
Abstract
There is an urgent need for additional therapeutic options for acute ischemic stroke considering the major pitfalls of the options available. Herein, we briefly review the role of cerebral blood flow, collaterals, vasoreactivity, and reperfusion injury in acute ischemic stroke. Then, we reviewed pharmacological and interventional measures such as volume expansion and induced hypertension, intra-aortic balloon counterpulsation, partial aortic occlusion, extracranial–intracranial carotid bypass surgery, sphenopalatine ganglion stimulation, and transcranial laser therapy with regard to their effects on flow augmentation and neuroprotection.
Keywords
Introduction
Stroke is a major health problem all over the world. 1,2 The only Food and Drug Administration (FDA)-approved therapy for acute stroke to date is recombinant tissue plasminogen activator (rtPA) which can be started within 3 hours from symptom onset although the American Heart Association has recommended its use within 4.5 hours from symptom onset in a selected group of patients. These constraints in timing has limited the number of patients who can be treated which was, in the early years, about 2% of all ischemic strokes, more recently the proportion has increased to around 10%. 3 Therefore, finding a therapeutic option for the patients who arrive to the hospitals beyond the thrombolytic window or who are not candidates for thrombolysis because they have a contraindication is a crucial target for stroke scientists.
The heterogeneous mechanisms involved in ischemic insults to the brain including but not limited to neuroinflammatory pathways, 4 excitotoxic cascades, 5 oxidative and nitrative stress, 6 free radicals, 7 Ca++ influx, 8 proapoptotic cascades, 9 and so on have been targeted in an effort to minimize the neuronal damage during an ischemic insult to the brain. To date, no neuroprotective drug has proven beneficial to limit ischemic injury, despite the incredibly huge investment on research. 10 As a result, there remains an urgent need for additional therapeutic options for acute ischemic stroke.
Herein, we briefly review the role of cerebral blood flow (CBF), leptomeningeal collaterals, and vasoreactivity in acute ischemic stroke. Then, we review pharmacological and interventional measures such as plasma volume expansion and induced hypertension (HTN), intra-aortic balloon counterpulsation (IABC), partial aortic occlusion, extracranial–intracranial (EC/IC) carotid bypass surgery, sphenopalatine ganglion (SPG) stimulation, and transcranial laser therapy (TLT).
Selection Criteria
The authors searched the Institute for Scientific Information Web of Knowledge, MEDLINE (National Library of Medicine), and Scopus databases as 3 major scientific search engines, from 1990 to 2014. They used the following MeSH key words as search terms: “ischemic stroke,” “cerebral blood flow,” “volume expansion,” “induced hypertension,” “cerebrovascular collaterals,” “intra-aortic balloon counterpulsation,” “partial aortic occlusion,” “extracranial–intracranial carotid bypass surgery,” “sphenopalatine ganglion stimulation,” and “transcranial laser therapy.” We also searched the reference lists of articles identified by this search strategy and selected those we judged relevant. Human and animal studies published in English were included (Table 1).
An Outline of the Main Preclinical and Clinical Studies Evaluating the Efficacy and Safety of Pharmacologically Induced Hypertension and Volume Expansion, IABC, Partial Aortic Occlusion, Emergency EC-IC Bypass Surgery, External to Internal Carotid Artery Flow Diversion, RTN, TLT, and SPG Stimulation in Acute Ischemic Stroke.a
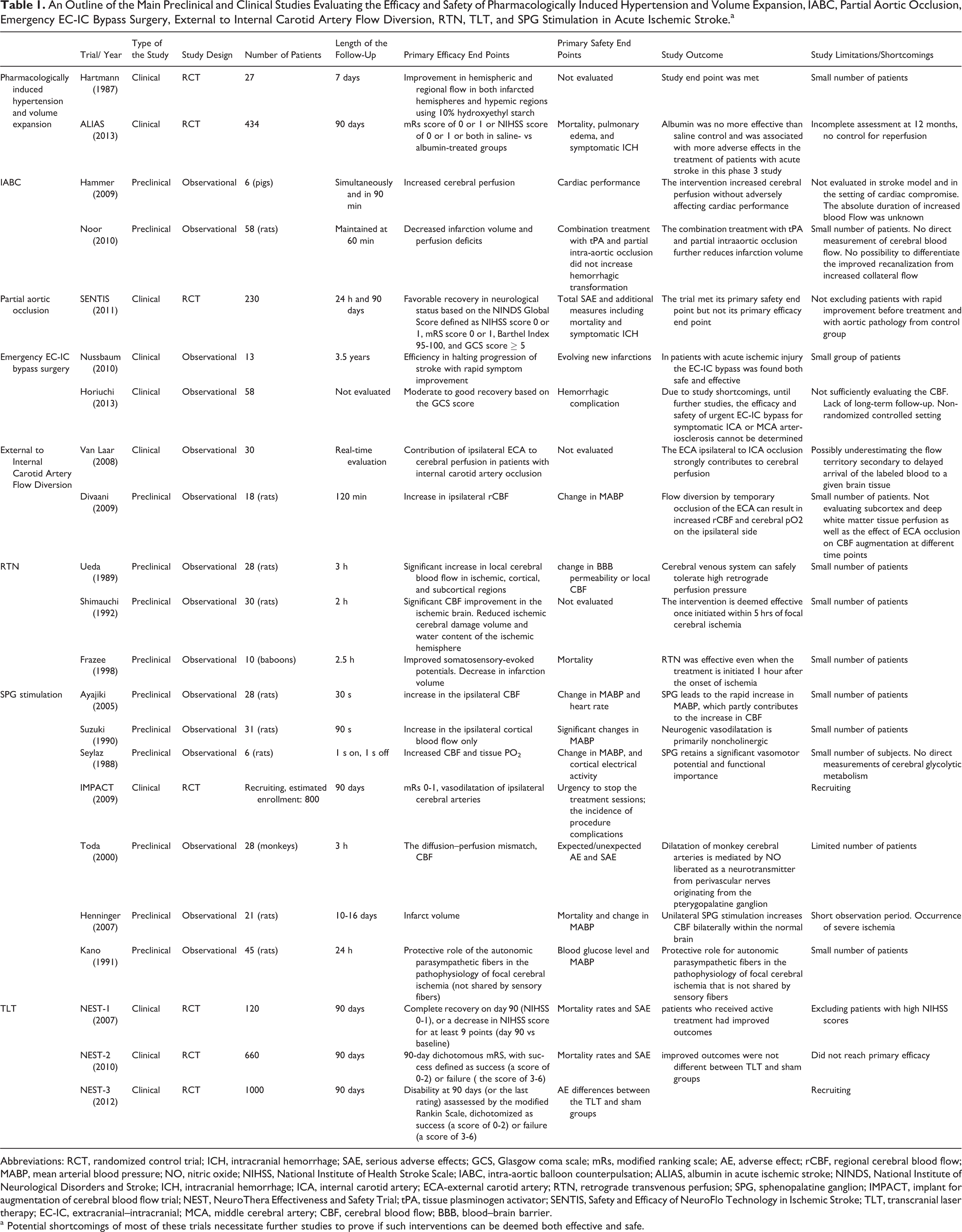
Abbreviations: RCT, randomized control trial; ICH, intracranial hemorrhage; SAE, serious adverse effects; GCS, Glasgow coma scale; mRs, modified ranking scale; AE, adverse effect; rCBF, regional cerebral blood flow; MABP, mean arterial blood pressure; NO, nitric oxide; NIHSS, National Institute of Health Stroke Scale; IABC, intra-aortic balloon counterpulsation; ALIAS, albumin in acute ischemic stroke; NINDS, National Institute of Neurological Disorders and Stroke; ICH, intracranial hemorrhage; ICA, internal carotid artery; ECA-external carotid artery; RTN, retrograde transvenous perfusion; SPG, sphenopalatine ganglion; IMPACT, implant for augmentation of cerebral blood flow trial; NEST, NeuroThera Effectiveness and Safety Trial; tPA, tissue plasminogen activator; SENTIS, Safety and Efficacy of NeuroFlo Technology in Ischemic Stroke; TLT, transcranial laser therapy; EC-IC, extracranial–intracranial; MCA, middle cerebral artery; CBF, cerebral blood flow; BBB, blood–brain barrier.
a Potential shortcomings of most of these trials necessitate further studies to prove if such interventions can be deemed both effective and safe.
Cerebral autoregulation
Cerebral autoregulation is the physiological mechanism by which the brain maintains a stable CBF, despite a wide range of changes in blood pressure (BP) or intracranial pressure over time. Cerebral autoregulation makes the CBF remain at a constant physiologic range 11 which is normally within a perfusion pressure ranging from 50 to 150 mm Hg, 12 although the dynamic cerebral autoregulation shows beat-to-beat changes in CBF in response to rapid changes in BP. 13 The limits of cerebral autoregulation may change depending on the habitual BP or a particular individual; that is to say, for individuals with HTN those thresholds may be shifted to the right, while in people with lower BP, for instance toddlers, the thresholds may be shifted to the left.
Cerebral autoregulation is regulated by metabolic, neurogenic, or myogenic mechanisms.
14
The myogenic mechanism plays its part at the level of small pial vessels altering the transmural pressure as a consequence of variation in BP.
15
The metabolic mechanism leads to cerebral vasodilation secondary to increased arterial pressure (Pa)
During the acute phase of stroke, ischemia affects the endothelial and smooth muscles, resulting in the impairment of cerebral autoregulation 18 , 19 which make the CBF depend on the changes in BP. From the clinical standpoint, changes in BP in the face of impaired autoregulation can lead to hemorrhagic transformation, brain edema, or further ischemic injury. 14 The loss of cerebral autoregulation not only makes the site of stroke succumb injury but also affects the contralateral hemisphere. This can be explained by the loss of interhemispheric connections leading to the functional depression of the contralateral side over the course of ischemic stroke. 20
Reperfusion injury
Reperfusion injury is defined as tissue damage in a previously hypoperfused area following recanalization. The impaired cerebral autoregulation results in the loss of adaptation in the thrombosed vessel making them incapable of re-establishing blood flow. In other words, the vessel that has been fully dilated in response to reduced blood flow distal to the thrombus loses the capacity for quick constriction to adjust itself with the increased flow following recanalization. Some major complications of reperfusion injury include vasogenic edema, headache, seizure, and, most importantly, the hemorrhagic transformation. The effect of reperfusion on the brain tissue which has been acutely exposed to hypoperfusion differs from that of chronically hypoperfused brain region. 21
Several mechanisms contribute to reperfusion injury. Cellular depolarization following Na/K adenosine triphosphatase (ATPase) pump failure induces the activation of enzymes of the apoptotic cascade. 22 The role of reactive oxygen species (ROS), both produced and targeted by mitochondria, is central to apoptosis induction under pathologic conditions such as ischemic stroke. Moreover, leukocyte infiltration may also play a role in blood–brain barrier (BBB) dysfunction by producing ROS. 23 Platelets are also involved in the reperfusion injury by occlusion of the microvascular beds distal to the thrombi leading to the no-reflow phenomenon. 24 They also release mediators such as thromboxane A2 and ROS causing temporary vasospasm. 25 The administration of rtPA leads to the upregulation of matrix metalloproteinases and results in BBB disruption. 26
The risk of reperfusion injury is higher in patients older than 75 years, those with chronic or postprocedural HTN, history of prior stroke, poor cerebrovascular reserve (eg, >90% internal carotid stenosis), and poor or stenotic collaterals. 27 The time to treat issue is another factor that is believed to affect the extent of hyperperfusion injury. To date, the question on the ideal time to start the treatment has remained controversial and open to debate. 28 This is mostly rooted in the potential risk of hemorrhagic transformation after recanalization. Nevertheless, recanalization within 6 hours of stroke onset would yield lower risk of intracranial hemorrhage (ICH). 29 –31
Hemorrhagic transformation is assumed to occur following the reperfusion into the injured vessels, which allows blood extravasation through the damaged BBB. Reperfusion injury and oxidative stress, leukocyte infiltration, vascular activation, and dysregulated extracellular proteolysis are considered as potential triggers for the hemorrhagic transformation. 23,26 Clinical factors that are shown to be associated with a higher incidence of hemorrhagic transformation include the profound neurological deficit, longer time to treatment, use of anticoagulants, low platelet counts, history of diabetes, elevated systolic BP, elevated glucose levels, and large infarct volume. 27,29
Cerebral Blood Flow
Cervicocephalic collaterals include the extracranial and intracranial collateral vessels. Extracranial collaterals per se comprise several anastomoses between branches of external and internal carotid arteries. Intracranial collateral channels are categorized into primary collaterals such as the communicating arteries of the circle of Willis and secondary collaterals including dural collaterals and leptomeningeal vessels. The interconnections of the circle of Willis are known to play a significant role in maintaining the cerebral circulation distal to a proximal occlusion. It has been shown that delayed recanalization (300 minutes) leads to better clinical outcome in those with good when compared to poor leptomeningeal collaterals. 32
There are some key variables determining the adequacy of collaterals that differ among individuals as follows. 33 There is an age and dose-dependent decline in the number and diameter of collaterals with their increased tortuosity, resulting in an increased collateral resistance. 34,35 The age per se may also decrease the cerebrovascular reactivity. History of HTN is shown to be significantly associated with poor collaterals. Moreover, pretreatment with statins increases the probability of good collaterals. 36
Cerebral vasoreactivity is speculated to be regulated by 2 vascular structures. First, smooth muscle aggregates, which are located in the intima layer of intracranial arteries known as intimal cushions. These are prominent in the area of bifurcations that are innervated by autonomic system. 37 Second, the intimal folds with their valve-like function which increase by age and secondary to high BP. 38
Blood Flow Augmentation Principles
The increased CBF and enriched collateral circulation may play an important part in decreasing the infarct size 39 and probably in preventing the hemorrhagic transformation. 40 Since the extent of CBF reduction during ischemia is a significant determinant of the extent of tissue damage, 41 strategies for early augmentation of CBF would seem as natural options, as augmenting CBF through collaterals can help extending the time window for other therapies including endovascular interventions. 33 In addition, increasing the blood flow through collaterals can help in better delivery of thrombolytic agents to both the proximal end of thrombus and the distal end resulting in good outcomes. 42,43 Flow augmentation mechanisms can be divided into pharmacological and nonpharmacological categories.
Pharmacological-Induced HTN and Volume Expansion
Although induced HTN in acute ischemic stroke using agents such as phenylephrine, norepinephrine, dopamine, dobutamine, and diaspirin cross-linked hemoglobin has been tried in small series, no well-designed large trial has successfully drawn a clear image in this regard. 44 The increased risk of hemorrhagic transformation, particularly in the patients who received thrombolytic therapy, is considered a major challenge. 45
Intravascular volume expansion using dextran 46 and hydroxyethyl starch 47 failed to show any improvement in acute ischemic stroke. The use of albumin has provided some early promising results. In addition to its hypervolemic effects, it also has antioxidant, antithrombotic, and anti-inflammatory properties. 48
Unfortunately, in a large trial known as “albumin in acute stroke” (ALIAS), high-dose albumin (2 g/kg) was infused within 5 hours of stroke and its effects was compared with placebo saline treatment. The trial did not reach its primary efficacy end point. The first 30-day mortality was higher in albumin-treated patients than the placebo group. However, the mortality rate after 30 days was similar in both the groups. It was then proposed that albumin may induce myocardial stress in susceptible patients. 49 While in a subset analysis excluding very elderly patients, albumin treatment resulted in a significantly more favorable outcome. 50 The negative results with regard to the primary outcome indicate that albumin cannot be recommended for the treatment of acute stroke, given the current evidence.
Intra-Aortic Balloon Counterpulsation
Complete or partial aortic occlusion of either the descending thoracic or the abdominal aorta above the renal arteries is shown to result in an increased cerebral blood volume remaining even after the deflation of the balloon. 51,52 Interestingly, this effect has persisted after balloon withdrawal. 52 Inflating the intra-aortic balloon during diastole would displace the blood volume from the thoracic aorta and once the balloon rapidly deflates during systole, it effectively reduces the afterload and consequently improves the cardiac output. 34 IABC was first administered successfully in patients with myocardial infarction-induced cardiogenic shock. 53
Thereafter, IABC was used in the treatment of subarachnoid hemorrhage (SAH)-induced vasospasm in some human case reports. 54 Studies in animals have yielded promising results with respect to the effect of IABC on cerebral perfusion. 35 , 52 To the best of our knowledge, there is no study regarding the use of IABC in humans with acute stroke and the method has solely been used for cerebral vasospasm. 55 At present, there is no evidence to support the use of IABC in the management of acute stroke.
Partial Aortic Occlusion
The results of IABC studies led to the development of the NeuroFlo catheter (CoAxia). Neuroflo is a dual balloon catheter placed in the abdominal aorta via a standard 9F femoral introducing sheath. Two independently inflatable balloons are placed immediately above and below the renal arteries. An aortogram should be obtained to ascertain the appropriateness of NeuroFlo treatment. Two balloons are independently inflated to occupy about 70% of the aortic lumen 6 cm above and below the renal arteries. During the sequential inflation (starting with the infrarenal balloon), the suprarenal and infrarenal pressures would be monitored. Balloons would be sequentially inflated until a pressure difference of 10 to 15 mm Hg across the suprarenal and infrarenal balloons is reached with a lower pressure at the infrarenal part. Balloons would then be left inflated for 45 minutes and then slowly deflated with the catheter removed. During the procedure, heparin may be used by the interventionist as indicated. 56
NeuroFlo was first used for symptomatic vasospasm after intracerebral aneurysm repair or coiling. This approach resulted in increased blood flow velocities in the middle cerebral arteries and neurological improvement in 83% of the cases. 57
The Safety and Efficacy of NeuroFlo Technology in Ischemic Stroke (SENTIS) trial investigated the applicability of CBF augmentation in patients with acute ischemic stroke 14 hours from the onset of symptoms. 55,58
The primary safety analysis showed no statistically significant difference between the 2 groups. The proportion of patients showing SAE was 42.8% in the control group and 43.9% in the treatment group (P ≥ .923). Meanwhile, there has been consistent reduction in stroke-related mortality in the case group. Stroke-related deaths and stroke-related deaths due to neurologic causes were also fewer among treated group. 59 According to the SENTIS trial, patients who presented within 5 hours after the onset of symptoms and those with the baseline NIHSS scores of 8 to 14 who were older than 70 years had a more favorable outcome. Based on such findings, the presence of highly developed collaterals in older patients makes CBF augmentation an effective option in this group. 58 In post hoc analysis, the favorable vascular profile, that is, intact circle of Willis and the presence of good cerebral perfusion pressure (mean arterial BP > 65 mm Hg), independently predicted the outcome in a subpopulation of SENTIS trial. 60
In summary, although the SENTIS trial failed to reach its primary efficacy end point, partial aortic occlusion may still remain a potential tool for treatment of stroke in acute phase, at least in a selected group of patients. Furthermore, Neuroflo has its own limitations due to its invasiveness. It may accompany the access site bleeding. The lack of availability of angiography suites in all hospitals makes this technique expensive compared to others.
Emergency Extracranial–Intracranial (EC/IC) Bypass Surgery
Extracranial–intracranial (EC-IC) arterial bypass surgery is connecting the superficial temporal artery with the middle cerebral artery (MCA) branches to bypass atherosclerotic stenosis or occlusions of the internal carotid artery (ICA) or MCA. 61 The results of studies using EC/IC bypass surgery in patients with acute ischemic stroke have shown that the procedure was both safe and effective. 62 , 53
However, the aforementioned case studies have been performed in patients with subacute rather acute stroke. In addition, the required general anesthesia for the bypass surgery in critically ill patients is taken as an obvious challenge. Taken together, the role of EC-IC bypass surgery in the management of acute stroke is yet to be elucidated through future randomized clinical trials.
External to Internal Carotid Artery Flow Diversion
Cerebral flow augmentation has also been attempted using the flow diversion by temporary occlusion of the external carotid artery (ECA) in the ipsilateral brain hemisphere without incurring any brain tissue injury due to the induced hyperperfusion condition. Preclinical studies as well as case reports have indicated the efficacy and safety of CBF augmentation, making it a potentially helpful treatment for ischemic stroke and vasospasm due to SAH or traumatic brain injury. 63
Studies by Van Laar et al 64 and Divani et al 63 have proved that ipsilateral ECA occlusion contribute to increased flow in ICA in acute ischemic phase. Temporary occlusion of the ECA with balloon angioplasty can be used for the patients who are waiting for thrombolytic therapy. Ipsilateral or bilateral occlusion of the subclavian artery distal to the vertebral artery origin can be administered to augment posterior circulation. These techniques are more appropriate for strokes involving “supra” Circle of Willis vessels. 63
Retrograde Transvenous Perfusion
Retrograde transvenous perfusion (RTN) can be performed by obtaining blood from a femoral artery with an external pump and passing that blood through catheters put into the transverse sinuses of the brain. From there, the blood would pass into the veins of the brain and capillary bed. 65 The cerebral venous system can tolerate up to 150 mm Hg retrograde perfusion pressure after MCA occlusion. 66 A gradual increase in the venous pressure will yield a lower risk of intracranial HTN. 67 Moreover, it is believed that the collateral venous network is large and quite redundant and can readily handle the change in the outflow pattern that occurs when RTN forces blood through the superior sagittal sinus in a retrograde fashion. So this method will not accompany a higher risk of hemorrhagic transformation. 65
The results of study by Shimauchi et al 68 indicated that this technique adjuncted with administration of verapamil had a beneficial effect on the ischemic brain. However, free radicals usually produced by 5 to 6 hours after the onset of ischemia might not be overcome by this technique. 69 Therefore, concurrent usage of the RTN with administration of mannitol as a free radical scavenger has been advocated. 70,71
In a study on baboons, RTN demonstrated a positive effect on ischemia according to somatosensory-evoked potential, stroke scores, and infarct size. Somatosensory-evoked potentials were improved 103.3% versus 75% of baseline. Combined neurological score for 6 days in the RTN-treated group was 99.2 versus 66.4. The mean contralateral hemisphere infarction volume was 0.3 ± 0.2% versus 8.8 ± 3.1% in the control group. 69 Despite the promising results in animals and small human series, the evidence to date does not support the use of this therapy for acute ischemic stroke.
Sphenopalatine Ganglion Stimulation
Recently, excitation of the SPG has been considered as a source of vasodilatory parasympathetic innervations to the anterior cerebral circulation in animal studies, 72,73 leading to significant increase in CBF in the ipsilateral and to a lesser extent in contralateral hemisphere. 72 –74
In addition, SPG stimulation, 15-minute epoch each time after the middle cerebral artery occlusion (MCAO) in 21 rats, is shown to induce an increased regional CBF in the peri-ischemic region and reduce the infarct volume 24 hours after the treatment. However, the observation period was short. 75 Meanwhile, resection of the SPG leads to an increased infarct volume following MCAO. 76,77
Based on such findings, the “Implant for augmentation of CBF trial 1” (ImpACT-1) was designed to investigate the efficacy, safety, and tolerability of the ischemic stroke system in patients with acute ischemic stroke within 24 hours of stroke onset. This system comprises 2 parts, that is, the implantable neural stimulator and the energy delivery control system including a controller, a driver, and a transmitter.
The implantable neural stimulator is a 1-inch long system implanted via the greater palatine canal using a minimally invasive oral procedure. When inserted, the platinum–iridium electrode locates in the extracranial sphenopalatine fossa, near the SPG, and transfers the stimulation pulse to the ganglion. To activate the implant, an external driver transmits the radio frequency energy via a transmitter coil to an electronic circuit located in the proximal end of the implant. The transmitter is positioned on the patient’s cheek with a disposable sticker removed after each treatment session. The final stimulation protocol is typically a 4-hour daily session for 5 successive days. This study is still ongoing and expected to be concluded in 2014. 78
Transcranial Laser Therapy
Laser therapy may decrease the cortical ATP content loss due to embolic stroke. 79 This can be achieved through activation of the cytochrome C oxidase enzyme complex and ATP production. The above-mentioned effects are exerted via oxidative phosphorylation in mitochondria, 80 inhibition of nitric oxide synthase or inducing antioxidants formation, angiogenesis, and neurogenesis. 81
The NeuroThera Effectiveness and Safety Trial 1 (NEST-1) has investigated the efficacy and safety of the NeuroThera Laser System (Photothera, Carlsbad, California) administered within 24 hours of the onset of stroke symptoms. This setup uses the near-infrared portion of the electromagnetic spectrum with a laser wavelength of 808 nm. These low-energy (10 mW/cm2) lasers beams are applied at 20 predetermined locations on the scalp with 2 minutes of irradiation at each site. The treatment protocol lasts for 1 hour. When compared to the sham-treated patients, patients who received laser therapy demonstrated a significant recovery (NIHSS 0 to 1) with a decreased NIHSS score of at least 9 points on day 90 versus baseline. In the NEST-1 trial, no difference in safety outcomes between the cases and control groups was noted. 82
The NEST-2 trial enrolled 331 and 327 patients to receive TLT or sham treatment, respectively. Patients with the history of receiving rtPA treatment and those with hemorrhagic transformation were excluded. Although the study showed a trend toward a better outcome in the TLT group, it failed to reach statistical significance (P = .094). Nevertheless, on post hoc analysis following the exclusion of patients with the most severe strokes (NIHSS, 16-22), a statistically significant benefit favoring TLT was reported. Findings from the NEST-2 trial confirm the safety profile of TLT as reported in previous studies. Currently, the NEST-3 clinical trial is ongoing. 82,83 Compared to SENTIS trial, laser therapy has better availability although there is uncertainty regarding its exact mechanism of action.
Conclusion and Future Direction
There are theoretical physiological reasons why cerebral flow augmentation can be a good adjuvant therapy for acute ischemic stroke alone or in combination with other modalities such as intravenous thrombolysis. Unfortunately, the evidence to date is either early in the animal experimentation phase or for those already tested in large randomized clinical trials; the results have not shown a beneficial effect on primary end points. Therefore, none of these therapies can be recommended for use in the routine management of ischemic stroke. As far as priority concerns, transcranial laser therapy and partial aortic occlusion seem to be more likely to be practical in future. Randomized clinical trials are strongly recommended to investigate the efficacy and safety of these methods in all patients with ischemic stroke or special subgroups.
Footnotes
Acknowledgment
We would like to sincerely thank Dr. Afshin A Divani for critical reading of the preliminary draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.