
Abstract

General Considerations
Timing of Prophylaxis
Venous thromboembolism (VTE) prophylaxis involves a balance of risks and benefits. Chemical prophylaxis poses a dilemma, as the closer it is administrated to surgery for a given dose, the better the thromboprophylaxis but the greater is the risk of bleeding complications. 1 In Europe, low-molecular-weight heparin (LMWH) is given at a lower dose prior to operation providing an anticoagulant effect to counteract the intraoperative activation of coagulation factors and venous stasis. However, if a given dose of the drug is administered too long before surgery, then, intraoperative blood levels would be inadequate for effective prophylaxis, whereas if given too close to surgery then surgical bleeding is a threat. In North America, LMWH is given after surgery at a higher dose and more frequently. This should reduce the risk of surgical bleeding, yet intraoperative thrombogenesis is not prevented and thrombi may have already begun forming. The drug is now expected to be therapeutic as well as prophylactic. Therefore, prophylaxis needs to be given close but not too close to surgery.2,3
Intermittent pneumatic compression (IPC) and foot impulse technology (FIT) sleeves are available in sterile packages that allow for intraoperative use, reducing both the risk of bleeding and the duration that the patient is not under LMWH prophylaxis.4–6
Spinal and Epidural Anesthesia
Meta-analyses show that spinal and epidural anesthesia reduce both thromboembolism and perhaps mortality in hip fractures surgery7,8 and total knee replacement (TKR).9–11 This method does not reduce risk sufficiently on its own but should be regarded as a useful adjunct. Initial European experience suggested that neuraxial anesthesia could be safely used in the presence of LMWH. 12 However, more recently there have been concerns that a spinal hematoma may develop on rare occasions.13,14 Guidelines have been suggested.15,16 The LMWH (or pentasaccharide) can be given safely 4 hours after removal of the epidural catheter (see section on Pregnancy). However, LMWH or pentasaccharide should be avoided while a continuous postoperative neuraxial block is in place. The catheter should not be inserted until serum levels of the chemical agent used are at their lowest. This means that postoperative administration of the agent is generally safer and more predictable than preoperative administration when epidural analgesia is needed.
Duration of Prophylaxis in Elective Orthopedic Surgery
Studies in patients having total hip replacement (THR)1,17–25 demonstrate that there is prolonged risk, with 45% to 80% of all symptomatic events occurring after discharge from the hospital.19,26–28 Randomized controlled trials (RCTs) in patients having THR indicate that prolonged thromboprophylaxis with LMWH for up to 35 days is safe and effective irrespective of whether inhospital prophylaxis was with LMWH or warfarin. It decreases the frequency of venographically detected total deep vein thrombosis (DVT), proximal DVT, and symptomatic VTE after the seventh day by more than 50%.25,29–33 One RCT compared warfarin prophylaxis (international normalized ratio [INR] 2-3) for 9 days with warfarin extended for 1 month after hospital discharge. The VTE occurred in 5.1% of inhospital prophylaxis patients and 0.5% in those having extended prophylaxis (relative risk [RR] 9.4; 95% confidence interval [CI] 1.2-73.5). 34 This study was prematurely terminated because of the superiority of prolonged prophylaxis. As indicated above, it has been subsequently demonstrated that extended prophylaxis with warfarin is associated with more hemorrhagic complications than with LMWH. 35 The RECORD2 study 36 that compared extended thrombophylaxis (35 days) using rivaroxaban with short-term enoxaparin (10-14 days) followed by placebo further confirmed the benefits of extended prophylaxis after THR suggested by the RECORD1 study. 37
Further studies are needed before recommendations can be made for prophylaxis beyond 35 days. The optimal duration of prophylaxis is unknown. Epidemiological data on postoperative death rates indicate a much longer duration of risk in subgroups such as emergency patients (eg, hip fracture) and patients with comorbidity (eg, rheumatoid arthritis) in which vascular deaths dominate.38,39
Elective Hip Replacement
The Risk
In the absence of prophylaxis, patients undergoing elective major joint replacement and those with hip fracture have a DVT risk of approximately 50% as shown in studies performed in the 1970s, 1980s, and 1990s19,40,41 (Table 6.1).42–91,67,92–109 Similar high rates of VTE were found in the placebo groups of 2 recent dose-ranging studies for enoxaparin and fondaparinux performed in Japan.110,111 The frequencies of proximal DVT (Table 6.2)63–65,67–69,112,113 and pulmonary embolism (PE; Tables 6.3112,114 and 6.4115,116) are also high, and symptomatic events range from 2% to 5%. 117 In a population-based study in Scotland, the incidence of VTE including fatal PE for the years 1999 to 2001 was 2.27% for primary hip arthroplasty and 1.79% for total knee arthroplasty. 118 The risk of clinical DVT and PE continues after hospitalization over a period of approximately 3 months19,20,117,119 (Table 6.5).18,120–123 Mortality studies have confirmed a reduced survival for 2 to 3 months following elective surgery with the highest death rate initially early after operation.38,124
The Frequency of all DVT in Orthopedic Surgery and Trauma, in the Absence of Prophylaxis (Diagnosed by Surveillance With Objective Methods: Phlebography, FUT, or DUS).a
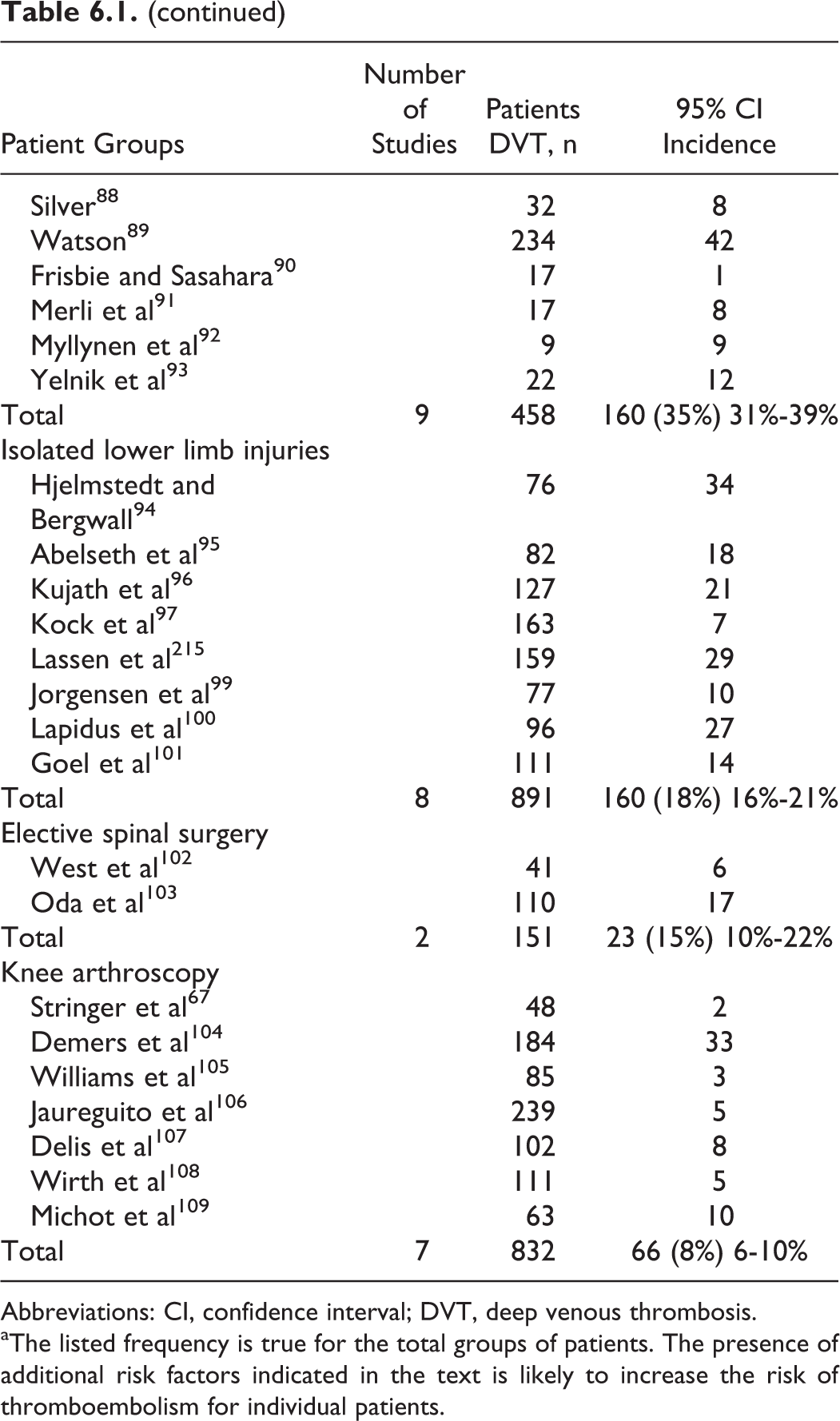
Abbreviations: CI, confidence interval; DVT, deep venous thrombosis.
aThe listed frequency is true for the total groups of patients. The presence of additional risk factors indicated in the text is likely to increase the risk of thromboembolism for individual patients.
The Frequency of Proximal DVT in the Absence of Prophylaxis Diagnosed by Surveillance With Objective Methods (Fibrinogen Uptake Test or Venography).
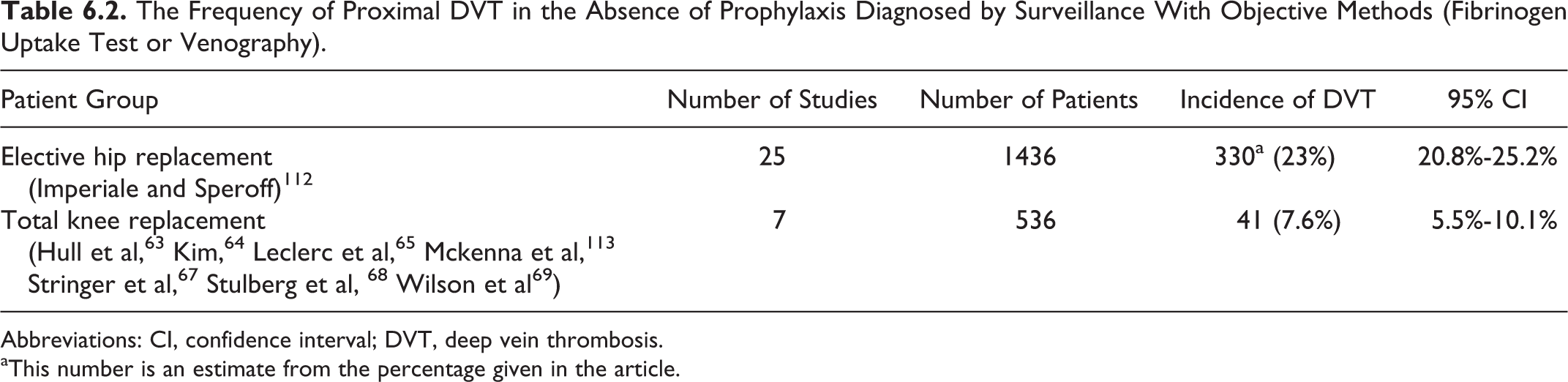
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis.
aThis number is an estimate from the percentage given in the article.
The Frequency of Clinical Pulmonary Embolisma in the Absence of Prophylaxis.

Abbreviations: CI, confidence interval; PE, pulmonary embolism.
a In most of the studies using an objective method of screening for DVT, patients found to have proximal thrombosis were treated with anticoagulants; the true incidence of clinical pulmonary embolism in series without such screening and intervention is unknown.
b
The Frequency of Fatal Pulmonary Embolism Without Prophylaxis.

Abbreviations: CI, confidence interval; PE, pulmonary embolism.
a In most of the studies using an objective method of screening for DVT, patients found to have proximal thrombosis were treated with anticoagulants; the true incidence of fatal pulmonary embolism in the absence of intervention is unknown.
Mortality After Elective Hip Replacement in the Absence of Routine Pharmacological Prophylaxis.a
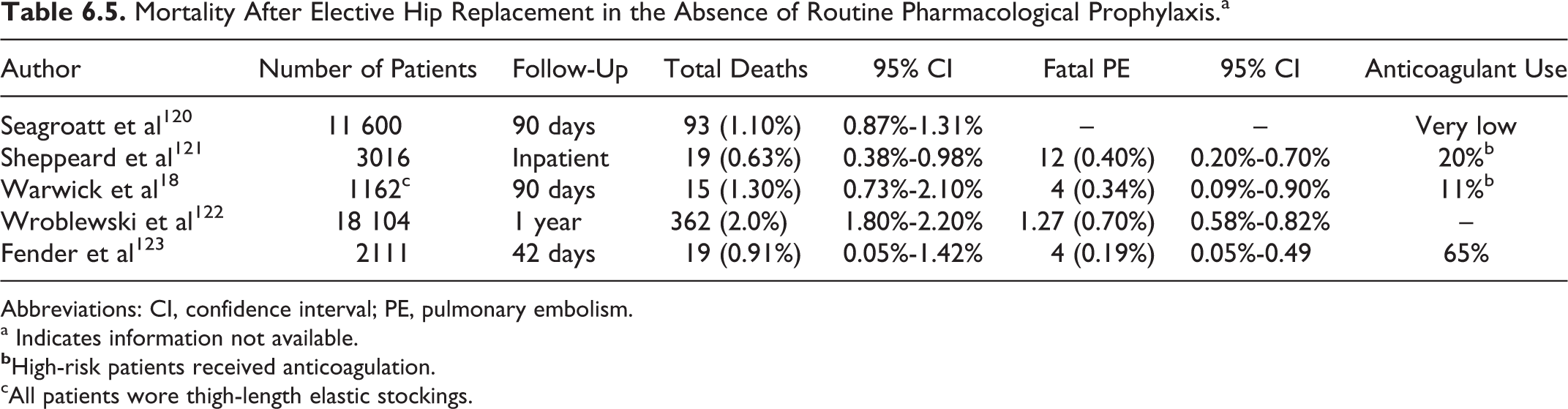
Abbreviations: CI, confidence interval; PE, pulmonary embolism.
a Indicates information not available.
cAll patients wore thigh-length elastic stockings.
There is a high incidence of proximal DVT (18%-36%) in patients having THR47,50,51,53,56,125–128 in contrast to patients having TKR in whom the preponderance of thrombosis is distal.66–68,129,130
Modern THR surgery is performed with a continuing reduction in hospital stay (3-6 days) so that patients are discharged while still at risk. Thus, the majority of clinical events appear after hospital discharge, giving a false impression of a decreasing problem.20,131,119
A recent meta-analysis of 10 RCTs that used venography in patients having THR treated by LMWH found that for every 5 patients with asymptomatic DVT in a screening program, 1 patient experienced symptomatic VTE within 3 months of the operation. 132 The consistency of this finding with previous reports strengthens the belief that asymptomatic DVT is a surrogate for symptomatic DVT.
Prophylactic Methods and Recommendations
General Considerations
Prophylactic methods that have been investigated in patients having THR include aspirin, fixed low-dose unfractionated heparin (LDUH), LMWH, heparinoid, recombinant hirudin, oral direct-Xa inhibitors, oral direct thrombin inhibitors, fixed mini-dose and adjusted doses of vitamin K agonists (VKA), graduated elastic compression (GEC) stockings, IPC, and FIT. To determine the risk reduction for each prophylactic method, only randomized studies with systematic screening tests for DVT have been used for the purposes of this analysis (Tables 6.6–6.84,69,114,130,133–139 and Figures 6.1–6.31,47,51,63,65,140–145).


Effect of Antiplatelet Therapy (eg, Aspirin) in the Prevention of DVT Diagnosed by Surveillance With Objective Methods (Fibrinogen Uptake in General Surgery and Phlebography in Orthopedic Surgery) in Randomized Controlled Studies (Antiplatelet Trialists' Collaboration). 114
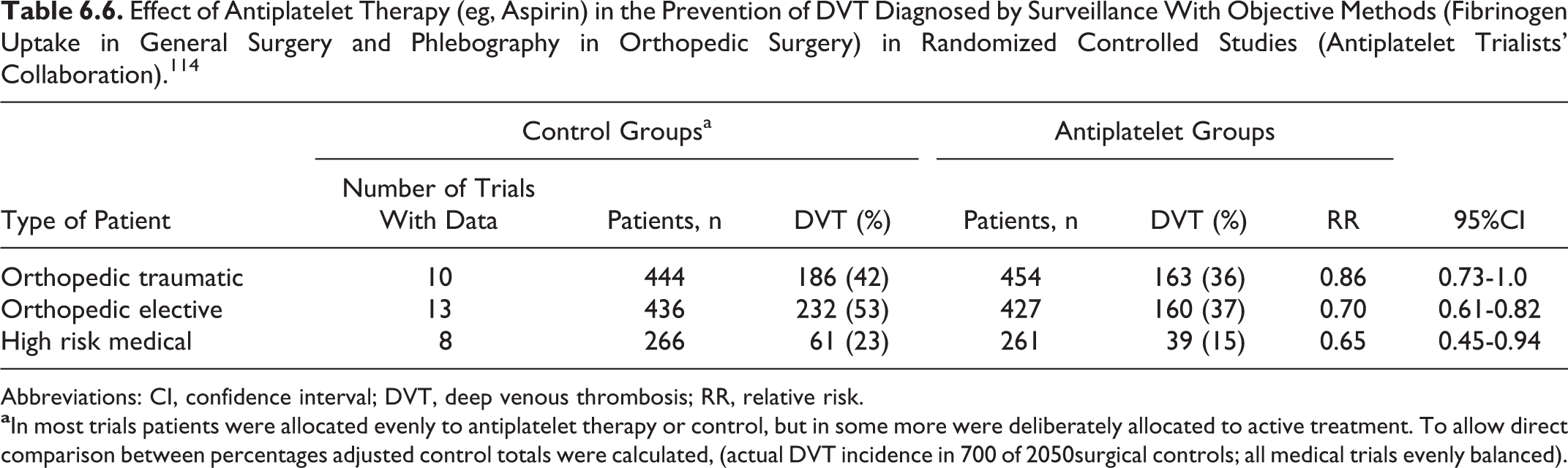
Abbreviations: CI, confidence interval; DVT, deep venous thrombosis; RR, relative risk.
Effect of Antiplatelet Therapy (eg, Aspirin) in the Prevention of PE in Randomized Controlled Studies (Antiplatelet Trialists' Collaboration). 114
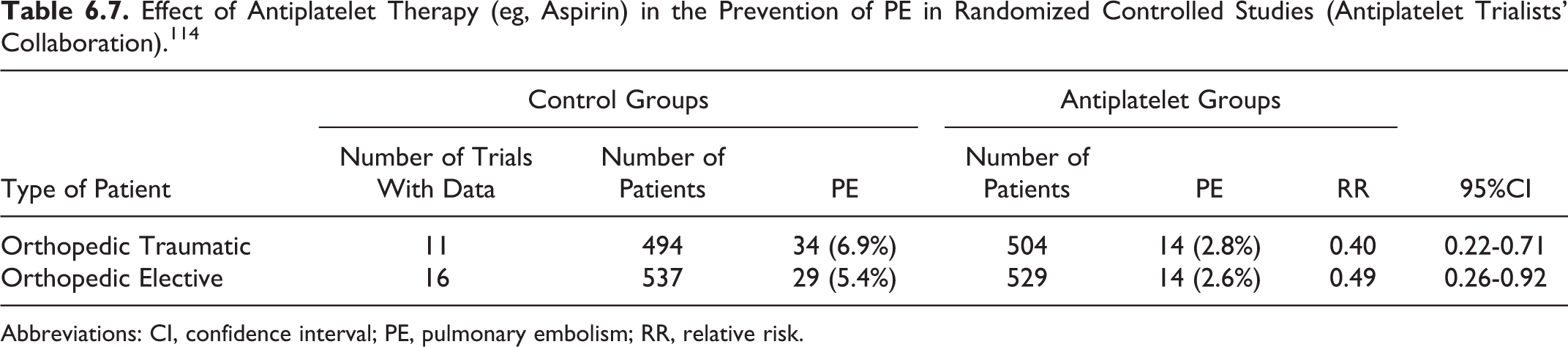
Abbreviations: CI, confidence interval; PE, pulmonary embolism; RR, relative risk.
Effect of Prophylaxis Using the Combination of Foot Impulse Technology (FIT) With Graduated Elastic Compression (GEC) on Proximal DVT, in Orthopedic Patients.
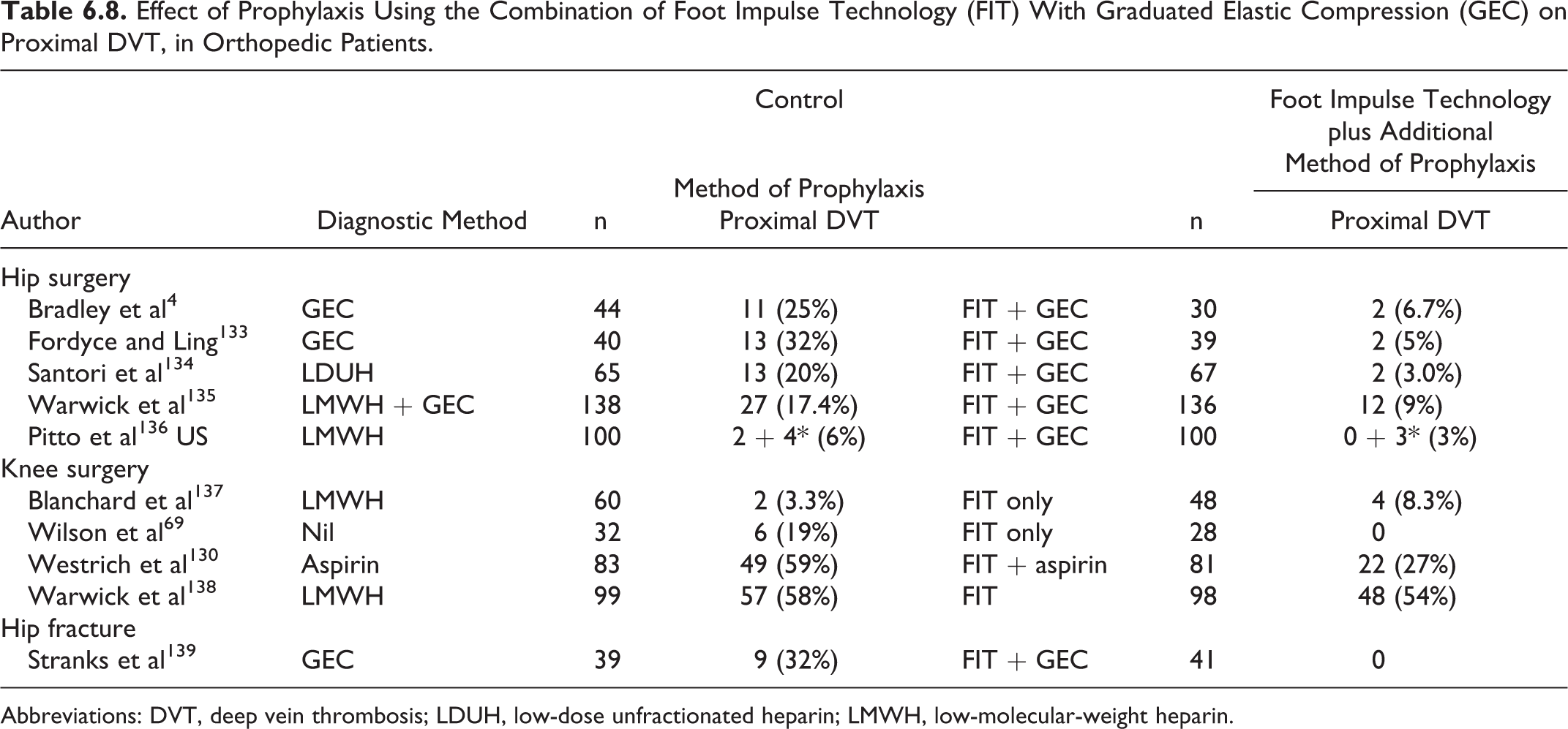
Abbreviations: DVT, deep vein thrombosis; LDUH, low-dose unfractionated heparin; LMWH, low-molecular-weight heparin.
The LDUH (5000 IU 8 or 12 hours) was found to be effective in reducing DVT from 46.8% to 23.3% (RR 0.50; 95% CI 0.43-0.58; meta-analysis of 20 randomized controlled studies in patients having elective THR) 115 and was the method of choice in the 1980s.
The LMWH has been subsequently demonstrated to be superior to LDUH for elective THR surgery, reducing DVT from 21.2% to 13.8% (RR 0.66; 95% CI 0.52-0.84) and PE from 4.1% to 1.7% (RR 0.4; 95% CI 0.19-0.84).32,128,146–153 Thus, LDUH is no longer recommended.
As indicated in the section on “General, Vascular, Bariatric and Plastic Surgical patients,” regulatory bodies in Europe and North America now consider the various LMWHs to be distinct drug products. They require clinical validation for specific indications of each drug. Therapeutic interchange among these products is not appropriate.
The RCTs have shown that recombinant hirudin (desirudin) is more effective than LDUH154–156 or LMWH. 155 Of 2079 patients studied, 1587 were included in the primary efficacy analysis. Overall, DVT was reduced with hirudin 15 mg twice daily (bid) compared to 40 mg enoxaparin from 25.5% to 18.45% (P = .001; relative risk reduction [RRR] 28.0%). The safety profile was the same in both the groups. 155
Several RCTs have compared VKA with LMWH. The LMWH was found to be more effective 1,142,157,158 or at least as effective 143 for preventing asymptomatic DVT. However, this was at the expense of a slight increase in hemorrhagic complications. When LMWH was started before or immediately after surgery, there was a marked reduction of proximal DVT from 3% to 0.8% (RR 0.28; 95% CI 0.1-0.74). 3 Symptomatic DVT was also reduced from 4.4% in the warfarin group to 1.5% in the LMWH group (RR 0.32; 95% CI 0.12-0.88). A meta-analysis of VKA in orthopedic surgery 159 showed a RR of 0.56 (95% CI 0.37-0.84) for DVT and 0.23 for PE (95% CI 0.09-0.59) compared to placebo. The VKAs were less effective than LMWH in preventing total DVT (RR 1.51; 95% CI 1.27-1.79) and proximal DVT (RR 1.51; 95% CI 1.04-2.17) although the risk of wound hematoma was increased from 3.3% in the VKA recipients to 5.3% in LMWH recipients (RR 2.29; 95% CI 1.09-7.75).
In a clinical trial for THR, 35 1279 patients were randomized on the third postoperative day to LMWH or to warfarin for the subsequent 6 weeks. The primary end point was the overall clinical failure rate that is symptomatic VTE (radiologically confirmed), major hemorrhage, or deaths. The failure rate was 3.7% in the LMWH group and 8.3% in the warfarin group (P = .01). Major bleeding occurred in 1.4% in the LMWH group and in 5.5% in the warfarin group. It appears that reduced bleeding seen initially after surgery due to the slow onset of action for warfarin is offset by long-term increased bleeding. Furthermore, national drug registries have shown warfarin to be a major cause of readmission and fatal bleeding.160,161 With these data, and because of the need for monitoring, the small therapeutic window and the risk of drug interactions, some surgeons find it difficult to see an advantage for VKA over LMWH.
In contrast to LMWH, the pentasaccharide fondaparinux is a pure synthetic chemical compound. It is a potent indirect inhibitor of factor Xa acting by a catalytic effect facilitating antithrombin binding to activated factor X and represents one of the many attributes of heparins. The drug is administered by subcutaneous injection once daily (qd). It has been registered internationally for major orthopedic surgery. Two large RCTs compared fondaparinux to enoxaparin.98,162 Reduction of asymptomatic DVT was 26% (RR 0.74; 95% CI 0.47-0.89) and symptomatic PE was 56% (RR 0.44; 95% CI 0.27-0.66) with fondaparinux. For the 2 studies combined, the incidence of major bleeding was 3% in the fondaparinux and 2.1% in the enoxaparin patients (P >.05). Fondaparinux may accumulate and increase bleeding in patients with impaired renal function.
A meta-analysis in the early 1990s 114 demonstrated that antiplatelet therapy in elective hip surgery is only moderately effective for protection against DVT (RR 0.7; 95% CI 0.61-0.82; Table 6.6), but the observed reduction in the risk of PE was substantial (RR 0.49; 95% CI 0.26-0.92; Table 6.7). However, the subsequent PEP study163,164 showed that aspirin is not as valuable as the meta-analysis suggested. Over 13 000 patients with hip fracture were randomized to have either aspirin or placebo. The overall death rate was identical in each group. Risk reduction for symptomatic VTE was from 2.5% to 1.6% and this was only one-half of that expected from LMWH and one-third from pentasaccharide. The reduced risk of VTE was matched by an increased risk of blood transfusion, gastrointestinal bleeding, and wound bleeding. In a supplementary group of 4000 patients with elective hip and knee replacement, there was an insignificant difference in symptomatic VTE. 164 The relative weak thromboprophylactic effect of aspirin therefore carries an alternative complication rate and its use might deprive patients of safer or more effective prophylaxis.
The Cochrane database 165 and an earlier meta-analysis 166 show that GEC is effective in reducing DVT in hospitalized patients, but there are few robust studies specific to orthopedic surgery.52,167 Because other methods of prevention are more effective, GEC stockings on their own are not recommended.
The IPC is effective in patients having THR47,51,140 (Figure 6.1) reducing DVT from 43.6% in the control groups to 21% in the compression groups (RR 0.48; 95% CI 0.36-0.64). Modern technology has made IPC devices light, silent, more portable, and more effective in preventing stasis by sensing venous volume so that the compression period follows immediately after venous refilling. In addition, different sleeve designs and materials have been used to improve patient compliance. 168 In a recent study involving 392 evaluable patients having THR in which IPC was compared to LMWH, the incidence of postoperative DVT was found to be 3% in both the groups. 169
Three subsequent RCTs have compared combined modalities with LMWH. In the first study 170 in 131 patients having THR and TKR, the combination of LMWH plus IPC was more effective than LMWH plus GEC stockings (DVT incidence 0% vs 28%). In the second study involving 277 patients, the combination of LMWH plus IPC was more effective than LMWH (DVT incidence 6.6% vs 19.5%). 171 In the third study involving 1803 patients having various orthopedic operations, the combination of LMWH plus IPC was also more effective than LMWH (DVT incidence 0.4% vs 1.7%). In the subgroup of 306 patients having THR, the incidence of DVT was 0% in the combined modalities group and 5.2% in the LMWH group (P <0.001 172 ; see section on combined modalities). In another study involving 121 evaluable patients having THR or TKR, in which IPC plus aspirin 100 mg daily was also compared to LMWH, the incidence of postoperative venographic DVT was found to be 6.6% in the IPC group and 28.3% in the LMWH group (RR 0.23; 95% CI 0.08-0.65). 173
The FIT combined with GEC is effective in reducing the incidence of proximal DVT in patients having THR or TKR (Table 6.8) with less bleeding and swelling. Direct comparisons with chemical prophylaxis are sparse; there is probably superiority to LDUH 134 and equivalence with LMWH for THR136,174 but not for TKR. 137
The IPC and FIT offer an alternative for patients with contraindications to chemical prophylaxis (Figure 6.1 and Table 6.9).
Effect of Antiplatelet Therapy (eg, Aspirin) in the Prevention of DVT Diagnosed by Surveillance With Objective Methods (Fibrinogen Uptake in General Surgery and Phlebography in Orthopedic Surgery) in Randomized Controlled Studies (Antiplatelet Trialists' Collaboration). 114
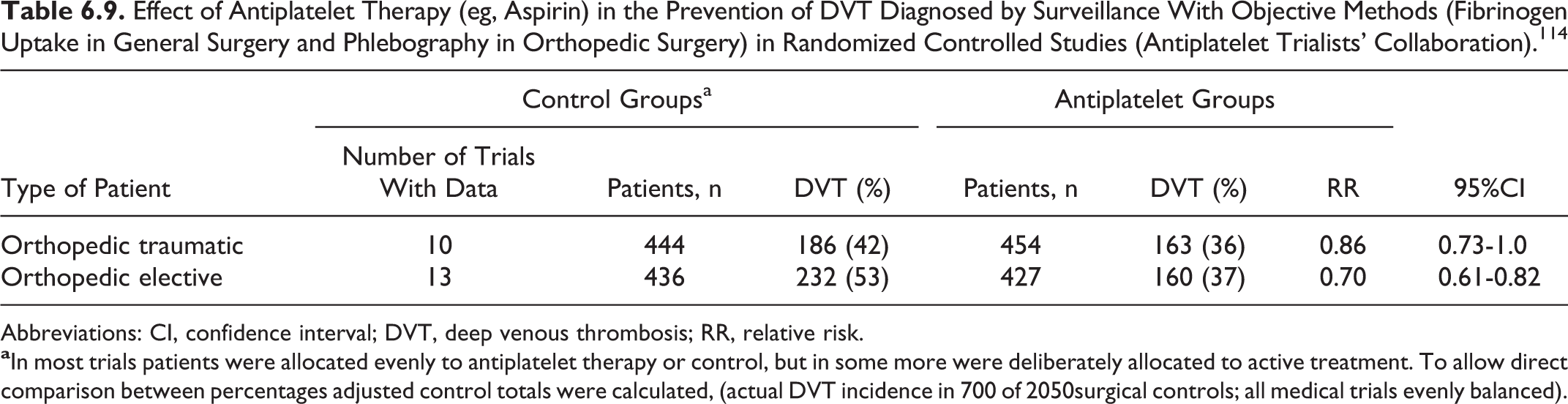
Abbreviations: CI, confidence interval; DVT, deep venous thrombosis; RR, relative risk.
Rivaroxaban is a new oral direct Xa inhibitor. Two studies (RECORD1 and RECORD2) have compared rivaroxaban with enoxaparin in patients having THR. In RECORD1 study that involved 3153 evaluable patients, both prophylactic regimens were given for 31 to 39 days. Superior efficacy of rivaroxaban was demonstrated, with an incidence of venographic VTE of 3.7% in the enoxaparin group and 1.1% in the rivaroxaban group (P < .001). The incidence of major and nonmajor clinically relevant bleeding was 2.5% in the enoxaparin group and 3.2% in the rivaroxaban group (not significant [NS]). 37 The RECORD2 study investigated the efficacy of extended thrombophylaxis (35 days) with rivaroxaban compared to short-term enoxaparin (10-14 days) followed by placebo. 36 The incidence of venographic VTE was 9.3% in the enoxaparin group and 2.0% in the rivaroxaban group (P < .0001). The incidence of major and nonmajor clinically relevant bleeding was 2.8% in the enoxaparin group and 3.3% in the rivaroxaban group (NS).
Apixaban is another new oral direct Xa inhibitor. In a double-blind placebo controlled study involving 5407 patients having THR, apixaban at a dose of 2.5 mg orally bid was compared with enoxaparin at a dose of 40 mg subcutaneously every 24 hours. Apixaban therapy was initiated 12 to 24 hours after closure of the surgical wound; enoxaparin therapy was initiated 12 hours before surgery. Prophylaxis was continued for 35 days after surgery, followed by bilateral venographic studies. The incidence of the primary efficacy outcome (asymptomatic or symptomatic DVT, nonfatal PE, or death from any cause during the treatment period) was 1.4% in the apixaban group and in 3.9% in the enoxaparin group (RR 0.36; 95% CI 0.22-0.54; P < .001) for both noninferiority and superiority. The incidence of major and clinically relevant nonmajor bleeding was 4.8% in the apixaban group and 5.0% in the enoxaparin group (P > 0.05). 175
Edoxaban is a new oral direct FXa inhibitor that is 10 000-fold more selective for FXa than thrombin. 176 In the randomized, double-blind, double-dummy STARS J-V trial (N = 503), edoxaban (30 mg qd) resulted in significantly fewer VTEs than enoxaparin (2000 IU bid; 2.4% vs 6.9%; P = .0157 for superiority). The difference between the incidence of major and clinically relevant nonmajor bleeding events between edoxaban (2.6%) and enoxaparin (3.7%) was not statistically significant (P = .475).
Dabigatran is a new oral direct inhibitor of thrombin. Two double-blind noninferiority trials evaluated the efficacy and safety of dabigatran in patients having elective THR. In the first study (RE-NOVATE), there were 3 groups of patients receiving dabigatran 150 mg, 220 mg, or enoxaparin 40 mg for 25 to 35 days (median 33 days) when bilateral venography was performed. The primary endpoint of total VTE and all-cause mortality occurred in 8.6%, 6.0%, and 6.7% of the groups, respectively (P < .0001 for noninferiority of each group versus enoxaparin). 177 In the second study (RE-NOVATE II) 220 mg of dabigatran was compared with 40 mg enoxaparin administered for the same period. 178 The primary end point of total VTE and all-cause mortality occurred in 7.7% in the dabigatran and 8.8% in the enoxaparin group (P < 0001 for noninferiority of dabigatran vs enoxaparin). There was no significant difference in major bleeding events between the various groups in either study.
Recommendations
The LMWH initiated and dosed according to the manufacturer’s recommendations (level of evidence: high), fondaparinux (level of evidence: high), VKAs (level of evidence: high), rivaroxaban (level of evidence: high), apixaban (level of evidence: high), dabigatran (level of evidence: high). IPC or FIT combined with GEC stockings are an equivalent alternative to LMWH (level of evidence: high) for those surgeons or anesthetists concerned about bleeding either in all or in certain patients. These devices can be used as long as tolerated and then replaced with chemical prophylaxis starting as soon as it is safe and continued for the rest of the 5-week period of risk. Desirudin is approved for short-term prophylaxis in approximately 20 European countries and the United States and can be used in patients with heparin-induced thrombocytopenia (level of evidence: high).
The LMWH combined with IPC is more effective than either prophylactic modality used alone and should be considered in all cases (level of evidence: high).
Prophylaxis with LMWH should be initiated either before or after operation depending on the adopted regimen (level of evidence: high). Fondaparinux should be started at least 6 to 8 hours after surgery. Prophylaxis should be continued for 4 to 6 weeks with LMWH (level of evidence: high) or fondaparinux (level of evidence: low; extrapolation from a hip fracture trial).
Elective Knee Replacement
The Risk
Data from THR should not be extrapolated to TKR. The incidence of asymptomatic DVT detected by venography is higher in patients having TKR than THR. However, the incidence of above-knee DVT is lower than in patients having THR (see section on THR above).
Prophylactic Methods and Recommendations
General considerations
The IPC is effective in patients having TKR (RR 0.27; 95% CI 0.14-0.49; Table 6.8). One small study demonstrated that
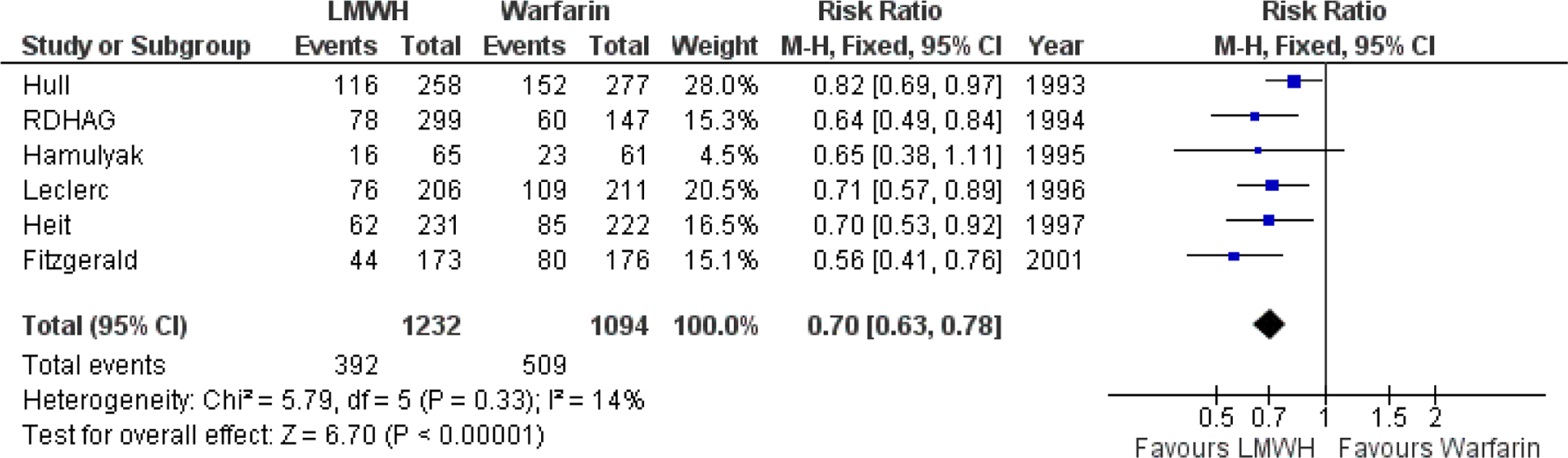
A RCT performed in 1992 demonstrated that LMWH was more effective than placebo. It reduced venographically detected DVT from 65% in the placebo group to 19% in the LMWH group (RR 0.30; 95% CI 0.16-0.58). 181 Subsequent studies demonstrated that LMWH was more effective than LDUH (RR 0.75; 95% CI 0.58-0.92)182,183 or warfarin (RR 0.68; 95% CI 0.62-0.76; Figure 6.3).
Fondaparinux (2.5 mg qd starting 6 hours after surgery) was more effective than enoxaparin (30 mg bid starting 12-24 hours after surgery) in 1 study. 184 The VTE (defined as venographically detected DVT, symptomatic DVT or symptomatic PE) was reduced from 27.8% in the enoxaparin group to 12.5% in the fondaparinux group (RR 0.45; 95% CI 0.32-0.62). However, major bleeding was more common with fondaparinux (2.1% vs 0.2%, P = .006). This increased rate of bleeding with fondaparinux was driven by a minority of patients given fondaparinux within 6 hours of surgery. The efficacy of fondaparinux was confirmed in a meta-analysis 185 that included the above study and 3 other RCTs comparing fondaparinux with enoxaparin in patients having orthopedic surgery other than TKR.
Rivaroxaban is a new oral direct anti-Xa inhibitor. Two studies (RECORD3 and RECORD4) have compared rivaroxaban with enoxaparin in patients having TKR. In RECORD3 study that involved 2531 evaluable patients, both prophylactic regimens were given for 10 to 14 days. The primary end point of total VTE was 18.9% enoxaparin and 9.6% for rivaroxaban (P < .001). The incidence of venographic DVT was 2.6% in the enoxaparin group and 1.0% in the rivaroxaban group (absolute risk reduction, 1.6%; 95% CI, 0.4-2.8; P < .01 for noninferiority). There was no significant difference in the incidence of major and nonmajor clinically relevant bleeding in the 2 groups. 186 The RECORD4 study 187 compared the efficacy and safety of rivaroxaban with the commonly used North American regimen of enoxaparin 30 mg bid until day 11 to 15 when bilateral venography was performed. The incidence of venographic VTE, PE, or death was reduced from 10.1% in the enoxaparin group to 6.9% in the rivaroxaban group (RR 0.69; 95% CI 0.51-0.92). There was no significant difference in the incidence of major and nonmajor clinically relevant bleeding in the 2 groups.
Apixaban is another new oral direct Xa inhibitor. Two randomized double-blind control studies compared apixaban with enoxaparin. In the first study, the overall rate of primary events was much lower than anticipated (primary efficacy outcome 9.0% with apixaban and 8.8% with enoxaparin) and apixaban did not meet the noninferiority criteria compared with enoxaparin 30 mg bid in the prevention of VTE after TKR 188 However, in the second study it demonstrated superiority against enoxaparin 40 mg qd (primary efficacy outcome 15% with apixaban and 24% with enoxaparin; RR 0.62; 95% CI 0.51-0.74, P < .0001) without any significant difference in bleeding between the 2 groups. 189
Dabigatran is a new oral direct inhibitor of thrombin. Two double-blind noninferiority trials evaluated the efficacy and safety of dabigatran in patients having elective TKR. In the first study (RE-MODEL) there were 3 groups of patients receiving dabigatran 150 mg, 220 mg, or enoxaparin 40 mg for 6 to 10 days when bilateral venography was performed. The primary end point of total VTE and all-cause mortality occurred in 40.5%, 36.4%, and 37.7% of the groups, respectively (P = .0003 and .017 for noninferiority of each group vs enoxaparin). 190 In the second study (RE-MOBILIZE), there were also 3 groups of patients receiving dabigatran 150 mg, dabigatran 220, or enoxaparin 30 mg bid administered for 12 to 15 days (median 13 days). 191 Noninferiority of either dabigatran dose was not confirmed. The primary end point of total VTE and all-cause mortality occurred in 33.7%, 31.1%, and 25.3% of the 3 groups, respectively. Among 1896 patients, dabigatran 220 and 110 mg showed inferior efficacy to enoxaparin (P = .02 and P < .001, respectively). In all 3 treatment groups, the composite primary end point was driven primarily by the occurrence of distal DVT whereas no significant difference was observed in mortality rates. There was no significant difference in major bleeding events between the various groups in either study.
Combined Modalities
Three trials have compared combined modalities with LMWH. In the first study 170 in which 131 patients have THR and TKR, the combination of LMWH plus IPC was more effective than LMWH plus GEC stockings. In the subgroup of patients having TKR, the incidence of VTE was 0% in the combined modalities group and 40% in the LMWH group using compression ultrasonography. In the second study involving 277 patients, the combination of LMWH plus IPC was more effective than LMWH (DVT incidence 6.6% vs 19.5%; P = .018). 171 In the third study involving 1803 patients having various orthopedic operations the combination of LMWH plus IPC was also more effective than LMWH (DVT incidence 0.4% vs 1.7%). In the subgroup of 133 patients having TKR, the incidence of DVT was 3.8% in the combined modalities group and 7.4% in the LMWH group (P < .038 172 ; see section on combined modalities).
Duration of Prophylaxis
The effect of extending prophylaxis using LMWH to 30 to 42 days beyond hospitalization on symptomatic DVT in patients having TKR is less (odds ratio [OR] 0.74; 95% CI 0.26-2.15; P > .05) than in patients having THR (OR 0.33; 95% CI 0.19-0.56; P < 0.05) as shown by a systematic review. 192
Recommendations
The LMWH (initiated and dosed according to the manufacturer’s recommendations; level of evidence: high), warfarin (although less effective; level of evidence: high), rivaroxaban (level of evidence: high), apixaban (level of evidence: high), dabigatran (level of evidence: high), and fondaparinux (level of evidence: high). The IPC is an alternative option (level of evidence: moderate due to small study size). The LMWH combined with IPC is more effective than LMWH prophylactic modality used alone and should be considered in all the cases (level of evidence: high).
Hip Fracture Surgery
The Risk
Patients having hip fracture surgery have the highest rates of DVT (46%-60%)81,193,194 and fatal PE (2.5%-7.5%; Tables 6.1, 6.3, and 6.4). 126,194,195 The VTE risk period lasts for 2 to 3 months after hip fracture surgery in spite of common short-term prophylaxis,20,117 and the 90-day risk of overall death is 13%. 196 After hip fracture, the risk is greater than the standardized mortality, the majority dying of vascular events despite the fact that most patients receive some form of short-term prophylaxis.38,124
Prophylactic Methods and Recommendations
General considerations
Because the risks of DVT and PE including fatal PE are high in patients with hip fracture (Tables 6.1, 6.3, and 6.4), prophylaxis should start as soon as possible after diagnosis and should be the same as that recommended for elective hip surgery.
Reduction in asymptomatic DVT has been demonstrated by IPC (RR 0.2; 95% CI 0.07-0.55) 140 and FIT in combination with GEC 139 (RR 0.32; 95% CI 0.32-0.67; Table 6.8). In the most recent study, 197 the combined end point of PE and proximal DVT using duplex ultrasound was reduced from 12% in the group without prophylaxis to 4% in the IPC group. More studies are needed.
A meta-analysis 114 demonstrated that antiplatelet therapy in traumatic orthopedic surgery is only slightly effective for protection against DVT (RR 0.86; 95% CI 0.73-1; Table 6.6), but the observed reduction in the risk of PE is substantial (RR 0.4; 95% CI 0.22-0.71; Table 6.7). In a randomized, placebo-controlled trial of patients undergoing surgery for hip fracture (13 356 patients) or for elective hip or knee arthroplasty (4088 patients), aspirin in a dose of 160 mg daily started preoperatively was used as the primary prophylactic agent for 35 days. The primary end point of the study was total mortality, and the study failed to detect any difference between the placebo and the aspirin groups. However, in the subgroup analysis of the patients with hip fracture, aspirin reduced the incidence of symptomatic DVT by 29% (95% CI 3%-48%; P = .03) and PE by 43% (95% CI 18%-60%; P = .002). The PE or DVT was confirmed in 105 (1.6%) of 6679 patients assigned aspirin compared to 165 (2.5%) of 6677 patients assigned placebo, which represents an absolute reduction of 9 per 1000 and a proportional reduction of 36% (95% CI 19%-50%; P = .0003). However, the complication rate (transfusion requirements and bleeding) offsets much of the reduction in symptomatic VTE. 163 Since other methods are more effective, aspirin on its own is not recommended for routine thrombophylaxis.
Several studies performed in the 1970s demonstrated that LDUH was effective in reducing asymptomatic DVT, as reported in an overview 115 (RR 0.51; 95% CI 0.42-0.62). Although a significant reduction in total PE was not demonstrated, there was a significant reduction in fatal PE. 115
The LMWH has been assessed against placebo,53,198 LDUH, 199 danaparoid, 200 high-dose (40 mg enoxaparin) LMWH, 201 and fondaparinux. 202 The LMWH has been found to be equally effective as LDUH without increase in hemorrhagic complications. 203
Three RCTs have demonstrated that VKAs are effective in preventing asymptomatic DVT with a 61% RRR for DVT and 66% for proximal DVT, compared to no prophylaxis.81,204,205 The increase in hemorrhagic complications reported varied from 0% to 47% without any increased bleeding in the most recent trial. 81
Fondaparinux given for 11 days was more effective when compared to LMWH in reducing VTE from 19.1% to 8.3% (RR 0.46; 95% CI 0.32-0.59) and proximal DVT from 4.3% to 0.9% (RR 0.22; 95% CI 0.09-0.53). 202 There was no difference in major bleeding but minor bleeding was increased from 2.1% in the enoxaparin group to 4.1% in the fondaparinux group (P = .02). In a second study, patients who received fondaparinux for 7 days were randomized to continuation with fondaparinux or placebo for a further 3 weeks. 206 The incidence of venographic DVT was 1.4% in the extended prophylaxis group and 35% in the placebo group (RR 0.04; 95% CI 0.01-0.13). Symptomatic VTE was 0.3% and 2.7%, respectively (RR 0.11; 95% CI 0.01-0.88). There was no difference in hemorrhagic complications.
Delayed admission to hospital or delayed surgery following hip fractures is associated with a high incidence of DVT developing prior to surgery.207–210 The incidence of preoperative DVT as shown by venography can be as high as 62% for all DVT and 14% for proximal DVT when the delay is 48 hours or more. 210 Thus, it is strongly recommended that if surgical delay is anticipated, prophylaxis is commenced as close to the fracture as possible. Prophylaxis should be restarted once postoperative hemostasis has been achieved.
None of the new oral anticoagulant regimens shown to be effective in elective hip and knee replacement have been tested in the hip fracture population.
Recommendations
The LMWH (initiated and dosed according to the manufacturer’s recommendations; level of evidence: high), fondaparinux (level of evidence: high), adjusted dose VKA (INR range 2-3; level of evidence: high), or LDUH (level of evidence: high). The IPC or FIT combined with GEC should be used when there are contraindications for pharmacological prophylaxis (level of evidence: low). If surgery is likely to be delayed, prophylaxis should be initiated with LMWH or IPC or FIT plus GEC as close to the fracture as possible (level of evidence: low). Prophylaxis should be provided for 4 to 5 weeks after surgery (level of evidence: high).
Knee Arthroscopy
The Risk
Knee arthroscopy is a very common procedure that varies from a simple diagnostic technique to an extensive repair of injured soft tissues. The use of a tourniquet, manipulation of the leg, and distension of the joint with fluid may all associate this procedure with a risk of VTE. However, symptomatic VTE is very rare. This poses a dilemma, rare events in a common procedure will lead to quite a high number of events even though the proportional risk is very low. However, universal prophylaxis would be very expensive, with uncertain cost benefit and risk benefit ratios.
The frequency of DVT in patients undergoing arthroscopic procedures in the absence of prophylaxis varies greatly between studies; symptomatic DVT occurs in perhaps 0.6%. 20 Meta-analysis of 6 studies104,105,107–109,211 by Ilahi in 2005 shows that asymptomatic DVT occurs in approximately 9.9%; however, there is a very large range; ultrasound demonstrates rates from 6% 212 to 16% 109 and venography from 3.1% 211 to 17.9% 104
Prophylactic Methods and Recommendations
General considerations
In a meta-analysis of 4 randomized studies in which different LMWHs given for 5 to 7 days, 213 the RR of thrombotic events was 0.16 (95% CI 0.05-0.52) compared to placebo (0.76% vs 8.2%). All thrombotic events but 1 PE in the LMWH group were distal. Adverse effects were more frequent in the intervention group (RR 2.04; 95% CI 1.21-3.44; 9.5% vs 4.5%). The number needed to harm was 20 for adverse effects. A recent study involving 1317 patients compared LMWH with GEC. 214 The 3-month cumulative incidence of asymptomatic proximal DVT, symptomatic VTE, and all-cause mortality was 3.2% (21 of 660 patients) in the GEC group and 0.9% (6 of 657 patients) in the 7-day LMWH group (RR 0.29; 95% CI 0.12-0.71). The cumulative incidence of major or clinically relevant bleeding events was 0.3% in the stockings group, 0.9% in the 7-day LMWH group (NS).
Thus, although clinical VTE is uncommon and fatalities are rare, the huge number of patients undergoing knee arthroscopy surgery makes VTE complications potentially relatively frequent. There is a clear correlation between age and degree of trauma with VTE. 67 This justifies prophylaxis in patients with additional risk factors or when extensive surgery beyond a simple diagnostic procedure is performed.
Recommendations
Recommendation for simple diagnostic arthroscopy.
A careful risk assessment should be undertaken. Routine prophylaxis is not recommended unless other risk factors are present (level of evidence: low).
Recommendation for arthroscopic surgery (eg, ligament reconstructions).
The LMWH starting before or after surgery (level of evidence: moderate) or IPC in the presence of contraindications to LMWH are recommended (level of evidence: low) until full ambulation.
Isolated Below Knee Injuries and Plaster Casts
The Risk
Patients with below knee injuries and immobilization have a DVT incidence in the range of 10% to 35% depending on the type and severity of injury (Table 6.1)94–97,99,215 and
Prophylactic Methods and Recommendations
General considerations
This group is so heterogeneous that studies and recommendations are difficult to devise. A clinical risk assessment is mandatory and for those with risk factors safe prophylaxis must be instituted. The risk of compartment syndrome, exacerbated by chemical thromboprophylaxis, must be considered in tibial fractures.
In one study of 253 patients with plaster casts of which the majority had soft tissue injuries, ultrasound incidence of DVT at cast removal was reduced from 17% in the control group to 5% in the LMWH group. 96 It was reduced from 4% in the control group to zero in the LMWH group in another study of 339 patients. 97 Considering both studies the RR was 0.21 (95% CI 0.09-0.49)
In patients with lower leg fractures, the 5-week incidence of venographic DVT was reduced from 18% in the control group to 10% in the LMWH group in one study (n = 293), 215 from 13% to 11% in another (n = 150), 99 and from 13% to 9% in a third study (n = 238). 101 In none of the 3 studies was the effect of LMWH on DVT significant (P > .05). However, in the subgroups of patients having Achilles tendon repair, the incidence of DVT was reduced from 21% to 6% in the first study 215 and from 29% to 10% in the second 99 However, in a more recent study 100 involving 93 patients LMWH was ineffective (28% vs 21%). More effective methods are needed in well-defined groups of patients.
A Cochrane review of the 1490 randomized patients concluded an OR of 0.49 for LMWH (95% CI 0.34-0.72) which supports a significant risk reduction for patients immobilized in plaster. 217 Furthermore, symptomatic VTE was also significantly reduced (OR 0.16; 95% CI 0.05-0.56). Complications were not increased in the LMWH group.
Recommendations
Currently available data based on a mixture of different types of injury suggest that routine LWMW prophylaxis should be considered for isolated limb trauma in the absence of contraindications (level of evidence: moderate). The drug will need to be administered in the outpatient setting until the patient is weight bearing.
Multiple Trauma
The Risk
The incidence of DVT in patients who have sustained major trauma is in excess of 50% 60,61,218–221 (Table 6.1) and PE is the third leading cause of death in those who survive beyond the first day.60,222–224 The risk is particularly high in patients with spinal cord injury, pelvic fracture, and those needing surgery.60,61,225–227
Prophylactic Methods and Recommendations
General considerations
Patients with multiple injuries have a particularly high risk for VTE. The tissue factor released by multiple injuries is potentiated by the likely surgical intervention and the subsequent prolonged immobility 225 which produces marked venous stasis. Routine venography has shown a DVT frequency of 58% in these patients. 60
Well-designed studies in this area are few and thromboprophylaxis has to be assessed according to the risk of bleeding. However, in the absence of intracranial bleeding and when bleeding is under control, LMWH (enoxaparin 30 mg bid) started within 36 hours of injury has been shown to be more effective than LDUH (5 000 IU bid). 218 The LMWH reduced the incidence of venographic DVT from 44% in the LDUH to 31% in the LMWH group (RR 0.70; 95% CI 0.51-0.97). The superiority of LMWH to LDUH has been confirmed by a subsequent study and a meta-analysis.220,228 A study comparing nadroparin fixed-daily dose versus a weight-adjusted dose did not demonstrate any significant difference (0% vs 3% DVT). 229
Five randomized controlled trials have tested the efficacy of IPC. The first was in 304 patients with pelvic fractures but the study was small and underpowered so that the DVT reduction from 11% in the control group to 6% in the IPC group was not significant (P > .05). 197 In the second, which involved 149 patients, IPC was compared with FIT with an incidence of DVT of 6% and 21%, respectively (P < .02). 230 The IPC or FIT were compared with enoxaparin 30 mg bid in the third study involving 372 patients with an incidence of DVT of 0.8% in the enoxaparin group, 2.5% in the IPC group, and 5.7% in the FIT. 231 The 2 most recent studies compared LMWH with IPC in 442 and 120 patients with trauma.232,233 In these studies the incidence of DVT was 0.5% and 6.6% in the LMWH groups, with 2.7% and 3.3% in the IPC groups, respectively. Thus, mechanical methods are attractive if chemical prophylaxis is contraindicated.
The RCT of the use of inferior venacava (IVC) filters to prevent PE in patients with trauma in the absence of DVT have not been performed. A recent systematic review of 7 observational studies suggested a potential reduction in PE but an associated 2% to 6% incidence of complications (IVC occlusion, filter migration, and thrombosis at the insertion site). 234
Recommendations
The LMWH started as soon as bleeding risk is acceptable (level of evidence: high) or IPC in the presence of contraindications to LMWH (level of evidence: high) and continued until full ambulation.
Electrical stimulation of the calf muscles may be considered in patients in whom pharmacological prophylaxis is contraindicated because of multiple injuries and IPC cannot be applied because of external fixation to a leg fracture. This is by extrapolation from studies in general surgery (level of evidence: low).
The use of IVC filter for primary prevention of PE when LMWH or IPC are contraindicated is not recommended (level of evidence: low).
Elective Spine Surgery
The Risk
Elective spine surgery consists of a mixture of types of surgical procedures ranging from simple laminectomy to complicated multilevel fusion. The procedures can be performed with a posterior, anterior, or combined approach. Data are very limited in elective spine surgery, both for efficacy and safety for different prophylactic methods. The incidence of DVT detected by routine venography in the absence of prophylaxis has been found to be 18% (Table 6.1).103,235 A review of studies on complications in patients having spinal fusion reported a 3.7% incidence for symptomatic DVT and 2.2% for PE. 236
Prophylactic Methods and Recommendations
General considerations
Two small randomized controlled studies, one comparing no prophylaxis with LDUH 237 and the other with enoxaparin, 238 demonstrated that prophylaxis reduces the incidence of asymptomatic DVT from 20% and 10%, respectively, to 0%.
Recommendations
Mechanical method
The IPC (level of evidence: low); drug: LMWH (level of evidence: low); initiation: before operation for IPC or after operation for LMWH; duration: during hospitalization (level of evidence: low).
Spinal Cord Injury
The Risk
In the absence of prophylaxis the incidence of silent DVT is of the order of 35% (Table 6.1). In this group of patients, PE is the third leading cause of death.239,240 In a series of 1649 patients undergoing rehabilitation, symptomatic DVT occurred in 10% and PE in 3%. 241
Prophylactic Methods and Recommendations
General considerations
Three studies have compared LDUH with placebo.90,91,242 Compared to controls, LDUH was associated with a nonstatistically significant reduction in the number of DVT (20.0% vs 29.4%; OR 0.55; 95% CI 0.11-2.64; P = .46). 243 Five studies have compared LDUH with LMWH.244–248 A meta-analysis comparing LDUH with LMWH has reported that although LMWH was associated with a nonstatistically significant reduction in the rate of all VTE (24.4% vs 22.7%; OR 0.78; 95% CI 0.24-2.53; P = .60, it was associated with a significant reduction in the rate of total PE (3.1% vs 9.2%; OR 0.29; 95% CI 0.090.95; P = .04). 243 Also, compared to LDUH, LMWH was associated with a nearly significant reduction in major bleeding (2.4% vs 5.2%; OR 0.50; 95% CI 0.24-1.04; P = .07).
When a combination of LDUH with IPC was compared to LMWH in a randomized controlled study, 247 results shown by routine venography were equally poor (63% vs 66%). It appears that patients with spinal cord injury are not only at high risk of VTE but also a highly resistant group to prophylactic measures. Further studies are needed.
Recommendations
The LMWH and/or LDUH (level of evidence: moderate) and LMWH plus IPC (level of evidence: low); initiation: IPC and GEC on admission and LMWH when bleeding risk is acceptable (level of evidence: low); duration: LMWH and IPC for 3 months and continuation with GEC indefinitely (level of evidence: low).