
Abstract

We have read with some interest and surprise the article by Barillari et al 1 on the use of prothrombin complex concentrates (PCCs) in a patient with FX Friuli disorder.
Such article contains a few scientific, historical, and deontological inaccuracies which should be corrected lest wrong data be circulated much to the confusion of the readers.
The FX Friuli variant was not discovered by Fair et al as stated by the authors in page 334, at the beginning of second column. 1 The article by Dr Fair, Revak, Hubbard, and Girolami of 1989 (quoted by the authors as ref 16) dealt only with the isolation and characterization of the FX Friuli abnormal protein. 2 The discovery of the mutation underlying the FX Friuli defect was reported in a 1991 article by James working in collaboration with the Padua group.3
The defect had been originally recognized and described in Padua in 1970 and 1971 in a series of articles, which firmly established the clinical features and the peculiar laboratory pattern (low activity in the extrinsic and intrinsic systems, normal activity in the Russell viper venom assay, normal antigen) of the condition. 4 –6
We cannot abstain from noting that it would have been scientifically correct to acknowledge this by quoting the original articles. Incidentally the patient presented by the authors belongs to the large kindred studied by us in 1970 and reported in one of the original articles (patient IVa of Figure1). 4 Basic deontological principles would have required such acknowledgment.
Furthermore, the authors could have obtained useful comparative information on the use of PCC in these patients by quoting another article of ours, 7 where they could have found useful information on survival times of administered FX. The citation of this article could have been surely more pertinent than some of the articles listed in the references. One could wonder, for example, why the authors quoted 3 articles 1 ,2,7 which have the same title and an almost identical content.
Finally, the patient is reported to have less than 1% FX clotting activity. This is surprising and probably untenable since all homozygous patients with homozygous FX Friuli defect have always shown levels of about of 3% to 6% of normal in the intrinsic and/or extrinsic systems. A level so low suggests the concomitant presence of inhibitors, liver damage, or amyloidosis.
This reported very low value is also in contradiction with what was stated by the authors in the discussion, namely that the FX activity in these patients is not very low (page 334, second column).
To avoid further wrong statements and to clarify fully the story of factor X Friuli, we thought it useful to summarize the events in the Table 1.
The Long Story of FX Friuli Disorder
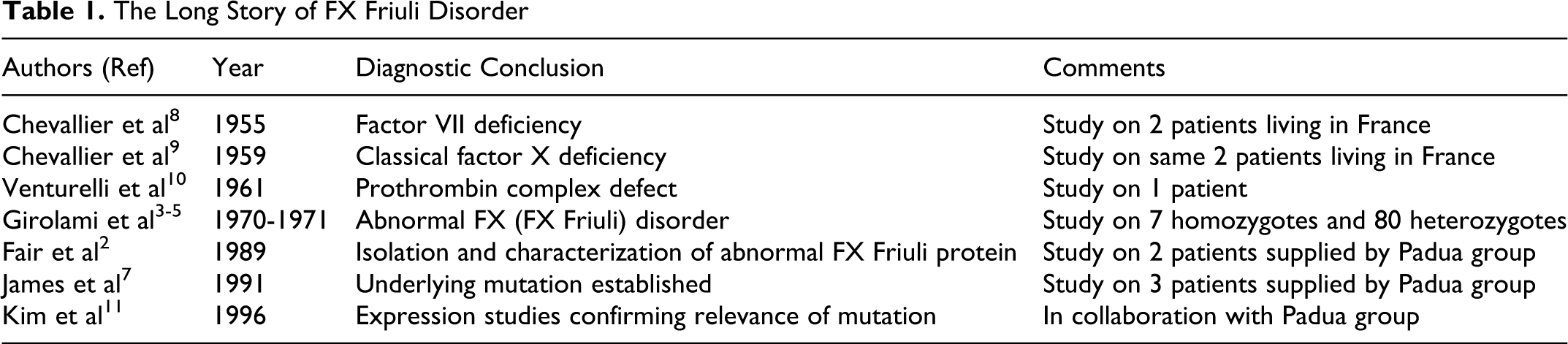
This gives an idea of the complexity and the difficulties encountered in the diagnosis of this peculiar defect and will be of interest to the readers. Many attempts were made through the years by several authors 8 –10 but the right diagnosis was reached by the Padua group in 1970. 4,5 Molecular biology confirmation of the correctness of the diagnosis was reached later in collaboration with the Department of Biochemistry of the Texas University at Tyler. 7,11
We do hope the authors will show in the future a more appropriate approach to the subject and a due respect to the work of those who originally studied the disorders and, more importantly, to the truth.