource intensiveness associated with SRAs, limiting their use in most settings around the globe. 86 While the sensitivity and specificity of SRAs and ELISA have not been compared in TTS patients, evidence extrapolated from HIT suggests that SRAs, however, could potentially be helpful in patients with negative or equivocal ELISA findings but strong suspicion of TTS, owing to their greater specificity in HIT. 87 However, this necessitates further investigations, considering that patients with negative ELISA results were excluded from this review.
We recommend that rapid HIT assays, such as CLIAs, latex-enhanced immunoassays, and lateral flow immunoassays, should not be used to confirm or exclude diagnosis of TTS. While these assays can provide rapid results with credible diagnostic accuracy in the case of HIT, 88 they were consistently negative in TTS patients included in this review.
Physicians suspecting TTS should have a lower threshold for conducting diagnostic investigations, including complete blood count and imaging based on presenting symptoms. Upon detection of thrombocytopenia and thrombosis, ELISA, D-dimers, fibrinogen, PT, and APTT should be immediately requested to confirm the diagnosis. In our review, suspected patients who were not tested with ELISA were more likely to expire than recover, highlighting the significance of early diagnostic investigations and subsequent treatment initiation.
In this review, unfractionated heparins were less commonly administered to patients compared to LMWHs. Because of inadequate sample size, we cannot conclusively comment on the safety of either of these in TTS patients. However, LMWHs might be safer considering that they have smaller sizes which limit their interaction with PF4 and platelets, translating into a lower risk of immune sensitization and subsequent development of HIT.89,90 If immune sensitization still occurs, the antibodies generated by LMWHs belong to the IgA and IgM classes, which are less associated with development of HIT, as opposed to the IgG antibodies generated by unfractionated heparins. 90
Non-heparin anticoagulants, such as argatroban, danaparoid, fondaparinux, or direct oral anticoagulants, remain a better alternative to heparin for TTS patients, considering that they are not associated with HIT and that patients not managed with non-heparin anticoagulants were more likely to expire than recover in our review. IVIG should also be used in conjunction with non-heparin anticoagulants, owing to its success in the treatment of spontaneous HIT.91,92 We also recommend avoiding platelet transfusions due to their potential of exacerbating the thrombotic symptoms. Our review identified a higher likelihood of mortality compared to recovery among patients receiving platelet transfusions.
While this review attempts to build upon the gaps in existing literature, more investigations are still required to completely understand the pathophysiological elements of TTS, considering that most existing theories have been extrapolated from evidence based on HIT. Additionally, despite the suggestive temporal relationship of AZD1222 or Ad26.COV2.S with TTS, caution is required when drawing conclusions about the safety of these vaccines. TTS is an extremely rare disorder, and the unexpected risk of TTS following vaccination is insubstantial compared to the risk of developing COVID-19 without vaccination. 3
This review has several limitations which need to be accounted for while interpreting our results. First, since TTS is an extremely rare disorder, we could only identify 160 patients, and those too with a lot of missing data, impacting the quality of our analyses. Second, some laboratory assessments were not conducted in a significant number of patients. Third, we included case reports and case series in this review, each of which might have separate confounders which could not be addressed due to reporting inconsistencies. Regardless of these limitations, however, this is the largest review on TTS reported till date.
Supplemental Material
sj-docx-1-cath-10.1177_10760296211068487 - Supplemental material for Thrombosis with Thrombocytopenia Syndrome After Administration of AZD1222 or Ad26.COV2.S Vaccine for COVID-19: A Systematic Review
Supplemental material, sj-docx-1-cath-10.1177_10760296211068487 for Thrombosis with Thrombocytopenia Syndrome After Administration of AZD1222 or Ad26.COV2.S Vaccine for COVID-19: A Systematic Review by Usama Waqar, Shaheer Ahmed, Syed M.H.Ali Gardezi, Muhammad Sarmad Tahir, Zain ul Abidin, Ali Hussain, Natasha Ali and Syed Faisal Mahmood in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-xlsx-2-cath-10.1177_10760296211068487 - Supplemental material for Thrombosis with Thrombocytopenia Syndrome After Administration of AZD1222 or Ad26.COV2.S Vaccine for COVID-19: A Systematic Review
Supplemental material, sj-xlsx-2-cath-10.1177_10760296211068487 for Thrombosis with Thrombocytopenia Syndrome After Administration of AZD1222 or Ad26.COV2.S Vaccine for COVID-19: A Systematic Review by Usama Waqar, Shaheer Ahmed, Syed M.H.Ali Gardezi, Muhammad Sarmad Tahir, Zain ul Abidin, Ali Hussain, Natasha Ali and Syed Faisal Mahmood in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Data Sharing Statement
All data relevant to the study are uploaded as Supplemental Material.
Author Contributions
UW and AH conceptualized the study. UW and SA designed the study, drafted protocol, and screened titles and abstracts of retrieved articles. MST and AH performed full-text review of shortlisted studies. UW and SA conducted quality assessment of all included studies. SMG, MST, ZA, and AH retrieved all data from included studies. SMG, MST, and ZA rechecked the complete dataset for accuracy. UW performed all statistical analyses. All authors contributed to interpretation of results. UW, SA, and SMG drafted the initial version of the manuscript which was reviewed and edited by all authors. All authors approved the final version of the manuscript to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.