
Abstract
The contribution of the hemostatic system in the development of cardiovascular disease (CVD) in patients with type 2 diabetes is not completely defined. The aim of this study was to elucidate associations of hemostatic factors with the development of CVD in patients with type 2 diabetes. Patients with type 2 diabetes without CVD (n = 113), with CVD (n = 94), and controls without CVD (n = 100) were enrolled in this study. Several hemostatic markers were measured. A disturbed hemostatic balance in patients with type 2 diabetes was observed as illustrated by hypofibrinolysis and increased levels of von Willebrand factor (vWF) and plasminogen-activator inhibitor 1 (PAI-1). Patients with type 2 diabetes with CVD have more thrombin generation compared to patients without CVD. This hemostatic imbalance might contribute to the development of CVD in patients with type 2 diabetes.
Introduction
Cardiovascular disease (CVD) is one of the major complications and the leading cause of death in patients with type 2 diabetes. Many risk factors, including age, gender, obesity, smoking, hyperinsulinemia, hyperglycemia, hypertension, and dyslipidemia contribute to the development of CVD. Disturbance of the hemostatic balance in patients with type 2 diabetes may also be a risk factor for the development of cardiovascular complications.1–3
Several factors are involved to maintain the hemostatic balance, including the vascular endothelium, the coagulation system, and the fibrinolytic system. In patients with type 2 diabetes, levels of von Willebrand factor (vWF) are elevated, which is regarded as an illustration of endothelial dysfunction resulting from vascular injury.4,5 Moreover, these patients show elevated levels of procoagulant proteins, including factor VII, factor VIII, factor X, factor XII, and fibrinogen6–8 that shift the balance to a hypercoagulant condition7,9 and making them more prone to suffer from thrombotic episodes.
The role of the fibrinolytic system in patients with diabetes is still under debate; however, most of the research indicates a hypofibrinolytic condition in these patients that is primarily ascribed to increased levels of plasminogen-activator inhibitor 1 (PAI-1).3,10,11 During fibrinolysis, plasminogen converts into plasmin after activation by tissue-type plasminogen activator (t-PA) or urokinase-type plasminogen activator. Plasmin is the main enzyme of the fibrinolytic system. It cleaves the fibrin fibers, resulting in the formation of partly degraded fibrin. The activation process of plasminogen can be inhibited by PAI-1 via complex formation between PAI-1 and t-PA. Moreover, complex formation between the fibrinolysis inhibitor antiplasmin and plasmin (called PAP complexes) reduces plasmin activity directly. Another inhibitor of the fibrinolytic system is thrombin-activatable fibrinolysis inhibitor (TAFI). After activation, activated TAFI cleaves C-terminal lysine residues from partly degraded fibrin, the binding sites for t-PA and plasminogen, resulting in less plasmin formation.
Although clinical interventions aim to reduce the risk of cardiovascular events, patients with type 2 diabetes still have an increased incidence of CVD. Since the role of hemostatic parameters including fibrinolytic components in the development of CVD in patients with type 2 diabetes is still not completely defined, the aim of this study was to elucidate associations of hemostatic parameters with type 2 diabetes mellitus and with the incidence of CVD in patients with type 2 diabetes. Therefore, we performed a case-control study in which we compared hemostatic parameters between controls and patients with type 2 diabetes and between patients with type 2 diabetes without and with cardiovascular complications.
Materials and Methods
Patients and Plasmas
To elucidate associations of hemostatic markers with CVD in patients with type 2 diabetes, we included patients with type 2 diabetes without and with CVD. Patients with type 2 diabetes that were attending the outpatient clinic of the Slotervaart Hospital in Amsterdam for their yearly routine comprehensive visit were asked to participate in this study. Based on the variation of the hemostatic tests, in particular the clot lysis assay, we aimed for 100 patients with proven CVD and 100 without CVD. Cardiovascular disease as reported by the patient or treating physician was ascertained by reviewing the patient records and/or discharge letters. Coronary artery disease was defined as a history of angina in combination with a proven stenosis of at least 50% at coronary angiography, a previous myocardial infarction, percutaneous transluminal coronary angioplasty, or coronary artery bypass grafting. Ischemic cerebrovascular disease was defined as ischemic stroke with typical neurological deficit lasting at least 24 hours and an early computerized tomography (CT) scan or magnetic resonance imaging (MRI) performed to rule out hemorrhagic stroke or transient ischemic attack in combination with a more than 50% stenosis in the carotid artery. Peripheral vascular disease was defined as typical complaints of intermittent claudication and an ankle to brachial pulse index <0.85, previous percutaneous transluminal angioplasty of a major peripheral artery or previous peripheral arterial bypass surgery for atherosclerotic disease. If patients reported cardiovascular complications that could not be confirmed or had signs or symptoms of CVD that were not confirmed by objective tests, these participants were excluded (n = 13). There were no other additional exclusion criteria. A control group of persons without diabetes mellitus and without CVD was included via recruitment by advertisements in the hospital. Besides the presence of diabetes mellitus, cardiovascular complications and age under 50 years, there were no additional exclusion criteria for this group. Most enrolled controls were accompanying persons of patients of the outpatient clinics at the Slotervaart Hospital. After including 50 persons, the mean age and distribution of gender was compared to the patients with type 2 diabetes. Subsequently, only persons with an age in the right range and with the right gender were asked to participate to obtain a control group of similar age and gender.
Of all participants, blood was taken in the morning between 8 and 10
Baseline Characteristics
Baseline characteristics were determined directly after blood sampling and questionnaires were filled in to obtain additional information such as medication and medical history. Fasting glucose levels were determined in serum using LX-20 (Beckman Coulter, Woerden, The Netherlands) and HbA1c levels were measured using an High-Performance Liquid Chromatography (HPLC) (Adams A1c HA-8160, Menarini, Valkenswaard, The Netherlands).
Lipid Analysis
To determine plasma lipid concentration, citrated plasma was analyzed by commercial assays on COBAS MIRA (Roche, Diagnostica, Woerden, The Netherlands). Used reagents for analyzing triglycerides (TG), total cholesterol, and apolipoprotein B-100 (ApoB) were purchased form Randox (Crumlin, UK) and reagents for analyzing low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol, and apolipoprotein A-1 (ApoA1) were from Wako (Richmond, Virginia).
Hemostatic Parameters
All hemostatic parameters were measured in citrated plasma. Normal pool plasma of at least 200 healthy volunteers was used as a reference. The general coagulation assays, prothrombin time (PT) and activated partial thromboplastin time (PTT), as well as fibrinogen levels were measured on an automated coagulation analyzer (Behring Coagulation System, BCS; Siemens Healthcare Diagnostics, Marburg, Germany). Reagents were from the manufacturer and assays were performed according to manufacturer’s protocols.
The overall fibrinolytic activity was determined by measuring clot-lysis times as described previously, with some minor modifications. 12 Briefly, 47 µL of citrated human plasma was activated by a mixture of 175 IU/mL Actilyse, 17 mmol/L CaCl2, 10 μmol/L phospholipids, and recombinant human tissue factor (Innovin, 105 dilution). Volumes were adjusted to 100 µL with hepes-buffered saline. Turbidity was followed in time at 37°C at 405 nm for 3 hours in a Thermomax microplate reader (Molecular Devices Corporation, Menlo Park, California, USA). The clot-lysis time was defined as the time difference between half-maximal lysis and half-maximal clotting.
Antigen levels of vWF were assayed by enzyme-linked-immunosorbent assay (ELISA) using antibodies from Dako (Glostrup, Denmark). Also, plasma levels of prothrombin fragment 1 + 2 (Siemens Healthcare Diagnostics), PAP complexes (DRG, Marburg, Germany), t-PA (Hyphen BioMed, Andrésy, France), and PAI-1 (Hyphen BioMed) were measured by ELISA. Plasminogen and antiplasmin were determined using the Berichrom plasminogen and antiplasmin activity kits according to the instructions of the manufacturer (Siemens Healthcare Diagnostics).
Statistics
Statistical analyses were performed using SPSS software, version 16.0. Baseline characteristics were compared by independent t-tests between patients with type 2 diabetes and controls and between patients with type 2 diabetes with and without CVD. Hemostatic parameters were adjusted for confounders by using multivariate analysis. To compare patients with type 2 diabetes with controls, parameters were adjusted for arterial disease-related confounders (age, gender, smoking, and medications) and parameters were adjusted for arterial disease and diabetes-related confounders (age, gender, smoking, medications, HbA1c. lipids, body-mass index [BMI], weight, hypertension, and duration of diabetes) to compare patient with type 2 diabetes with and without CVD. Parameters that did not contribute significantly to the model were removed by a step-backwards method. In a secondary analysis, hemostatic parameters were compared between patients with type 2 diabetes with ischemic cerebrovascular disease, coronary artery disease, and peripheral arterial disease to patients with type 2 diabetes without CVD by using multivariate analysis after adjustment for diabetes and arterial disease-related confounders. Odds ratios were calculated by using logistic regression. Results are presented as mean ± standard deviation.
Results
Baseline Characteristics
We enrolled 113 patients with type 2 diabetes without CVD, 94 patients with type 2 diabetes with CVD, and 100 controls in this study. Patients were exclusively selected on the diagnosis for type 2 diabetes and the presence or absence of a history of cardiovascular complications. Consequently, patients used several medications at the time of inclusion. The baseline characteristics of the patients and control persons are presented in Table 1.
Baseline Characteristics
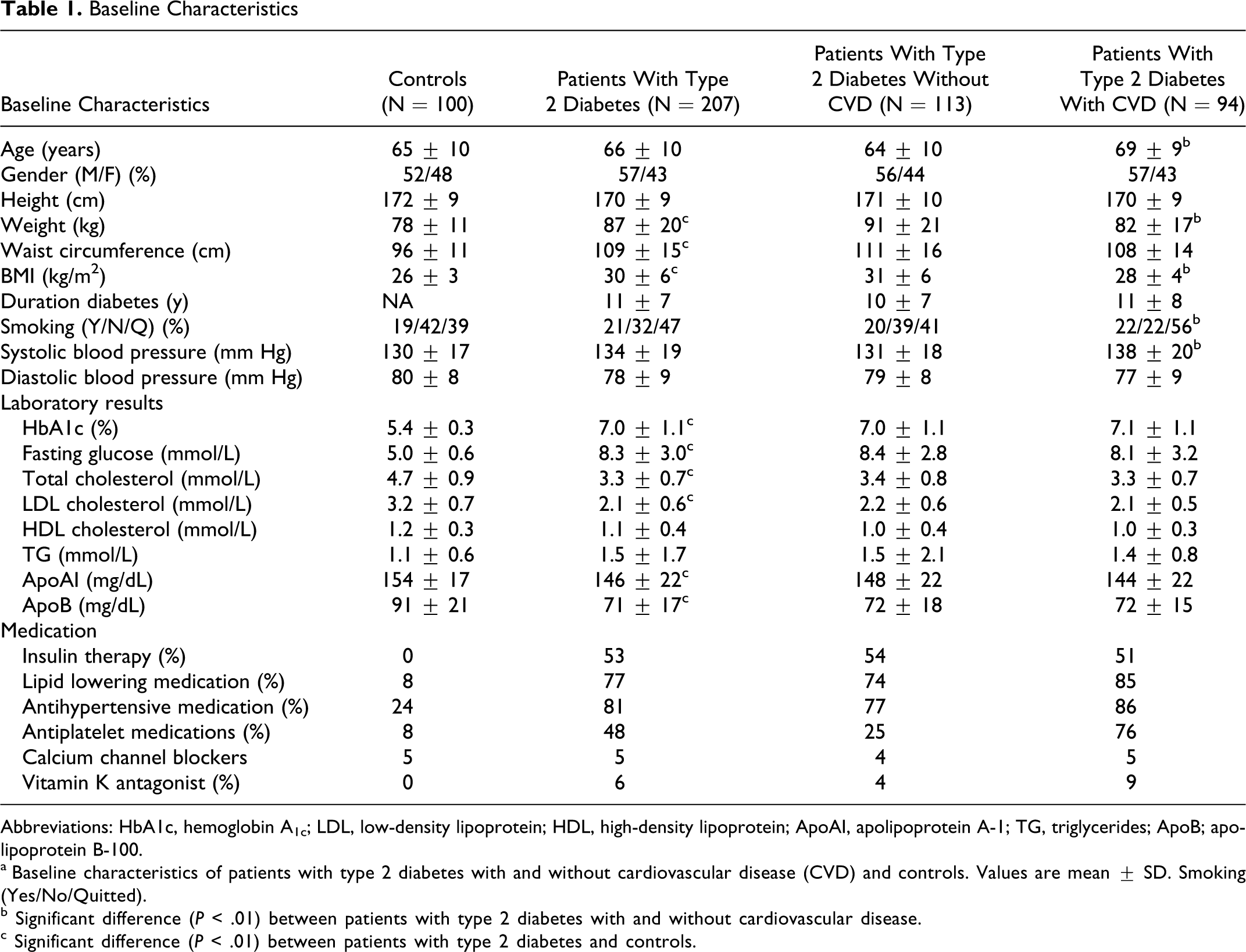
Abbreviations: HbA1c, hemoglobin A1c; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ApoAI, apolipoprotein A-1; TG, triglycerides; ApoB; apolipoprotein B-100.
a Baseline characteristics of patients with type 2 diabetes with and without cardiovascular disease (CVD) and controls. Values are mean ± SD. Smoking (Yes/No/Quitted).
b Significant difference (P < .01) between patients with type 2 diabetes with and without cardiovascular disease.
c Significant difference (P < .01) between patients with type 2 diabetes and controls.
First, patients with type 2 diabetes were compared to the controls. No differences were observed between these groups in age, gender, smoking, and height. As expected, weight, waist circumference, BMI, HbA1c, and fasting glucose were elevated in the patients with type 2 diabetes. Values of the systolic and diastolic blood pressure did not differ statistically between patients with type 2 diabetes and the controls. This may be explained by the higher proportion of patients with diabetes using antihypertensive therapy (diabetes 81% versus controls 24%).
Second, baseline characteristics were compared in patients with type 2 diabetes without and with a cardiovascular complication. No differences were observed between these groups in gender, height, waist circumference, duration of diabetes, diastolic blood pressure, levels of HbA1c, and fasting glucose levels. As expected, patients with diabetes and CVD were older at the time of inclusion and showed increased systolic blood pressure compared to the patients without CVD. Furthermore, an increased number of these patients smoked or had smoked. Although obesity is a risk factor for CVD, we found decreased bodyweight and BMI in patients with diabetes and CVD compared to patients without CVD.
Lipids
To further characterize the participants included in this study, lipid levels were examined (Table 1). As expected, a higher proportion of patients with diabetes used lipid lowering therapy (77% of patients with diabetes versus 8% of the controls). In line with this, we found decreased levels of total cholesterol, LDL-cholesterol, ApoA1, and ApoB in patients with type 2 diabetes compared to the control persons. Triglyceride and HDL-cholesterol levels were similar between patients with diabetes and controls.
In addition, lipoproteins were compared between the patients with type 2 diabetes without and with cardiovascular complications. The lipid-lowering medication taken by 74% of the patients without CVD and by 85% of the patients with CVD might be responsible for no differences in lipoprotein profiles between patients with type 2 diabetes with and without CVD.
Hemostatic Parameters
To elucidate the association of hemostatic markers with type 2 diabetes, we compared several coagulation and fibrinolytic markers between patients with type 2 diabetes and controls (Table 2). Coagulation times, PT and PTT, did not differ significantly between these 2 groups and patients with type 2 diabetes showed hypofibrinolysis as measured by prolonged clot-lysis times (71 ± 21 versus 65 ± 12 minutes) compared to the control group. Focusing on individual hemostatic markers, no significant differences were observed between patients with type 2 diabetes and the controls in levels of prothrombin fragment 1 + 2, fibrinogen,
Hemostatic Parameters of Patients With Type 2 diabetes a
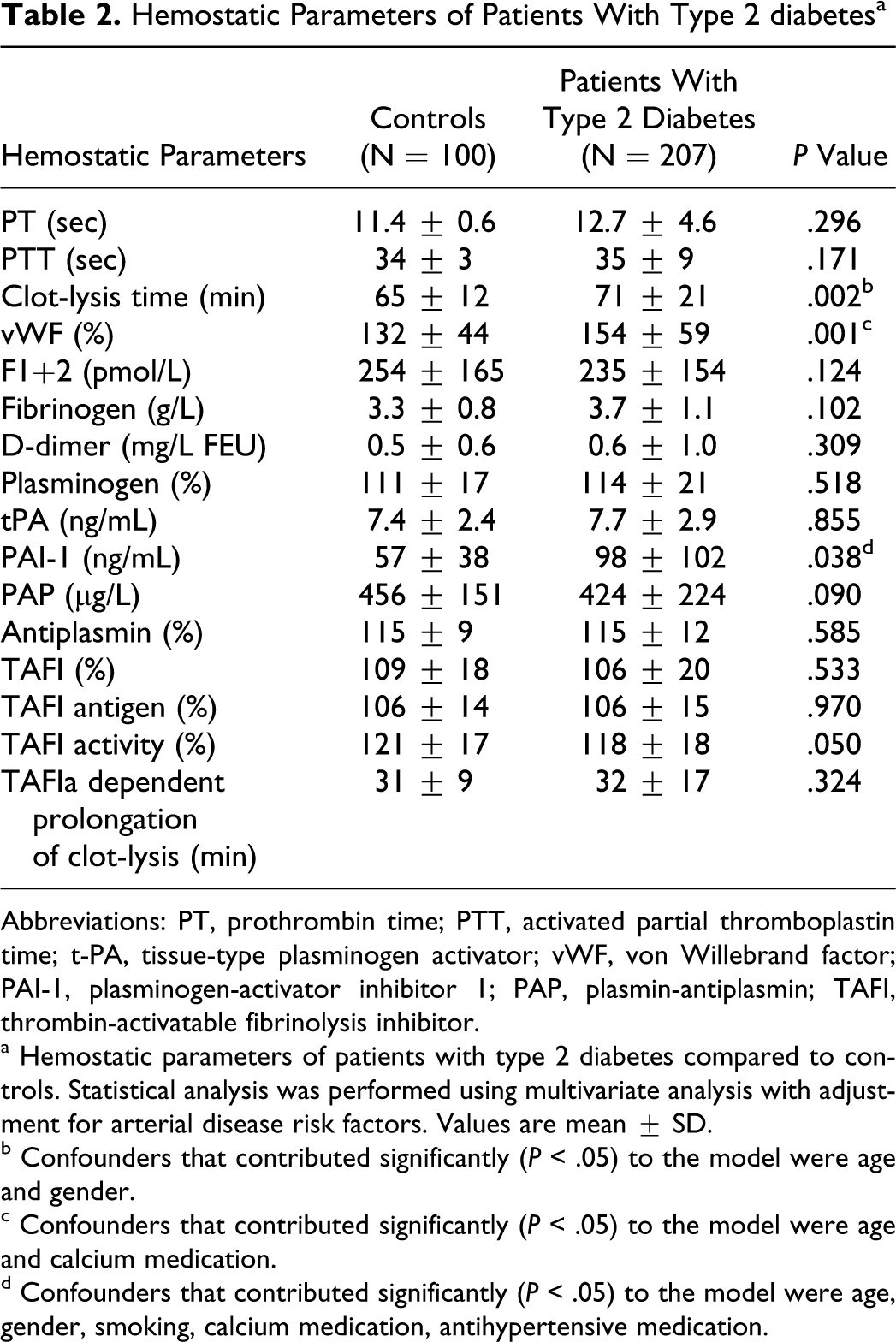
Abbreviations: PT, prothrombin time; PTT, activated partial thromboplastin time; t-PA, tissue-type plasminogen activator; vWF, von Willebrand factor; PAI-1, plasminogen-activator inhibitor 1; PAP, plasmin-antiplasmin; TAFI, thrombin-activatable fibrinolysis inhibitor.
a Hemostatic parameters of patients with type 2 diabetes compared to controls. Statistical analysis was performed using multivariate analysis with adjustment for arterial disease risk factors. Values are mean ± SD.
b Confounders that contributed significantly (P < .05) to the model were age and gender.
c Confounders that contributed significantly (P < .05) to the model were age and calcium medication.
d Confounders that contributed significantly (P < .05) to the model were age, gender, smoking, calcium medication, antihypertensive medication.
To answer the main research question—whether hemostatic markers are associated with the incidence of CVD in patients with type 2 diabetes—we compared levels of several hemostatic parameters between patients with type 2 diabetes without and with CVD (Table 3). No significant differences were observed in the overall coagulation assays (PT and PTT) and in clot-lysis times. Moreover, no differences were found between patients with type 2 diabetes with and without CVD in levels of vWF, fibrinogen,
Hemostatic Parameters of Patients With Type 2 Diabetes Without And With Cardiovascular Disease a
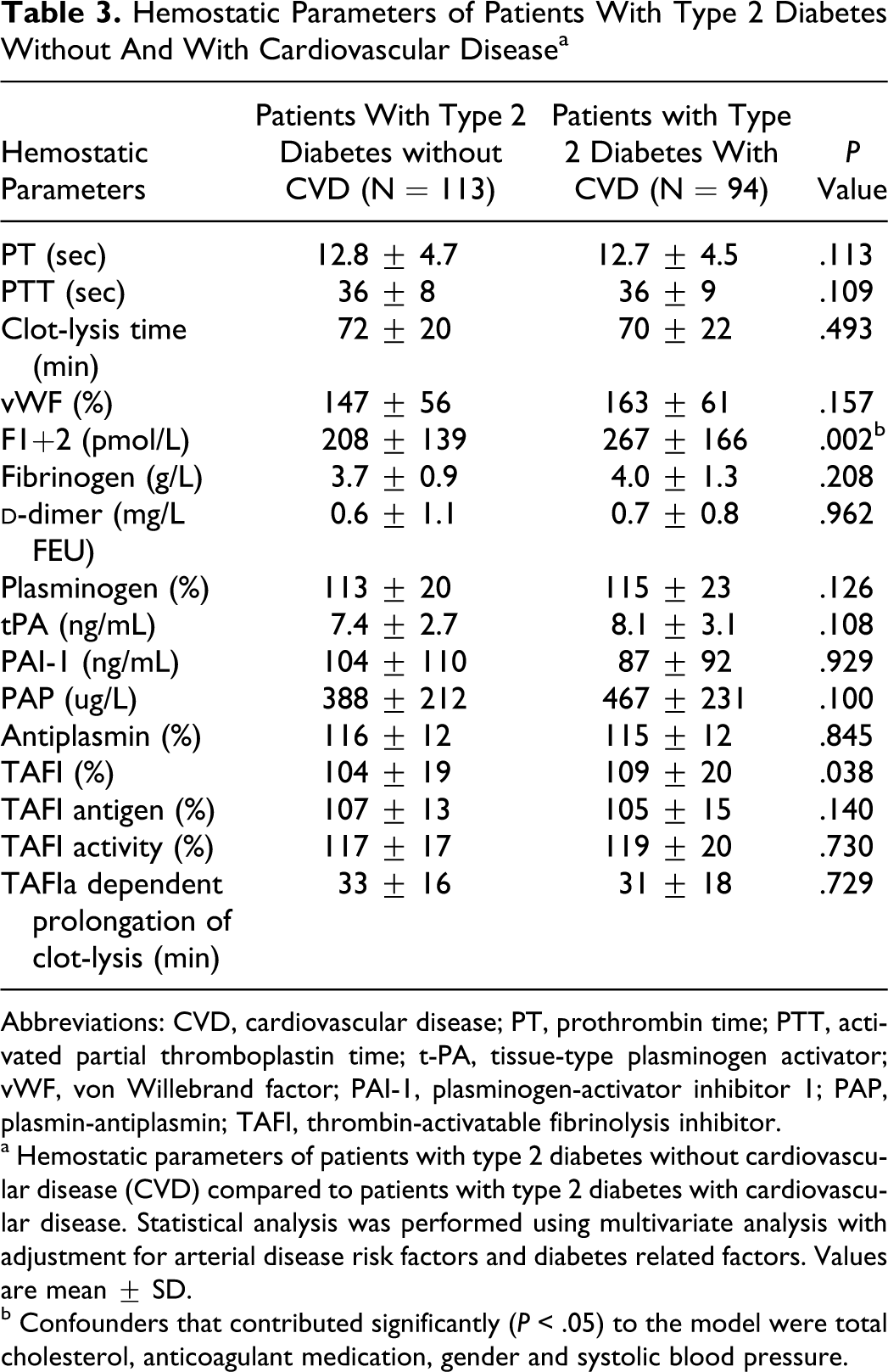
Abbreviations: CVD, cardiovascular disease; PT, prothrombin time; PTT, activated partial thromboplastin time; t-PA, tissue-type plasminogen activator; vWF, von Willebrand factor; PAI-1, plasminogen-activator inhibitor 1; PAP, plasmin-antiplasmin; TAFI, thrombin-activatable fibrinolysis inhibitor.
a Hemostatic parameters of patients with type 2 diabetes without cardiovascular disease (CVD) compared to patients with type 2 diabetes with cardiovascular disease. Statistical analysis was performed using multivariate analysis with adjustment for arterial disease risk factors and diabetes related factors. Values are mean ± SD.
b Confounders that contributed significantly (P < .05) to the model were total cholesterol, anticoagulant medication, gender and systolic blood pressure.
Hemostatic Parameters in Patients With Peripheral Vascular Disease, Ischemic Cerebrovascular Disease, or Coronary Artery Disease
A secondary analysis was performed to elucidate the association of hemostatic parameters with 3 major types of CVDs in patients with type 2 diabetes. Patients with CVD were divided into coronary artery disease, ischemic cerebrovascular disease, or peripheral vascular disease and were compared to the patients with type 2 diabetes without cardiovascular complications (Table 4). Elevated levels of vWF and plasminogen were observed in patients with coronary artery disease compared to patients without CVD. Levels of prothrombin fragment 1 + 2 were significantly increased in patients with peripheral vascular disease, while a trend toward increased levels of prothrombin fragment 1 + 2 was observed in patients with coronary artery disease and ischemic cerebrovascular disease compared to the patients without cardiovascular complications. Moreover, levels of fibrinogen were elevated in patients with ischemic cerebrovascular disease and a trend toward increased levels of fibrinogen was found in patients with peripheral vascular disease. A trend toward elevated levels of t-PA was observed in patients with coronary artery disease as well as peripheral vascular disease compared to patients without CVD. All other measured parameters were not different between groups. These data imply that in patients with type 2 diabetes, levels of vWF and plasminogen are associated with coronary artery disease, levels of prothrombin fragment 1 + 2 are associated with peripheral vascular disease, and levels of fibrinogen are associated with ischemic cerebrovascular disease.
Hemostatic Parameters of Patients With a Certain Type of Cardiovascular Disease a
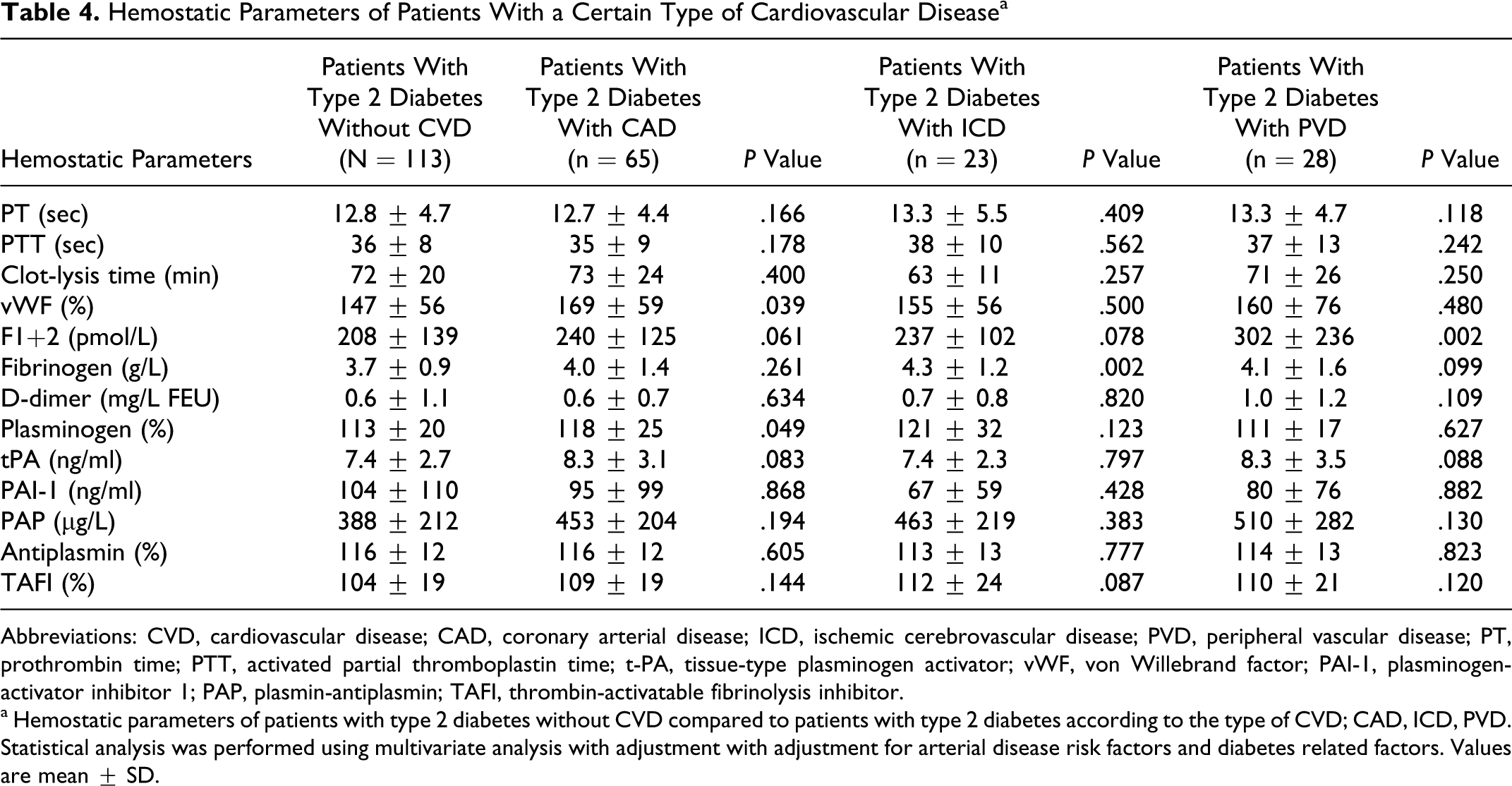
Abbreviations: CVD, cardiovascular disease; CAD, coronary arterial disease; ICD, ischemic cerebrovascular disease; PVD, peripheral vascular disease; PT, prothrombin time; PTT, activated partial thromboplastin time; t-PA, tissue-type plasminogen activator; vWF, von Willebrand factor; PAI-1, plasminogen-activator inhibitor 1; PAP, plasmin-antiplasmin; TAFI, thrombin-activatable fibrinolysis inhibitor.
a Hemostatic parameters of patients with type 2 diabetes without CVD compared to patients with type 2 diabetes according to the type of CVD; CAD, ICD, PVD. Statistical analysis was performed using multivariate analysis with adjustment with adjustment for arterial disease risk factors and diabetes related factors. Values are mean ± SD.
Discussion
In this relatively well-regulated population of patients with type 2 diabetes, we observed a disturbed hemostatic balance that was illustrated by hypofibrinolysis and a procoagulant condition. Although we cannot prove a causal relationship with this case-control design, it is likely that this imbalance may play an essential role in the development of CVD in patients with type 2 diabetes.
Previous studies showed a procoagulant condition in patients with type 2 diabetes demonstrated by increased levels of several coagulation markers, 14 including elevated levels of vWF. Studies focused on the fibrinolytic system showed mostly a hypofibrinolytic condition that was visualized by increased levels of PAI-1. Since procoagulant and hypofibrinolytic conditions may enhance the risk for venous as well as arterial thrombosis, it was suggested that this hemostatic imbalance may contribute to the development of CVD in patients with type 2 diabetes. This study extends previous observations by establishing the association of hemostatic markers with CVD in patients with type 2 diabetes.
In line with other studies, we observed elevated levels of PAI-1 and prolonged clot-lysis times in patients with type 2 diabetes; however, no differences in levels of these markers were observed between patients without and with a proven CVD. This suggests that hypofibrinolysis is present in patients with type 2 diabetes but does not discriminate between those with or without CVD. An explanation might be that patients with type 2 diabetes without cardiovascular complications often have subclinical atherosclerotic disease. It is possible that this subclinical atherosclerosis may cause a similar disturbed hemostatic balance. In addition, platelet reactivity may have contributed to CVD in patients with type 2 diabetes; however we have not measured any platelet markers in this study.
The levels of prothrombin fragment 1 + 2, the marker for thrombin generation, associated with the presence of CVD, suggesting a more procoagulant condition in patients with type 2 diabetes with CVD compared to the patients without cardiovascular complications. Levels of TAFI were also associated with the presence of CVD. Since the biological relevance of this difference was suspicious, other TAFI markers were measured and these markers did not associate with CVD in patients with type 2 diabetes. This implies that the previous observation for TAFI was a coincidental finding. Therefore, we suggest that both the coagulation and fibrinolytic systems are involved in the hemostatic imbalance in patients with type 2 diabetes; however, the coagulation system may tip the hemostatic system into a more thrombotic condition in patients with type 2 diabetes on top of a background of hypofibrinolysis. This hemostatic imbalance together with the presence of other risk factors for CVD may result in the development of CVD.
Furthermore, we observed associations of the hemostatic markers with 3 subgroups of patients with coronary artery disease, peripheral vascular disease, and ischemic cerebrovascular disease. However, since these analyses were secondary with limited statistical power, the results should be interpreted with caution and we regard these secondary analyses as exploratory data.
Additional comments related to the included patients have to be mentioned. All patients were recruited at the outpatient clinic of a hospital. In the Netherlands, the majority of patients with beginning or uncomplicated diabetes is treated by the general practitioner. Patients with complications, intensive insulin regimens, or comorbidity are referred to an internist, often at a hospital-based outpatient clinic. Since there were no exclusion criteria and all patients were enrolled regardless of the severity of their complications, medication, or comorbidity, this study reflects a “real life” population. The patients in this study were relatively well regulated, had a quite long duration of diabetes, and most patients showed adequately regulated blood pressure and lipid profiles. As a consequence, our results cannot be extrapolated to individuals or populations with more recent onset of diabetes or with a poorer regulation.
In conclusion, we observed in patients with type 2 diabetes a disturbed hemostatic balance illustrated by hypofibrinolysis and increased levels of vWF and PAI-1. This imbalance might contribute to the development of CVD in patients with type 2 diabetes. Levels of prothrombin fragment 1 + 2 were associated with the presence of proven CVD in patients with type 2 diabetes.
Footnotes
Acknowledgment
We thank B A Hutten for statistical assistance and personnel of the Department of Experimental Vascular Medicine of the Academic Medical Center, University of Amsterdam, for technical assistance.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Grant from the Dutch Diabetes Research Foundation (Grant 2005.00.016 to JCMM and PFM).