
Abstract
Warfarin treatment requires regular and proper monitoring to avoid overanticoagulation and at the same time to prevent thromboembolic complications. This study assessed the quality of warfarin anticoagulation at Princess Marina Hospital in Botswana. This cross-sectional study consecutively enrolled patients who were on warfarin for at least 3 months in the outpatient medical clinic. The level of anticoagulation was determined by the time in therapeutic range (TTR) using the Rosendaal method that calculates the percentage of days when the international normalized ratio is in the therapeutic range (2.0-3.0). Poor anticoagulation control was defined as an estimated TTR <65%. We performed univariate and multivariate logistic regression to assess predictors of poor anticoagulation control. Of total, 410 (68.8% women) patients whose median age was 46 (interquartile range [IQR], 35-58) years were enrolled. Indications for warfarin included mechanical heart valves, 185 (45.1%); deep vein thrombosis, 114 (26.8%); and atrial fibrillation, 68 (17.8%). Of the 2004 tests (an average of 4.9 tests per patient) assessed, only 20% of the tests were within the therapeutic range. The median TTR was 30.8% (IQR, 15.2-52.7). Most (85.1%) patients had poor anticoagulation control. Cigarette smoking and pulmonary hypertension perfectly predicted poor anticoagulation. Hypertension was a predictor of poor anticoagulation control (adjusted odds ratio = 2.24; 95% confidence interval: 1.02-4.94). The quality of anticoagulant therapy with warfarin in Botswana patients is poor. The evidence calls for efforts to improve the level of anticoagulation control among patients on warfarin in Botswana.
Background
Warfarin is the most common oral anticoagulant used in clinical practice. 1,2 Because of its narrow therapeutic window, multiple drug interactions, and individual variability in dose response, the management of warfarin therapy is often challenging. 3 Close monitoring through systematic international normalized ratio (INR) measurement minimizes the risk of bleeding while maximizing protection against thromboembolic events. 4,5 The therapeutic INR recommended for most warfarin indications is 2.0 to 3.0, a level of anticoagulation that has been shown to protect patients from blood clots while minimizing the risk of hemorrhage attributable to excessive anticoagulation. 5 –7 The percentage of time in therapeutic range (TTR) summarizes INR control over time. 5,8 A TTR above 65% has been reported to be beneficial against stroke and vascular events among patients on warfarin. 9,10 On the other hand, TTRs of less than 40% are not associated with any significant mortality benefit. 10
A substantial proportion of warfarin-treated patients has remained suboptimally anticoagulated. 7,11 –13 The level of anticoagulation control varies with many factors including study setting, frequency of INR monitoring, and variant alleles of the CYP2C9 and VKORC1 genes among patients. 5,7,11,14,15 Variations in the VKORC1 and CYP2C9 genes across races–ethnic groups partly contribute to differences in warfarin dose requirement, sensitivity to warfarin, and the quality of anticoagulation. 16 The proportion of patients with optimal anticoagulation control varies with setting from as low as 0% in developing countries to about 49.4% in developed countries. 9,13
Because of diligent laboratory monitoring and timely warfarin dose adjustments, clinical trials have been reporting better anticoagulation control than in routine community practices. 7 Novel oral anticoagulants (NOACs) have similar efficacy and safety to warfarin in patients with venous thromboembolism and atrial fibrillation (AF). 9,17 As frequent laboratory monitoring and dose adjustments are not required with NOACs, they may be more convenient alternatives to warfarin in routine clinical settings and particularly when anticoagulation control with warfarin is suboptimal. 9,17,18 Unfortunately, NOACs are associated with an increased risk of thromboembolic and bleeding events among patients with mechanical heart valves. 19 Warfarin is, therefore, the only anticoagulation option in patients with mechanical heart valves. Rheumatic heart disease (RHD) has the highest prevalence in sub-Saharan Africa and continues to be one of major causes of cardiovascular morbidity and mortality among young people in this region. 20 –22 Some patients with RHD undergo valve replacement often at a relatively young age. 20,21 Patients with mechanical heart valves and those who develop pulmonary hypertension, AF, and stroke as a sequela of RHD need long-term anticoagulation with warfarin. 20,21 Even though warfarin is the most common anticoagulant in the Botswana, there is no published information on the level of anticoagulation control. In this study, we sought to assess the quality of anticoagulation control (expressed as TTR) among patients on warfarin at Princess Marina Hospital medical outpatient clinics in Gaborone Botswana.
Methods
Patients and Setting
This was a cross-sectional study conducted at Princess Marina Hospital, Botswana’s largest tertiary and referral hospital. As there is no specialized anticoagulation clinic at Princess Marina Hospital, patients who are on warfarin are usually seen in the general medical clinics. Most patients with prosthetic valves are seen at the cardiac clinic. Patient clinic visits are at least once in every 4 to 8 weeks or more as needed for patients with labile INR values. Changes of warfarin dosages are made accordingly to achieve therapeutic INR ranges.
All patients on warfarin between October 2014 and October 2016 were eligible for enrollment. Male and female patients with varying indications for warfarin on treatment for at least 30 days and with a minimum of 4 INR values recorded were included. A study research nurse obtained written informed consent from eligible patients willing to participate in the study. The research assistant administered a questionnaire to all consenting patients and reviewed respective medical records. The questionnaire aimed to capture demographic information, clinical conditions, and indications for warfarin anticoagulation.
We determined the level of anticoagulation measured by the TTR using the Rosendaal method, which calculates the percentage of days when the INR values are in the therapeutic range (2.0-3.0). 8 The TTR was calculated for each patient as the number of person-days with an INR of 2.0 to 3.0 divided by the total number of person-days on warfarin. The method uses INR values from patients with at least 2 valid intervals separated by 56 days (8 weeks) or less, without an intervening hospitalization. Individual patient TTRs were used to calculate the overall TTR for the hospital. A poor anticoagulation control was defined as an estimated TTR <65%. 9
Statistical Analysis
We analyzed the data using SPSS version 23.0 for Windows (SPSS Inc., Chicago, Illinois). We present the medians with interquartile ranges (IQRs) for continuous variables and counts (percentage) to describe categorical variables (indications for warfarin, smoking, alcohol intake, age, sex, TTR control categories, and comorbid conditions). We performed univariate logistic regression and multivariate logistic regression to determine the predictors of poor anticoagulation control. In the regression, sex, age, stroke, diabetes, and HIV infection were a priori decided as potential confounders, and any other variables with P < .20 were included in the final model. Smoking and pulmonary hypertension were perfect predictors of poor coagulation and therefore not included in the final model. We report the crude and adjusted odds ratios. We considered a P value of <.05 as statistically significant.
Ethical Consideration
The study was approved by the institutional review boards of the University of Botswana, Ministry of Health and Princess Marina Hospital Institutional Review Boards (PMH 5/79[101]). Before data collection, informed consent was obtained from all individual participants included in the study.
Results
The study included 410 patients, whose median age was 46 (IQR, 35-58) years (Table 1). Two hundred and eight-two (68.8%) participants were females. The most common indications for warfarin were mechanical heart valves, deep vein thrombosis (DVT), and AF. The median weekly dose of warfarin was 35 (IQR, 35-52.5) mg, consistent in all indications. The most common comorbidities were HIV infection, hypertension, and prior history of stroke/transient ischemic attack (TIA). Patients with DVT were more likely to be HIV-infected than those with other indications (48.2% vs 16.9%, P < .001). Smoking and alcohol intake was reported in 21 (5.1%) and 24 (5.9%) patients, respectively.
Clinical and Demographic Characteristics of Patients on Warfarin at Princess Marina Hospital in Botswana.
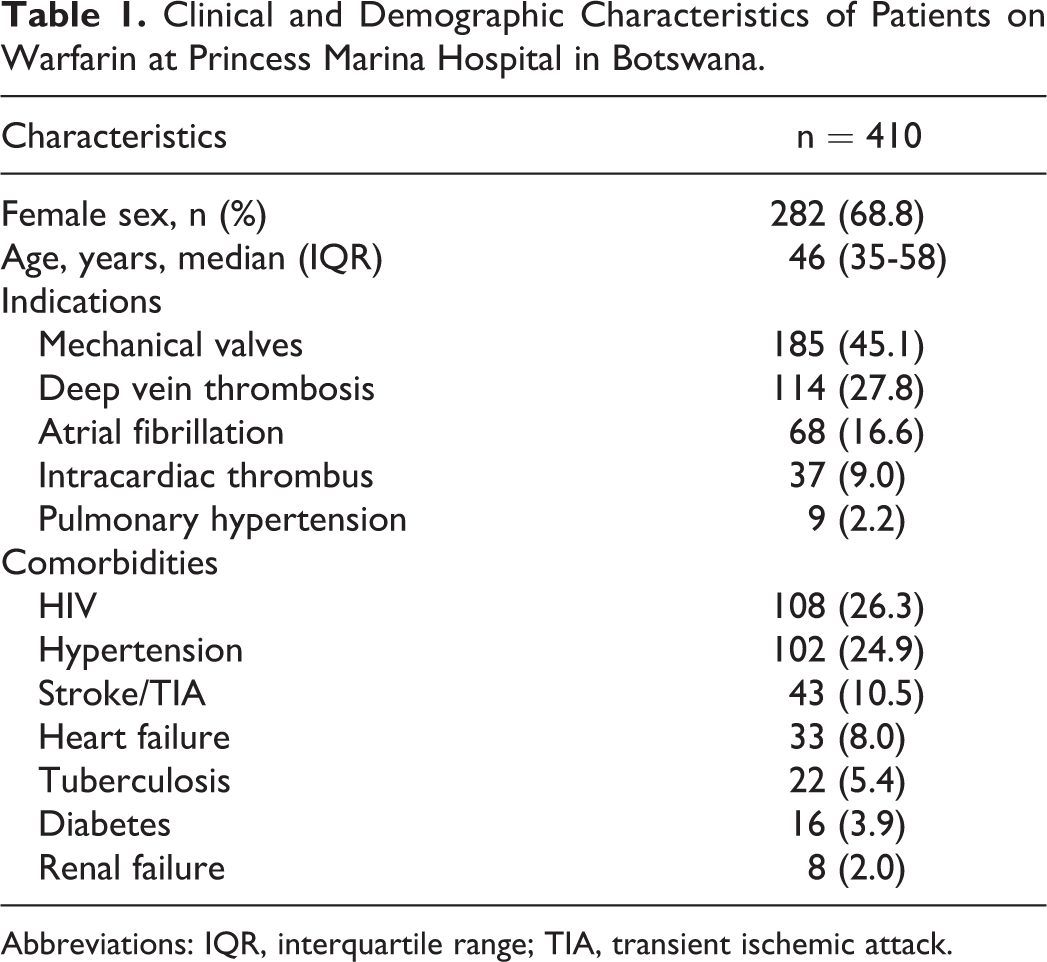
Abbreviations: IQR, interquartile range; TIA, transient ischemic attack.
Table 2 describes INR control among patients with different indications for warfarin. A total of 2004 INR values were assessed over a median duration of 126.0 (IQR, 89.8-167.3) days per patient. Each patient had a mean of 4.9 (standard deviation 0.4) INR results assessed and the median percentage of tests in therapeutic ranges was 20% (IQR, 0-40).The median TTR was 30.8% (IQR, 15.2-52.7). Sixty-one (14.9%) patients had TTR in the therapeutic range while 254 (61.9%) patients had TTR below 40%. The percentage of poor anticoagulation control was therefore 85.1%.
International Normalized Ratio Control of Patients on Warfarin at Princess Marina Hospital in Botswana.
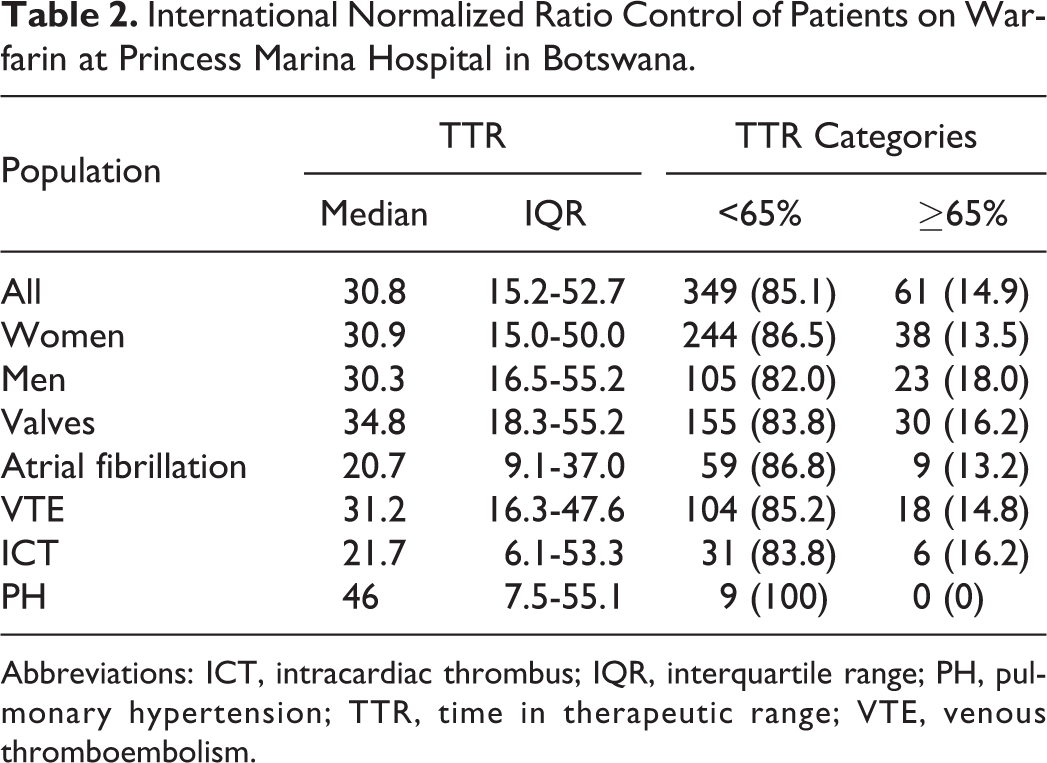
Abbreviations: ICT, intracardiac thrombus; IQR, interquartile range; PH, pulmonary hypertension; TTR, time in therapeutic range; VTE, venous thromboembolism.
Poor anticoagulation control was not associated with gender, age, alcohol consumption, or indications for warfarin (Table 3). Cigarette smoking was observed in 6.0% of the patients with poor anticoagulation control and none in well-controlled patients.
Predictors of Poor Anticoagulation Control Amongst Patients on Warfarin at Princess Marina Hospital in Botswana (n = 410).
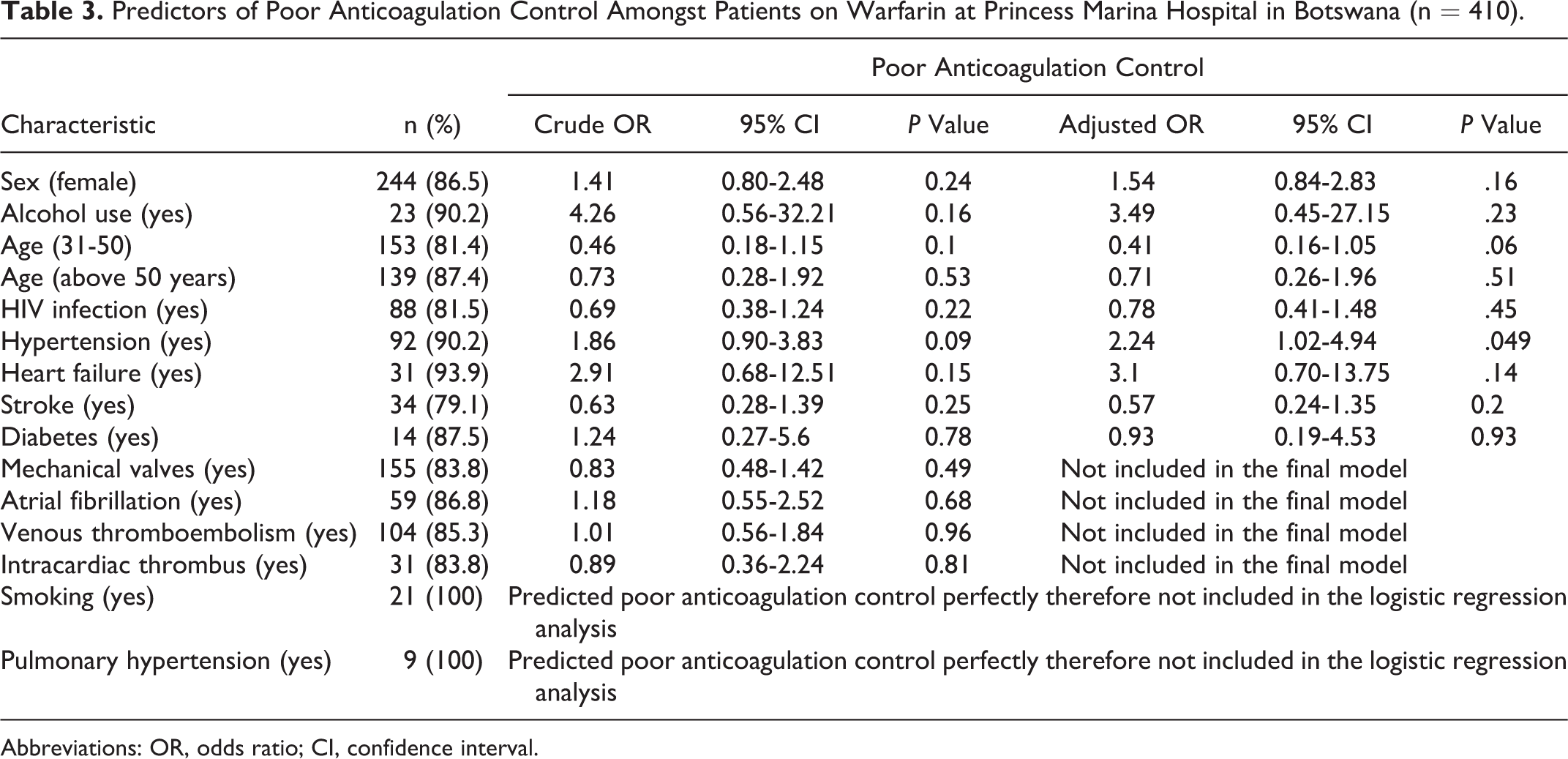
Abbreviations: OR, odds ratio; CI, confidence interval.
Discussion
Warfarin is the only available anticoagulant for patients in public health facilities in Botswana. To the best of our knowledge, this is the first study measuring anticoagulation control among patients on warfarin in Botswana. We found that patients on warfarin anticoagulation were within the therapeutic time in about 30.8% of the time and about 85.1% patients had poor anticoagulation control. Anticoagulation control did not vary with patients’ age, gender, indications, or weekly dosage of warfarin. As poor anticoagulation control has a strong association with worse outcomes, these findings have important implications for patients on long-term warfarin anticoagulation. 9,10
The level of anticoagulation control varies with many factors including study setting, frequency of INR monitoring, and variant alleles of the CYP2C9 and VKORC1 genes among patients. 5,7,11,14,15 The low TTR in our patients is comparable to findings from routine clinical practice settings but poorer than reports from clinical trials and specialized anticoagulation clinics. 9,12,23,24 Consistent with our findings, the mean TTR reported in the Global Anticoagulation Registry in the FIELD-atrial fibrillation (GARFIELD-AF Registry) for patients on warfarin in routine practice in India was 31.1%. 24 Similarly, Sarawate et al observed a mean TTR of 28.6% in patients without chronic valvular AF hospitalized in community practice in the United States. 12 In another study in Ethiopia, a comparable low TTR (29%) was reported among warfarin-treated patients. 25 Infrequent INR monitoring partly explains the poor anticoagulation control in these settings. 26
The TTR obtained in the present study was, however, lower than reports from specialized anticoagulation clinics in Africa. 9,23 Manji et al in Kenya reported a mean TTR of 64.6% in an anticoagulation clinic in Eldoret. 23 Similarly, the mean TTR (46.3%) reported from specialized clinics in South Africa was better than the level in our hospital. 9 Due to close monitoring of INR and timely dose adjustments, specialized anticoagulation clinics and clinical trials have consistently shown better anticoagulation control than routine practices. 7 Lack of a specialized anticoagulation clinic at Princess Marina Hospital may partly explain the poor anticoagulation control because of infrequent INR monitoring. There is strong evidence that anticoagulation control level improves with frequent INR monitoring. 26 Monthly monitoring of INR has been shown to keep about 50% to 60% of patients in therapeutic range. The level of anticoagulation control further improves to 77% to 85% and 92% if INR is monitored weekly and every 3 days, respectively. 26 With few health facilities that can offer INR testing in Botswana, patients travel long distances and as a result spend long time off work and incur extra cost to access centralized anticoagulation services. Frequent INR would, therefore, require decentralization of the anticoagulation services in the country.
In the present study, 85.1% of our patients had poor anticoagulation control. This high proportion of patients with poor anticoagulation control level is consistent with previous reports from South Africa and Asia where the proportions were 100% and 83.3%, respectively. 9,13 Although TTR does not provide information about over- or underanticoagulation, there is evidence that warfarin-treated patients who lie outside the therapeutic INR range are more likely underanticoagulated than overanticoagulated. 7 Given that the rates of stroke, systemic embolism, and all-cause death are higher in patients who are underanticoagulated, it is likely that our patients succumb to these complications. 13 Except for patients with mechanical heart valves, some of these patients could benefit from NOACs instead of warfarin use. 17,19,27 Unfortunately, these drugs are not only more expensive than warfarin but also not readily available in the public setting in Botswana.
Our patients had several comorbid conditions such as HIV, hypertension, diabetes mellitus, heart failure, and prior history of stroke or TIA. The presence of these comorbidities has been associated with poor anticoagulation control and an increased risk of stroke, even in patients without AF. 28,29,30 Interactions between warfarin and medications used for these comorbid conditions have been reported to affect warfarin levels and consequently anticoagulation control. 3,30 As expected, hypertension was the most common comorbid condition in our exclusively black population. 31 Consistent with previous reports, being hypertensive was associated with poor anticoagulation control. 30 In contrast, the presence of other comorbidities was not associated with poor anticoagulation control. 29 The median age of our population was lower than reported in other studies of patients on warfarin. 7 This may partly explain the lower burden of age-dependent comorbidities. 3,7
The most common indication for warfarin treatment among our study participants was mechanical heart valves. This observation is not surprising because sub-Saharan Africa has the highest prevalence of RHD. 21 Patients with RHD would not only undergo valve replacement at a relatively young age but may also develop pulmonary hypertension and AF that require lifelong anticoagulation. 20 Thus, majority of warfarin-treated patients are young and most indications for anticogulation are related to RHD. 20 This is in contrast to situation in developed countries where warfarin-treated patients are old and the commonest indication is nonvalvular AF. 7 Nevertheless, despite of the young age of our patients, the overall mortality, hospitalization, and stroke rates for patients with valvular AF are similar to the rates in the patients without valvular AF. 32 Another common indication for warfarin anticoagulation among our patients was DVT. This may be explained by the high prevalence of HIV among our study participants. The incidence of venous thrombosis is reported to be 2- to 10-fold higher in HIV-infected individuals than in HIV-negative individuals of the same age. 33 HIV infection is associated with a decrease in anticoagulants such as antithrombin III, protein S, and protein C and an increase in procoagulants particularly the endothelial tissue expression and thrombogenic properties of microparticles. 33
There were a small number of cigarette smokers and those who reported of any alcohol intake in our population. Current cigarette smokers were more likely to have poor anticoagulation control than nonsmokers. Although our sample size is small, our observation is consistent with previous studies which reported the negative influence of smoking on the quality of warfarin anticoagulation. 34 Smoking has been reported to enhance the clearance of warfarin and consequently reducing its anticoagulation effect. 35,36 Therefore, patients should be counselled on smoking cessation once on warfarin anticoagulation. 36 Patients reporting alcohol use were at 4-fold odds of poor coagulation even though this was not statistically significant. Our sample size was, however, small with insufficient power. Alcohol is reported to increase metabolism of warfarin by inducing hepatic microsomal enzymes. 37
Study Limitations
Being a cross-sectional study, the time intervals for which the anticoagulation levels were assessed may not be a true reflection of what happens all the time. Using TTR, we were also unable to provide information about over- or underanticoagulation. Nevertheless, this type of snapshot TTR assessment has generally been used in most studies and has been found to be better than other methods in assessing anticoagulation control. Small sample sizes made it impossible for us to statistically assess some factors known to be associated with poor anticoagulation control. In addition, the association of anticoagulation control and adverse events was not studied. It is, however, known that poor anticoagulation control is associated with both thrombotic and bleeding complications. A study on factors associated with poor anticoagulation control is, however, important given the high levels of suboptimal control and is thus recommended.
Conclusion
The quality of anticoagulant therapy among patients on warfarin therapy in Botswana patients is poor. Poor level of anticoagulation is associated with cigarette smoking, being hypertensive, and pulmonary hypertension. The level of anticoagulation control did not vary with age, gender, dose, or indication of warfarin. Poor TTR reported in this study calls for efforts to improve the level anticoagulation control among patients on warfarin in Botswana.
Footnotes
Authors’ Note
JC Mwita contributed to concept of the study, data collection, data analysis, and manuscript writing. JM Francis contributed to data analysis and interpretation; AA Oyekunle and MGMD Magafu contributed in data interpretation and manuscript writing; M Gaenamong and M Goepamang contributed in data collection. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.