
Abstract
The information about the thromboembolic events, the optimal treatment choice, the dose, and duration of antithrombotic therapy in children are limited. More clinical data are required. Recombinant tissue plasminogen activator (r-tPA) is increasingly used in pediatric thrombosis. We retrospectively analyzed the clinical course of 7 children (9.3 ± 2.1 years; 34 days to 16 years) with arterial thrombosis (n = 1) and intracardiac thrombosis (n = 6). The children were treated with r-tPA. The dose ranged between 0.2 and 0.4 mg/kg per h infused for 3 to 4 hours. This dose was repeated between 2 to 7 times till the thrombolysis was achieved. Treatment side effects were closely monitored. Complete clot lysis was achieved in all cases. None of them had severe bleeding except mild recurrent epistaxis occurring in 2 cases. In conclusion, r-tPA is an effective and safe therapy under close hemostatic control in children.
Introduction
Venous and arterial thromboembolic events (TEs) are increasingly recognized in infants and children. Within the general population, the incidence of thrombosis in children is estimated 1 at 0.7 per 100 000. The etiology of thromboembolism is thought to be multifactorial and one of the underlying reasons is cardiac disorders such as congenital heart diseases (CHDs), intracardiac defects, cardiac procedures, and acquired heart disease. In the literature, the frequency of thrombosis related to cardiac abnormalities was reported 1 –4 as 5.5% to 20%. Intracardiac thrombi might lead to life-threatening situations. 5 –7 Therefore, adequate and effective treatment must be instituted. Recombinant tissue plasminogen activator (r-tPA) is one of the choices. There is only limited information on the optimal choice of r-tPA, dose, and duration of thrombolytic therapy in children. Therefore, in this report, we retrospectively investigated the efficacy and safety of r-tPA in 7 children with cardiac disorders treated consecutively between the years 2005 and 2010.
Patients and Methods
Patients treated with systemic thrombolytic agents between the years 2005 and 2010 were identified from the registry of Department of Pediatrics, running under the control of university hospital director. The registry had records of 128 consecutive patients admitted with thromboemboli. Seven (5%) of these children were treated with systemic thrombolytic agents due to increased risk of mortality and organ damage. The validity of information was overseen by the directors of pediatrics. Gender, age, vascular involvement and location, underlying etiology, diagnostic investigations, treatment, duration of admission, and outcome at discharge were recorded. Characteristics of the patients were shown in Table 1 . The study was approved by the ethics committee of the Uludag University, and the parents of the patients gave informed consent before the enrollment.
Characteristics of Patients.
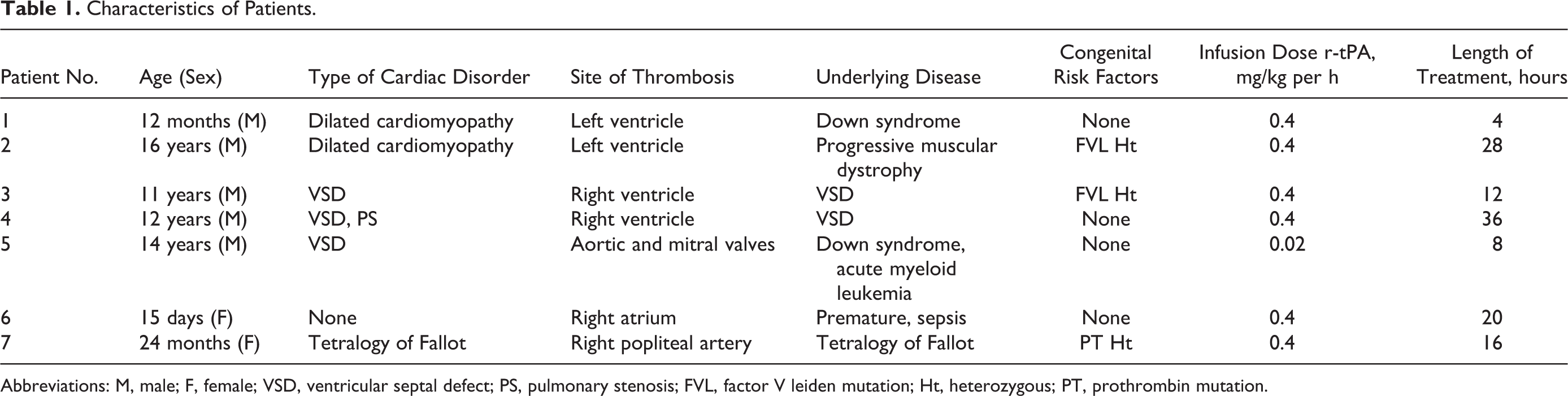
Abbreviations: M, male; F, female; VSD, ventricular septal defect; PS, pulmonary stenosis; FVL, factor V leiden mutation; Ht, heterozygous; PT, prothrombin mutation.
Acquired (systemic infection, surgery, heart disease, and catheter) and congenital prothrombotic risk factors (factor V Leiden, prothrombin 20210 G-A gene mutation and methylenetetrahydrofolate reductase [MTHFR] 677C-T genotypes) were searched.
The diagnosis of formation of an intracardiac or vessel thromboemboli was established using Hewlett-Packard echocardiograph 2000 or 5500, equipped with a 3.5-MHz transducer. Two-dimensional and Doppler recordings were obtained in parasternal long- and short-axis, apical 2- and 4-chamber and subcostal views and Doppler ultrasonography and/or clinical examination. The initial echocardiograms were reviewed by an experienced echocardiographer masked to subsequent clinical outcomes. Thrombus was defined by the presence of a distinct echogenic mass, identified in at least 2 different views and associated with regional or global wall-motion abnormality.
Thrombolytic Treatment
Arterial and venous thrombi that have potential to cause mortality, organ damage, or loss of limb are well-accepted indications for thrombolytic therapy. Central venous catheter was placed in all patients for enabling thrombolytic therapy. Their activated partial thromboplastin time (aPTT), thrombin time (TT), and serum fibrinogen level were in normal ranges prior to each r-tPA administration. The complete blood count was determined in every 6 to 12 hours. The fibrinogen levels and platelet counts were kept above 100 mg/dL, 75 000 mm3, respectively, during treatment. The dose of r-tPA ranged between 0.06 and 0.4 mg/kg per h (Actilyse 50 mg flacon). The systemic infusion was given continuously for 4 hours of courses. The treatment response was evaluated by recurrent echocardiography and/or Doppler ultrasonography and clinical examination after the end of each r-tPA course. If there was no evidence of response, second or third 4 hours infusions were immediately administered and the dose was increased according to the recent American College of Chest Physician guidelines. 8 The infusion was interrupted if there was persistent bleeding. These children received fresh frozen plasma to stop bleeding. Recombinant tissue plasminogen activator infusion was restarted, after the bleeding was stopped.
The effect of thrombolytic treatment was assessed by echocardiography and Doppler ultrasonography. The treatment was considered successful when the thrombus had been completely dissolved and radiologic imaging confirming recanalization of occluded vessel.
Major bleeding was defined as any event requiring the transfusion of red blood cells or a drop in hemoglobin of >2 g/L, and the others were accepted as minor bleeding. Following the thrombolytic treatment with r-tPA, the patients were commenced on prophylactic antithrombosis treatment with low-molecular-weight heparin (enoxaparin) given 0.5 mg/kg once daily for 3 to 6 months.
Results
All patients (n = 7) received r-tPA and the courses ranged from 1 to 8. Mean age of children was 9.3 ± 2.1 years (34 days to 16 years). Five of the patients were male. Table 1 summarizes the precipitating factors associated with the thrombotic event. All children had intracardiac thrombosis except one with arterial thrombosis. Of the 7 children, 6 had an underlying cardiac disorder. These disorders were congenital cardiac defects in 4 children (ventricular septal defect (n = 3), tetralogy of Fallot [n = 1]) and dilated cardiomyopathy in 2 children. One premature baby had developed cardiac thrombus due to severe sepsis.
The median thrombolytic therapy period was 13.4 ± 6.3 hours (6 hours to 3 days). Treatment effect was consecutively followed by clinical examination and echocardiography and/or Doppler ultrasonography following each course of 4 hours r-tPA infusions. In addition to that, coagulation tests (prothrombin time [PT], aPTT, TT, and fibrinogen) were also evaluated after each course. Treatment of r-tPA caused an increase in PT, aPTT, and TT values and decrease in plasma fibrinogen levels. Complete clot lysis was detected in all patients. In 3 patients (patients 3, 5, and 7), it had to be temporarily interrupted due to bleeding symptoms (mild epistaxis, local bleeding at venopuncture sites) and low fibrinogen levels. Recombinant tissue plasminogen activator infusion was successfully completed after fibrinogen substitution. In addition, coagulation studies showed a modest decrease in fibrinogen concentrations (1-1.5 g/dL) in 4 cases; a transient abnormal elongated PT and activated partial thromboplastin time were seen in all children, but all values were restored to normal. Major bleeding and thrombolytic therapy-related deaths did not occur. None of the children developed rethrombosis at the site of previous thrombus within 8 months after completion of r-tPA treatment.
Discussion
Venous and arterial TEs are potential sources of morbidity and mortality in any patient population. 1 Although management strategies have been well defined in the adults, there is a paucity of such information in the pediatric group. Effective and safe thrombolytic treatment is essential in the management of children with life-threatening thrombosis. Efficient thrombolytic agents available are streptokinase, urokinase, and r-tPA. Nowadays, r-tPA is commonly recommended because of its short halftime (about 5 minutes), nonantigenic qualities, and local-specific action on plasminogen bound fibrin. 8 In this study, r-tPA was used in all children.
In this case series, all children had intracardiac thrombosis. Intracardiac thrombi are considered a life-threatening situation. They have been shown to cause superior vena cava syndrome, occlusion of the tricuspid valve, and valvular insufficiency with rapidly progressive heart failure. They can also act as a potential nidus of infection and lead to dissemination of emboli to the lungs or the systemic circulation. 4 For these reasons, adequate and effective treatment must immediately be instituted.
The optimal use, dosage, efficacy, bleeding, and toxicity of tissue plasminogen activator thrombolysis in children are unknown. We chose a low dose of r-tPA starting dose of 0.06 mg/kg per h in children for both local and systemic thrombolysis rather than published recommendations of 0.1 to 0.5mg/kg per h. The dose was increased (maximum dose: 0.4 mg/kg per h) according to the treatment response confirmed by consecutive echoencephalography. The treatment effect of different dosing schedules for r-tPA has not been compared in children. A perception of increased r-tPA-associated bleeding has limited the use of thrombolysis in children, and a recent report with standard doses (0.5 mg/kg per h average dose) also revealed significant bleeding complications. 7,8 Increasing evidence suggests that low-dose infusion of r-tPA may be at least as effective as published standard doses and related to a decreased incidence of major bleeding. 7 Hartmann et al have also shown complete resolution in 78% of neonates treated with a continuous infusion of 0.2 mg/kg per h of r-tPA. 9 In the same report, minor bleeding complications at the puncture sites were observed in 14%. No major bleeding was reported. Major bleeding and death rate with the use of r-tPA within the dose interval between 0.5 and 0.7 mg/kg per h, occurred in 15% and 1.5% of the cases, respectively. 9 –14 The same dose was reported in 22% of the cases for the minor bleedings including mucosal and bleedings from vascular puncture sites. 12–13 In our series, severe complications, intracerebral hemorrhage, and death did not occur. Only 3 children had minor bleedings.
The thromboembolism etiology is thought to be multifactorial caused by congenital and acquired risk factors. Acquired risk factors in our data were present in all children. The frequency of thromboses related to cardiac abnormalities was reported as 5.5% by the Society of Turkish Pediatric Hematology. 15 In this report, congenital cardiac malformation was the major cardiac disorder causing intracardiac thrombosis. Another study by Gurgey et al showed that in 8 of 12 patients with intracardiac thrombosis and CHD had either cyanotic or acyanotic CHD. 5 In our series, 5 patients had CHD and 2 patients had dilated cardiomyopathy.
In the current study, factor V Leiden, MTHFR, and PT 20210 mutations were analyzed and present in 3 of 7 children. The German childhood thrombophilia group showed that the frequencies of the genetic and acquired risk factors in 261 thrombotic children were 57% and 62%, respectively. 16 Günes et al also have reported that acquired and inherited risk factors precipitating TE in 60 children were present in 75% and 40% of the children, respectively. 17 Therefore, thrombosis in children is usually thought to be triggered by the acquired factors.
In our cohort of patients, low dose r-tPA seemed to be found effective and relatively safe and did not lead to any significant bleeding complications. Limitations of this study are the small size of the patient population. Cooperative prospective controlled trials in children can provide long-term data on the true efficacy and safety of this therapy.