
Abstract

General Considerations
The periprocedural management of patients requiring temporary interruption of vitamin K antagonists (VKAs) such as warfarin due to an elective invasive procedure or elective surgery is a common clinical problem. 1 In North America alone an annual estimate of 250 000 patients who are receiving antithrombotic therapy will be assessed for an elective surgical or invasive procedure. 2 Management of these patients is difficult due to the risk of bleeding when antithrombotic therapy is administered in close proximity to an invasive procedure or surgery versus the risk of thromboembolism if antithrombotic therapy is interrupted. A careful bleeding and thrombotic risk assessment should be performed in the individual patient undergoing a specific procedure to determine (1) whether interruption of antithrombotic therapy is needed in the periprocedural period and (2) whether bridging anticoagulation is needed among those patients requiring temporary interruption of antithrombotic therapy. Bridging anticoagulation can be defined as the use of short-acting parenteral anticoagulants such as unfractionated heparin (UFH) or subcutaneous (sc) low-molecular-weight heparin (LMWH)—usually in therapeutic doses—in the pre- and postprocedural period to maintain an anticoagulant effect during temporary interruption of VKA when the international normalized ratio (INR) is subtherapeutic.
The impact of major bleeding in the periprocedural period is greater than previously thought and may be associated with significant morbidity and a case-fatality rate of up to 9%. 3 Moreover, postoperative bleeding delays resumption of antithrombotic therapy, thereby placing patients at risk of thromboembolism. 4 Bleeding risk assessment involves considerations of patient- and procedure-related risk factors for bleeding. For the patient, factors such as a history of prior bleeding, especially prior periprocedural bleeding, or the use of multiple antithrombotic drugs may place that patient at higher risk for bleeding. Although there is no validated procedure-related bleeding risk score, it is helpful to characterize procedures into a 2-tiered risk scheme of high- and low-bleed risk in developing a periprocedural management strategy. High bleeding risk procedures include most major operations lasting >45 minutes, vascular procedures, major orthopedic procedures, cardiothoracic procedures, extensive cancer surgery, and prostate or bladder surgery. 5 In addition, invasive procedures such as resection of colonic polyps, prostate, liver, or kidney biopsy, or pacemaker or defibrillator implantation may place the patient at increased risk of bleeding or significant pocket hematomas.6,7 Most operations lasting <45 minutes or minor invasive procedures including diagnostic gastrointestinal procedures, dermatological and dental procedures, or ophthalmologic procedures carry a low bleeding risk. 8
Thrombotic risk assessment should account for the estimated risk of arterial thromboembolism or venous thromboembolism (VTE) and include procedural-related risks. A thrombotic risk assessment is based on the 3 most common indications for VKA therapy (mechanical heart valve [MHV], atrial fibrillation (AF) or VTE, and patients may be classified into a high, moderate, and low VTE risk groups (Table 22.1). Although an increased risk of VTE in the postoperative setting has been well documented, there are emerging data suggesting up to a 10-fold increased risk of arterial thromboembolism (compared to the risk derived from mathematical modeling) in the perioperative setting, especially among patients undergoing major surgery. 9
American College of Chest Physicians: Suggested Risk Stratification for Perioperative Thromboembolism. 5
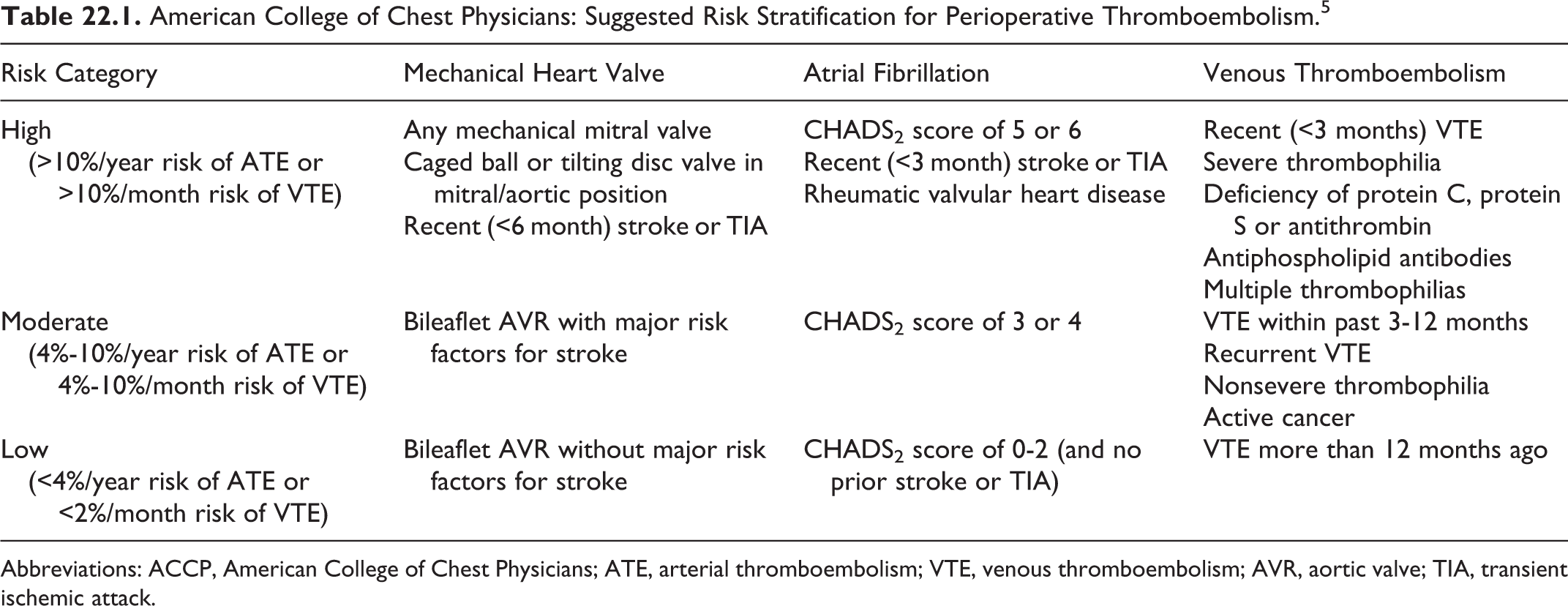
Abbreviations: ACCP, American College of Chest Physicians; ATE, arterial thromboembolism; VTE, venous thromboembolism; AVR, aortic valve; TIA, transient ischemic attack.
An overall risk assessment of bleeding and thrombotic risk factors for arterial thromboembolism or VTE should be made taking into account both patient-related and procedure-related factors in order to develop a periprocedural antithrombotic strategy. The case fatality of a major bleed is approximately 8% to 9%, an embolic stroke is associated with a case fatality or permanent major neurologic defect approaching 70%, and thrombosis of a heart valve can lead to fatality 15% of the time.3,10,11 For VTE, the case fatality is approximately 5% to 9%. 3 Finally, it appears that an INR >3.0 at the time of surgery may confer a higher risk for bleeding complications (odds ratio 1.6; 95% confidence interval: 0.4-4.0). 12
Periprocedural Management of Patients Undergoing Minor Procedures
Minor dental, dermatological, or ophthalmological procedures comprise approximately 20% of the procedures in patients receiving VKA. 5 Randomized trials and prospective cohort studies indicate that patients who continue VKA during dental extraction, especially with coadministration of antifibrinolytic drugs such as tranexamic acid mouthwash, had similar rates of major and clinically significant nonmajor bleeding (<5%) and rare thromboembolic events (<1%), as did patients who discontinued VKA.13–15 Partial interruption of VKA 2 to 3 days prior to a dental procedure has also been associated with low bleed risk. 16 In addition, prospective cohort studies in patients undergoing dermatological and ophthalmological procedures (specifically cataract extraction) showed a low incidence of major bleeding and support the notion that VKA can be continued around the time of certain minor procedures.17–19
Interruption of VKA and Bridging Anticoagulation
Basic principles for patients receiving VKA who require temporary interruption and bridging anticoagulation with parenteral UFH or LMWH are as follows:
For patients undergoing a high-bleeding risk procedure or surgery where there is intent to minimize the antithrombotic effect of VKA in the preprocedural period, approximately 5 days of interruption of warfarin is needed, based on a half-life of approximately 36 to 42 hours.
16
In elderly patients or patients on a longer lasting VKA such as the less widely used phenprocoumon (with a half-life of 96-140 hours), longer periods of interruption may be necessary.
20
There appears to be a detectable residual anticoagulant effect, as measured by anti-FXa ≥ 0.10 IU/mL, if therapeutic dose LMWH is given within 12 hours of the start of the procedure.
21
Preoperative administration of low-dose vitamin K orally (1-2.5 mg) in patients with an elevated INR (≥1.5) does not appear to be associated with resistance to reanticoagulation when VKA is resumed after surgery.
22
Current global coagulation tests such as the activated partial thromboplastin time, prothrombin time, and heparin anti-FXa level are likely to be inadequate to measure the dual anticoagulant effects of both VKA and heparin in the periprocedural period, while other emerging tests such as the thrombin generation assay may have improved sensitivity in detecting the global anticoagulant effects of both LMWH and VKA.
23
In the postprocedural period, administration of antithrombotic therapy at close proximity to the procedure or at therapeutic versus prophylactic doses may increase the bleeding risk. Therefore, in high bleeding risk procedures, delaying resumption of bridging therapy (for 48-72 hours after the procedure), decreasing the dose of bridging therapy (ie, prophylactic dose), or avoiding postprocedure bridging anticoagulation may decrease the risk of bleeding.
24
There is no evidence that nontherapeutic dose bridging anticoagulation with UFH or LMWH is effective for preventing arterial thromboembolism.
25
Periprocedural discontinuation and reinitiation of VKA and use of heparin bridging therapy should be based on an explicit, evidence based, and standardized protocol with careful consideration of patient and procedural risk factors for thrombosis and bleeding.
26
There are substantial cost savings with the use of LMWH as bridging therapy due to facilitation of management in an outpatient setting compared to intravenous UFH used inhospital.
27
Bridging Anticoagulation in Patients With a MHV, AF, or VTE Receiving VKA
There are multiple prospective cohort studies in which bridging anticoagulation has been assessed in patients with a MHV that included patients with aortic, mitral, or dual position MHVs as well as a minority of patients with older, caged-ball MHVs. The majority of these studies included therapeutic-dose LMWH regimens (ie, enoxaparin 1 mg/kg sc twice daily or 1.5 mg/kg once daily, dalteparin 100 IU/kg twice daily, or 200 IU/kg once daily) and none had control groups without bridging therapy. The pooled perioperative arterial thromboembolism event rate was low (~1%), with no reported episodes of MHV thrombosis, and the overall rate of major bleeding was ~3%.4,28–31 One recent study of 172 patients with prosthetic heart valves on chronic VKA needing temporary interruption for an elective procedure or surgery found one arterial thromboembolic event and an overall adverse event rate of 5.5% using mostly outpatient-based treatment dose LMWH as bridging therapy. 28
Some recent cohort studies have assessed intermediate-dose LMWH as bridging therapy (ie, 70 anti-Xa IU/kg twice daily) with low thromboembolic and bleed rates. 32 The incidence of thromboembolic events with older studies using intravenous UFH as bridging therapy found more variable arterial thromboembolic event rates. 33 Mathematical modeling of a patient with a MHV not treated with a VKA in the periprocedural period is estimated at 0.046% per day (17% annual risk divided by 365 days) or approximately 0.4% for 8 days. The finding of a higher arterial thromboembolic event rates in bridging studies suggest a higher than expected risk.
There are also prospective cohort studies in which mostly therapeutic dose LMWH bridging anticoagulation was assessed in patients with AF.4,24,29,30,34 The pooled risk of perioperative arterial thromboembolism was also approximately 1%. Most patients described in such studies had at least 1 additional stroke risk factor as per CHADS2 criteria. There are reports that collectively describe an arterial thromboembolic event rate of approximately 1% in patients with permanent AF that did not receive bridging anticoagulation, which is higher than mathematical modeling predicts (ie, approximately 0.1% for 8 days, 5% annual risk divided by 365 days). 35 More recent larger studies have included intermediate dose LMWH bridging regimens with good outcomes in patient populations that have included patients with AF.32,36,37
There is a need for placebo-controlled studies in VKA-treated patients with MHV or AF indications for warfarin to obtain strong evidence for efficacy and safety of bridging anticoagulation in the periprocedural period. Toward this end, the PERIOP-2 (clinicaltrials.gov/NCT00432796) and BRIDGE (clinicaltrials.gov/NCT00786474) studies have been initiated and are actively enrolling VKA-treated patients who require elective surgery and will be randomly allocated to bridging or no bridging regimens.
Multiple prospective cohort studies have evaluated bridging anticoagulation with therapeutic-, intermediate-, or low-dose regimens of various LMWHs in patients with VTE.24,29,34,36,38 The pooled risk of recurrent symptomatic VTE was low (<1%). These studies did not include control groups.
There are no clinical data available to optimize periprocedural administration of the novel small molecule antithrombotic agents such as the direct thrombin inhibitor dabigatran and direct anti-FXa inhibitor rivaroxaban. However, the pharmacological properties of these agents with their relatively short half-lives have the potential to eliminate the need for bridging therapy. Perioperative guidelines for the use of these agents based on their pharmacokinetic and pharmacodynamic properties have been suggested.39–41 Dabigatran (with its mostly renal elimination) can be discontinued 24 hours before a low-bleed risk procedure and approximately 2 to 4 days before a high-bleed risk procedure in patients with a creatinine clearance (CrCl) >50 mL/min. 40 In patients with moderate renal insufficiency (CrCl 30-50 mL/min), dabigatran should be discontinued at least 2 days before a low-bleed risk procedure and 4 days before a high-bleed risk procedure, respectively. As rivaroxaban is not predominately cleared by renal elimination, it can be stopped approximately 24 hours before a procedure in most circumstances. 39 Resumption of therapy for both agents can occur within 24 hours after low-bleed risk procedures and approximately 48 to 72 hours after high-bleed risk procedures. 39 Prospective cohort studies with dabigatran in the periprocedural period have recently been initiated.
Recommendations
In patients undergoing minor dermatological and ophthalmological procedures (specifically cataract extraction) and receiving VKA, continuing VKA around the time of procedure should be considered (level of evidence: low). For dental procedures, consider coadministration of an oral prohemostatic agent (tranexamic acid) while continuing VKAs (level of evidence: moderate). Another option in patients undergoing dental procedures includes stopping VKA 2 to 3 days before the procedure (level of evidence: low).
In patients undergoing a high-bleeding risk procedure or surgery, discontinuation of VKA (warfarin) approximately 5 days prior to allow adequate time for the INR to normalize is indicated (level of evidence: moderate). In patients who are receiving therapeutic-dose LMWH as bridging therapy, the last dose should be administered 24 hours before the procedure or surgery at approximately half the total daily dose (level of evidence: low). For intravenous UFH, we suggest stopping approximately 4 hours prior to the procedure or surgery (level of evidence: low). In patients whose INR is still elevated 1 to 2 days before the procedure (INR ≥ 1.5), consider administering low dose (1-2.5 mg) oral vitamin K to normalize the INR (level of evidence: low). In patients undergoing a minor invasive or surgical procedure, bridging anticoagulation with LMWH should be resumed within 24 hours after the procedure if there is adequate hemostasis (level of evidence: low). In patients undergoing major surgery or high-bleeding risk procedures, consider 1 of 3 options (1) delay LMWH approximately 48 to 72 hours after surgery until hemostasis is achieved; (2) administer low-dose LMWH (usually within 24 hours after a procedure); or (3) avoid postprocedural bridging therapy altogether (level of evidence: low). The LMWH should be used in the outpatient setting as bridging therapy over inhospital
In patients with MHV and AF at high arterial thromboembolic risk or patients with VTE at high VTE risk, bridging therapy with LMWH or UFH in the periprocedural period during temporary interruption of VKA should be considered (level of evidence: low). The LMWH should be preferred over UFH. In patients at moderate arterial thromboembolic or VTE risk, assessment of individual patient- and surgery-related factors should be considered over a standardized approach on whether to use bridging therapy (level of evidence: low). In patients at low arterial thromboembolic or VTE risk, no bridging over bridging therapy should be considered (level of evidence: low). In all patients undergoing major procedures or operations for which there are international guideline recommendations for VTE prevention in the postoperative period, an appropriate prophylactic agent should be used during reinitiation of VKA if postoperative heparin bridging is not used (level of evidence: moderate).