
Abstract
Hormonal agents (estrogen and progesterone) are being studied for their use in bleeding. This observance was initially explored in a patient with hereditary hemorrhagic telangiectasia (HHT) with epistaxis had variation in bleeding depending on her menstrual cycles.1 Thus, hormonal therapy was initially used in patients with HHT to control episodes of epistaxis.2 The literature on hormonal therapy in patients with life-threatening bleeding from gastrointestinal (GI) lesions is very limited. There are a few clinical trials in patients with chronic bleeds. However, no definite guidelines exist on their use in life-threatening GI bleeding in patients with uremia. Here, we describe a case with a life-threatening GI bleeding requiring multiple endoscopies and intensive care unit stay that responded to conjugated estrogens. We have done extensive research on English medical literature on PubMed and Google Scholar on the use of hormonal therapy for GI bleeding in patients with renal failure, and here we present the data as a review.
Case
A 67-year-old lady with a medical history of hypertension, end-stage renal disease on hemodialysis, polycystic kidney disease, and multiple medical problems initially presented to an outside hospital following a fall. She was diagnosed with fracture of left hip and underwent surgery. Her postoperative period was complicated by gram-negative bacteremia. Six days after admission, she developed melena and hemoglobin dropped to 6 g/dL. Esophagogastroduodenoscopy (EGD) revealed gastric ectasia. She continued to have melena and hematemesis and had a total of 5 endoscopies and multiple transfusions prior to transfer. At our institution, 2 days after the transfer (24 days after her initial admission), a capsule endoscopy was nondiagnostic for any evidence of bleeding. On the day after the capsule endoscopy, she developed melena and her hemoglobin dropped to 6.7 g/dL despite 6 units of packed red blood cells (PRBCs). The patient was started on octreotide drip, intravenous proton pump inhibitor, desmopressin, and epsilon amino caproic acid. An emergent EGD showed normal upper and middle third of the esophagus, and mild esophagitis seen in the lower third of the esophagus. Blood was found in the stomach and fundus and an ulcer was seen in the stomach. There were areas of angioectasia and angiodysplasia (AD) found in the antrum and empiric norepinephrine intragastric injections were given. Over the next 4 days, she continued to have intermittent bleeding requiring 3 more units of PRBC’s. In addition, she also received multiple transfusions with fresh frozen plasma, cryoprecipitate, and platelets. A repeat EGD showed blood in the fundus and multiple ulcers in the fundus of the stomach. At this time, empiric left gastric artery embolization was performed. Despite the procedure, after 1 day, the patient had another significant GI bleed requiring blood transfusions and a repeat EGD. This again showed active upper GI bleed from the stomach. At this time, it was decided to start the patient on conjugated estrogens 25 mg intravenous for 5 days. Within 2 days of starting conjugated estrogens, patient hemoglobin stabilized and she did not require any further endoscopies. Her hemoglobin improved to 9.7 g/dL and discharged to a nursing home. The patients bleed did recur a few months later; however, conjugated estrogens were discontinued at her nursing home.
Discussion
The rationale for the use of hormonal therapy in the treatment of bleeding from vascular malformations was provided by observations that epistaxis due to HHT decreased during pregnancy and worsened in the postmenopausal period, 2 several days before menstruation, or after oophorectomy. 1 Since then, hormonal therapy has been reported in several case reports, series, and a few uncontrolled and controlled studies of GI bleeding. All these publications report either an arrest of bleeding or an increase in hemoglobin for the duration of follow-up and an important reduction of transfusion requirements. The successes have been mainly anecdotal and none of the trials have been on patients with renal failure and with a life-threatening GI bleeding.
To date, there are seven3–9 reported trials on the efficacy of conjugated estrogens in patients with renal sufficiency and bleeding. In addition, Bronner et al 10 used either estrogen alone or estrogen in combination with progestrone. Also, there are 5 reported clinical trials on the use of combined (estrogen and progestrone) therapy.11–15 Van Cutsem et al 14 published the first crossover study in 1990. However, this study was somewhat extended to another publication 15 and thus reducing the comparisons among only 4 different studies. We have summarized them in Table 1. All these studies are heterogeneous in type of patients included, method of study, associated with or without additional therapy, inclusion and exclusion criteria, and so on, and hence, it is difficult to compare results across these studies. The studies have included both men and women and none of them have reported a difference in response based on this. None of the trials have included patients with life-threatening GI bleeding with renal failure. Our patient is unique in this regard and also that this life-threatening bleed, which did not respond to any other modality of treatment, responded to hormonal therapy and the patient survived a long and complicated hospital stay. The exact mechanism of action of hormones is unknown. However, a number of theories have been proposed. 2 These include stabilization of fragile vessels through increased keratinization of surrounding squamous epithelium, improvement of possible coagulation abnormalities, shortening of bleeding time, reduction in leaking from fragile capillaries, improved vasoconstrictive effect of vasopressin and noradrenaline 16 , and reduction of mesenteric blood flow through increased stasis. In patients with HHT, estrogen and progesterone receptors have been detected in nasal and skin telangiectatic lesions. Estrogen-receptor binding and improved endothelial integrity have been observed in patients with HHT. Hormones may also decrease vascular endothelial growth factor. 17 There is no evidence, however, that the GI ADs will regress with this therapy.
Summary of Clinical Trials Reported to Date on the Use of Hormonal Therapy for GI Bleeding.
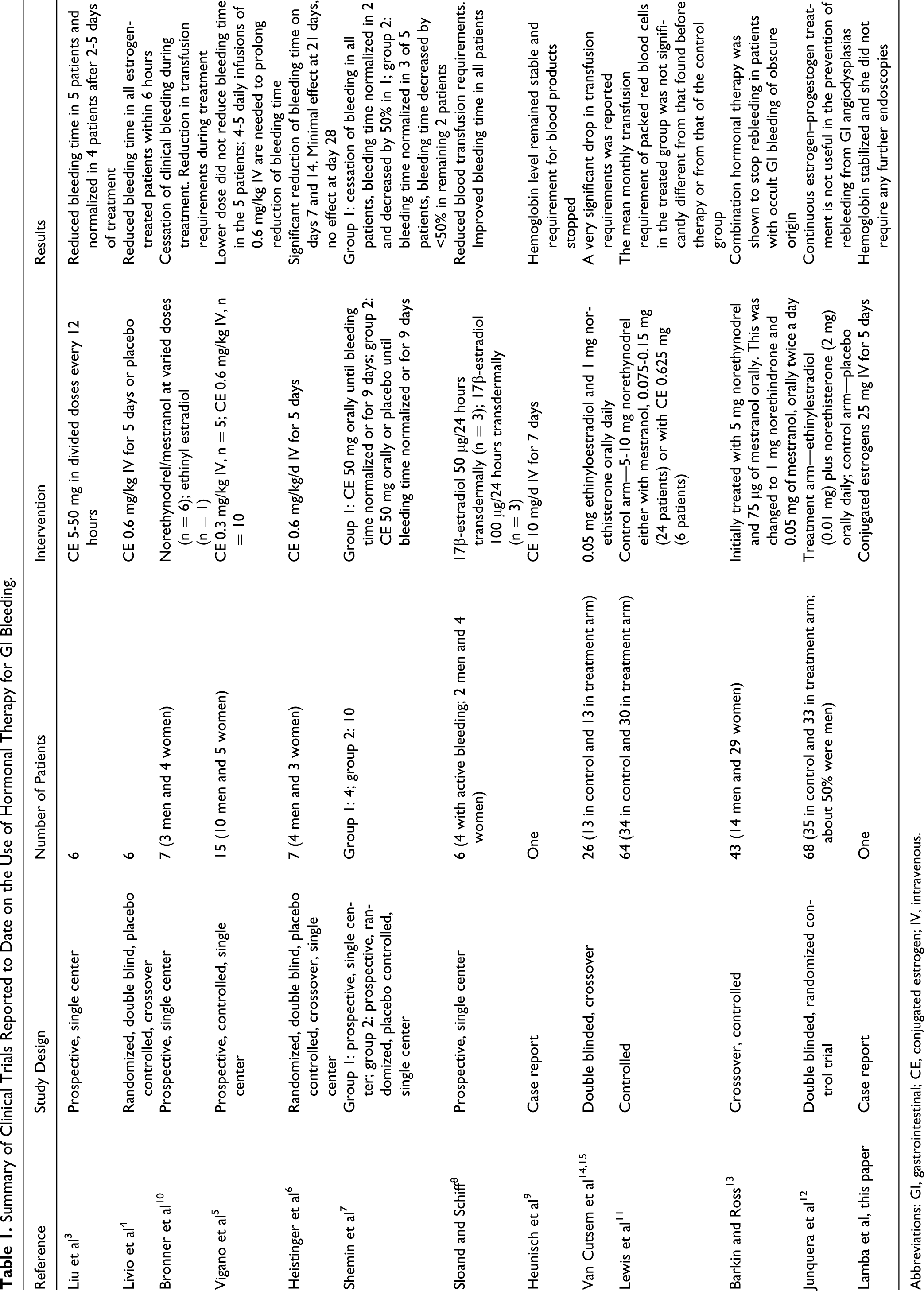
Abbreviations: GI, gastrointestinal; CE, conjugated estrogen; IV, intravenous.
Galbusera et al 18 recently published guidelines for management of bleeding in dialysis patients. They recommend the use of conjugated estrogens by intravenous infusion in a cumulative dose of 3 mg/kg as daily divided doses (ie, 0.6 mg/kg for 5 consecutive days). This should be utilized in persistent chronic bleeding. There are no guidelines about their use in an acute life-threatening bleed like our case. At this time, therefore, there are no clear guidelines on this issue. Furthermore, there are a number of relative and absolute contraindications on the use of these hormones. In addition, there are several side effects that may limit use of these hormones. These include an increased risk of stroke, deep vein thrombosis, pulmonary embolism, and myocardial infarction. Hormonal therapy is also associated with an increased risk of endometrial and breast cancer, dementia, gall bladder disease requiring surgery, hypercalcemia, and angioedema. Contraindications include undiagnosed abnormal genital bleeding, known, suspected, or history of estrogen-dependent neoplasia except in appropriately selected patients being treated for metastatic disease, active deep vein thrombosis, pulmonary embolism, or a history of these conditions, active or recent arterial thromboembolic disease, liver dysfunction or disease, known thrombophilic disorders, and known or suspected pregnancy.
To conclude, estrogen therapy is currently reserved for selected patients, in whom frequent recurrent bleeding occurs and endoscopy or surgery is ineffective or inapplicable due to the extent or distribution of the lesions or existence of comorbid disorders. Our patient had a total of 8 upper GI endoscopies with unsuccessful use of epinephrine injections, cautery, and argon photocoagulation. She also had extensive comorbidities, including renal failure, hypertension, and prior bowel surgery, making her ineligible for gastrectomy. However, after initiation of estrogen therapy, her bleeding stopped, and she was eventually discharged from the hospital. Estrogen therapy can thus be used for emergency and short-term control of bleeding with more definitive therapies to follow. We, therefore, urge other physicians to be aware of the use of hormonal therapy in similar patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.