
Abstract

The Risk
There is a spectrum from mild to severe risk of venous thromboembolism (VTE) in patients with burns. All ages are represented although the risk is higher after the age of 50 and in females. 1 Some patients have additional injuries to other organs or comorbid diseases requiring a multidisciplinary approach and intensive care. The incidence of deep vein thrombosis using routine screening with duplex scanning in the absence of prophylaxis varies between 6% and 27% (Table 7.1).2–5 Symptomatic VTE occurs in 0.2% to 7.0% of patients.3,6,7
The Frequency of all DVT in Trauma, Surgery, and Medical Patients in the Absence of Prophylaxis (Diagnosed by Surveillance With Objective Methods: Phlebography, FUT, or DUS).a
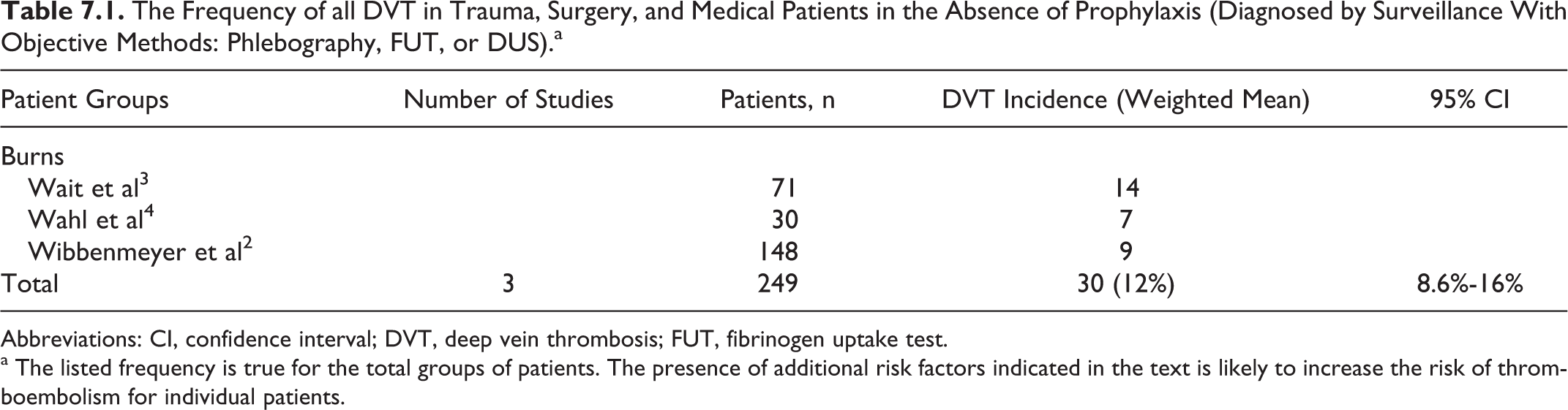
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; FUT, fibrinogen uptake test.
a The listed frequency is true for the total groups of patients. The presence of additional risk factors indicated in the text is likely to increase the risk of thromboembolism for individual patients.
Prophylactic Methods and Recommendations
General Considerations
A recent survey in the United States showed that most centers used VTE prophylaxis, mostly in the form of combined mechanical (intermittent pneumatic compression) and low-dose unfractionated heparin (LDUH) prophylaxis. 8 Faced with the lack of evidence-based data, prophylaxis has to be individually assessed as it is in multiple injured patients. Therefore, recommendations for patients with burns are extrapolated from the latter group of patients.
In view of the potential renal impairment associated with burns, a low-molecular-weight heparin (LMWH) that is eliminated mainly through the liver (eg, dalteparin) is preferable.
Recommendations
The LDUH or LMWH (level of evidence: low) should be initiated as soon as it is considered safe to do so and continued for as long as the patient remains at risk (level of evidence: low). For patients at high risk of bleeding, mechanical thromboprophylaxis with graduated elastic compression and intermittent pneumatic compression is recommended (level of evidence: low) if the burns do not involve the lower limbs. Foot impulse technology is an alternative (level of evidence: low).