
Abstract
Severe thrombocytopenia is a serious condition that frequently arises in patients with myelodysplastic syndrome (MDS) and is associated with poor prognosis. Few studies have investigated the prognostic significance of platelet recovery in patients with MDS having thrombocytopenia. We retrospectively analyzed 117 patients with de novo MDS complicated with thrombocytopenia (platelet count [PLT] < 100 × 109/L). Patients received decitabine treatment (schedule A) or decitabine followed by allogeneic hematopoietic stem cell transplantation (allo-HSCT; schedule B). Severe thrombocytopenia (PLT < 20 × 109/L), identified in 31 (26.5%) patients, was associated with poor survival. The PLT increased significantly after decitabine treatment in the 2 groups. Patients with thrombocytopenia treated with schedule B showed a superior prognosis compared to those treated with schedule A. On analysis of overall survival by platelet response in patients with severe thrombocytopenia, a significant survival advantage was observed in patients who achieved a platelet response, who would further benefit from allo-HSCT following decitabine therapy. The results indicate a potentially favorable prognostic impact of platelet response achieved with decitabine. Patients with MDS having severe thrombocytopenia may benefit from the effective recovery of platelets and further allo-HSCT following decitabine therapy.
Keywords
Introduction
The myelodysplastic syndromes (MDSs) comprise heterogeneous clonal myeloid malignancies characterized by peripheral blood cytopenia, ineffective hematopoiesis, recurring cytogenetic and molecular abnormalities, and increased risk of progression to acute myeloid leukemia (AML). 1,2 The pathophysiological causes of this disease include intrinsic genetic abnormalities in myeloid progenitors, altered epigenetics, and extrinsic changes in the bone marrow microenvironment, 3 highlighting the complexity of MDS.
Thrombocytopenia, defined as platelet count (PLT) < 100 × 109/L, is a significant clinical manifestation of MDS, affecting 37% to 67% of patients. 4,5 In a retrospective analysis of 2410 patients, severe thrombocytopenia (PLT < 20 × 109/L) was observed in 415 (17%) patients and moderate thrombocytopenia (PLT: 20-50 × 109/L) was observed in 618 (26%) patients. 4 The mechanisms of thrombocytopenia in MDS remain to be elucidated. Postulated mechanisms include suppression of megakaryocytic differentiation by inhibitory cytokines, enhanced apoptosis, and defective responses to growth factors. 1 In conjunction with abnormal platelet function in MDS, thrombocytopenia contributes to an increased risk of bleeding. Hemorrhagic complications in patients with MDS having thrombocytopenia included minor events (eg, bruising, petechiae) and life-threatening events (eg, gastrointestinal, intracranial hemorrhage). 1 Studies have shown that 40% to 65% of patients with MDS experience hemorrhagic complications due to thrombocytopenia, with these complications being cited as the cause of death in 10% to 20% of MDS cases. 4,6 Thrombocytopenia is also found to be associated with increased risk of transformation to AML. 4,7 –10 Patients with lower risk MDS suffering from severe thrombocytopenia have median overall survival (OS) of 15.4 months, 8 similar to that of patients with International Prognostic Scoring System (IPSS) intermediate 2 risk disease. Thus, thrombocytopenia is an important manifestation of MDS that can influence clinical outcome.
In terms of treatment, 5-aza-2′-deoxycytidine (decitabine) is an inhibitor of DNA methylation with a strong antileukemic effect that has been shown to induce response rates of 45% to 50% in elderly high-risk patients with MDS. 11 Decitabine may induce the differentiation and maturation of myelodysplastic megakaryocytes in patients with MDS. 12 A phase II study showed that 58% of the patients having thrombocytopenia with MDS achieved a platelet response after 1 cycle of decitabine therapy and 69% of the patients showed a response during therapy. 13 In vivo and in vitro, decitabine was shown to increase PLTs by enhancing platelet release and megakaryocyte maturation. 14 In addition, allogeneic hematopoietic stem cell transplantation (allo-HSCT) offers potentially curative treatment for MDS. Even in patients who fail to respond to DNA methyltransferase inhibition, allo-HSCT is associated with better outcomes compared to nontransplant therapies. 15 In this study, we systematically analyzed the clinical outcomes of patients with de novo MDS having thrombocytopenia, who received decitabine and allo-HSCT.
Patients and Methods
We retrospectively reviewed the medical records of patients who were referred to The First Affiliated Hospital of Soochow University from July 2012 to January 2016. All patients included in the study were newly diagnosed with MDS according to the classification from the World Health Organization (WHO), with PLT < 100 × 109/L. Eligibility criteria also included adequate performance status (ECOG score: 0-1) and adequate cardiac and hepatorenal function. Patients were excluded if no data were available on outcome, patient sex, cytogenetic analysis, or PLT or if they had MDS secondary to previous chemotherapy and/or radiotherapy for another malignancy, a history of seizure, or uncontrolled concurrent illness. All procedures were performed in accordance with the Declaration of Helsinki. All patients were followed until death or until August 2017.
Response Criteria and Cytogenetic Evaluation of MDS
Response criteria for complete remission (CR) and partial remission (PR) were identical to the ones used for AML but required response durability for at least 4 weeks. 16 A CR required normalization of the bone marrow and peripheral counts with ≤5% marrow blasts, granulocyte count of ≥1 × 109/L, and PLT ≥100 × 109/L or more, for a duration of ≥4 weeks. A PR was similar to CR (except for persistent marrow blasts >5%) but reduced by ≥50%. A marrow CR referred to the reduction of marrow blasts to ≤5% without normalization of peripheral counts. Cytogenetic categories were categorized as good, intermediate, or poor, according to IPSS.
Treatment
Patients either received decitabine treatment (schedule A) or decitabine followed by allo-HSCT (schedule B). Decitabine (20 mg/m2) was given intravenously daily for 5 days. Patients on schedule B received a standard regimen for prophylaxis of graft-versus-host disease and infectious complications. Graft-versus-host disease prophylaxis consisted of cyclosporin A (CSA) and methotrexate (MTX) in patients who received transplants from matched related donors; all others received antithymocyte globulin and mycophenolate mofetil together with CSA and MTX. In cases of severe bleeding, fresh apheresis platelets were regularly infused in patients with PLT <20 × 109/L. Fresh frozen plasma was administered to patients with moderate to severe bleeding.
Evaluation of Platelet Recovery
Response to therapy was evaluated during 4 to 6 weeks after decitabine administration, before the next cycle of treatment. 17 A “major response” was defined as an absolute increase of ≥30 × 109/L in patients with a pretreatment PLT <100 × 109/L. For platelet transfusion-dependent patients, a “major response” required stabilization of the PLT and platelet transfusion independence. A “minor response” was defined as a ≥50% increase in PLT with a net increase of 10 to 30 × 109/L, in patients with a pretreatment PLT <100 × 109/L. All other patients were considered to show “no response.”
Statistical Analysis
The significance of individual factors was analyzed by standard univariate analysis. Survival was calculated from the date of referral to our institution. Overall survival was defined as the time from initial diagnosis until death from any cause or until the last follow-up. The Kaplan-Meier method was used to estimate survival-type distributions. The 2-sided log-rank test was used to compare treatment outcomes. Cox proportional hazards model was used to determine independent prognostic importance of several factors and to obtain hazard ratio (HR) estimates and the corresponding 95% confidence interval (CI). SPSS version 17 (IBM Company, Chicago, Illinois) was used for statistical analyses. Differences were considered statistically significant at P < .05.
Results
During the period from July 2012 to January 2016, 117 patients from The First Affiliated Hospital of Soochow University were enrolled in this study (schedule A, N = 55; schedule B, N = 62). Patient characteristics are presented in Table 1. Groups were matched for sex, age, ECOG score, WHO subtype, IPSS, IPSS-R, decitabine course, and number of patients with severe thrombocytopenia. The study included 79 males and 38 females. Median age for the entire cohort was 42 years (range, 7-75 years). Patients were classified according to the WHO classification as RCMD (21, 17.9%), refractory anemia with excess blasts 1 (RAEB-1, 35, 29.9%), RAEB-2 (55, 47.0%), MDS-U (5, 4.3%), or MDS/MPN (1, 0.9%). Median PLT was 36 × 109/L (range, 4-99 × 109/L). Severe thrombocytopenia (PLT < 20 × 109/L) was observed in 31 (26.5%) patients. Median hemoglobin level was 73 g/L (range, 30-142 g/L). The median neutrophil count was 1.87 × 109/L (range, 0.01-34.7 × 109/L).
Patient Demographics and Clinical Characteristics.
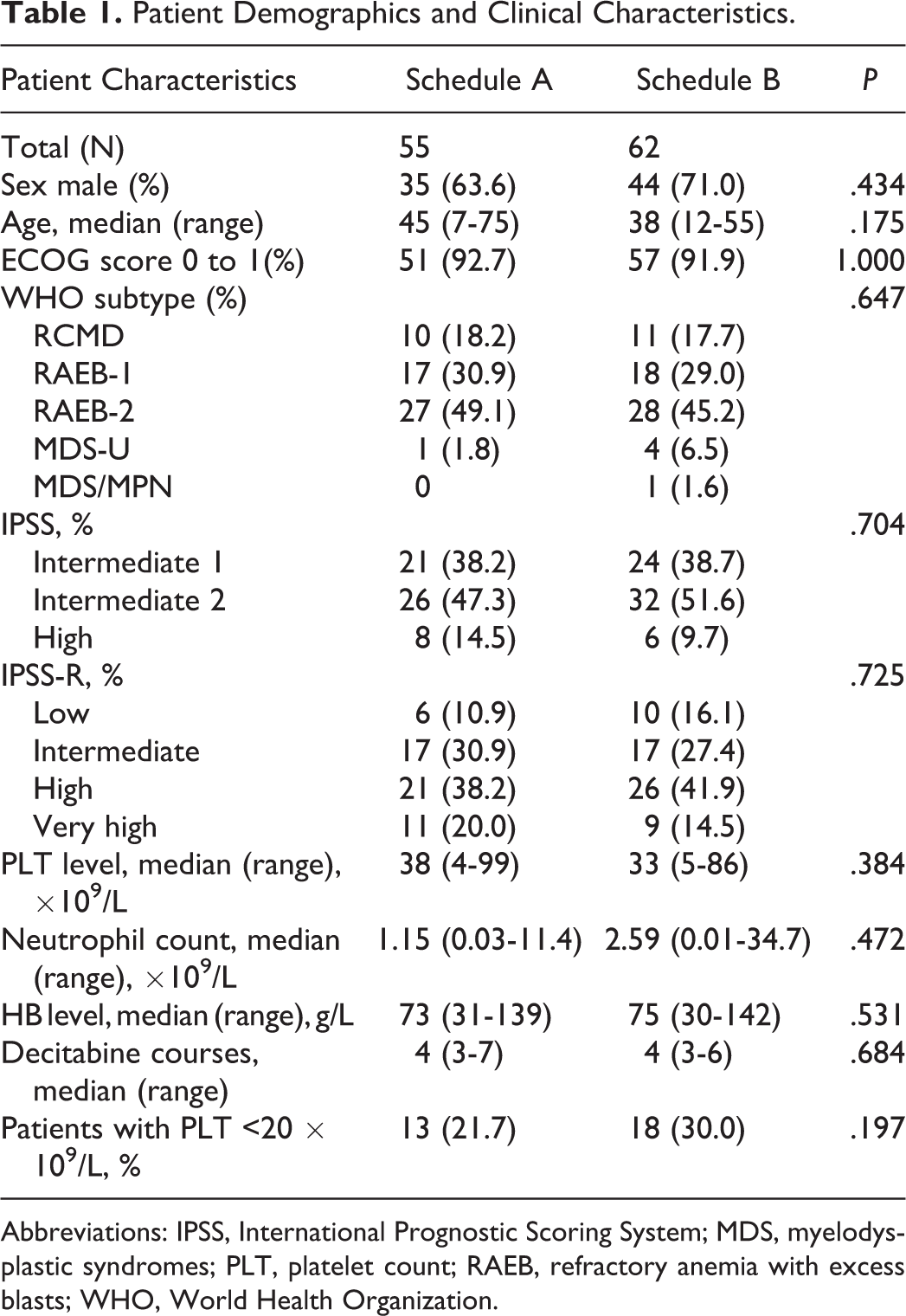
Abbreviations: IPSS, International Prognostic Scoring System; MDS, myelodysplastic syndromes; PLT, platelet count; RAEB, refractory anemia with excess blasts; WHO, World Health Organization.
The results of cytogenetic analysis were classified according to the IPSS score as good (normal, Y, del[5q], del[20q]), poor (chromosome 7 anomalies, complex [≥3 abnormalities]), or intermediate (all other aberrations). In terms of IPSS score, 45 (38.5%) patients were intermediate 1 risk, 58 (49.6%) patients were intermediate 2 risk, and 14 (12.0%) patients were high risk. Patients were categorized by IPSS-R risk as low risk (16, 13.7%), intermediate risk (34, 29.1%), high risk (47, 40.2%), or very high risk (20, 17.1%). Thrombocytopenia was significantly associated with poor performance status, higher IPSS-R risk, increased blast percentages, poor cytogenetics, and advanced MDS phase.
Response and Outcome
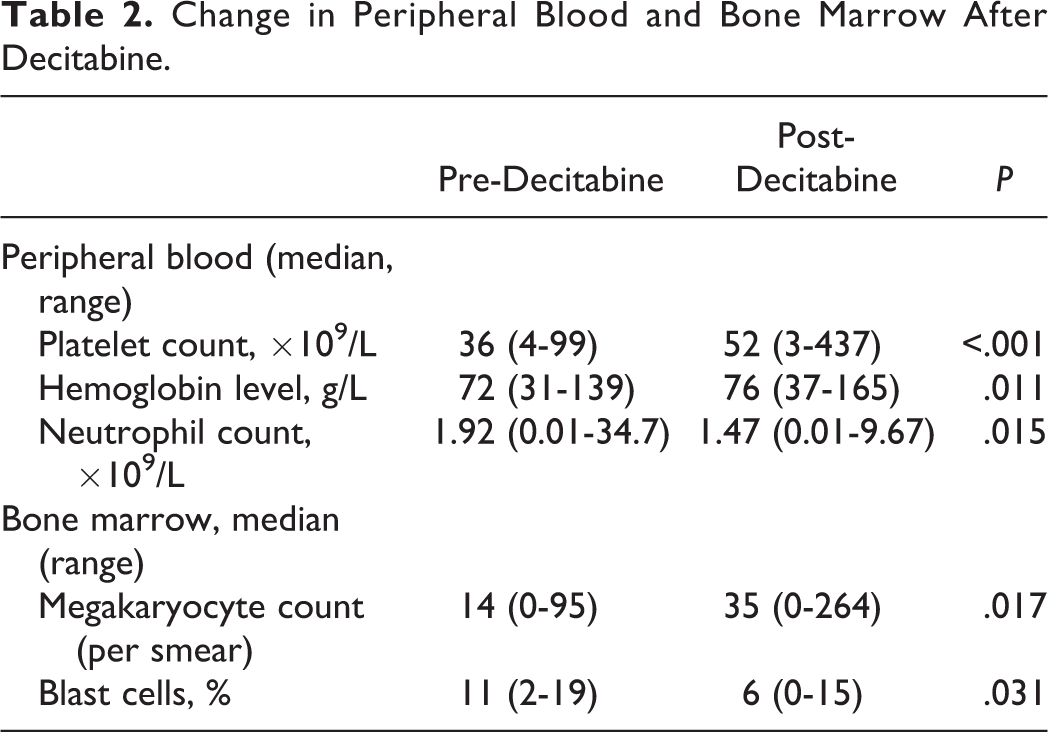
The median number of decitabine courses administered was 4 courses (range, 3-7 courses). In both groups, PLTs increased significantly after decitabine treatment (P < .001; Table 2). A major response was achieved in 74 (63.2%) of the patients with thrombocytopenia who received decitabine; minor response was observed in 18 (15.4%) patients. In both groups, decitabine treatment resulted in higher hemoglobin level (P = .011) and lower neutrophil count (P = .015). Recovery of hemoglobin was achieved in 40.7% of patients; neutrophil recovery was observed in 27.8%. Bone marrow morphological analysis revealed low levels of megakaryocytes before treatment, with a significant increase after decitabine treatment (Table 2).
Change in Peripheral Blood and Bone Marrow After Decitabine.
Overall Survival
A significant survival advantage was achieved in patients with a PLT of 20 to 100 × 109/L compared to those with severe thrombocytopenia (PLT < 20 × 109/L; median OS, 42 vs 11 months, respectively; HR, 2.21; 95% CI, 1.25-3.89; log-rank P = .004; Figure 1A). Patients with thrombocytopenia (PLT < 100 × 109/L) in schedule B showed superior prognosis (median OS, 17 months vs not reached, respectively; HR, 0.41; 95% CI, 0.22-0.76; log-rank P = .003; Figure 1B). Similar results were found in patients with a PLT of 20 to 100 × 109/L (median OS, 22 months vs not reached, respectively; HR, 0.42; 95% CI, 0.19-0.92; log-rank P = .023; Figure 1C). For patients with severe thrombocytopenia, there was no difference in OS between 2 groups (median OS, 19 months vs not reached, respectively; HR, 0.55; 95% CI, 0.23-1.34; log-rank P = .172; Figure 1D).
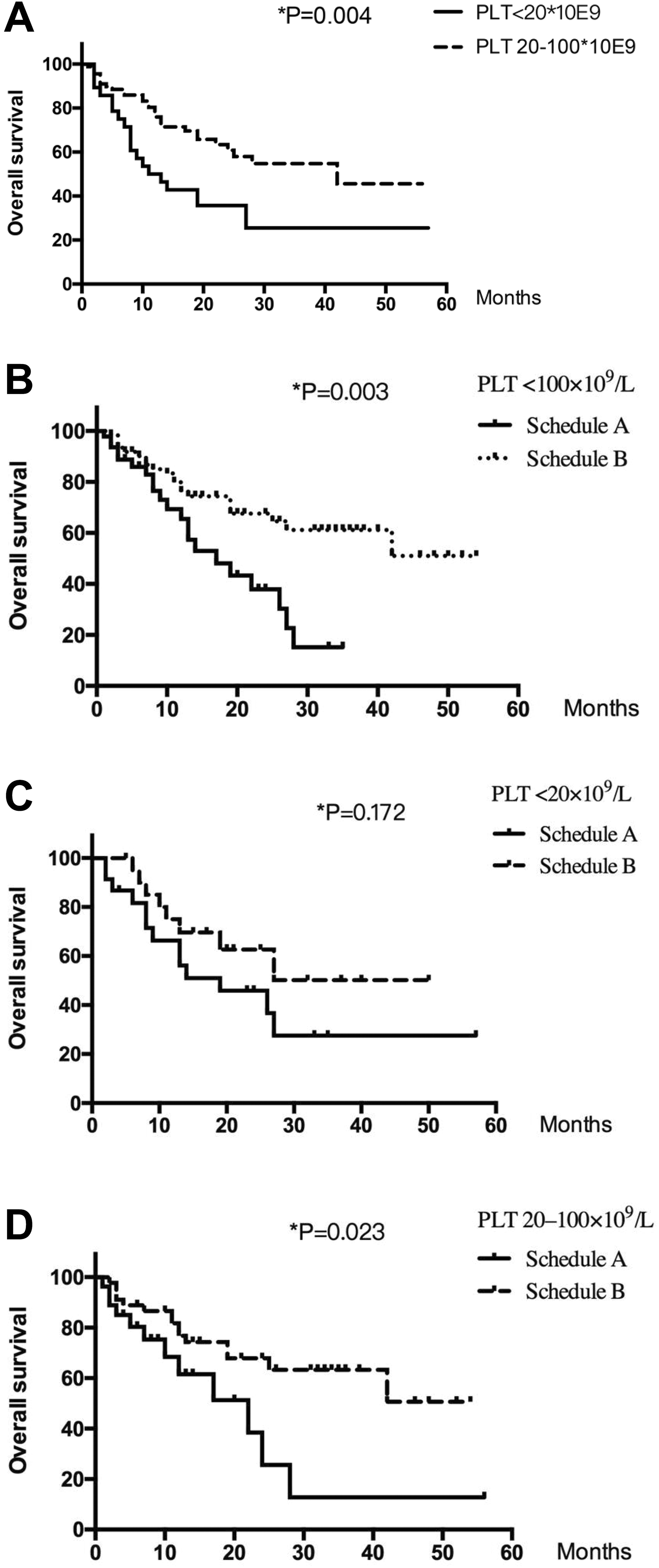
Analyses of overall survival according to platelet count (PLT) and study arm. (A) Survival by PLT; (B) survival by study arm for PLT <100 × 109/L; (C) survival by study arm for PLT <20 × 109/L; and (D) survival by study arm for PLT from 20 to 100 × 109/L.
No significant difference in OS was observed among patients with thrombocytopenia (PLT < 100 × 109/L) who did or did not achieve a platelet response after decitabine treatment (median OS, 27 vs 25 months, respectively; HR, 1.59; 95% CI, 0.86-2.94; log-rank P = .135; Figure 2A). On analysis of OS by platelet response in patients with severe thrombocytopenia (PLT < 20 × 109/L), a significant survival advantage was observed in patients who achieved platelet response, with a median OS of 27 months in patients who showed a platelet response compared to 10 months in patients who did not respond (P = .029; Figure 2B). We further analyzed OS in the different groups of patients with severe thrombocytopenia who showed a platelet response, and a more favorable outcome was achieved with schedule B than with schedule A (median OS, 42 vs 22 months, respectively; HR, 0.48; 95% CI, 0.24-0.97; log-rank P = .033; Figure 2C). There was no significant difference for those without platelet response between the 2 groups (median OS, not reached vs 10 months, respectively; HR, 2.07; 95% CI, 0.69-6.22; log-rank P = .184; Figure 2D).
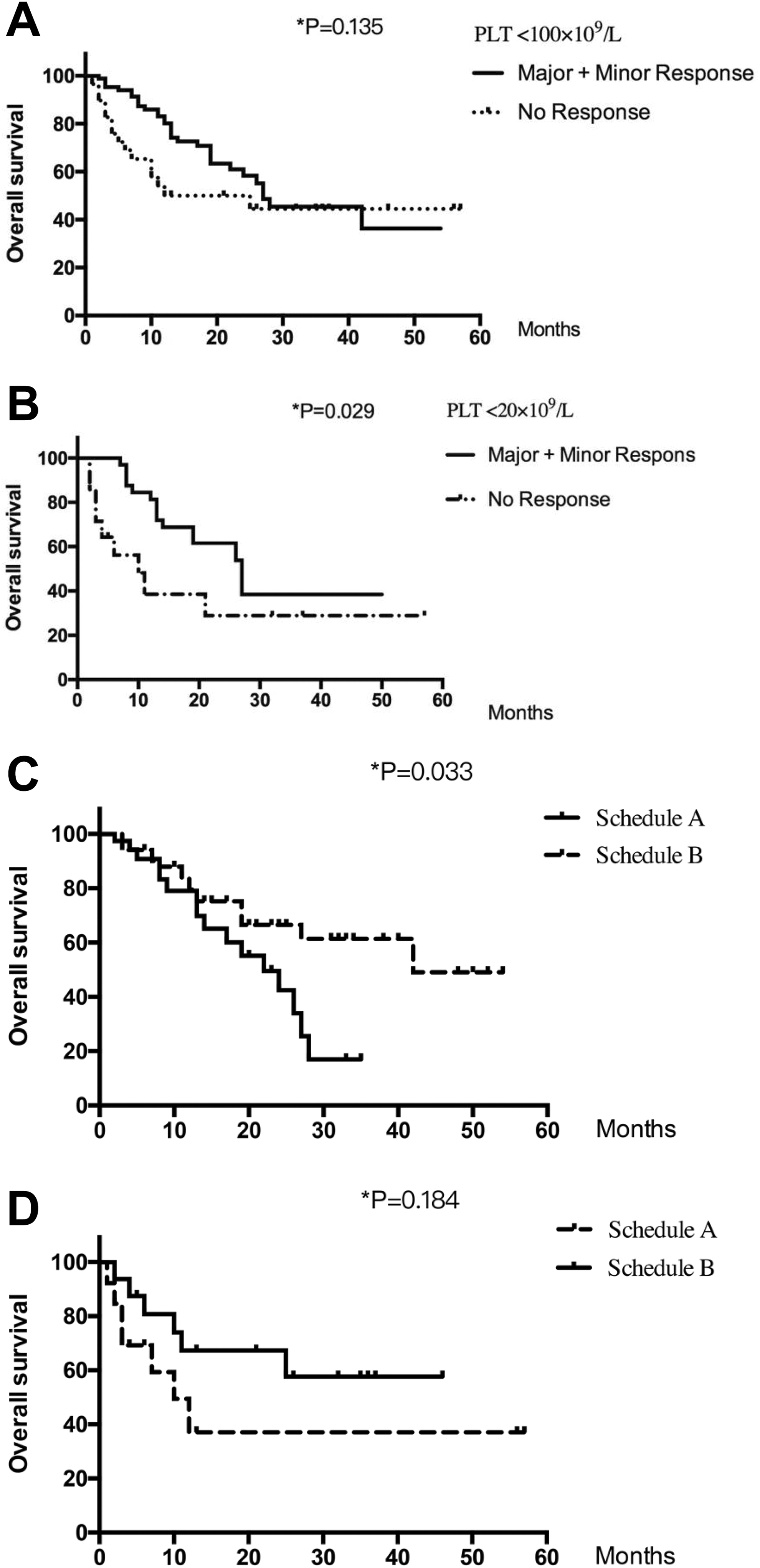
Analyses of overall survival according to study arm and platelet recovery. (A) Survival by platelet recovery for platelet count (PLT) <100 × 109/L; (B) survival by platelet recovery for PLT <20 × 109/L; (C) survival by study arm for various degrees of platelet recovery; and (D) survival by study arm for patients without platelet recovery.
Univariate analysis of prognostic factors for OS revealed the following adverse prognostic factors (P < .05): severe thrombocytopenia, neutrophil count <0.5 × 109/L, hemoglobin <60 g/L, very high-risk IPSS-R subtype, poor cytogenetics, and non-HSCT. For multivariate analyses, all parameters with prognostic significance in the univariate analyses were included in a multivariate Cox logistic regression procedure. Severe thrombocytopenia and 4 other variables retained their independent prognostic influence: hemoglobin <60 g/L, very-high-risk IPSS-R subtype, poor cytogenetics, and non-HSCT (Table 3).
Cox Univariate and Multivariate Analyses of Overall Survival.
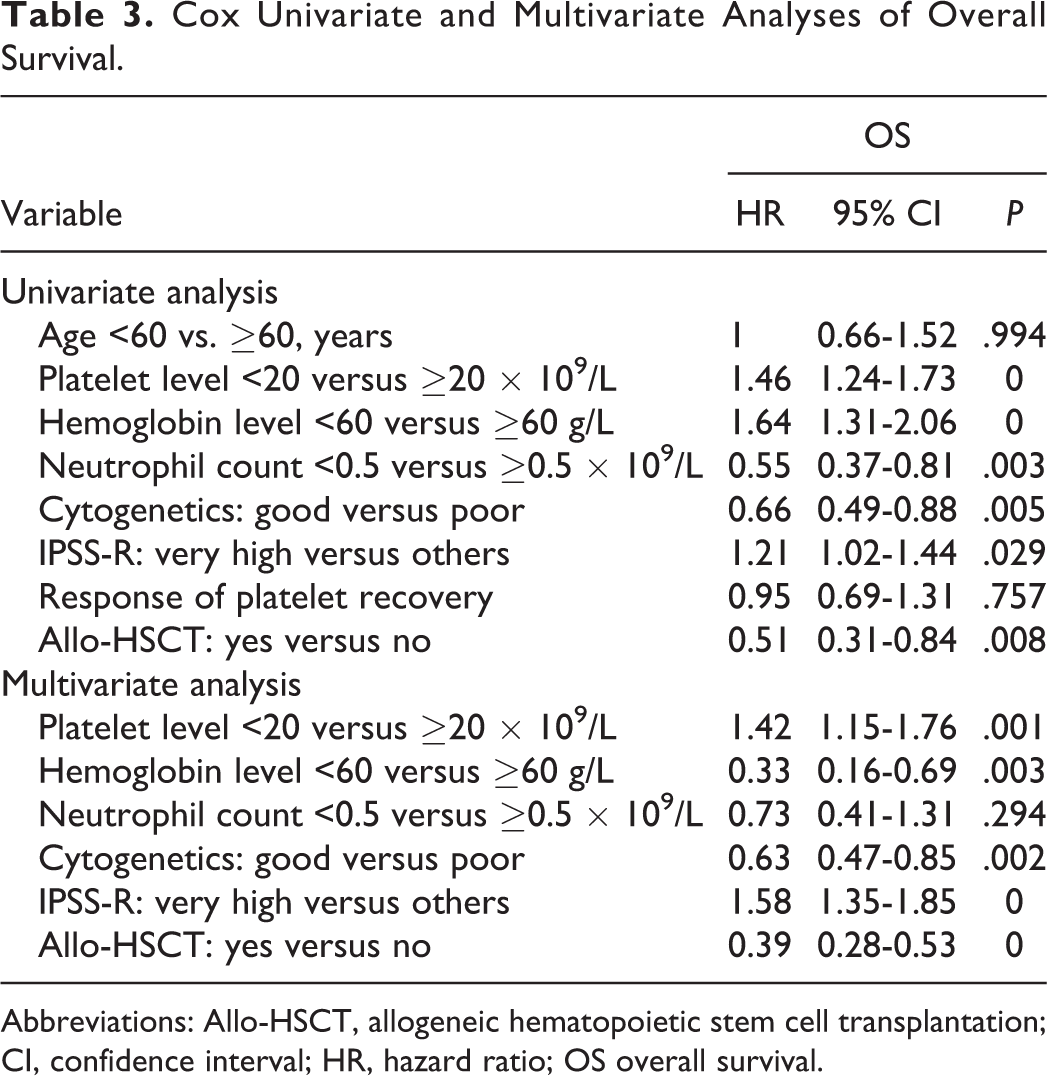
Abbreviations: Allo-HSCT, allogeneic hematopoietic stem cell transplantation; CI, confidence interval; HR, hazard ratio; OS overall survival.
Discussion
In this study, thrombocytopenia showed significant independent prognostic value in predicting OS in patients with MDS after adjustment for known predictors. However, thrombocytopenia was deemphasized as a manifestation of MDS at diagnosis and during the course of disease. 5 Two or more cytopenias translated into a score of only 0.5 in IPSS risk evaluation, which does not reflect the significance of thrombocytopenia. IPSS-R for MDS was modified to incorporate the degree of thrombocytopenia as an independent factor predicting poor prognosis.
Decitabine has changed the clinical course of MDS by improving the hematologic response and survival rate. 18,19 Given that decitabine treatment is limited in terms of eradicating MDS clones, allo-HSCT is shown to be the only curative treatment approach for patients with MDS. As reported previously, allo-HSCT appeared to increase long-term OS among patients with thrombocytopenia who participated in the study. However, this advantage was not maintained in patients with severe thrombocytopenia. We assumed that the limited number of cases may have contributed to the results, but the poor prognosis showed no improvement even with allo-HSCT.
We further focused on the prognostic significance of platelet recovery in MDS with severe thrombocytopenia, and a significant survival advantage was observed in patients who achieved platelet response. The results showed the platelet level improvement with decitabine, which may serve as a potentially good marker to assess the prognosis. Further analysis of the 2 groups showed that patients with a platelet response would benefit from allo-HSCT following decitabine. For those without a platelet response, no significant difference in OS was observed between the 2 groups, indicating that the dismal prognosis could not be improved even by allo-HSCT.
We report significant efficacy of decitabine in platelet recovery in MDS, with a major response rate of 62.5% and a minor response rate of 15.8%. Our findings are comparable to previous results: 67% of low- or intermediate-risk patients with MDS achieved RBC and platelet independence. 20 When decitabine was administered to patients with MDS at much higher doses (40-50 mg/m2 per day for 3 days), platelet response was observed in 69% of patients with thrombocytopenia. 13 Compared to the studies above, this study involved the administration of a lower dose of decitabine (20 mg/m2 for 3 consecutive days) and enrolled more high-risk patients with MDS. The observed effects of myelosuppression were relatively mild. Response rates were comparable between studies. Furthermore, 1 patient with platelet recovery and 2 without platelet recovery experienced transformation to AML during the study period. Due to the limited number of cases, conclusions regarding the effect of decitabine on the rate of transformation to AML cannot be reached at present.
Conclusion
Our study showed the effective recovery of platelets in patients with MDS having severe thrombocytopenia after decitabine treatment, with improved survival when patients with platelet recovery also received allo-HSCT. The findings provide initial data demonstrating the potential prognostic value of platelet response achieved with decitabine in guiding clinical decisions in MDS. This study has several limitations, including the absence of records documenting patients’ molecular abnormalities. Further study will be necessary to elucidate the mechanism of platelet recovery in patients with MDS.
Footnotes
Author Contribution
Yaqiong Tang and Xinyou Zhang contributed equally to this study and are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (grant no. 81270591, 81470346, and 81670132), Jiangsu Province of China (BE2016665 and BK20150356), Jiangsu Provincial Special Program of Medical Science (BL2012005), and Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).