
Abstract
The frequency of methylenetetrahydrofolate reductase (MTHFR) mutations varies between racial and ethnic groups, and there are also conflicting data regarding MTHFR gene mutations in Asian patients with venous thromboembolism (VTE). The aim of this study was to examine the association between common MTHFR gene mutations (677C>T and 1298A>C) and risk of VTE in Koreans. This study was a retrospective case–control study. We enrolled 203 patients with VTE and 403 controls. For the 677C>T polymorphism, there was no difference in the frequency of the CT genotype and TT genotype between the patients with VTE and the controls. However, in the recessive analysis (CC + CT vs TT), the frequency of the TT genotype was significantly higher in VTE than in controls (odds ratio = 1.700; 95% confidence interval = 1.108-2.607, P = .015). In conclusion, the TT genotype of MTHFR 677C>T increases the risk of VTE in Koreans. This finding was supported by meta-analysis of previous Asian studies.
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), represents a public health concern in Western and Asian countries. Venous thromboembolism often complicates the course of hospitalized patients but may also affect ambulatory and otherwise healthy people. The classic risk factors for VTE are cancer, surgery, prolonged immobilization, fracture, paralysis, oral contraceptive use, and hereditary coagulopathies. In addition to these classic risk factors, hyperhomocysteinemia is a known risk factor for both arterial and venous thrombosis. Hyperhomocysteinemia can result from inherited or nutrient-related disturbances in homocysteine metabolism; hyperhomocysteinemia attributed to inherited deficiencies is associated with alterations in enzymes such as cystathionine β-synthase, methionine synthase, and methylenetetrahydrofolate reductase (MTHFR).
MTHFR is a key enzyme in folate metabolism and DNA synthesis. It catalyzes the reduction of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, the methyl donor for the conversion of homocysteine to methionine, while 5,10-methylenetetrahydrofolate and its derivatives are essential cofactors for both thymidylate and de novo purine synthesis. 1 Two common polymorphisms (MTHFR 677C>T and 1298A>C) are associated with mild-to-moderate hyperhomocysteinemia that is attributed to a 50% to 60% decrease in the catalytic activity of MTHFR.2,3 The 677C>T mutation results in the substitution of valine for alanine at position 222 of the MTHFR enzyme, resulting in a thermolabile enzyme with a 50% reduction in activity.2,4,5 The 1298A>C mutation, which is located within the C-terminal regulatory domain of MTHFR, results in the substitution of glutamate for an alanine residue and is associated with a mild reduction in enzymatic activity.3,6,7
In a previous meta-analysis, 8 Den Heijer et al reported that the MTHFR 677TT genotype is associated with a 20% higher risk of VTE compared with the 677CC genotype. Subsequently, hyperhomocysteinemia has become recognized as an important independent risk factor for VTE. The frequency of MTHFR gene mutations varies between racial and ethnic groups, and there are also conflicting data regarding MTHFR gene mutations in Asian patients with VTE. Therefore, mutations of the MTHFR gene remain a controversial risk factor for VTE in Asians.9–11 The aim of this study was to examine the association between common MTHFR gene mutations and risk of VTE in Koreans.
Patients and Methods
Study Population
Patients with consecutive VTE with recent (<6 months) objective diagnosis of DVT or PE, who visited to the CHA Bundang Medical Center (Seongnam, Korea) or Kyemyung University hospital (Daegu, Korea) between May 2005 and December 2009, were enrolled in the study. We enrolled the patients with symptomatic VTE and excluded the patients with asymptomatic VTE. Venous thromboembolism was defined as provoked or unprovoked, depending on the presence or absence of any of the following risk factors: recent surgery (<3 months), recent trauma/fracture (<3 months), immobilization (>7 days), malignancy, stroke, severe medical disease, autoimmune disease, pregnancy, use of oral contraceptives, and known inherited thrombophilia. Venous thromboembolism was classified as provoked in the presence of at least one of these risk factors. The control group was selected among patients visiting the CHA Bundang Health Promotion Center for periodic health examinations, who had no medical history of VTE. The Institutional Review Board of CHA Bundang Medical Center approved the research protocol and written informed consent was obtained from all participating individuals.
Sample and Data Collection
Venous blood samples were collected by venipuncture into tubes containing sodium citrate for MTHFR genotyping. We reviewed all medical records for clinical data (age, gender, smoking status, history of hypertension, diabetes, hyperlipidemia, thrombotic disease, and malignancy).
Methylenetetrahydrofolate Reductase Genotyping
DNA was extracted from peripheral blood leukocytes using DNA extraction kits (QIAmp blood kit, Qiagen, Hilden, Germany) according to the manufacturer’s protocol. The MTHFR 677C>T and 1298A>C genotypes were identified as previously described. 2 The regions containing the 2 polymorphisms were amplified separately using the following polymerase chain reaction (PCR) primers: 677 nucleotide polymorphism, 5′-GCA CTT GAA GAG AAG GTG TC-3′ (forward) and 5′-AGG ACG GTG CGG TGA GAG TG-3′ (reverse); 1298 nucleotide polymorphism, 5′-CTT TGG GGA GCT GAA GGA CTA CTA C-3′ (forward) and 5′-CAC TTT GTG ACC ATT CCG GTT TG-3′ (reverse). Human genomic DNA (200 ng) was amplified with 100 pmol of each forward and reverse primer, 1.5 mmol/L MgCl2, 0.2 mol/L each deoxynucleotide triphosphate, and 1 unit Taq polymerase (Takara; Seongnam, South Korea) in a total volume of 100 μL. The PCR conditions were as follows: denaturation at 94°C for 5 minutes, followed by 35 cycles at 94°C for 30 seconds, 51°C for 30 seconds, and 72°C for 30 seconds, and a final elongation at 72°C for 5 minutes. The PCR products were digested with HinfI (for nucleotide 677) or Fnu4HI (for nucleotide 1298) for 2 hours at 37°C.
Amplification success was monitored by 3.0% agarose electrophoresis. For the 677 nucleotide, an undigested PCR product (203 bp) indicated a homozygous wild type, 3 bands of 203, 173, and 30 bp indicated the heterozygous genotype, and 2 bands of 170 and 30 bp indicated the homozygous genotype. For the 1298 nucleotide, a single band of 138 bp indicated wild-type and 2 fragments of 119 and 19 bp indicated the homozygous genotype.
Meta-Analysis
For meta-analysis of Asian studies, extensive search was performed on all major electronic data bases (MEDLINE, PUBMED, and EMBASE) from 1990 to 2010 (using the terms MTHFR, methylenetetrahydrofolate reductase, and venous thrombosis, pulmonary embolism, deep vein thrombosis, or venous thromboembolism). Therefore, we enrolled 453 cases and 722 controls from 3 previous studies (Taiwan, Japan, and China) and present study (Korea).9–11 We performed the meta-analysis with random effect model.
Statistical Analysis
Statistical analyses were conducted using the SPSS 19.0 (IBM, New York). Differences between the patients with VTE and controls were assessed using the Student t test. Categorical variables were compared using the chi-square test. The distribution of allele frequencies for the MTHFR 677C>T and 1298A>C gene polymorphisms were calculated by Chi-square test to determine whether the observed genotype distributions conformed to the expected Hardy-Weinberg equilibrium. Logistic regression analyses were performed to calculate the relative risk of VTE associated with each genotype. Multivariate analysis was performed to select independent risk factors for VTE among genotypes and clinical variables using logistic regression analysis. Odds ratio (OR) and corresponding 95% confidence interval (CI) were calculated. Statistical significance was determined to be P < .05.
Results
Characteristics of the Studied Population
Baseline characteristics of patients with VTE and controls are shown in Table 1. A total of 203 patients with VTE and 403 controls were enrolled in the study from January 2006 to June 2009. The mean age of the patients with VTE was 56 years, and 103 patients were male (50.7%). There was no significant difference in the clinical variables between patients with VTE and the controls. Venous thromboembolism was unprovoked in 93 patients and provoked in 110. Among the provoked VTE cases, VTE was related to recent surgery, trauma/fracture, immobilization (n = 62), malignancy (n = 12), stroke (n = 17), severe medical disease (n = 5), autoimmune disease (n = 4), pregnancy (n = 4), use of oral contraceptives (n = 5), inherited thrombophilia (n = 6), and other (n = 9).
Baseline Characteristics in Patients With VTE and Control Individuals.
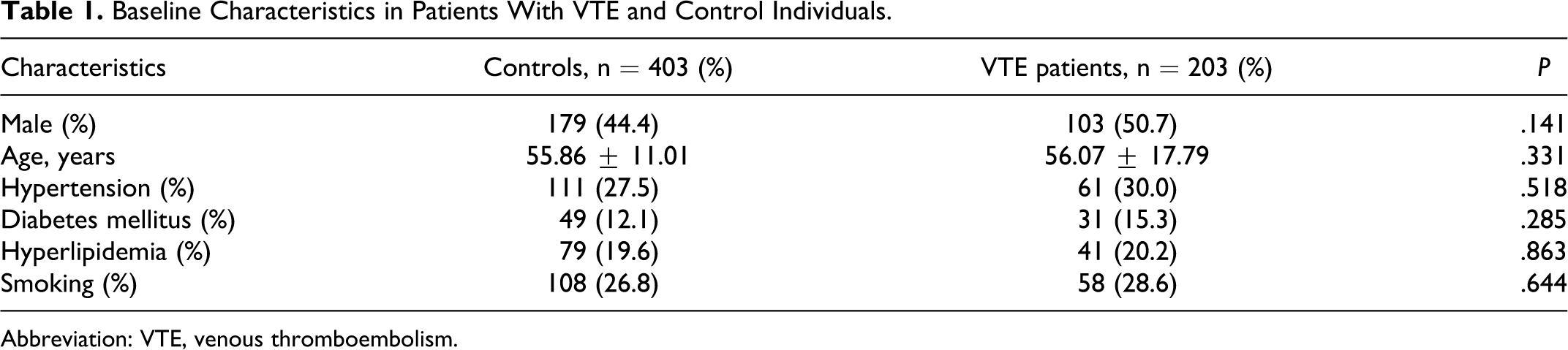
Abbreviation: VTE, venous thromboembolism.
Genotype Frequencies of MTHFR 677 C>T in Patients With VTE
In the patients with VTE, genotype frequencies for wild type (CC), heterozygous (CT), and homozygous (TT) forms of the 677C>T polymorphism were 36.5% (n = 74), 40.4% (n = 82), and 23.2% (n = 47) compared with 34.7% (n = 140), 50.4% (n = 203), and 14.9% (n = 60), respectively, in the controls. The genotype frequencies of the MTHFR 677C>T polymorphism conformed to Hardy-Weinberg equilibrium in controls and in patients with VTE (P > .01). In multivariate analysis, after adjusting for age, sex, and clinical variables (hypertension, diabetes mellitus, hyperlipidemia, and smoking), no differences in the frequency of the CT heterozygous (OR = 0.755; 95% CI = 0.513-1.110, P = .152) and TT homozygous (OR = 1.443; 95% CI = 0.894-2.328, P = .134) genotype were found between patients with VTE and the controls. A comparable OR was calculated for the 677C>T polymorphism in the unprovoked VTE group, showing no association between unprovoked VTE and the CT heterozygous genotype (OR = 0.686; 95% CI = 0.405-1.163; P = .162) or TT homozygous genotype (OR = 1.419; 95% CI = 0.761-2.647; P = .271). When homozygous and heterozygous patients were combined for statistical analyses (dominant model), genotype distributions were not significantly different between patients with VTE and the controls. However, when heterozygous and wild-type patients were combined for statistical analyses (recessive model), the frequency of the homozygous genotype was significantly higher in patients with VTE (OR = 1.700; 95% CI = 1.108-2.607, P = .015) than in controls (Table 2).
Genotype Frequencies of MTHFR 677C>T and 1298A>C in Patients With VTE and Control Individuals.
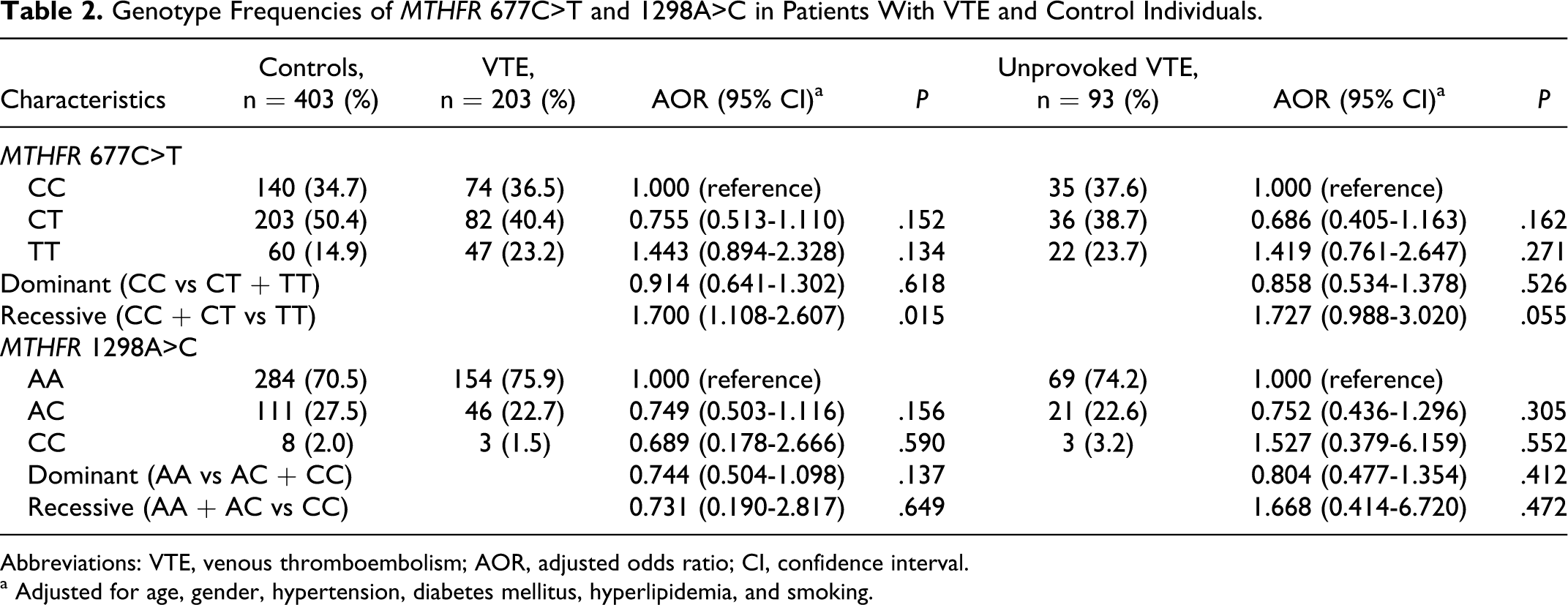
Abbreviations: VTE, venous thromboembolism; AOR, adjusted odds ratio; CI, confidence interval.
a Adjusted for age, gender, hypertension, diabetes mellitus, hyperlipidemia, and smoking.
Genotype Frequencies of MTHFR 1298 A>C in Patients With VTE
In the patients with VTE, genotype frequencies for wild type (AA), heterozygous (AC), and homozygous (CC) forms of the 1298A>C polymorphism were 75.9% (n = 154), 22.7% (n = 46), and 1.5% (n = 3) compared with 70.5% (n = 284), 27.5% (n = 111), and 2.0% (n = 8), respectively, in the controls. In multivariate analysis, after adjusting for age, sex, and clinical variables, no difference in the frequency of the AC heterozygous genotype and CC homozygous genotype was found between patients with VTE and the controls. A comparable OR was calculated for the 1298A>C polymorphism in the unprovoked VTE group, showing no association between unprovoked VTE with the MTHFR 1298A>C polymorphism (Table 2).
Combined Genotype Frequencies of MTHFR 677 C>T and 1298 A>C in Patients With VTE
Combined genotype analyses were conducted to evaluate the combined effect of the 2 common MTHFR polymorphisms on the risk of VTE. Six combined genotypes (CC/AA, 22.2%; CC/AC, 12.8%; CC/CC, 1.5%; CT/AA, 30.5%; CT/AC, 9.9%; and TT/AA, 23.2%) were estimated from the 2 polymorphisms in patients with VTE. No differences in the frequency of combined polymorphisms of the MTHFR gene were found between patients with VTE and the controls (Table 3).
Combined Genotype Frequencies for MTHFR 677C>T and 1298A>C in Patients With VTE and Control Individuals.
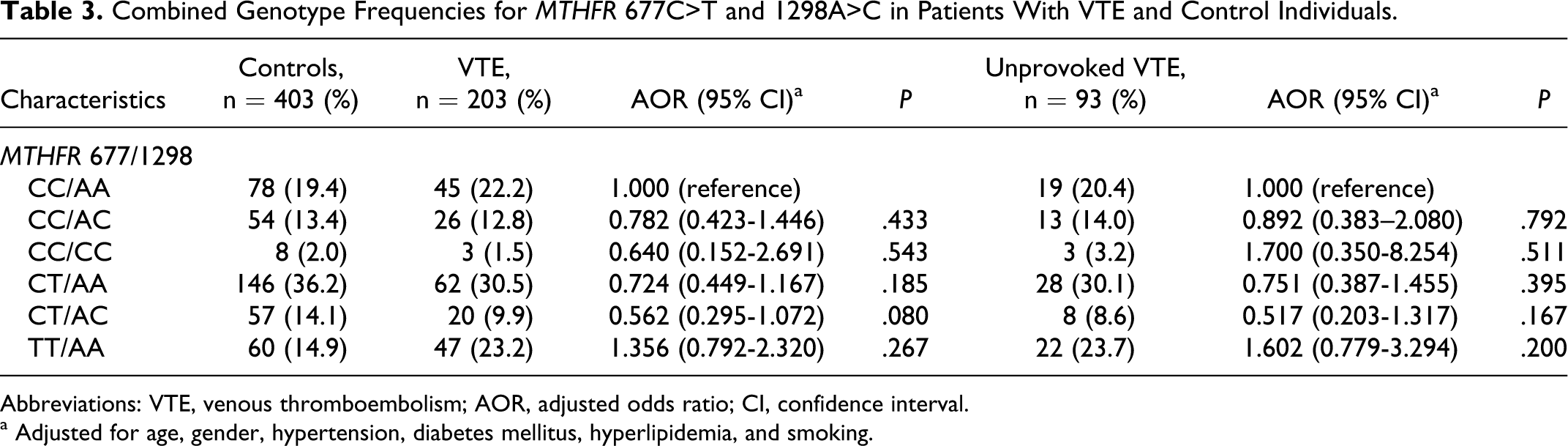
Abbreviations: VTE, venous thromboembolism; AOR, adjusted odds ratio; CI, confidence interval.
a Adjusted for age, gender, hypertension, diabetes mellitus, hyperlipidemia, and smoking.
Meta-Analysis of Asian Studies for MTHFR 677 C>T and 1298A>C in Patients With VTE
We analyzed combined data of 3 previous studies conducted in Asian populations and our study. There was no heterogeneity between the results of studies (P = .526). The TT homozygous genotype of 677C>T polymorphism was an independent risk factor for VTE in studies conducted on Korean and Chinese populations, but the Japanese (P = .19) and Taiwanese (P = .05) studies did not show statistically significant association.9–11 When we performed meta-analysis for these 4 Asian studies, we found that the TT homozygous genotype for the 677C>T polymorphism increases the risk of VTE in the combined Asian population (OR 1.726; 95% CI: 1.189-2.506; Figure 1).
Discussion
In the present study, we investigated whether 677C>T and 1298A>C mutations of the MTHFR gene are related to an increased risk of VTE in Korean populations. The current study showed that the TT homozygous genotype of 677C>T was an independent risk factor for development of VTE in the recessive analysis (CC + CT vs TT). However, no association was observed between the 1298A>C polymorphism and risk of VTE. Additionally, when we conducted meta-analysis with data from 3 previous Asian studies and our study,9–11 the findings of our study indicated that the TT homozygous genotype for the 677C>T polymorphism increases the risk of VTE in Asian populations.
Hyperhomocysteinemia is the key factor that links the MTHFR 677C>T mutation and VTE. There are several mechanisms that can explain the relationship between hyperhomocysteinemia and VTE. Previous studies reported that hyperhomocysteinemia activates factor V, 12 reduces protein C activation, inactivates the cofactor activity of thrombomodulin, 13 suppresses anticoagulant heparan sulfate expression, 14 and blocks tissue plasminogen activator. 15 However, the association between homocysteine levels and VTE remains controversial. From meta-analysis, Den Heijer et al reported that a 5-μmol/L increase in measured homocysteine was associated with a 27% (OR = 1.27; 95% CI = 1.01-1.59) increased risk of VTE in prospective studies and a 60% (OR = 1.60; 95% CI = 1.10-1.34) increased risk in retrospective studies. 8 Meta-analysis of the association between MTHFR 677C>T mutation and the risk of VTE showed that the TT homozygous genotype was associated with a 15% (95% CI = 2-13) higher risk of VTE than the CC genotype in European populations. 8 However, the TT genotype had no effect on VTE in North American populations. These contrasting results may be partially explained by different folate intake habits in these countries.16,17 However, the genetic contribution of MTHFR mutations to VTE has not been elucidated in Asian populations. Three studies were previously conducted in Asian populations (Taiwanese, Japanese, and Chinese).9–11 The Japanese and Taiwanese studies showed no statistically significant association between MTHFR mutations and the risk of VTE,9,10 whereas the Chinese study showed that the CT heterozygous genotype and TT homozygous genotype were, respectively, associated with a 36% (OR = 3.6; 95% CI =1.7-7.7) and 34% (OR = 3.4; 95% CI = 1.3-9.5) higher risk of VTE compared with the CC genotype. 11 Our study also showed a significant association between the TT homozygous genotype and the risk of VTE in recessive analysis. This result was supported by meta-analysis of the Asian studies, which showed that the TT homozygous genotype was an independent risk factor for VTE in the combined Asian population (OR = 1.726; 95% CI = 1.189-2.506).
The second important genetic variant of the MTHFR gene implicated in VTE pathogenesis is the 1298A>C mutation. This polymorphism is known to have a lower effect on MTHFR activity than the 677C>T mutation. Combined heterozygosity for the 677C>T/1298A>C polymorphisms showed association between higher homocysteine concentrations and decreased plasma folate3,18 in some studies. Therefore, the 1298A>C mutation might be involved in the pathogenesis of VTE in an additive manner when in combination with 677C>T. 1 This could be explained by the distinct location of the 2 polymorphisms: the 677C>T mutation is in the region encoding the N-terminal catalytic domain, whereas the 1298A>C substitution is located in the C-terminal regulatory domain. 1 However, when only the 1298A>C mutation was studied in the different populations, no association with VTE was observed.19,20
The present study has several limitations. First, although our study had the largest sample size among Asian studies, the study population was still not large enough to generalize the association between MTHFR gene mutations and the risk of VTE in Asians. Therefore, we performed meta-analysis of all Asian studies to support our results. Second, we could not consider the individual participants' dietary habits and did not measure homocysteine levels, therefore we could not evaluate the correlation between homocysteine levels and MTHFR mutations in Koreans, because homocysteine levels are affected by dietary habits and genetic mutations.
In conclusion, our study suggests that TT homozygous genotype of 677C>T was a significant risk factor for VTE in Asian populations. Our results might increase the understanding of association between MTHFR mutations and VTE in Asian populations. Further larger and prospective studies are needed to confirm the relationship between MTHFR mutations in Asians.
Footnotes
Authors' Note
Moon Ju Jang and Young Joo Jeon contributed equally to this work.
Acknowledgments
The biospecimens for this study were provided by the
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: partly supported by the National Research Foundation of Korea Grant funded by the Korean Government (2009-0070341) and partly supported by Priority Centers Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2009-0093821).