
Abstract

Venous thromboembolic events (VTEs) are life-threatening complications in patients with cancer and remain the second most common cause of death in hospitalized patients with cancer, after death from cancer itself. 1 Patients with breast cancer, however, are considered to be at relatively low risk of developing VTE. 2 In a cohort of 108 255 patients with breast cancer, the 1- and 2-year cumulative incidence of VTE was estimated to be 0.9% and 1.2%, respectively. 3 Both chemotherapy in general and the agent used in particular were found to increase the risk of developing VTE. A systematic screening for thrombosis during anthracycline-based regimens in adjuvant settings revealed a higher VTE (10%) 4 rate when compared to the conventional cyclophosphamide methotrexate fluorouracil therapy (5.4%). 5 The route of application of chemotherapeutic agents represents another high risk factor for the development of VTE. Catheter-related thrombosis (CRT) involves 70% to 80% of all upper extremity thrombotic events and represents about 10% of all cases of VTE in patients with cancer receiving chemotherapy. 6 The role of acquired thrombophilia such as the induction of antiphospholipid antibodies (aPL-abs) and lupus anticoagulant (LAC) in the pathogenesis of VTE in patients with breast cancer has been reported but is still a matter of debate.
In a prospective, case-controlled study, we assessed the rate of symptomatic VTE in primary nonmetastatic, patients with breast cancer who received adjuvant anthracycline-based chemotherapy regimens postoperatively via an intravenous port-catheter device (Hickman port, Celsite® Access Port venous low-profile composite access ports with titanium chamber, Braun Melsungen AG, Germany). The standard combination administered every 3 weeks and for 6-treatment cycles was as follows: cyclophosphamide 500 mg/m2, doxorubicin/epirubicin 15 mg/m2, and flurouracil 1000 mg/m.
2
Prior to primary surgery and each of the 6 cycles of chemotherapy, laboratory tests for anticardiolipin antibodies (aCL-ab; immunoglobulin [Ig] G-, IgM-enzyme-linked immunosorbent assay [ELISA] >15 U/mL), LAC (partial thromboplastin time ratio > 1.2), resistance to activated protein C (APC, Coatest; Chromogenix, Mölndal, Sweden; APC ratio < 2.0), and
Over a period of 1.5 years, 42 patients with breast cancer (age: 60.6 ± 7.5 years) were recruited; 49 age-matched healthy women served as controls (age: 59.0 ± 11.2 years; P = .41).
In the study period, 7.2% of the patients with breast cancer (n = 3) developed symptomatic VTE, which were all localized in the subclavian vein at the side of the port-catheter. All of them occurred after the first chemotherapy cycle and were proven by contrast phlebography. Low-molecular-weight heparin at therapeutic dose was initiated and continued until removal of the device after the sixth cycle of chemotherapy. Symptomatic thrombosis of the pelvic veins, lower extremities, or in other regions was not detected in any of the patients during the study period. Test results for aCL-ab (Figure 1A and B) and LAC were negative in all of the patients, prior to surgery, prior to the start of chemotherapy, and prior to each cycle of chemotherapy. In one of the controls, however, aCL-ab was elevated, but her medical history was uneventful, and there were no clinical signs of thrombosis.
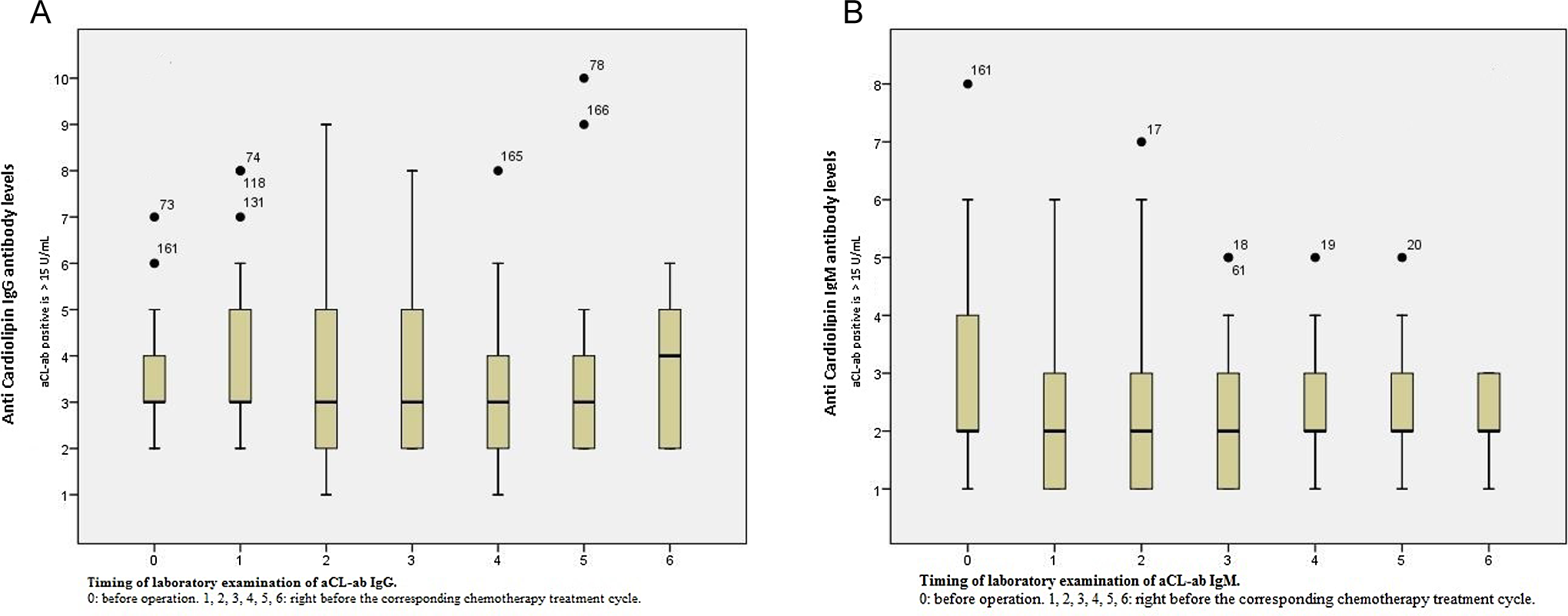
A, Box plot showing the aCL-ab IgG levels before the breast operation and before each of the treatment cycles. Dots: outliers. B, A box plot showing the aCL-ab IgM levels before the breast operation and before each of the treatment cycles. Dots: outliers. aCL-ab indicates anticardiolipin antibody; Ig, immunoglobulin.
Mean
None of the patients included in the present study had elevated aPL-absat the time of primary diagnosis of breast, and we did not detect any increase in aCL-ab or LAC concentrations in the follow-up during the chemotherapy cycles. We therefore assume that the induction of aCL-ab or LAC—in the sense of an acquired thrombophilia—is an infrequent phenomenon in patients with breast cancer receiving standard anthracycline-based chemotherapy.
The 7.2% incidence of CRT in our cohort is comparable to that described in 1 study 6 but contrary to others. 7,8 Zuckerman et al reported that 22% of the patients presenting with malignancies in their cohort showed elevated aCL-ab concentrations, compared with 3% in the control group without malignancies. Moreover, the aCL-ab-positive patients had a significantly higher rate of VTE than aCL-ab-negative patients. Interestingly, the levels of aCL-ab decreased after successful treatment in 4 patients who remained free of thrombotic events thereafter. 7 In a systematic review, Gómez-Puerta et al concluded that the increase in aCL-ab occurs in a wide range of different malignancies and that they decrease in more than one-third of the patients after cancer treatment. 8 The APC resistance, either acquired or inherited (factor V Leiden mutation), was also incriminated as a possible cause of VTE in patients with cancer. Haim et al found that the prevalence of acquired functional APC resistance was significantly higher in patients with cancer who developed VTE. They concluded that resistance to APC is a risk factor for VTE and that acquired functional APC resistance is a common finding in patients with cancer having venous thromboembolism while the factor V Leiden mutation was unusual. 9 These results are contradictory to our findings. We observed that none of our patients developed symptomatic VTE elsewhere apart from CRT, and this made us to believe that most likely the mechanisms inducing CRT are different from those causing pelvic or lower extremities thrombosis; therefore, the coagulation tests as used in this study may be inappropriate to predict CRT.
Nijziel et al reported an increased resistance to APC in 56 patients with node-positive breast cancer 1 year or more after chemotherapy in comparison with 28 healthy control participants. 10 In our cohort, we could not find any elevation in APC resistance before and during chemotherapy both in patients affected with VTE and those who were not. It is worth mentioning that no other breast cancer study relating to the course of functional acquired thrombophilia (APC resistance and aPL-ab) during chemotherapy considering the development of VTE has been published yet.
From our results and through comparing them to the published relevant literature, we conclude that an increase in aCL-ab, LAC, hence antiphospholipid syndrome, and functional resistance to APC as well are infrequent events in patients with breast cancer receiving adjuvant anthracycline-containing chemotherapy combination, even in those patients who developed port-catheter thrombosis.
Footnotes
Authors’ Note
A. A. Soliman contributed to the concept and design of the study, shared in the data collection and its statistical analysis as well and shared in the critical writing of the manuscript; R. Csorba shared in the literature search and critical writing of the manuscript; A. Ullrich took a main part in the data collection, tabulation and statistical analysis; P. Tsikouras shared in the statistical analysis of the data and putting the manuscript in its final form to be published; W. Rath contributed to the search of literature and to the final revision of the intellectual content; and finally, G.-F. von Tempelhoff contributed substantially to the concept and design of the study, shared in the statistical analysis, and gave approval to the final version of the manuscript to be published.