
Abstract

Mean platelet volume (MPV) is a marker of platelet reactivity. High level of MPV is an unfavorable predictor of cardiovascular events among the survivors of acute myocardial infarction (AMI). There are limited studies that evaluate the correlation between high MPV level and postinterventional thrombolysis in myocardial infarction (TIMI) flow grade reflecting reperfusion in patients with AMI. Herein, we aimed to evaluate the correlation between MPV level and reperfusion in patients with AMI treated with primary percutaneous coronary intervention (PCI).
A total of 556 patients with an ST elevation AMI were evaluated retrospectively. Upon admission, MPV was measured by the automated hematology analyzers Sysmex XT-1800i (Roche Diagnostic, Istanbul, Turkey). The patients' angiographic data were evaluated from catheter laboratory records and postinterventional TIMI flow was documented for each patients. Herein, we evaluated reperfusion with epicardial TIMI flow grade, and we did not check other methods assessing myocardial perfusion including ST segment resolution, myocardial blush grade, and biochemical markers increment. Patients were classified according to MPV quartiles and TIMI flow for statistical analysis. The TIMI 0-1-2 flow defined as abnormal reperfusion and MPV quartiles was calculated as <7.2 fL, ≥7.2-7.8 fL, ≥7.8-8.5 fL, and ≥8.5 fL. All groups compared by chi-square and Pearson correlation analysis according to preinterventional clinical and demographic features. The TIMI 3 flow was secured in the 73.7% of the cases and rest of the patients were classified as abnormal reperfusion. Patients were treated with 300 mg aspirin and 600 mg clopidogrel loading dose before intervention and 10 000 U unfractionated heparin applied to all cases after intubation of infarct-related artery. Glycoprotein 2b/3a inhibitor (tirofiban) was not utilized before and also during the procedure. Patients with abnormal postinterventional TIMI flow are treated with tirofiban after procedure. Mean MPV was 7.89 ± 1.0 fL, ranging from 5.1 to 13.0 fL. Increased age, female gender, presence of diabetes mellitus, and hypertension were associated with abnormal reperfusion (Table 1 ). The MPV levels and MPV quartiles did not differ in abnormal reperfusion group contrary to literatures.1,2 Univariate regression analysis also did not show correlation between MPV, MPV quartiles, and TIMI <3 flow (odds ratio [OR] = 0.88, P = .24; and OR = 1.13, P = 0.67, respectively). It was reported that higher MPV level was associated with no-reflow and unfavorable long-term outcomes in the AMI.1–3 However, different cutoff points for MPV level was proposed in each studies (Huczek et al 10.3 fL, Maden et al 9.05 fL, and Goncalves et al 9.1 fL), which might be associated with the usage of different analyzing devices. Standard threshold for MPV level still has not been defined. Demirin et al 4 had investigated MPV level in the healthy participants, and they proposed MPV >11.7 fL as a cutoff point for thrombotic arterial disease. Acceptance of such a higher threshold could change the former investigations' result. In our study, fourth quartiles of MPV (≥8.5 fL) was more frequent in the abnormal reperfusion group, but it was statistically insignificant (P = .29). Median value of fourth quartiles was 9.0 fL, which may indicate cutoff point. Correlation of higher MPV level and abnormal reperfusion was also obtained in the patients with AMI treated with thrombolytics. Yasar et al speculated that higher MPV value may indicate impaired response to thrombolytics and they defined 8.8 fL as a cutoff point of MVP. 5 Successful deployment of stent may counteract larger sized platelets with mechanical effect, which could be an explanation of better reperfusion result, irrespective of MPV level in the primary PCI. Such scenario may be a supporting evidence of our reverse results. Huczek and colleagues demonstrated 10.8% abnormal postinterventional TIMI flow that indicates better success rate comparing to our series (26.3% abnormal TIMI flow in our series). The main differences between 2 series were the loading dose of clopidogrel (300 vs 600 mg in our series) and prehospital delay time (4.7 ± 3.6 hour in MPV normal group and 6.1 ± 4.6 hour in MPV high group vs 5.2 ± 2.6 hour in MPV normal group and 5.7 ± 2.9 hour in MPV high group in our series). These 2 occasions could explain the contrast result for MPV, although higher success rate of intervention was obtained.
Distribution of Clinical and Demographic Characteristics of the Patients According to Postinterventional TIMI Blood Flowa
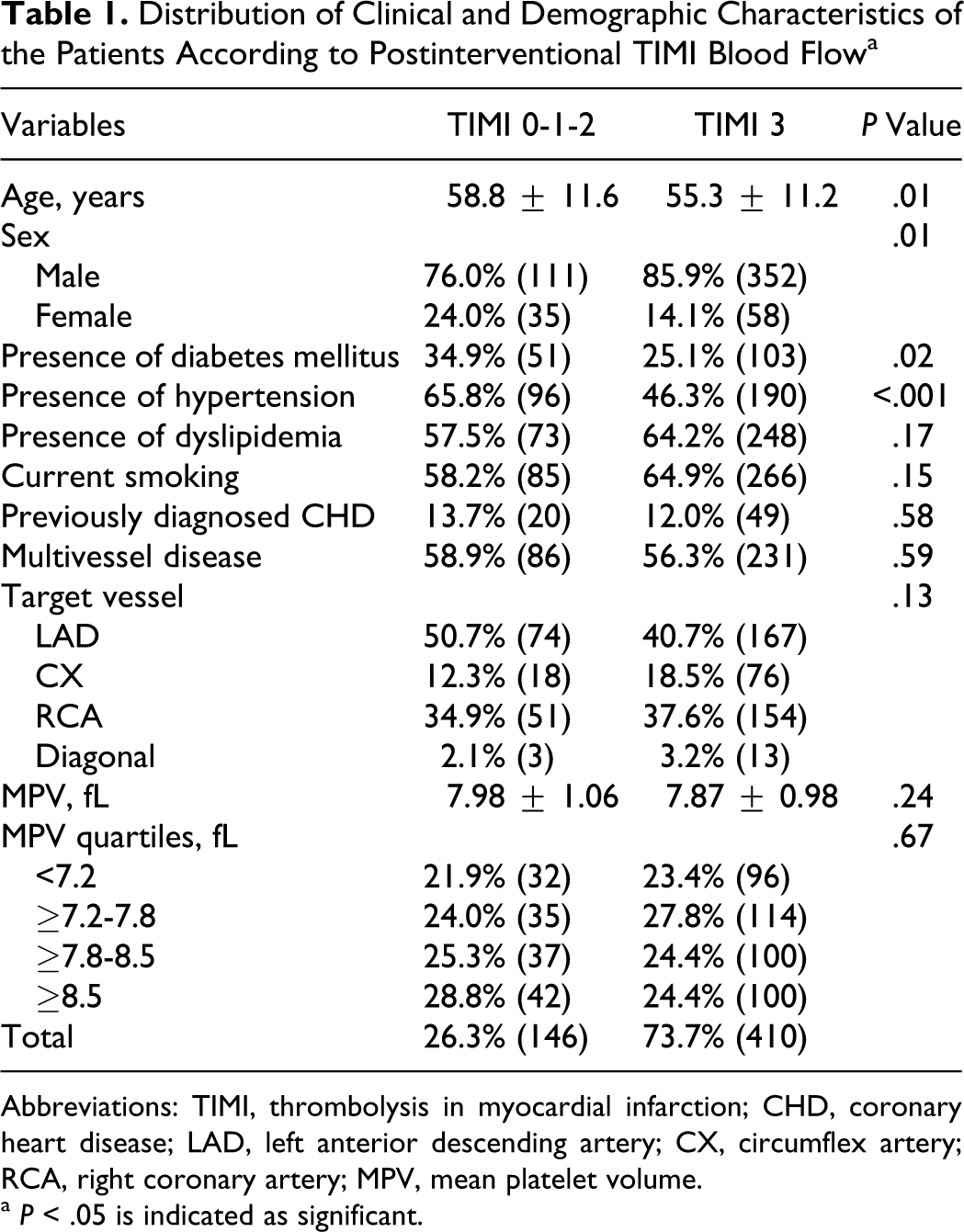
Abbreviations: TIMI, thrombolysis in myocardial infarction; CHD, coronary heart disease; LAD, left anterior descending artery; CX, circumflex artery; RCA, right coronary artery; MPV, mean platelet volume.
a P < .05 is indicated as significant.
MPV reported as predictive factor of abnormal TIMI flow and also a prognostic factor in the AMI with previous studies. However, a standard cut-off point that contribute to risk assessment in the AMI has not been proposed yet. In addition, successful primary PCI may diminish the worse predictive effect of MPV on postinterventional TIMI flow, as our study result. Furthermore, large-scale investigations including different types of measurement techniques and devices would clarify the cutoff point and clinical implication of MPV in the patients with AMI.