
Abstract
Atrial fibrillation (AF) is a well-known cause for thromboembolism. Although blood stasis in the left atrium and hypercoagulable state of the blood have been emphasized as important mechanisms, limited attention has been paid to the endocardial changes in maintaining the balance of local coagulation, which may also contribute to the thrombus formation in AF. In the present study, left atrial appendage samples were obtained at heart surgery from nonvalvular AF and non-AF patients without atrial thrombus. Immunohistochemistry for endocardial markers including thrombomodulin (TM) and tissue factor pathway inhibitor (TFPI) was performed and semiquantitatively graded. In immunohistochemistry analysis, decreased expression of TM was found in patients with nonvalvular AF compared with those without AF (P < .001). There was no difference in TFPI expression between the 2 groups (P = .213). Patients with TM score of 0 or 1 seemed to have larger left atrial diameter (LAD) than those with TM score of 2 or 3 (44.0 (7.9) vs 40.6 (3.9); P = .009), while no relationship between LAD and TFPI expression was found (43.4 (7.0) vs 42.9 (7.8); P = .485). In conclusion, TM expression in the atrial endocardium is decreased in nonvalvular AF without atrial thrombus, while TFPI expression is not. Downregulated TM expression might be associated with enlarged LAD.
Introduction
Atrial fibrillation (AF) is the most commonly sustained cardiac arrhythmia and the most important risk factor for cardioembolic stroke. 1 The left atrium (LA), particularly the left atrial appendage (LAA), is the most frequent location of the embolic thrombi. 2 Intracardiac thrombus formation during AF may result from Virchow’s triad of endothelial damage, stagnant blood flow, and a hypercoagulable state. Although decreased blood flow through the atrial appendage 3,4 and activation of coagulation 5,6 have been demonstrated before in patients with AF, there were limited studies about endocardial changes in these patients.
Previous studies suggested that AF could induce acute deficiency in the endocardial expression of anticoagulant factors, such as thrombomodulin (TM) and tissue factor pathway inhibitor (TFPI). 7,8 However, endocardial changes in nonvalvular AF without atrial thrombus are still unclear. The present study was designed to explore the expression levels of TM and TFPI in the LAA endocardium in nonvalvular AF without atrial thrombus.
Methods
Patients and LAA Sampling
From February 2015 to April 2016, 53 patients with nonvalvular AF underwent modified endoscopic ablation at our center. Only 1 (1.9%) patient had LAA thrombus and was excluded. The other 52 (98.1%) patients were all included in our study. The surgical technique was described before. 9 Overall, the procedure was performed through 3 ports around the subscapular angle line of the left chest wall. The pericardium was opened about 10 mm anterior to the descending aorta. The bilateral pulmonary veins and the posterior LA were exposed after the suspension of the pericardium. Bilateral pulmonary vein isolation was performed using AtriCure Isolator Synergy ablation clamp (AtriCure, Inc., West Chester, OH). A circumferential left atrial ablation was made using the clamp from the left inferior pulmonary vein to the right superior pulmonary vein. The LAA was excised using the EZ 45 stapler (Ethicon Endosurgery, Cincinnati, OH) or Endo GIA (Covidien, Minneapolis, MN) and was collected for analysis. Other linear lesions, including from the left pulmonary vein to the incision of LAA and from the left inferior pulmonary vein to the mitral valve annulus, were made using the AtriCure Synergy ablation pen (AtriCure, Inc). The ligament of Marshall was divided and the ablation of ganglionic plexi on the posterior LA was performed.
In control group, LAAs were obtained at other heart surgery (coronary artery bypass grafting) from patients without AF. None of these patients had atrial thrombus. To exclude the possible effects of anticoagulants on endocardial markers, patients receiving any anticoagulation therapy were not included in the present study. Other exclusion criteria were blood coagulative disease, neoplasia, hepatic pathologies, acute and chronic inflammatory diseases, and thyroid dysfunction. This study was approved by the institutional review board and individual consents were obtained.
Immunohistochemistry
Tissues obtained from the LAA were fixed in buffered 10% formalin, processed overnight, and embedded in paraffin wax. Three-micrometer sections were cut from tissues and were deparaffinized and rehydrated prior to staining. Antigen retrieval was performed. Sections were placed in a pressure cooker containing Tris/EDTA buffer (ProteinTech, Wuhan, China) of pH = 6 (both TM and TFPI) and the pressure cooker was heated. Sections were incubated serially with the following solutions: (1) 3% hydrogen peroxide for 25 minutes to block endogenous peroxidase activity, (2) 0.3% Triton-X 100 for 15 minutes to permeabilize the membrane, (3) 10% normal goat serum for 60 minutes to reduce nonspecific binding of the antiserum, (4) primary antisera for 16 hours at 4°C (antibody dilution 1:100 for TM and TFPI [ProteinTech]), and (5) horseradish peroxidase–labeled goat anti-mouse immunoglobulin G (Dako, Glostrup, Denmark) at a dilution of 1:1 for 50 minutes. Immunoreactive sites were visualized by incubation with 0.025% 3,3-diaminobenzidine and 0.01% hydrogen peroxide for 3 minutes. Phosphate-buffered saline (pH 7.4) was used to dilute each solution and to wash the sections 3 times between each step. Finally, sections were counterstained with hematoxylin.
Slides were photographed together in a single run with the same illumination and exposure time on the light microscope. Tissues were examined independently by 2 board-certified pathologists. Each slide was scored as having no staining, weak focal staining, multifocal moderate staining, or diffuse strong staining, giving a score of 0, 1, 2, or 3, respectively. All factors were assessed on endothelium. Investigators who performed staining and scoring were blinded to the AF status. If the scores provided by 2 pathologists were not the same, the slide would be referred to a third pathologist, whose score would be final. Figures 1 to 4 show typical results of the staining of endocardial tissue for the intensity of TM and TFPI.
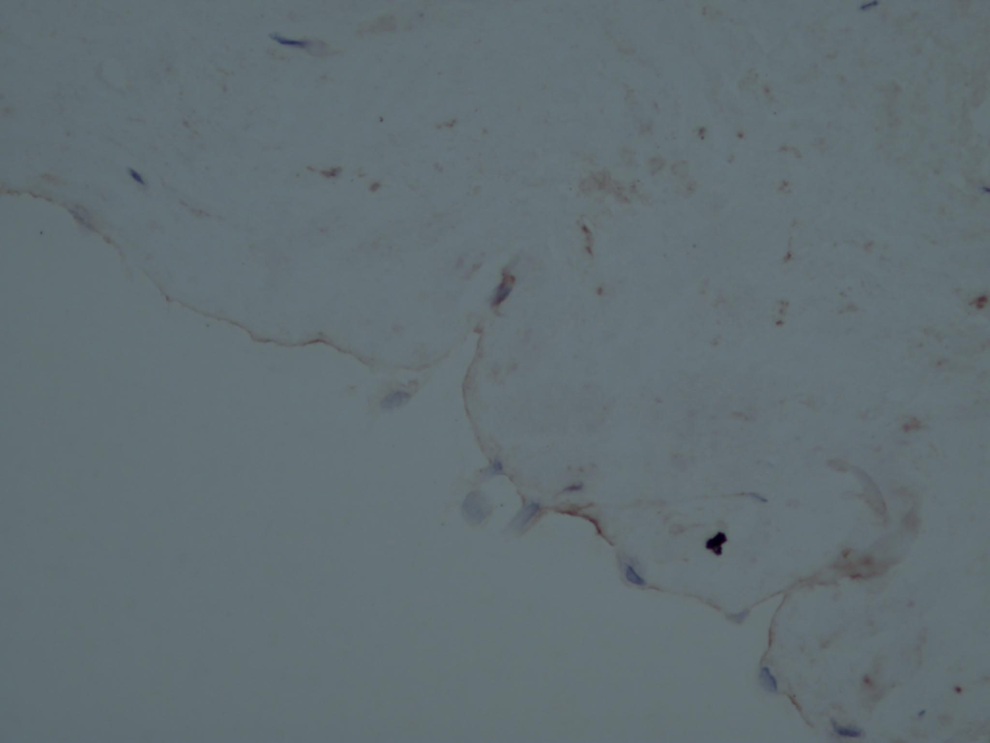
Typical TM staining intensity (score 0) of a section of the left atrial appendage. TM indicates thrombomodulin.
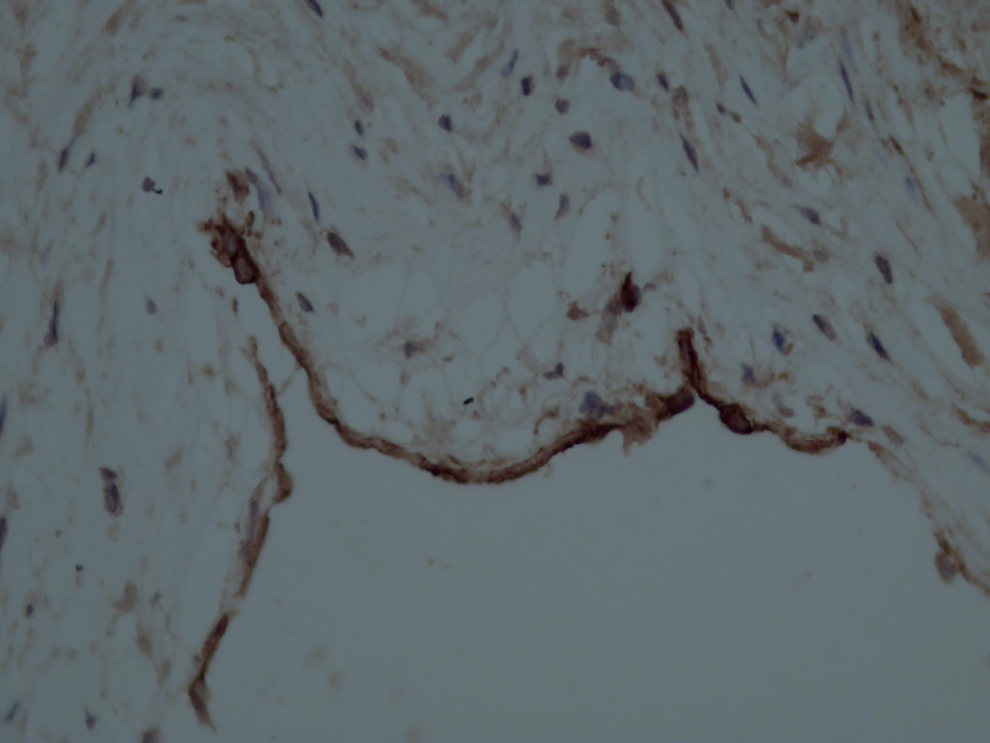
Typical TM staining intensity (score 3) of a section of the left atrial appendage. TM indicates thrombomodulin.
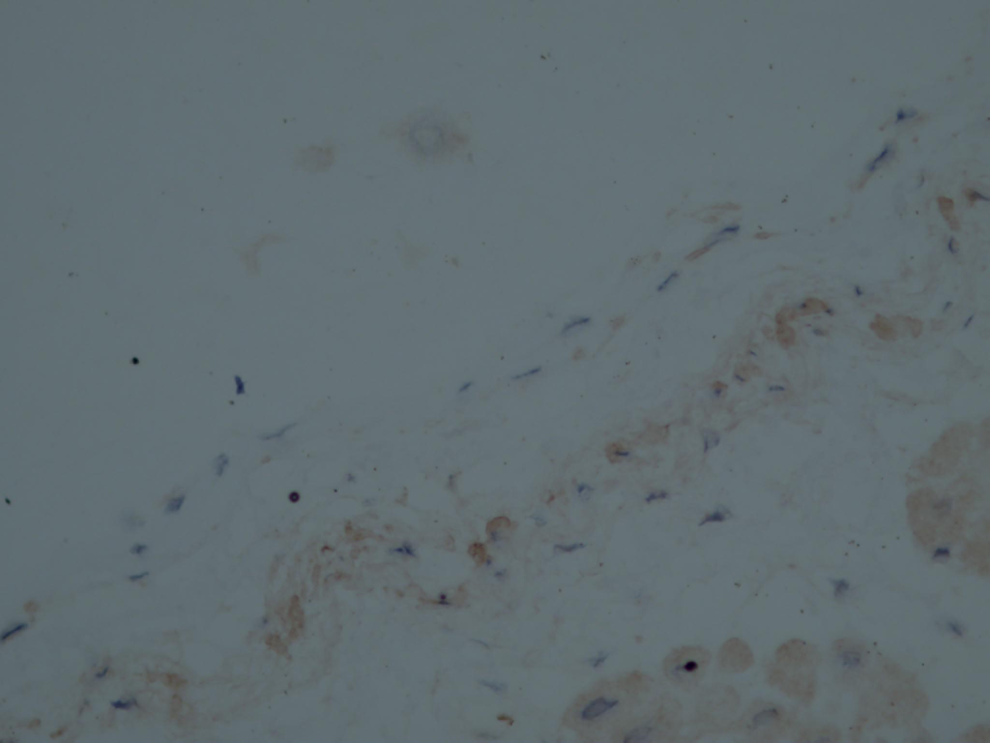
Typical TFPI staining intensity (score 0) of a section of the left atrial appendage. TFPI indicates tissue factor pathway inhibitor.
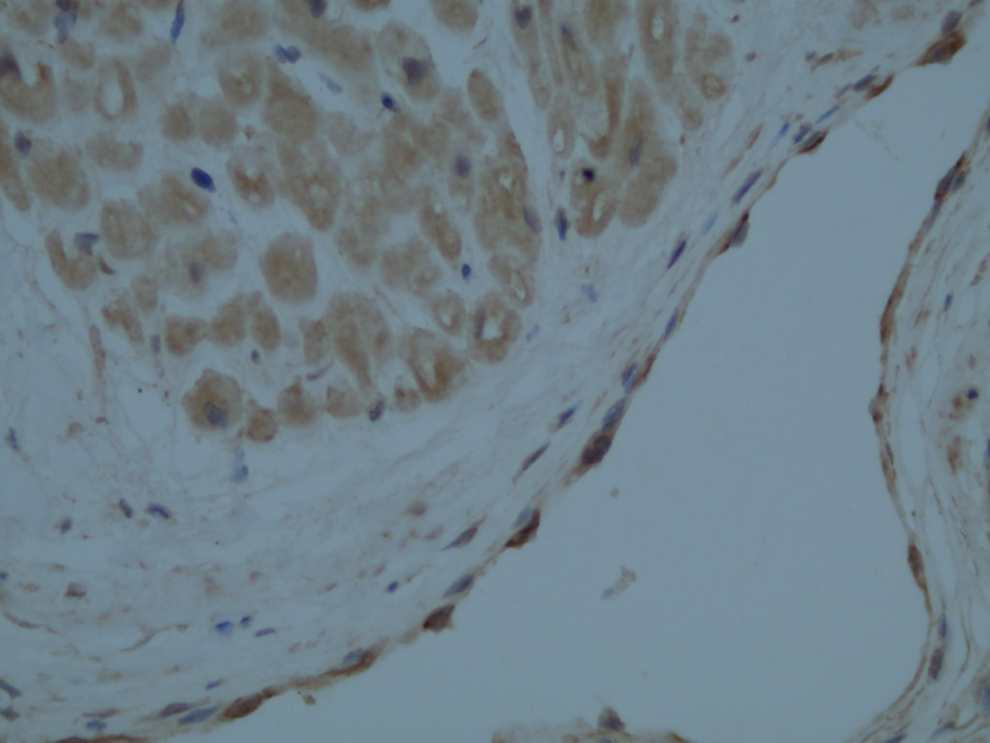
Typical TFPI staining intensity (score 3) of a section of the left atrial appendage. TFPI indicates tissue factor pathway inhibitor.
Statistical Analysis
Continuous variables were expressed as means (standard deviations) unless otherwise specified, and categorical data were expressed as counts and proportions. Normally distributed continuous variables were compared by using t test, while abnormally distributed continuous variables were compared by using nonparametric tests. The χ2 test was used for categorical variables. Statistical analyses were performed using the Statistical Package for Social Sciences, version 18.0 (SPSS, Chicago, Illinois).
Results
Baseline characteristics of patients are presented in Table 1. The nonparoxysmal AF included persistent AF and long-standing persistent AF. Patients who developed AF seemed to have larger LAD than those without AF (43.2 (7.3) vs 36.7 (3.1); P = .001).
Baseline Characteristics of Patients.a
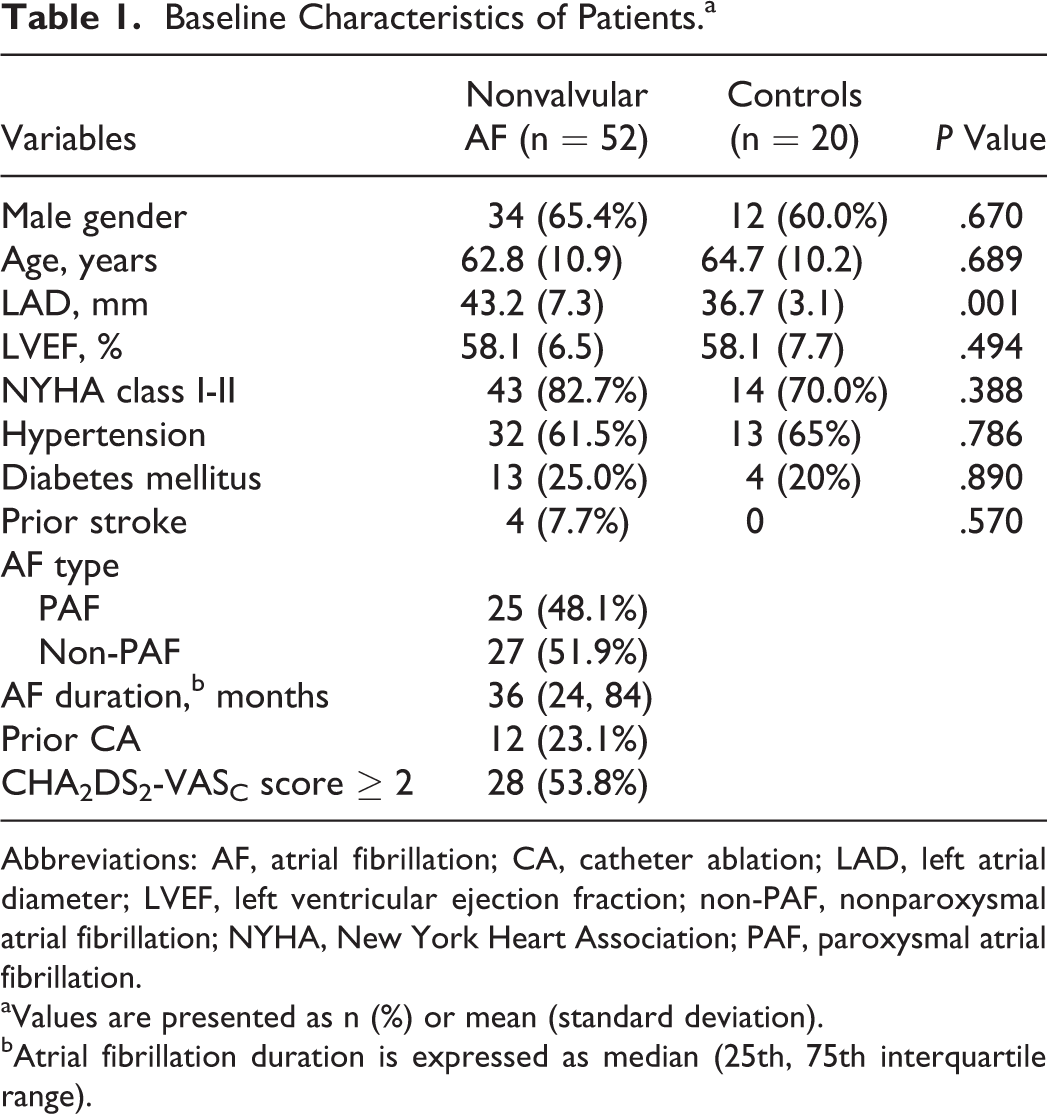
Abbreviations: AF, atrial fibrillation; CA, catheter ablation; LAD, left atrial diameter; LVEF, left ventricular ejection fraction; non-PAF, nonparoxysmal atrial fibrillation; NYHA, New York Heart Association; PAF, paroxysmal atrial fibrillation.
aValues are presented as n (%) or mean (standard deviation).
bAtrial fibrillation duration is expressed as median (25th, 75th interquartile range).
Table 2 shows the atrial endocardial expression of TM and TFPI between patients with nonvalvular AF and controls. Decreased expression of TM was found in nonvalvular patients with AF compared with those without AF (P < .001). There was no difference in TFPI expression between the 2 groups (P = .213).
Tissue Expression of TFPI and TM by LAA in Patients With and Without AF.
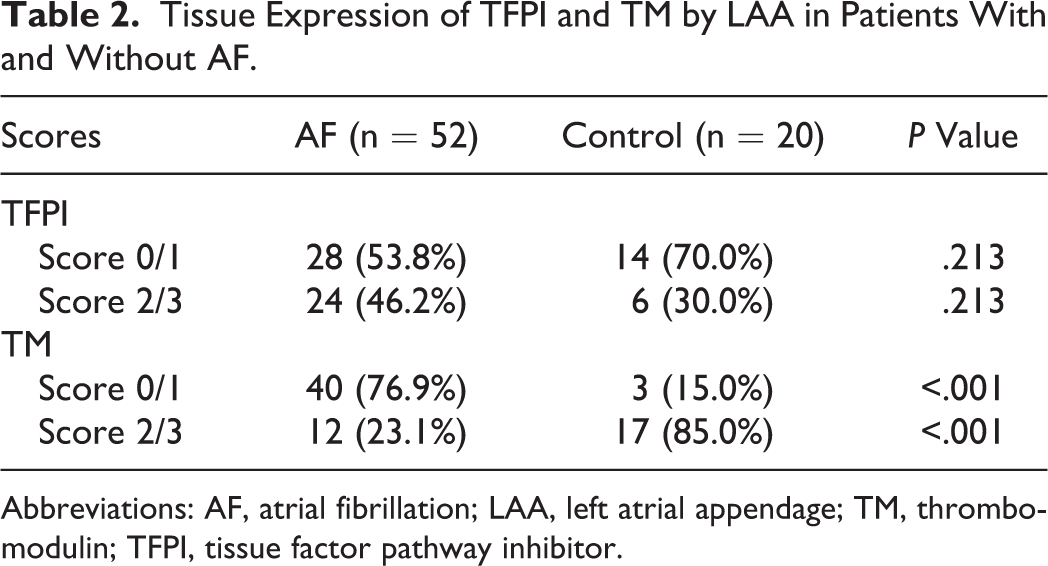
Abbreviations: AF, atrial fibrillation; LAA, left atrial appendage; TM, thrombomodulin; TFPI, tissue factor pathway inhibitor.
To identify the association between left atrial diameter (LAD) and endocardial expression of TM/TFPI, we divided patients with nonvalvular AF according to the staining score. Patients with TM score of 0 or 1 seemed to have larger LAD than those with TM score of 2 or 3 (44.0 (7.9) vs 40.6 (3.9); P = .009), while no relationship between LAD and TFPI expression was found (43.4 (7.0) vs 42.9 (7.8); P = .485; Figure 5).
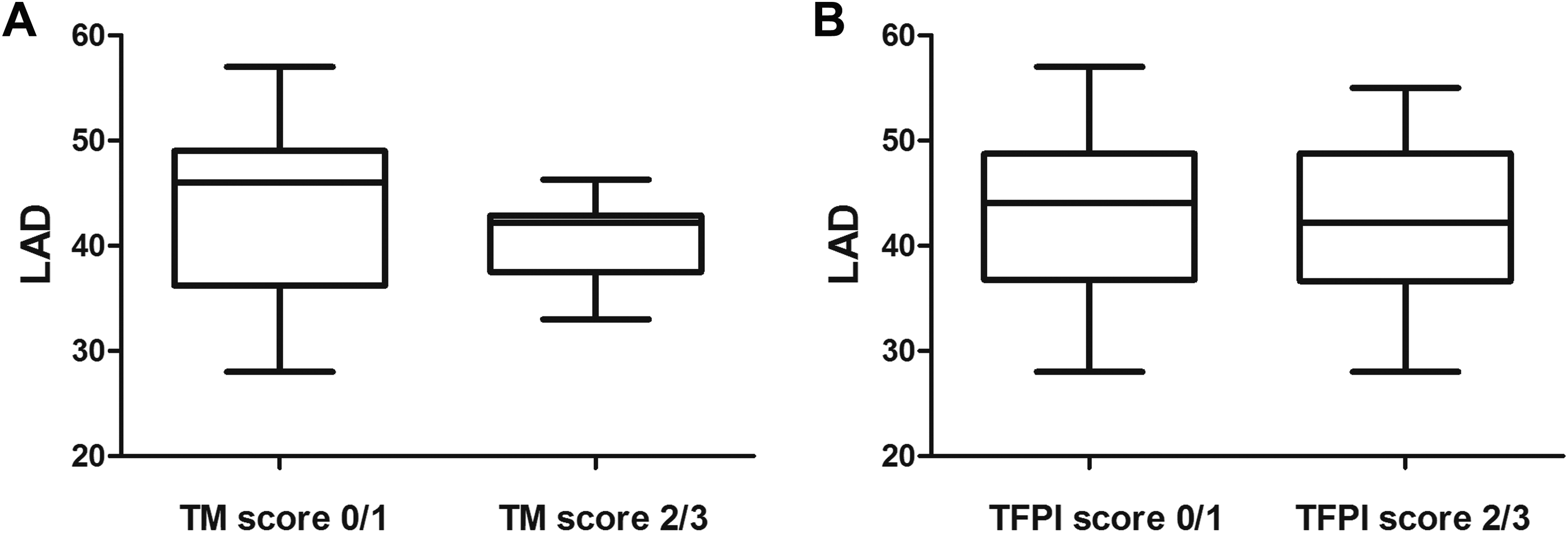
A, Comparison of LAD between TM score of 0/1 and 2/3 among patients with nonvalvular AF (P = .009). B, Comparison of LAD between TFPI score of 0/1 and 2/3 among patients with nonvalvular AF (P = .485). LAD indicates left atrial diameter; TM, thrombomodulin; TFPI, tissue factor pathway inhibitor.
Discussion
Atrial fibrillation predisposes to the development of atrial thrombi, most commonly in the LAA, which is the dominant source of embolism in AF. Approximately 90% of atrial thrombi in nonvalvular AF are seen within the LAA. 10 Although decreased laminar flow and hypercoagulable state of the blood have been emphasized as important mechanisms, there were limited reports about the role of endocardial changes in the atrial thrombi formation. During normal sinus rhythm, the atrial endocardium should act as an anticoagulant barrier. 11 In patients with AF, this barrier might be stripped, 7 followed by the increased expression of prothrombotic molecules. 12 These changes may contribute to the risk of thrombus formation in patients with AF.
Thrombomodulin is a pivotal determinant of normal coagulation balance. Endothelial TM forms a complex with thrombin and changes its substrate specificity as an intrinsic thrombin inhibitor. Thrombin bound to TM cannot activate protein C, which has a potent anticoagulant effect. 13 However, reports about TM expression in the atrial endocardium of patients with AF are rare. In our study, 85% of non-AF patients had intense staining of TM (score of 2 or 3) and immunohistochemistry analysis showed fully TM-covered LAA endocardium. On the other hand, only 23.1% of patients with AF had expression score of 2 or 3 and immunohistochemistry analysis suggested the TM barrier was stripped. This may in part explain the fact that LAA is susceptible to thrombus formation in patients with AF. The downregulation of TM might be multifactorial. Yamashita et al 7 created paroxysmal AF model in anesthetized rats and found that rapid atrial pacing acutely downregulated the expression of TM in the LA endocardium at the genetic level. Besides, previous studies also suggested that TM could be released from the endocardium as a soluble particle. 13,14 In patients with AF, fibrillating atrium might increase the release of TM from the endocardium, causing increased circulating TM levels and decreased endocardial expression. 7
Although studies about endocardial expression of TM are rare, TM expression in other sites has been reported before. Gosling et al 15 found that the endothelial expression of TM in human saphenous vein was significantly decreased under arterial flow. They concluded that increased shear stress is associated with decreased TM expression. However, Sperry et al 16 found through animal experiments that pressure-induced stretch and distension, rather than shear stress changes, play an important role in TM expression in saphenous vein. Considering the fact that the intra-atrial shear stress of blood flow is relatively low in patients with AF, 17 we hypothesized that increased intra-atrial pressure and atrial distension in AF might explain the endocardial changes of TM. In our study, patients with TM score of 0 or 1 seemed to have larger LAD than those with TM score of 2 or 3 (P = .009). Left atrium size is thought to represent left ventricular (LV) diastolic function in patients without significant mitral valve disease. 18,19 Left ventricular diastolic dysfunction leads to a reduction in passive LA emptying, with the development of increased atrial pressures during diastole and enhanced LA contraction during systole as compensation. 20 These stretching and distension may participate in the endocardial expression of TM, besides the initiation and progression of AF.
Tissue factor pathway inhibitor is another important intrinsic anticoagulant between the blood and the vasculature cells. 13,14 Tissue factor pathway inhibitor regulates the initial step of the extrinsic coagulation pathway mediated by tissue factor (TF). In a factor Xa-dependent feedback system, TFPI binds directly and inhibits the factor VIIa-TF complex. 14 Like TM, reports about TFPI expression in the human atrial endocardium are also limited. In our study, there is no difference in the endocardial expression of TFPI between AF and non-AF patients (P = .213) nor is the TFPI expression associated with the LAD (P = .485). Interestingly, only 30.0% of non-AF patients had TFPI score of 2 or 3. Our result is actually supported by the findings of Nakamura et al, 8 who also found TFPI was not significantly upregulated in the atrial endocardium of patients with nonvalvular AF compared with those without AF. Their results also showed that of 4 normal controls (non-AF patients), only 2 patients had a TFPI expression score of 2 or more. On the other hand, Yamashita et al 7 reported that gene expression of TFPI is downregulated in rapid-pacing LA endocardium in the rat model, which is opposite to our findings. Thus, further studies are needed to identify the TFPI expression and its role in patients with AF.
Left atrial diameter is the most common method to quantify LA size, although recent studies demonstrated that LA size is better measured by volume rather than diameter. 21 In nonvalvular AF, enlarged LAD can be explained by various mechanisms, such as LV diastolic dysfunction (followed by atrial stretch and distention), 20 atrial fibrosis, and remodeling. 22 Our study only demonstrated possible association between LAD and TM expression, but the mechanism remains unclear. This is one of the limitations of our study. Increased intra-atrial pressure and distention caused by LV diastolic dysfunction might be one possible explanation, as mentioned above. Recent studies also showed that atrial myocytes and fibroblasts were able to secrete certain factors (eg, transforming growth factor) that altered endocardial expression of TM, 23,24 suggesting atrial fibrosis might play a role in the endocardial changes. Further molecular and biological investigations are required to understand a more detailed mechanism. Besides, studies with larger sample size are still needed to confirm our findings.
In conclusion, TM expression in the atrial endocardium is decreased in nonvalvular AF without atrial thrombus, while TFPI expression is not. Downregulated TM expression might be associated with enlarged LAD.
Footnotes
Acknowledgments
The authors thank Saie Shen, MD, Ms Huihua Chen, and Ms Yu Su for their excellent experimental and clinical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Commission of Shanghai Municipality (grants 13XD1403200 and 11441900200) and the Xinhua Hospital (grant 13YJ29).