
Abstract
Purple toe syndrome is a rare complication of warfarin therapy. It occurs usually after 3 to 8 weeks of therapy and it is caused by cholesterol emboli from atheromatous plaque. Sudden onset of pain in affected area, typically in toes and feet, is the main characteristic of the syndrome. We describe a case of a 65-year-old female with purple toe syndrome after 6 weeks of warfarin. Indication of warfarin was a proximal deep venous thrombosis, which developed after prolonged immobilization. Factor V (FV) Leiden and persistent high FVIII activity were found as additional eliciting factors for venous thromboembolism. After warfarin withdrawal and enoxaparin treatment, symptoms disappeared promptly but a slight discoloration of the toe persists.
Introduction
Oral anticoagulation treatment (OAT) with warfarin (Warfarinum natricum, Orion, Espoo, Finland) has been used for many years worldwide. The most frequent complication of OAT is bleeding, but the variety of nonhemorrhagic, cutaneous lesions have been also reported: allergic purpura, alopecia, skin necrosis, and purple toe syndrome.1,2 This syndrome is an extremely uncommon complication and it is characterized by the sudden appearance of usually bilateral, painful, purple lesions on the toes and sides of the feet that blanch with pressure. The syndrome usually develops 3 to 8 weeks after the start of warfarin therapy. However, earlier 3 and later 4 onset of symptoms have been described as well. Purple toe syndrome was first described by Fisher et al in 1960, 5 followed by Feder and Auerbach in 1961. 6 Multiple cholesterol emboli syndrome) in 4 patients was described by Rosansky et al. 7
Case Report
A 65-year-old caucasian female was referred to our department in the end of April 2008 for pain and swelling of the left low limb. Eight weeks previously, while skiing in France, she collided with a snowboarder at a high speed. She was transported to the local emergency department. x-Ray revealed a fracture of the left clavicle and magnetic resonance imaging (MRI) revealed a fracture of pelvis and os sacrum. After 1 week, she was transferred to the Czech Republic and admitted to our orthopedic department. The patient has been taking simvastatin (Zocor—simvastatinum, Merck Sharp Dohme, Haarlem, the Netherlands) for 4 years to treat hypercholesterolemia.
Upon arrival, MRI confirmed the fracture of pubic bone and an impact on the lateral mass of os sacrum. She was treated conservatively and after 6 weeks of rehabilitation, she was discharged. Enoxaparin (Clexane—enoxaparine natrium, Sanofi-Aventis, France) 0.4 mL was given subcutaneously once daily as prophylaxis for thromboembolic events during her entire stay in hospital and tapered off after she was discharged. She was able to ambulate with minimal weight bearing on the left leg. There were no problems until 7 days after discharge when the pain in the left leg began. She took some pain medications, but the next day left leg was swollen and she came to our hospital. Ultrasound detected proximal deep vein thrombosis (DVT, femoropopliteal) in the left leg.
Clexane in therapeutic dosage was administered and warfarin was introduced on the second day. After 1 week, she was discharged with international normalized ratio (INR) in the therapeutic range (2-3) for 2 successive days. Selected laboratory results and thrombophilia workup at the time of DVT diagnosis are shown in the Table 1
.The OAT was monitored in our center for thrombosis and INR was carefully maintained in the therapeutic range. Interestingly,
aCoagulation and thrombophilia work-up
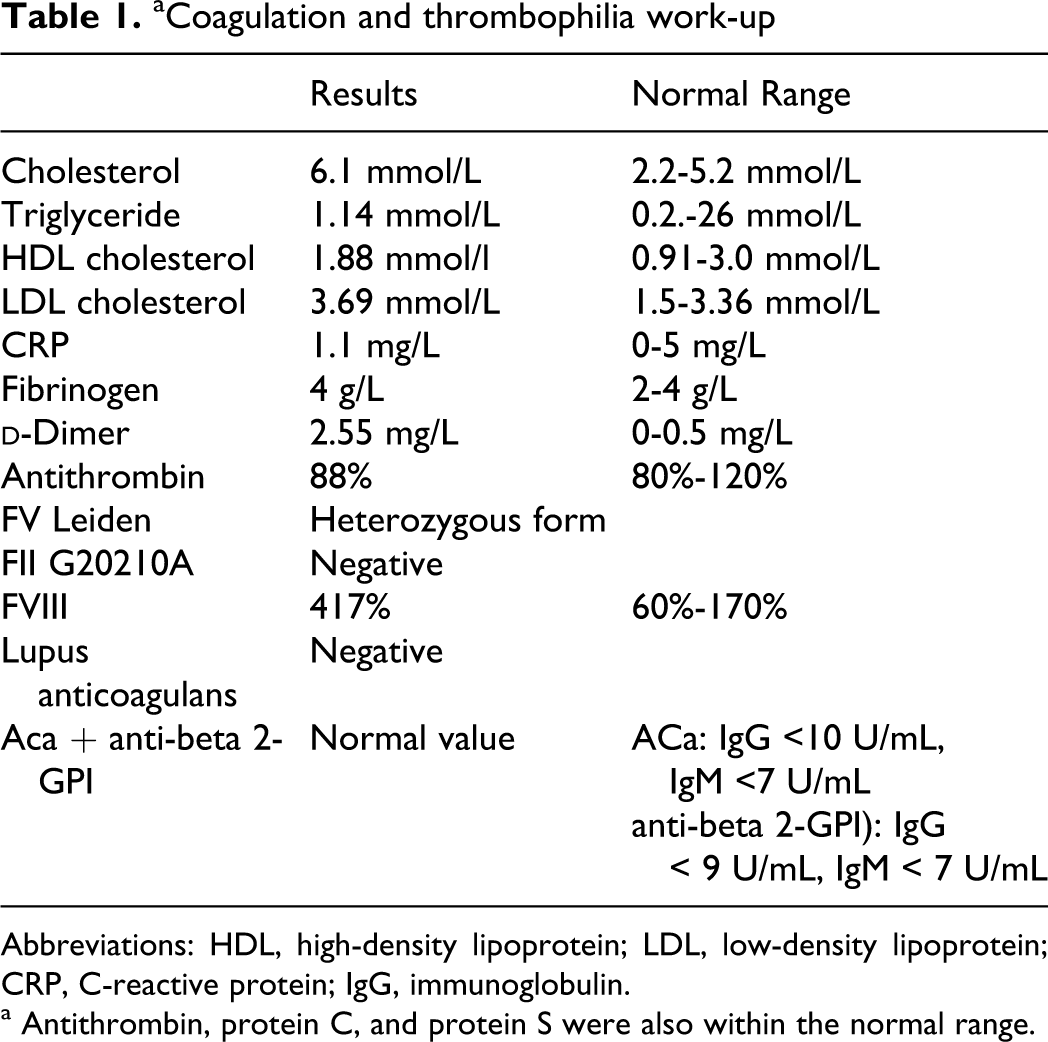
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; CRP, C-reactive protein; IgG, immunoglobulin.
a Antithrombin, protein C, and protein S were also within the normal range.
We therefore excluded underlying malignancy (examination of the gastrointestinal, reproductive organs, and breasts) and initiated thrombophilia workup. Factor V (FV) Leiden mutation in heterozygous form and high FVIII activity were detected. There was no positive personal or family history of VTE. She was once pregnant, without thrombotic event.
After 6 weeks of commencing OAT, she felt burning pain on her left toe. The toe became purple in 1 day, without loss of pulse and sensitivity, whereupon she returned to our center for thrombosis. Physical examination revealed normal pulse and temperature. Dominant finding was the purple color of left toe and sides of the feet with blanched under pressure. The patient’s history of OAT, duration of OAT, hypercholesterolemia in therapy, typical symptoms, and discoloration of skin led us to diagnose purple toe syndrome (Figure 1). Warfarin was immediately stopped and therapy was switched to half a therapeutic dose of enoxaparin. Pain and sensation improved rapidly within 1 week. After 3 months, only a slight, mild purplish area at the sides of left feet (Figure 2) remained. The dose of enoxaparin was reduced to prophylactic level (40 mg daily). Since then, there have been no signs of recurrent DVT or local problems. After 6 months, we wanted to stop enoxaparin as United States detected only residual partial calf thrombosis, but we respected patients' wish to continue therapy. Doppler ultrasound 6 months later was completely normal. At this time, enoxaparin is still administered in the prophylactic dose. We also checked FVIII and its activity remained elevated: 309% in March 2009 and 344% in November 2009. Other markers of inflammation such as C-reactive protein and erythrocyte sedimentation rate were normal.

Purple toe

Toe after 3 months
Discussion
Purple toe syndrome is a very rare reported adverse effect of warfarin. The mechanism of this syndrome has various explanations. Direct toxic effect on the capillaries has been postulated. However, the phenomenon is currently attributed to cholesterol crystals being released usually from an atheroslerotic plaque and travels along with the bloodsteam to the other places in the body, where it obstructs blood vessels. It is a result of warfarin-induced bleeding into atherosclerotic plaques. Anticoagulant therapy interferes with the formation of a protective fibrin layer over an eroded or ulcerated plaque as well as cementing of cholesterol and atheromatous debris by fibrin. In general, antithrombotic therapy aims to inhibit the formation and growth of an occluding thrombus in a damaged vessel and, in this way, to decrease the risk of embolism. The important protective role of fibrin in stabilizing atherosclerotic lesions is reinforced by the occurrence of peripheral cholesterol emboli during thrombolytic and heparin therapy.
Purple toe syndrome is described as a purple dark cutaneous lesion with blue discoloration of the feet and lower leg.8,9 The big toes are affected most often. The majority of lesions are bilateral and the skin blanches with pressure. The toes do not appear to have hemorrhagic lesions. Despite apparently good arterial flow, patients with multiple cholesterol emboli experience intense pain. The syndrome typically occurs 3 to 8 weeks after starting warfarin. It is a rare syndrome and the optimal treatment in patients needing continued anticoagulation is not well known. This treatment consists of the discontinuation of warfarin and replacement with heparin. This therapy usually leads to a marked improvement in symptoms over the next few days, but no significant change in the appearance of toes. The toes remain pain free but residual discoloration is present. 3 Recently, the first case describing late onset purple toe syndrome with successful substitution with fondaparinux was described. 4 We believe further warfarin therapy should be contraindicated. This view is supported in a case of a patient who had had a relapse of symptoms after continuing warfarin therapy against medical advice. Cholesterol embolism is treated by removing the cause and with supportive therapy; statin drugs have been found to improve the prognosis.
The definitive goal of treatment of atheromatous embolization is the eradication of the source of atheromatous material. Emboli frequently originate from the aorta originating below renal artery. 10 There is a lack of data about the association of thrombophilia and purple toe syndrome. It has been described only in antiphospholipid syndrome. 11
What is a particularly interesting in our case is the onset of DVT despite low-molecular-weight heparin, persistent significant elevation of
To the best of our knowledge, this is the first purple toe syndrome with FV Leiden mutation in heterozygous form and high FVIII activity described in the literature so far.
Conclusion
We encountered a patient who developed purple toe syndrome after 6 weeks of warfarin therapy for DVT. The OAT was stopped and switched into enoxaparin. The symptoms improved rapidly and local affection disappeared as well. Although it is a rare complication of this therapy, clinicians should be aware of this syndrome in patients taking warfarin.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by research project No. 00179906 of Czech Ministry of Health.