
Abstract
We aimed to identify the prevalence of acetylsalicylic acid (ASA) nonresponse in patients after coronary artery bypass graft (CABG) surgery and the possible consequences for the rate of major cardiovascular events. This prospective, observational, bicentric cohort study was conducted in two German University hospitals. A total of 400 patients (200 in each study center) undergoing elective CABG surgery were enrolled after written informed consent. Platelet function was analyzed on day 3 (d3) and day 5 (d5) postoperatively following stimulation with arachidonic acid (ASPItest) and with thrombin receptor–activating peptide 6 (TRAPtest) using multiple electrode aggregometry (Multiplate). Individuals with an ASPItest ≥40 AU·min were categorized as ASA nonresponders. A 1-year follow-up recorded the combined end point of cardiovascular events, hospital admissions, or deaths related to cardiovascular disease. The prevalence of ASA nonresponse was 51.5% on d3, and it significantly increased to 71.3% on d5 (P = .0049). The area under the aggregation curve in the TRAPtest (P < .0001), the platelet count on d5 (P = .009), and the cardiopulmonary bypass time (P = .01) were identified as independent predictors of an ASA nonresponse. A 1-year follow-up recorded 54 events fulfilling criteria for the combined end point with no difference between ASA responders and nonresponders. This study indicates a high incidence of perioperative ASA nonresponse in patients following CABG. No effect on the incidence of cardiovascular events was recorded in the 1-year follow-up. Therefore, a randomized dosage adjustment trial should elucidate whether a tailored ASA treatment after CABG surgery represents a useful concept.
Introduction
A long-term antiplatelet therapy with acetylsalicylic acid (ASA) is one of the mainstays in the prevention of adverse events, such as myocardial infarction or stroke in patients with cardiovascular disease. 1 Various studies have shown that some patients lack the anticipated antiaggregatory effect and named this condition “ASA resistance” or “ASA nonresponse.” Meta-analyses have attempted to adjust for different definitions and diagnostic methods of this state. One of the largest meta-analyses, incorporating 42 studies, found an overall incidence of 24% for ASA nonresponding individuals. 2 The influences by genetic predisposition and risk factors, such as diabetes, obesity, or a metabolic syndrome, are under discussion but have not yet been fully clarified. 3,4 Individuals with a reduced response to ASA treatment had an increased risk of cardiovascular or cerebrovascular events such as myocardial infarction or stroke. 2,5,6
A problem addressed by most meta-analyses was the heterogenous definition of ASA nonresponse in the included studies with different technical devices and laboratory analyses used for the detection of ASA nonresponse. Multiple electrode aggregometry (MEA) is a frequently used analyzer of platelet function, which has been used for the detection of ASA nonresponse in patients with cardiovascular disease. 7,8
The aim of this study was to assess the prevalence and predictors of ASA nonresponse detected by MEA in patients after coronary artery bypass graft (CABG) surgery. The effects of ASA nonresponse on the occurrence of major adverse cardiovascular and cerebrovascular events (MACCEs) were determined for the first year after surgery.
Methods
Trial Design and Patients
This observational, prospective bicentric cohort study was conducted at the University Hospital Frankfurt am Main, Germany (center 1), and the University Medical Center Göttingen, Germany (center 2). The present study was complied with the Declaration of Helsinki and was approved by the local scientific and ethics review board of both participating centers (approval numbers: 33/13 [center 1] and 19/4/13 [center 2]). The study was registered at ClinicalTrials.gov (NCT01824147).
After written informed consent was obtained, 400 consecutive patients with elective CABG surgery and an ongoing therapy with 100 mg of ASA per day were enrolled in the study. Acetylsalicylic acid therapy was not administered on the day of the operation and continued on the first postoperative day. Uncoated ASA 100 mg was used as the standard medication in both centers. Patients were not eligible for the study if they had a known allergy to ASA or were pregnant.
The trial had a mere observational nature and no adjustments in medication were considered in ASA nonresponding individuals. Demographic data, preexisting diseases, and details concerning the surgical procedure were drawn from patients’ electronic records.
Hematological Analyses Data Collection
Blood samples were obtained on the third (d3) and fifth (d5) postoperative day from a perioperatively established central venous catheter using a 2-mL syringe (Injekt Solo; B. Braun Melsungen AG, Melsungen, Germany) to discard 2 mL of blood or with a single venous puncture using a 21-G butterfly needle (Safety-Multifly Set; Sarstedt AG & Co, Nümbrecht, Germany). For MEA analyses, the blood was collected into 2-mL heparin-anticoagulated and calcium-balanced tubes (Blood Gas Monovette; Sarstedt AG & Co). For hemoglobin and platelet counts, blood was collected into a 4.7-mL EDTA tube (Sarstedt AG & Co).
Multiple Electrode Aggregometry
Multiple electrode aggregometry was performed using the whole blood impedance aggregometer Multiplate (Roche AG, Grenzach-Wyhlen, Germany), which is based on impedance aggregometry as described by Cardinal and Flower. The methodological principles of the MEA have been described previously. 9 The in vitro platelet aggregation was initiated by 0.5 mmol/L of arachidonic acid (ASPItest) or 32 mmol/L of thrombin receptor–activating peptide 6 (TRAP-6, TRAPtest) using commercially available reagents (Roche AG). The extent of platelet aggregability was calculated as area under the aggregation curve (AUC), which was presented in arbitrary “aggregation units” (AU·min). The reference ranges for healthy participants given by the manufacturer were 71 to 115 AU·min for the ASPItest and 92 to 151 AU·min for the TRAPtest. According to the manufacturer’s instructions, a sufficient effect of an antiplatelet therapy with ASA was assumed for an ASPItest <40 AU·min.
Primary End Point
The ex vivo-induced platelet aggregation in the ASPItest was defined as the primary end point (AU·min). The patients with an ASPItest ≥40 AU·min were considered to be ASA nonresponders.
Secondary End Point
Ex vivo-induced platelet aggregation in the TRAPtest of MEA (AU·min) and a combined end point defined as MACCEs (myocardial infarction, cerebrovascular infarction, limb ischemia, stent implantation), hospital admission, and/or death related to the cardiovascular disease within the first 12 months after CABG were defined as secondary end points. Data on the occurrence of MACCE were acquired by a standardized follow-up phone call 12 months after surgery.
Sample Size and Statistical Analyses
To assess the prevalence of an ASA nonresponse using MEA with a 95% confidence interval and a maximum range of 10%, a sample size of at least n = 383 was calculated. To compensate for potential dropouts, n = 400 patients, with n = 200 patients for each center, were enrolled.
Depending on the distribution of the data from the Kolmogorov-Smirnov test, the results are given as the mean (standard deviation) or the median (25th and 75th percentiles, interquartile range). Aggregometric measurements were compared using a Mann-Whitney U test. Fisher exact test was used to compare the incidence of the ASA nonresponse in the different groups.
Multiple logistic linear regression analysis including the variables age, gender, body mass index (BMI), nicotine abuse, hemoglobin, platelet count, cardiopulmonary bypass (CPB) time, and use of extracorporeal circulation for CABG (on-pump CABG) was performed to identify potential independent risk factors for an ASA nonresponse. For this analysis, ASA nonresponse was defined as a nonresponse on the third and/or the fifth postoperative day. This definition was also applied for comparing demographics and evaluating data from the follow-up interview. The statistical analyses were performed using Statistica 12 (StatSoft Inc, Tulsa, Oklahoma).
Results
During April 2013 and November 2014, a total of 400 patients (center 1: n = 200; center 2: n = 200) were enrolled in the study. Thirty-two patients were lost to follow-up (center 1: n = 30; center 2: n = 2). The sociodemographic and clinical characteristics of the 400 evaluated patients are presented in Table 1, and the flow of patients is depicted in Figure 1.
Demographic Data.
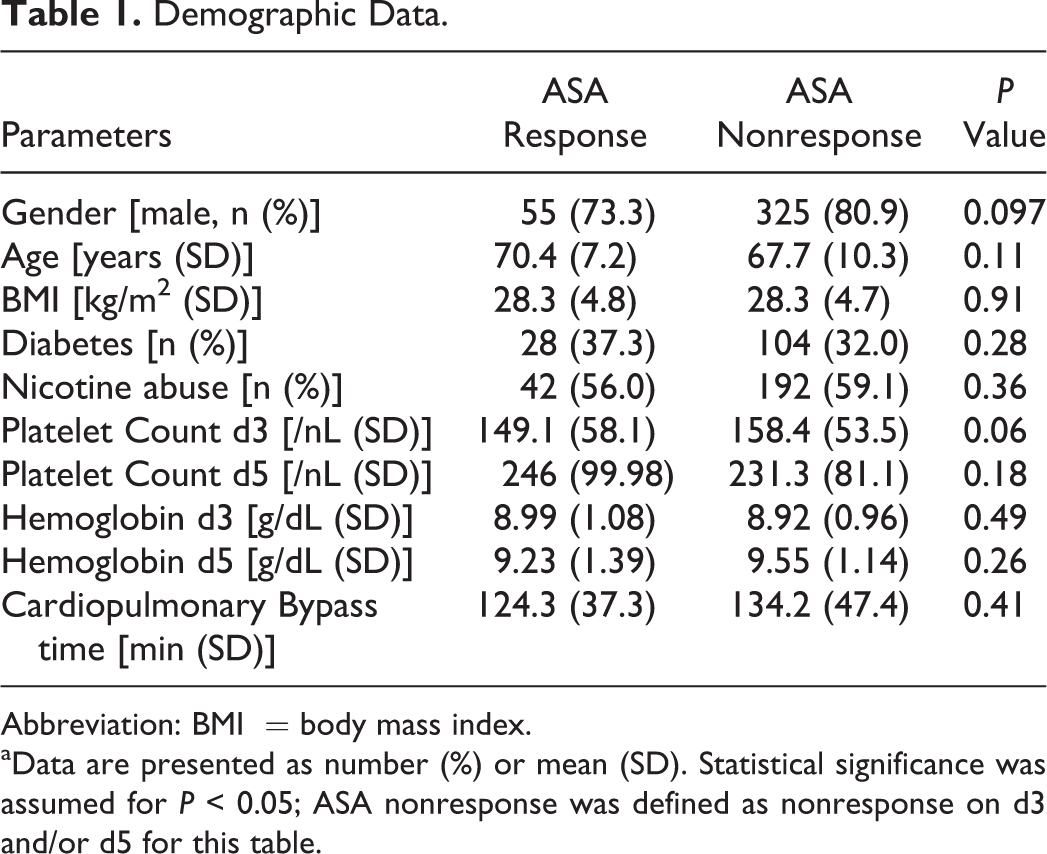
Abbreviation: BMI = body mass index.
aData are presented as number (%) or mean (SD). Statistical significance was assumed for P < 0.05; ASA nonresponse was defined as nonresponse on d3 and/or d5 for this table.
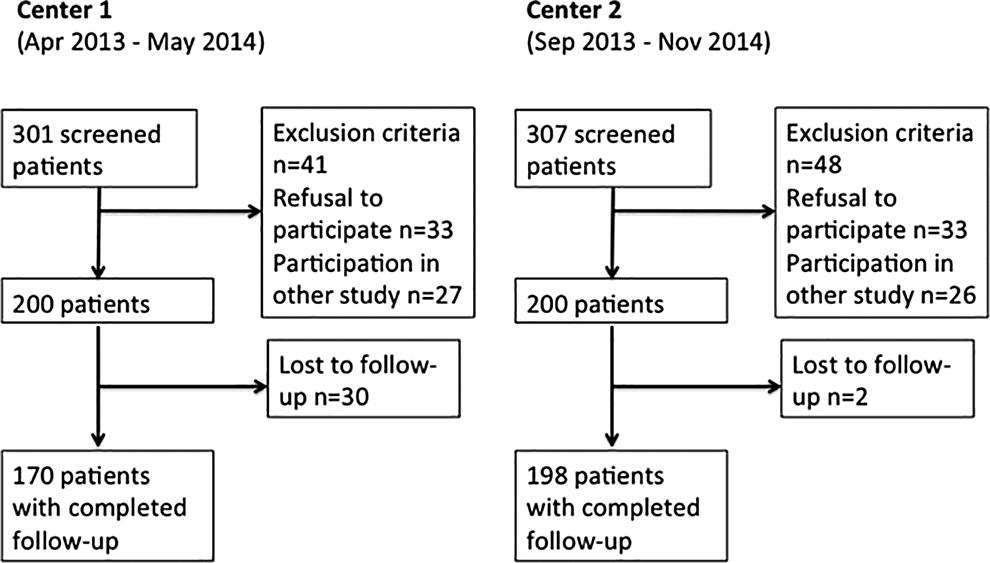
Flow of patients for center 1 and center 2.
With a cutoff of 40 AU·min in the ASPItest, patients were allocated into either the ASA response group (ASPItest <40 AU·min) or the ASA nonresponse group (ASPItest ≥40 AU·min). In total, 51.5% (n = 206) of the patients showed insufficient ASA response on the third postoperative day. The rate of ASA nonresponders significantly increased to 71.3% (n = 285) on the fifth postoperative day (P = .0049).
Figures 2 and 3 show the results of aggregometric analyses of platelet function. Acetylsalicylic acid responders not only showed a significantly lower median AU·min in the ASPItest on both days but also a significantly lower AU·min in the TRAPtest compared to ASA nonresponders (Table 2).
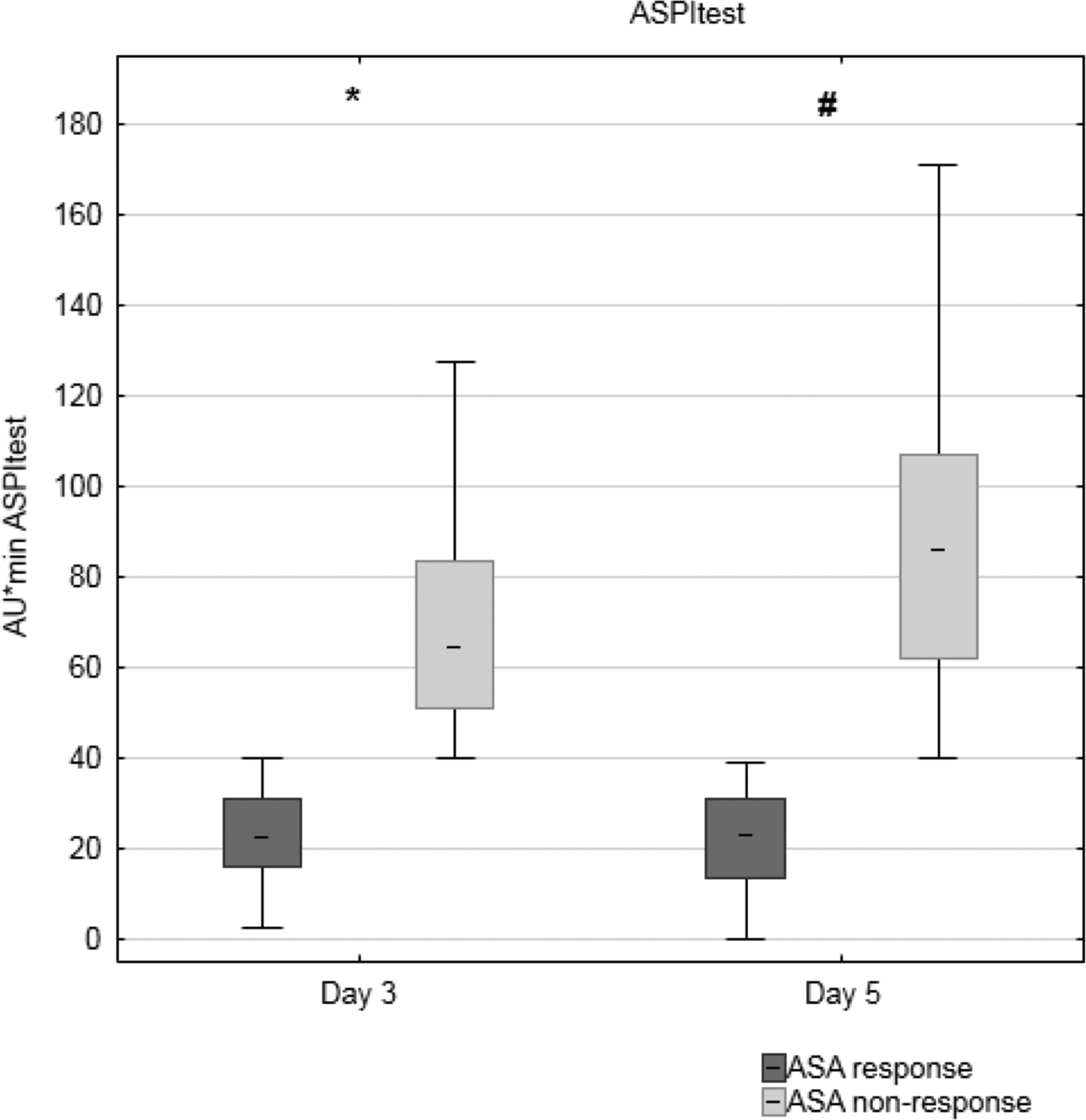
Ex vivo-induced platelet aggregation following stimulation with arachidonic acid (ASPItest) on the third (d3) and fifth (d5) postoperative day after coronary artery bypass surgery (CABG) surgery. *A significant difference between the groups on d3 (P < .0001). #A significant difference between the groups on d5 (P < .0001). Acetylsalicylic acid (ASA) response (d3 n = 194; d5 n = 115); ASA nonresponse (d3 n = 206; d5 n = 285).
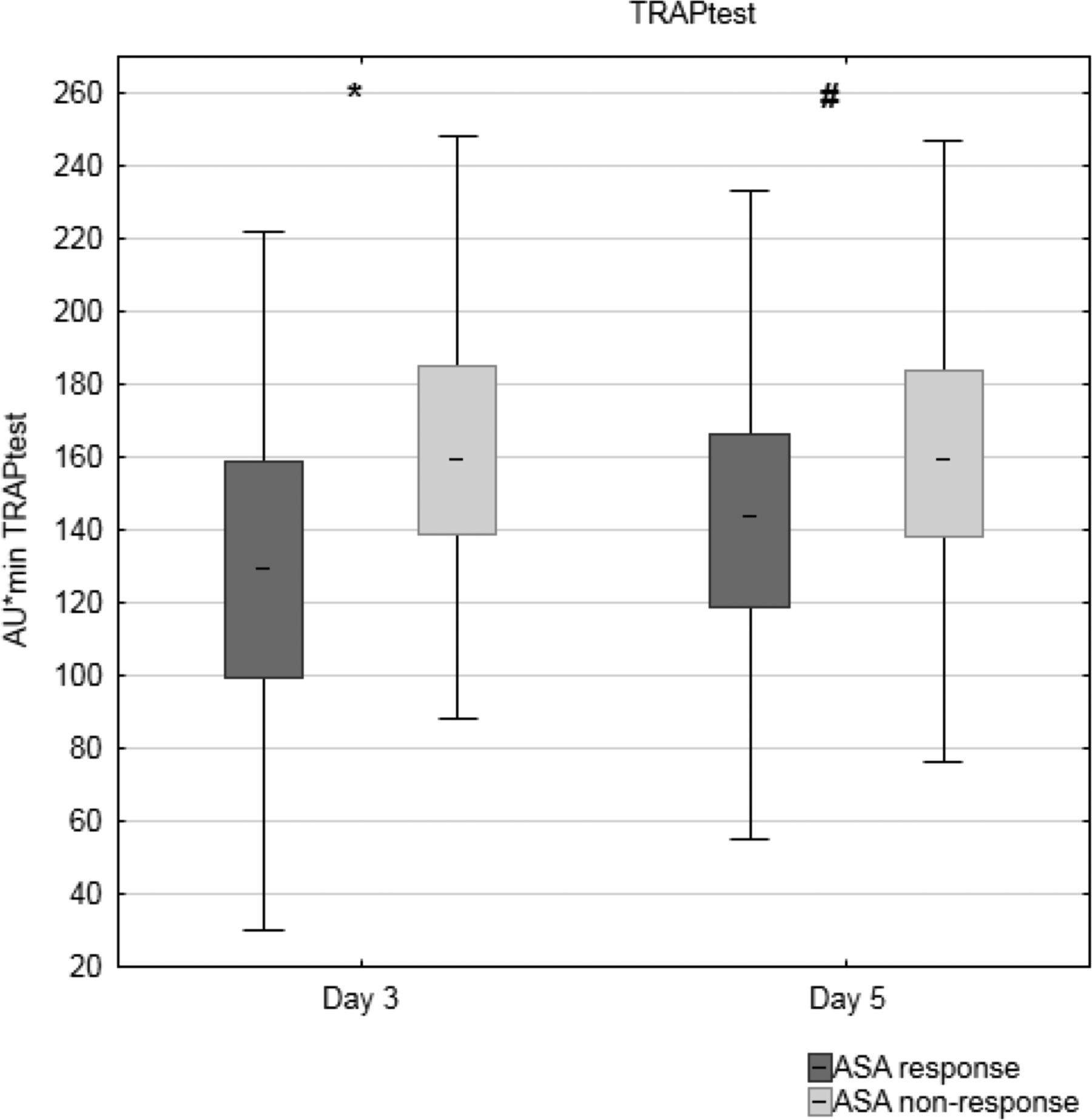
Ex vivo-induced platelet aggregation following stimulation with thrombin receptor–activating peptide (TRAPtest) on the third (d3) and fifth (d5) postoperative day after coronary artery bypass surgery (CABG) surgery. *A significant difference between the groups on d3 (P < .0001). #A significant difference between the groups on d5 (P < .0001). Acetylsalicylic acid (ASA) response (d3 n = 194; d5 n = 115); ASA nonresponse (d3 n = 206; d5 n = 285).
Aggregometric Measurements.
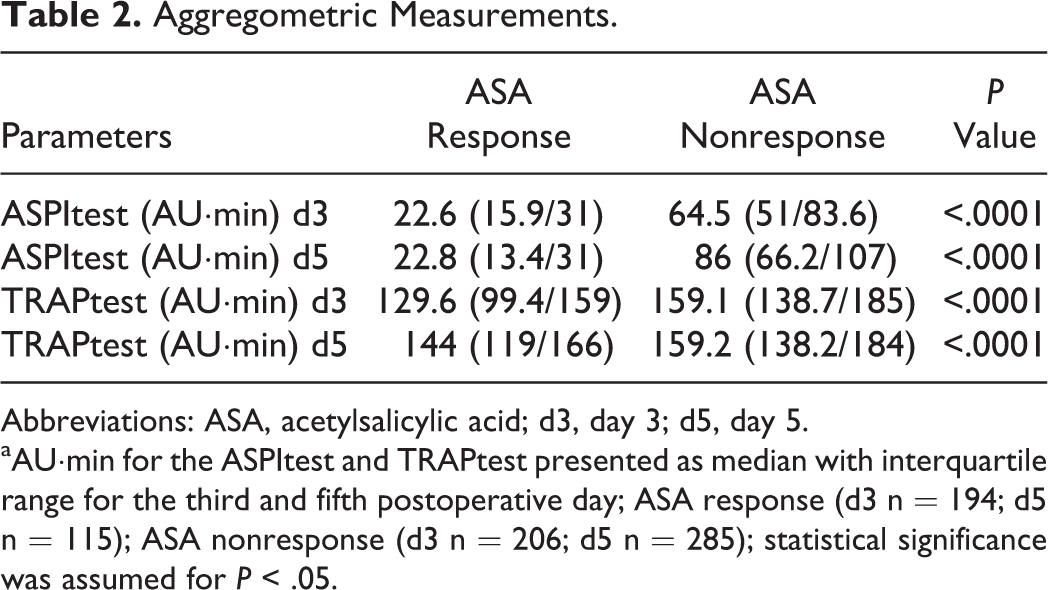
Abbreviations: ASA, acetylsalicylic acid; d3, day 3; d5, day 5.
aAU·min for the ASPItest and TRAPtest presented as median with interquartile range for the third and fifth postoperative day; ASA response (d3 n = 194; d5 n = 115); ASA nonresponse (d3 n = 206; d5 n = 285); statistical significance was assumed for P < .05.
Multiple logistic linear regression analysis identified the AUC in the TRAPtest (P < .0001), the platelet count on the fifth postoperative day (P = .009), and the CPB time (P = .01) as independent predictors of ASA nonresponse.
The 1-year follow-up revealed 54 events in 52 patients fulfilling criteria for the combined end point of MACCE, hospital admission, or death related to the cardiovascular disease. Details on the rate of each event are summarized in Table 3. There was no significant difference between the groups with an event rate of 16.7% in the ASA response group and 14.4% in the ASA nonresponse group (P = .40). Four of the 54 events occurred within the first 4 postoperative weeks (ASA response n = 0, ASA nonresponse n = 4; P = .45).
Incidence of the Events Included in the Combined End Point.
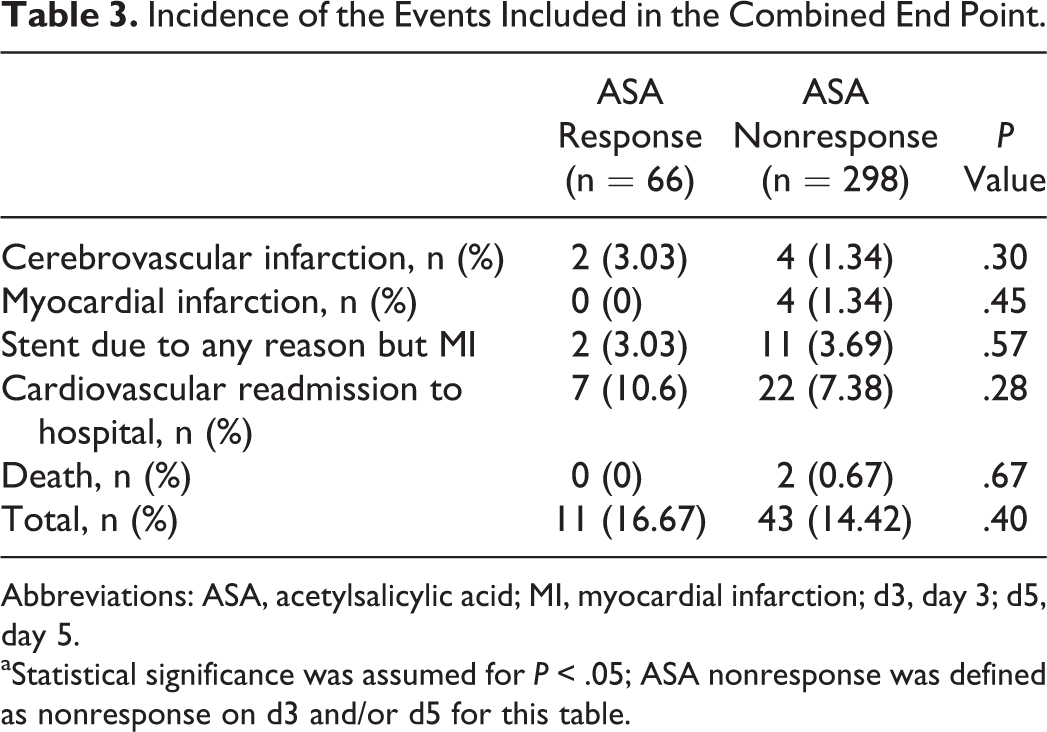
Abbreviations: ASA, acetylsalicylic acid; MI, myocardial infarction; d3, day 3; d5, day 5.
aStatistical significance was assumed for P < .05; ASA nonresponse was defined as nonresponse on d3 and/or d5 for this table.
Discussion
The aim of this study was to analyze platelet function using MEA and determine the prevalence and predictors of ASA nonresponse in patients after CABG surgery. Demographic and laboratory characteristics were prospectively collected to identify independent risk factors for a postoperative ASA nonresponse. We performed a 1-year follow-up survey to investigate the effects of a postoperatively diagnosed ASA nonresponse on the incidence of the predefined combined end point.
We observed an ASA nonresponse in more than half of the patients on the third postoperative day, with a significant increase on the fifth postoperative day. Furthermore, we identified a higher AUC in the TRAPtest and a longer CPB time as independent risk factors for an impaired effect of postoperative ASA treatment. However, the follow-up survey did not unveil any differences in the incidence of the predefined combined end point between patients with and without ASA nonresponse.
The rate of ASA nonresponders in our study was markedly higher than the rates of 25% to 28% reported previously in large meta-analyses. 5,6,10 However, Hovens et al noted that the definitions of ASA nonresponse are heterogeneous and vary in their sensitivity regarding ASA responsiveness. 2 Multiple electrode aggregometry is known to detect the effects of ASA treatment sensitively and reliably. 7,11 Given that meta-analyses included studies evaluating less sensitive methods, which detected lower nonresponse rates as well, the average nonresponse rate calculated in these meta-analyses could be lower than the rates detected with MEA alone. In the present study, individuals with ≥40 AU·min in the ASPItest were considered as ASA nonresponders as recommended by the manufacturer. Nevertheless, this cutoff was higher than the 30 AU·min used in other studies and has to be considered when comparing results. Nevertheless, the ASA nonresponse rates after on-pump cardiac surgery appear to be increased. Petricevic et al found a nonresponse rate of approximately 33% with MEA on the fourth postoperative day after CABG surgery and a therapy with 300 mg of ASA per day. 12 Using the PFA-100 (Siemens Healthcare Diagnostics GmbH, Eschborn, Germany) device, Zimmermann et al also identified very high rates of ASA nonresponse after cardiac surgery. 13 In contrast, studies evaluating patients with stable coronary artery disease without surgical interventions found markedly lower nonresponse rates. 14,15
One reason contributing to the increased ASA nonresponse rates after on-pump CABG surgery might be an increased perioperative platelet turnover. Arazi et al identified a significant correlation between this condition and a postoperative ASA nonresponse. 16 Assuming that a longer extracorporeal circulation leads to greater impairment of platelet function, one could suppose that the identification of the CPB time as an independent risk factor for an ASA nonresponse in the present study reflects a higher platelet turnover in patients with a longer CPB time. Because no laboratory markers for an increased platelet turnover were measured in this study, this question cannot be answered by the current results.
The significantly higher TRAPtest of ASA nonresponders in our study, which was also identified as an independent risk factor, cannot be explained by an increased platelet turnover. In the present study, patients with an ASA nonresponse appeared to exhibit enhanced overall platelet responsiveness as well. The trend toward a hypercoagulatory disposition and toward an increased risk of venous thromboembolism in the postoperative period after major surgery has been demonstrated in several studies. 17,18 This state can have manifold causes, such as tissue factor release due to surgical trauma, impaired fibrinolysis, or inflammation. 19,20 Lison et al found an initial decrease in platelet function for the first 2 days after major surgery followed by a continuously increasing AU·min in MEA measurements from the second to the sixth postoperative day. 21 Because Lison et al excluded patients with cardiac surgery, these results and the presented data can only be compared to a limited extent. However, the tendency to higher platelet responsiveness appeared to be present in patients after cardiac surgery with CPB as well. 22 To what extent this higher responsiveness may account for an ASA nonresponse in patients cannot be answered by our data. Nevertheless, the incidence of ASA nonresponse observed postoperatively in this study was markedly higher than the numbers reported in patients without surgical trauma. 4
In addition to the effects of increased platelet turnover and postoperative hypercoagulability described above, the analgesic medication may have contributed to the high rates in ASA nonresponse. Pyrazolone, as well as other nonsteroidal anti-inflammatory drugs, has been shown to interfere with the inhibitory effect of ASA on the synthesis of thromboxane within the normal therapeutic range. 23,24 Polzin et al demonstrated that this interaction has a relevant in vivo effect in patients with coronary artery disease. 25 The postoperative analgesic therapy in both centers included a basal medication with the pyrazolinone metamizole, which could have had an additive effect on the incidence of ASA nonresponse.
The negative effect of an ASA nonresponse on the rate of MACCEs in patients having a stroke or an acute coronary syndrome has been demonstrated. 26 –28 The postoperative ASA nonresponse observed in many patients, though, appeared to be a transient phenomenon. 13,29 Zimmermann et al detected high nonresponse rates on the fifth postoperative day using the PFA-100 analyzer and a nearly complete ASA response in the follow-up after 6 months. 13 Its effect on the postoperative mortality and morbidity is still not fully clarified yet. The follow-up after 1 year in the current study did not show an increased risk of MACCEs or hospital readmission in patients, which had displayed a postoperative ASA nonresponse. This fact did not change, even when considering a lower cutoff ≥30 AU·min as it has been used in other studies evaluating ASA nonresponse. This was in line with other studies evaluating the effect of ASA nonresponse after CABG or the implantation of a ventricular assist device. 30 –32 In contrast, Poston et al report a correlation between results of whole blood aggregometry and an early graft thrombosis within the first 5 days after off-pump coronary artery bypass. 33
Two studies evaluated the effect of dual antiplatelet therapy by adding 75 mg clopidogrel to the treatment in patients with an ASA nonresponse to 300 mg ASA. 8,12 Gasparovic et al reported less adverse events after 6 months for the subgroups of patients on dual antiplatelet therapy with a BMI >30 kg/m2 and age <65 years, 8 whereas Petricevic et al did not find any effects of a dual antiplatelet therapy on the outcome of patients after CABG. 12 Both studies observed event rates during their 6-month follow-up comparable to the results obtained in our present study. However, platelet monitoring in both studies was only used to identify ASA nonresponsive patients and not to confirm the effect of the intervention on platelet activation by arachidonic acid. Paikin et al demonstrated that the response to ASA after CABG could be significantly improved by a regime with a repetitive application of ASA 4 times a day versus a single daily dosage regime. 34 Considering this, further dosage adjustment studies should use platelet function testing not only to allocate patients to a study group but also to verify the effect of a possible intervention.
The current study has some limitations. First, the sample size was calculated mainly to identify the incidence of postoperative ASA nonresponse. Therefore, this study may have been underpowered with respect to the occurrence of the predefined combined end point. Second, we did not conduct platelet function testing as part of the follow-up. Thus, we could only assume that the high incidence of ASA nonresponse found in the current study was only a transient effect as it has been shown in other studies. 13,29 Third, we did not perform light transmission aggregometry (LTA) as a gold standard for the measurement of platelet aggregation, which seemed reasonable considering the costs and complexity of the method and the fact that a good correlation between LTA and the results of MEA has been demonstrated repeatedly. 35
In conclusion, the present study showed a high incidence of perioperative ASA nonresponse in patients following CABG surgery. Potential causes for this increased incidence compared to an outpatient population may be various and include inflammation, increased platelet turnover after CPB, and analgesic medication with nonopioids. In the current study, an ASA nonresponse was not associated with the occurrence of MACCEs or hospital readmission during a 1-year follow-up period. Paikin et al demonstrated that the inhibition of thromboxane synthesis after CABG surgery could be improved by a higher dosage of ASA or multiple dosages of ASA per day. 34 Considering this result, a randomized dosage adjustment trial using platelet function monitoring may be helpful in the further evaluation of the question if and to what extent an individually adjusted ASA dosage represents a potentially beneficial concept for the postoperative management of patients after CABG surgery.
Footnotes
Authors’ Note
The trial was registered with clinical trials with the identifier NCT01824147 on March 26, 2013. IRB approval was granted on March 28, 2013 (center 1, approval number 33/13), and on June 19, 2013 (center 2, approval number 19/4/13).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the University of Frankfurt and the University of Göttingen and was performed without any industrial support. SW received speaker’s honoraria from CSL Behring, PM received research grants from the German Research Foundation (ME 3559/1-1, ME 3559/3-1), International Anesthesia Research Society, German Society of Anaesthesiology and Intensive Care Medicine, and European Society of Anaesthesiology; received grants from B. Braun Melsungen, CSL Behring, Fresenius Kabi, and Vifor Pharma for the implementation of Frankfurt’s Patient Blood Management Program; from Pfizer for investigator-initiated trial; honoraria for scientific lectures from B. Braun Melsungen, Vifor Pharma, Ferring, CSL Behring, Heinen & Löwenstein, and Aesculap Academy. NKS received speaker’s honoraria from 3M Inc and CSL Behring. KZ received research grants from the German Research Foundation (ME 3559/1-1, ME 3559/3-1, SFB 834 B4, SFB 815 A17, KFO TP07, ECCPS, LOEWE TP 6) and European Union; received grants from B. Braun Melsungen, CSL Behring, Fresenius Kabi, and Vifor Pharma for the implementation of Frankfurt’s Patient Blood Management Program; honoraria for scientific lectures from B. Braun Melsungen, Vifor Pharma, Ferring, TEM International, Med Update GmbH, Bayer, Biotest AG, Nordic Group, Fresenius Kabi, AIT Wien, Haemonetics SA, Edwards, Fresenius Medical Care, Fresenius Kabi, Masimo SA, Photonics Healthcare, Abbvie Deutschland GmbH, Teleflex GmbH, Serumwerk Berneburg, DELAB, Aesculap Akademie, Index Venture, Art Tempi, Heinen & Löwenstein, Siemens, Medi Didac GmbH, Hamilton, Baxter, Grünenthal, and CSL Behring. AFP received speaker’s honoraria from HeartWare Inc. CFW received speaker’s honoraria from Roche, Verum Diagnostics, Tem International, and B. Braun