
Abstract
In this study, lymphocyte subgroups including blood CD3, CD4, CD8, CD4/CD8, CD19, and CD16.56 values were analyzed in children with Down syndrome (DS). The study includes 85 children with DS, followed at Department of Pediatrics, Faculty of Medicine, Yüzüncü Yil University and 64 healthy age-matched control participants. Blood CD3, CD4, CD8, CD4/CD8, CD19, and CD16.56 values were examined in both the groups. Significantly decreased blood CD3, CD4, and CD19 values were found in the study group (P < .05) when compared with the control group. In conclusion, we would like to emphasize that blood CD3, CD4, and CD19 levels were found to be decreased in children with DS. Based on these finding, we think that these decreased lymphocyte subgroups might be responsible for increased susceptibility to infections in children with DS.
Introduction
Down syndrome (DS) is characterized by the presence of an extra copy of the chromosome 21 or part of it, and the most frequent chromosomal alternation. 1 The immunological defects include both specific and nonspecific immunity; however, the basis of the immune defects is still unclear. A critical point is to understand why children with DS show such a high frequency of immunodeficiency. 2 The clinical picture of DS has been associated with a combined deficiency of antibody and cell-mediated immunity. 3 Abnormal proportions of peripheral blood lymphoid subsets, cellular dysfunction, and autoimmune phenomena have also been described in patients with DS. 4 There are limited studies evaluating various arms of the immune system in patients with DS, including T cell subsets. 3
In this study, lymphocyte subgroups including blood CD3, CD4, CD8, CD4/CD8, CD19, and CD16.56 values were analyzed in children with DS. Our aim is to determine whether there was any difference for lymphocyte subgroups between children with DS and healthy children.
Materials and Methods
The study includes 85 children with DS, followed at Department of Pediatrics, Faculty of Medicine, Yüzüncü Yil University and 64 healthy age-matched control participants. A total of 85 children (48 girls [56%] and 37 boys [44%]), aged 1 to 131 months (mean 20.91 ± 26.92 months), with DS and 64 healthy children (40 girls [65%] and 24 boys [35%]), aged 1 to 96 months (mean 23.11 ± 23.40 months), were included in the study. All patients were karyotyped and had trisomy 21. CD3, CD4, CD8, CD4/CD8 ratios, CD19, and CD16.56 were studied in the lymphocyte subgroup surface antibodies in the patient and control groups. For this purpose, 2 mL of blood was added into the standard blood count tubes, which contained EDTA. Red blood cells were eliminated after they had passed through the Coulter Q-Prep device (Beckman Coulter Inc., Brea, CA, USA) together with Immunoprep solutions. Positive cell count was performed using a flow cytometer device (Coulter Epics XL) after adding 20 µL monoclonal antibodies, antihuman antiCD3 immunoglobulin (Ig) G1 (fluorescein isothiocyanate [FITC]), antiCD4 IgG1 (FITC), antiCD8 IgG1 (phycoerythrin [PE]), antiCD16 IgG1 (PE), antiCD19 IgG1 (PE) and antiCD56 IgG1 (PE) into a 100-µL solution that contained mononuclear cells. Immunoglobulin G1-type antibodies were used for control samples.
In the statistical analysis, 1 sample Kolmogorov-Smirnov test was used to analyze groups for distribution, and Student independent t test was used to compare the groups. Data were given as mean ± standard error. A P value of <.05 was considered as a significant.
Results
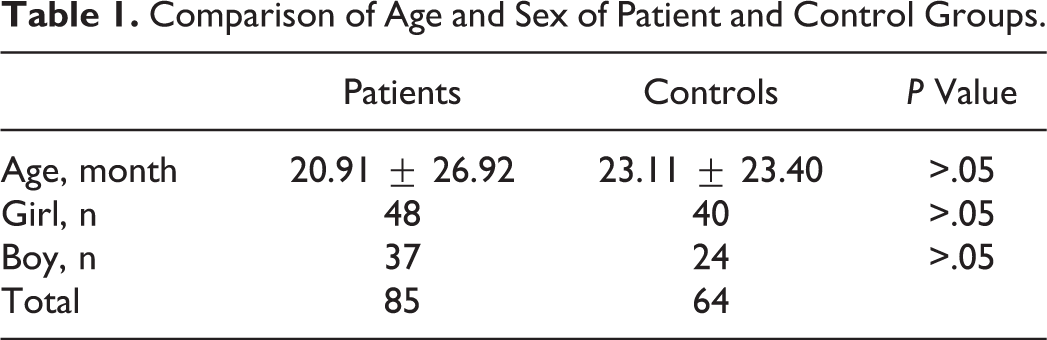
A total of 85 children with DS who were between 1 and 131 months (mean 20.91 ± 26.92 months) were enrolled into the study. Of the 85 children, 48 (56%) were girls while 37 were boys (44%), and the girls–boys ratio was 1.3. The ages of 64 children in the control group varied between 1 and 96 months (23.11 ± 23.40 months). Of the 64 children, 40 (65%) were girls and 24 (35%) were boys. No statistically significant difference for age or sex was found between the patient and the control groups (P > .05; Table 1).
Comparison of Age and Sex of Patient and Control Groups.
Of these patients, all of them have development delay, joint laxity, hypotonia, 45 (52.9%) had short stature, 44 (51.7%) had strabismus, 34 (40%) had congenital heart disease, and 1 (1.1%) had micropenis. Hypothyroidism was found in 2 patients. Of the patients with DS and congenital heart disease, ventriculer septal defect was found in 11 (12.9%) patients, atrioventricular septal defect in 7 (8.2%) patients, atrial septal defect in 7 (8.2%) patients, patent ductus arteriosus in 5 (5.8%) patients, and tetralogy of fallot in 4 (4.7%) patients.
Table 2 demonstrates CD surface antibody ratios in patient and control groups. When compared with the control group, significantly decreased blood CD3, CD4, and CD19 values were found in the study group (P < .05). However, there was no significant difference in CD8, CD4/CD8, and CD16.56 values between the control and the study groups (P > .05).
Comparison of the Proportion of Lymphocytes Expressing Surface Antibody Markers in Peripheral Blood of Patient and Control Groups.
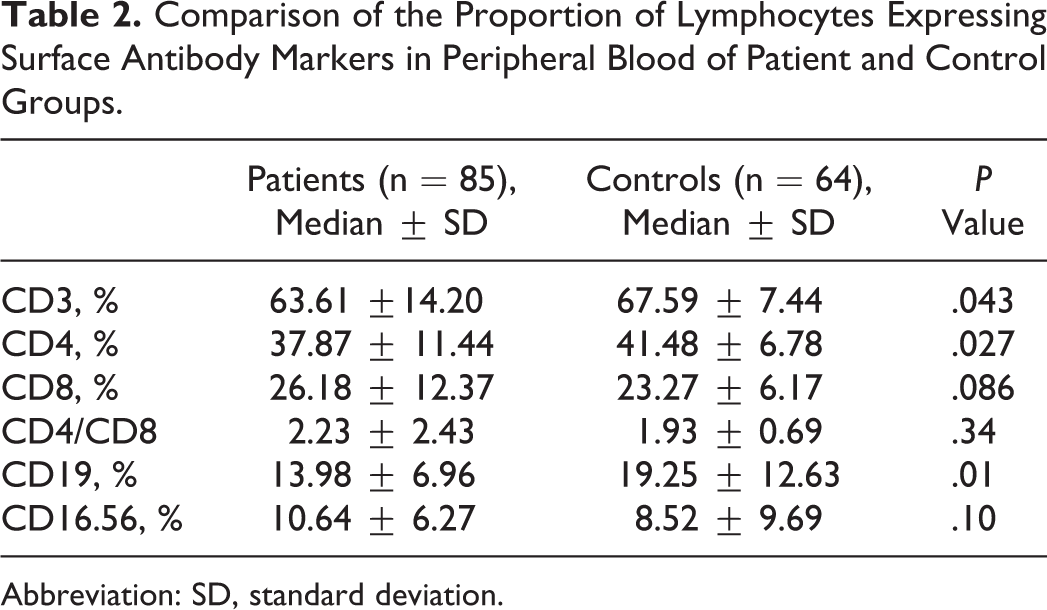
Abbreviation: SD, standard deviation.
Discussion
Down syndrome is an important genetic anomaly, and this syndrome still constitutes a relevant health care problem with relatively high cost of medical expenditures, because mental retardation, endocrine, cardiovascular, and immune defects are frequently associated with the syndrome. 5,6 The increased susceptibility to infections, due to the deficiency of the immune system, has been well known for many years. 7
The thymus is smaller in patient with DS, even in newborn, and has an abnormal structure. 8 The DS thymus shows a decreased proportion of phenotypically mature thymocytes expressing high level of the α-β form of the T-cell receptor and associated CD3 molecule and overexpression of tumor necrosis factor α and interferon γ cytokines. 9,10
Patient with DS present a precocious aging of the immune system with several alterations including, among others, alterations of B and T lymphocyte subsets and natural killer cells, defective phagocytosis, and chemotaxis of polymorphonuclear leukocytes. Studies on peripheral blood subsets in children with DS revealed a reduction, often quite small, in the absolute number of T lymphocytes and abnormal proportions of different T cell subpopulation. 11
Recent observations even show a significant decrease in B lymphocytes (CD19) in fetuses with DS. 12 These abnormalities can be due to either an intrinsic B lymphocyte defect or the consequence of deficient T-helper lymphocyte function causing inadequate control of B lymphocyte activation and proliferation. 13
In a study which was conducted by Burgio et al, 14 the percentage of circulating T cells forming rosettes with sheep erythrocytes, either in the presence or in the absence of fetal calf serum in children with DS, was found to be significantly lower than in appropriately matched controls. In contrast, the percentage of T cells forming rosettes with human erythrocytes was significantly higher in children with DS than in controls. Finally, the author suggested that these data support the hypothesis that a defective T-cell maturation is an early integral feature of DS. 14
Bertotot et al designed a study to investigate the lymphocyte surface phenotypes in patients with DS. They analyzed the lymphocyte surface phenotypes in the blood of 7 noninstitutionalized adults with trisomy 21 and in 10 karyotypically normal control participants by fluorescent microscopy. They found that the proportions of CD3, CD4, and CD6 levels were similar in the 2 groups, and the percentages of both CD8 and CD10 positive trisomic lymphocytes were significantly higher. They finally indicated that these findings were defined as biological implications of the underlying immunopathology in DS. 15
In another study, which include comparing of peripheral blood mononuclear cells from children with DS and who were less than 6 years of age with cells from age-matched controls, it was found that the children with DS had reduced numbers of circulating CD4+ T cells and a significantly depressed ratio of CD4+ to CD8+ T cells. In conclusion, the authors told that these findings provided evidence that the primary immune defect in DS was in part a depressed number and function of helper T cells. 16 On the other hand, Licastro et al investigated immune defects in 43 children with DS. They detected decreased peripheral CD4+T lymphocytes, increased CD3/HLA-DR-positive cells, large granular lymphocytes (CD16/CD56 positive cells), and higher plasma interleukin 6 levels in children with DS compared to controls. 5
In a study conducted by Raziuddin et al, CD45R+, CDW29+, CD4+, and CD8+ levels were evaluated in 19 children with DS. They observed a marked increment in percentage of CD4+ CD45R+ cells (suppressor inducer) and decrement in CD4+ CDW29+ cells (helper/inducer) in all patients with DS according to controls. So they denoted that a deficiency exists in patients with DS in the CD4+ CDW29+ helper/inducer T-cell subset, which may contribute to their impaired cell-mediated immunity. 6
In another study, plasma zinc levels, CD4, CD4/CD8 ratios, and CD19 levels were evaluated in 43 children with DS and 40 normal children; increment in CD8 level according to the control group and decrement in plasma zinc levels were detected in the DS group. It indicated about immune defects of children with DS; zinc level is not only etiologic cause, thymic changes and gene overexpression-related molecular abnormality localized on chromosome 21 locus may also have role. 17
In a study in which 15 children with DS were included, significant decrement in absolute number of CD4+cells, significantly increment in CD8+cells’ percentage, and a decrement in the activity of CD57, CD16, and CD56 natural killer were detected, and as a result decreased endocrine activity in children with DS may be responsible for thymic T cells and natural subgroups. 18
Nespoli et al designed a normal proportion of CD4+ T cell but a marked imbalance in the CD+ subpopulations, whereas the percentage of suppressor-cytotoxic CD8+ lymphocytes is markedly increased. 19 On the contrary, Corsi et al showed that peripheral CD4+ T cells were lover in children with DS, whereas mean values of cytotoxic CD8+ T cell were comparable with those of healthy children. 20
When compared with the control group, the present study found significantly decreased blood CD3, CD4, and CD19 values in patient with DS (P < .05). However, there was no significant difference in CD8, CD4/CD8, and CD16.56 values between the control and the patients with DS (P >.05).
Our study suggests that there are abnormalities involved in both T cell and B cell of the immune response, in children with DS. They finally indicated that the findings of reduced lymphocytes subgroups that carry CD3, CD4, and CD19 values may be defined as biological implications of the underlying immunopathology in DS. Further studies are need to lighting the underlying mechanisms of this immunopathology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.