
Abstract

The Risk
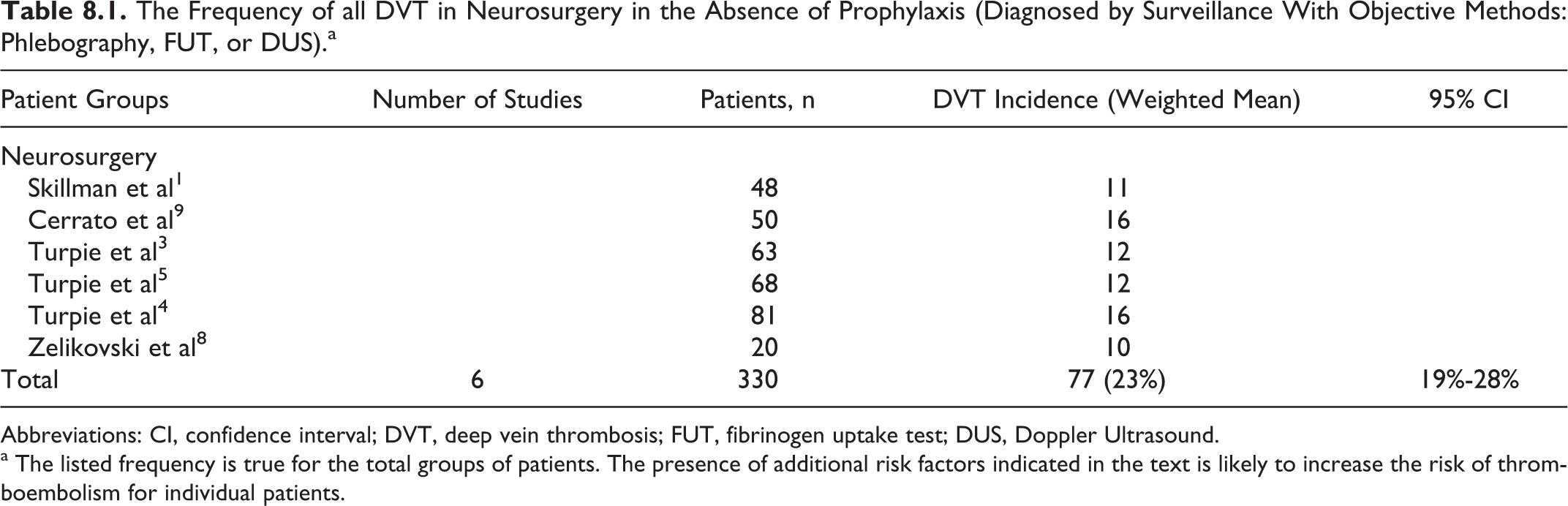
In the absence of prophylaxis, the incidence of asymptomatic deep vein thrombosis (DVT) in the 1970s and 1980s detected by the fibrinogen uptake test (FUT) was approximately 23%, with proximal thrombosis found in 5% (Table 8.1).1–9 The prevalence of DVT after neurosurgery is high (5 [13.5%] of 37), even when graduated elastic compression (GEC) is used. 10 The risk is particularly high (21%-32%) in patients with glioma11–16 and persists for a year or more. 11
The Frequency of all DVT in Neurosurgery in the Absence of Prophylaxis (Diagnosed by Surveillance With Objective Methods: Phlebography, FUT, or DUS).a
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; FUT, fibrinogen uptake test; DUS, Doppler Ultrasound.
a The listed frequency is true for the total groups of patients. The presence of additional risk factors indicated in the text is likely to increase the risk of thromboembolism for individual patients.
Prophylactic Methods and Recommendations
General Considerations
In a randomized controlled study involving 161 patients, intermittent pneumatic compression (IPC) reduced the incidence of silent DVT from 23.5% in the no prophylaxis group to 1.5% in the test group (risk ratio [RR] 0.07; 95% confidence interval [CI] 0.009-0.49). 3 This efficacy was confirmed by a second study involving 95 patients where the incidence of silent DVT was reduced from 25% to 8.3% (RR 0.33; 95% CI 0.11- 0.94). 1 In a third randomized-controlled trial (RCT), IPC combined with GEC reduced the incidence of silent DVT from 20% in the control group to 9% in the treatment group (RR 0.45; 95% CI 0.20-1.04). 4 In a recent RCT 17 involving 150 patients, the efficacy of calf compression using a new mechanical device plus GEC reduced the incidence of asymptomatic DVT to 4% compared to 18.7% in the control group that had GEC only (RR 0.21; 95% CI 0.05-0.75). In addition, it reduced proximal DVT from 8.0% to 2.7% and symptomatic DVT from 2.7% to 0%.
An RCT involving 100 patients compared low-dose unfractionated heparin (LDUH) with no prophylaxis. 9 The incidence of DVT was reduced from 34% in the control group to 6% in the heparin group (RR 0.18; 95% CI 0.05-0.56). There was no increase in hemorrhagic complications. A second similar RCT failed to show efficacy but confirmed the safety shown by the first study. 18
Two large RCTs involving 604 evaluable patients compared the effect of adding low-molecular-weight heparin (LMWH) to GEC.19,20 The LMWH with GEC was more effective than GEC alone in reducing venographic DVT (17.9% vs 28.9%; RR 0.62; 95% CI 0.46-0.84), and it also reduced proximal DVT/pulmonary embolism (5.7% vs 12.0%; RR 0.48; 95% CI 0.27-0.83). The incidence of major hemorrhage was 3.4% in the LMWH plus GEC group and 2.0% in the GEC group (RR 1.73; 95% CI 0.64-4.71).
In a prospective double blind clinical trial, 150 patients undergoing craniotomy for brain tumor were randomized to LDUH or LMWH (enoxaparin) in addition to GEC and IPC in both the groups. Symptomatic VTE did not occur, but there was a 9.3% incidence of asymptomatic DVT, equal in both the groups and mostly confined to the calf. 21
An early meta-analysis of 4 randomized controlled studies (827 patients), 3 of which involved LMWH and 1 LDUH, demonstrated reduction in the incidence of all DVT from 29.0% in the control group to 15.6% in the heparin group (RR 0.54; 95% CI 0.41-0.70) and a reduction in proximal DVT (2 studies; 616 patients) from 12.5% to 6.25% (RR 0.50; 95% CI 0.30-0.84). 24 Major hemorrhage increased from 2.5% to 3.1% (RR 1.23; 95% CI 0.60-2.53). Overall bleeding increased from 2.9% to 5.9% (RR 2.0; 95% CI 1.09-3.67). Thus, the number needed to treat for VTE was 7.7 and the number needed to harm was 102.
Another meta-analysis of 18 RCTs performed in 2008 showed that LMWH or IPC devices were effective in reducing DVT (LMWH: RR 0.60; 95% CI 0.44-0.81; IPC: RR 0.41; 95% CI 0.21-0.78). 22 However, the pooled rates of intracranial hemorrhage and minor bleeding were higher in the heparin therapy group (2.1% with heparin vs 1.1% with mechanical methods).
A recent meta-analysis performed in 2011 reported results of 6 RCTs involving 1170 patients undergoing elective cranial neurosurgery. The pooled RR was 0.58 (95% CI 0.45-0.75) in favor of heparin. Intracranial hemorrhage was more common in those receiving heparin, but this was not statistically significant. For every 1000 patients who received heparin prophylaxis, 91 venous thromboembolism (VTE) events were prevented (approximately 35 of which were proximal deep vein thrombosis or pulmonary embolism and 9-18 of which were symptomatic), whereas 7 intracranial hemorrhages and 28 more minor bleeds occurred. The authors concluded that heparin prophylaxis for patients undergoing elective cranial neurosurgery reduces the risk of VTE but may also increase bleeding risks with a ratio of serious or symptomatic VTE relative to serious bleeding that is only slightly favorable. 23
Recommendations
Recommendations for prophylaxis in this group consist of the use of IPC in all patients with or without GEC stockings (level of evidence: high). Addition of LMWH is associated with an increase in efficacy (level of evidence: high). However, the use of, and timing of, LMWH administration should be individualized because of increased risk of bleeding.