
Abstract
This study proposed an information-response model, which hypothesized that information acquisition determines individuals’ preventive behaviors during the pandemic through cognitive, affective, and instrumental processes. Through a two-wave survey (N = 1,501) conducted in Hong Kong, results revealed that information acquisition was associated with perceived risk, perceived efficacy, affective response, and preventive behaviors. Moreover, source trust was positively related to information utility, which mediated the effect of information acquisition on perceived efficacy and affective response. Our research model contributes to theories of information behavior by highlighting the role of instrumental factors necessary for individuals to translate information into preventive actions.
Keywords
The COVID-19 pandemic has posed severe challenges for citizens worldwide. Existing literature on the pandemic increasingly cites public access to accurate and reliable information as a key coping strategy for citizens seeking to fill an information void, mitigate risk, and inform preventive actions (Alamsyah & Zhu, 2022). During this crisis, the health authorities have been the main source of information in most countries (Calderón et al., 2021; Liu et al., 2023). Timely, comprehensive, and accurate information has been crucial for establishing trust and satisfying citizens’ information needs during the pandemic (Beshi & Kaur, 2020; Mansoor, 2021).
A growing body of research has examined the impact of health information seeking on various health-related outcomes, including but not limited to cancer screening intention (Chae & Lee, 2019), healthy lifestyles (Zhang & Jiang, 2021), and increased health knowledge and literacy (Jin et al., 2019). In addition, recent literature has linked risk information seeking to preventive behaviors (mask-wearing, vaccination intention, etc.) during the pandemic (Li & Zheng, 2022; Zheng et al., 2022). Still, the mechanisms underlying the pathway from information acquisition to decision-making remain understudied. Furthermore, only a few longitudinal studies have explored the direction between information acquisition and follow-on responses. Among these studies, Chae and Lee (2019) specifically probed the role of cognitive and affective responses in mediating the impact of cancer information exposure on cancer screening intention through a two-wave panel survey. However, instrumental factors such as information utility and source characteristics, which might be more influential in explaining behavioral outcomes (Wang et al., 2021), were neglected. Moreover, it is important to acknowledge that studying the relationship between information acquisition during a pandemic context may differ from that in the context of cancer screening, as such a global health crisis involves nearly every citizen. Therefore, in light of this urgent and unique context, a well-defined theoretical framework outlining the pathways from information acquisition to health outcomes could offer valuable insights into how the public responds to this global crisis.
The purpose of this study is to theoretically propose and empirically validate an information-response model. More specifically, we aim to understand how health information influences individuals’ behavioral changes through cognitive, affective, and instrumental factors. In a turbulent pandemic context, we investigate how COVID-19 information acquired from governmental sources affects individuals’ psychological status and subsequent behavioral changes. We tested our theoretical framework using a two-wave longitudinal survey conducted in Hong Kong. Methodologically, the use of a longitudinal panel design addresses the call for clearer causality between information acquisition and follow-on responses. This study thus sheds light on the processes through which pandemic information influences the public’s adoption of preventive behaviors.
Literature Review
Theoretical Framework: An Information-Response Model
Various theoretical frameworks have been proposed and tested to explain why and how individuals seek and obtain information during the pandemic (Wang et al., 2021). These frameworks mainly conceptualize information seeking/acquisition as a dependent variable, and identify different predictor types (e.g., cognitive, affective, and social) of information acquisition. The tendency to focus on predictors may be due to the prevalent conceptualization of information acquisition as a process of knowledge accumulation that gradually triggers behavioral changes (Rimal & Real, 2003). This body of research provides a conceptual understanding of how and why individuals acquire information. Even so, these frameworks and relevant empirical studies have not explicitly answered the question of how people use information to make health-related decisions (Lewis et al., 2022).
Some studies have explored health information seeking as a predictor of health outcomes. For example, Morton and Duck (2001) found that media exposure to skin cancer has an impact on risk judgments. Similarly, through a national survey in China, Zhang and Jiang (2021) showed that health information seeking from different media outlets increases patient-centered communication, which further triggers healthy lifestyles. Furthermore, only a few studies have examined the pathway from information acquisition to health outcomes using longitudinal data (e.g., Chae & Lee, 2019; Lewis et al., 2022; Yang & Cao, 2022). In particular, drawing upon the literature on media effect (e.g., Clarke & Everest, 2006; Morton and Duck, 2001) and the integrative model of behavior prediction (Fishbein, 2000), Chae and Lee (2019) proposed a research model linking cancer-information exposure to cancer screening intention. Results from a two-wave panel survey confirmed that exposure to cancer information is positively associated with cancer fear, cancer worry, and risk perception at Wave 1, which consequently affects screening intention measured at Wave 2. This model explicates the pivotal role of cognitive and affective responses in mediating the impact of information exposure on health-related behaviors. However, after information exposure, instrumental factors such as information utility and source trust that may play a role in determining health-related outcomes were neglected in the model development process (Wang et al., 2021).
To this end, we propose a theoretical framework of information responses to systematically examine pathways from information acquisition to preventive behaviors. We explain preventive behaviors as a direct and mentally mediated response to acquisition of information during the COVID-19 pandemic through the lens of stimulus-organism-response (SOR) theory. Developed by Mehrabian and Russell (1974), SOR theory conceptualizes individuals’ behaviors as occurring in an environment consisting of various “stimuli.” These stimuli can influence cognitive and affective states, referred to as “organisms.” Finally, these organisms lead to behavioral responses. In addition to the direct link between stimuli and response, the SOR framework underscores the mediating role of organisms in this process.
In the context of the COVID-19 pandemic, several studies have adopted the SOR framework to understand behavioral changes in environments characterized by the rapid pace at which COVID-19-related information is shared with the public. Such an environment may consist of information stimuli that trigger people’s psychological and behavioral responses (Song et al., 2021). For example, Zheng et al. (2022) found that seeking vaccine information on the internet (S) was associated with perceived information overload, negative emotions, and risk perception (O), which further reduced COVID-19 vaccination intention (R). Similarly, taking the SOR framework as a theoretical base, Soroya et al. (2021) revealed that searching for COVID-19 information via various sources (S) triggered information overload and anxiety (O), leading to information avoidance (R).
Applying these insights to our inquiry, we suggest that information acquired from governmental sources could be an informational stimulus that triggers different types of cognitive, affective, and instrumental processes. Suggested by the Comprehensive Model of Information Seeking (CMIS, Johnson & Meischke, 1993) and the model proposed by Chae and Lee (2019), we include individuals’ perceived risk, perceived efficacy, affective response, source trust, and information utility as organisms. Finally, we supposed, these organisms determine COVID-19-preventive behaviors. Our theoretical model is illustrated in Figure 1. The following sections elaborate the relevant theories that informed the relationships we posit between these variables.
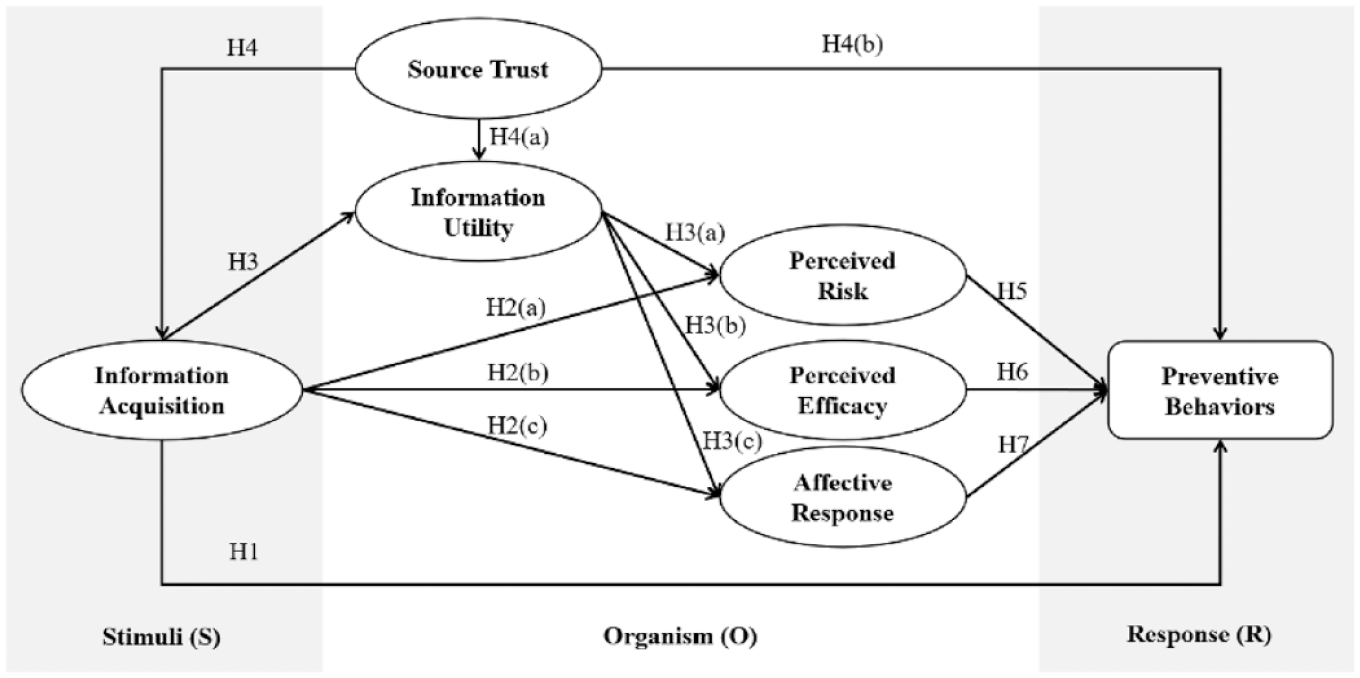
Theoretical Framework: The Information-Response Model.
From Information Acquisition to Preventive Behaviors
Information acquisition, referring to the information gathered or received from different sources (Berger, 2002), plays an important role in shaping health outcomes. People may receive information either in an active way (e.g., purposeful information seeking) or in a passive way (e.g., information scanning). Previous research on information acquisition (including exposure, seeking, and scanning) 1 examined its role in predicting different health outcomes, such as adoption of e-Government applications for risk communication (Park & Lee, 2018), healthier lifestyles (exercising, diet, and smoking, Lewis et al., 2022; Rimal et al., 1999), reduced vaping habits (Yang et al., 2019), increased health knowledge and literacy (Jin et al., 2019; Qian et al., 2023), cancer preventive behaviors (Chae & Lee, 2019; Hornik et al., 2013), and preventive behaviors during the COVID-19 pandemic (Yang & Cao, 2022; Zheng et al., 2022; Zhou & Roberto, 2022). For example, using a two-wave data of 158 students in United States, Zhou and Roberto (2022) found that COVID-19 vaccination intention was determined by vaccine-related information seeking. Similarly, Yang and Cao (2022) examined the effect of online health information seeking on protective behaviors during the pandemic using a two-wave longitudinal survey of 557 U.S. adults. They found that online information seeking at Wave 1 had a significant and direct effect on protective behaviors at Wave 2. Thus, we hypothesize the following:
Hypothesis 1: Information acquisition will be positively associated with preventive behaviors.
Information Acquisition as an Environmental Stimulus
Borrowing from the SOR model, we conceptualized information acquisition as a “stimulus” capable of influencing individuals’ cognitive and affective states, which are referred to as “organisms.” The effects of cognitive perceptions and affective response toward risk on information acquisition have been extensively theorized (e.g., Kahlor, 2010). Yet exposure to risk information can also work in the opposite direction and change psychological predispositions. Wilson’s model of information behavior (Wilson, 1997) recognized information management as an iterative process consisting of seeking, processing, activating mechanisms (risk perceptions and self-efficacy), and continued seeking.
According to McGuire’s Communication-Persuasion Matrix, obtaining and processing new information is an essential part of individuals’ belief or attitude changes (McGuire, 1989). Specifically, information about COVID-19 could be positively associated with an individuals’ reported levels of risk perception and efficacy, depending on the type of information that they acquire (Nazione et al., 2021). With the ongoing progression of the pandemic, government authorities keep conveying timely, accurate, and consistent information to the public (Turner et al., 2013). They may emphasize the risk of the coronavirus, like its severity and susceptibility, along with providing some effective and easy preventive measures. On one hand, some messages containing health-threatening information (e.g., infected cases per day) may increase risk perception and affective response. On the other hand, some messages mentioning useful prevention measure against the virus (e.g., washing hands and wearing masks) could help the citizens build self-efficacy, nurturing more confidence to combat the pandemic. Therefore, the effects of the information acquired from the government authorities could be intricate and dynamic. Previous studies have indicated that effective and timely communication from the government authorities during the COVID-19 pandemic can influence how citizens perceive risks and accordingly develop self-efficacy associated with the crisis (Flores & Asuncion, 2020; Nazione et al., 2021). Notably, information acquisition is related to affective response (Griffin et al., 1999). For example, exposure to COVID-19 information is likely to arouse negative emotions, such as anger, anxiety, and sadness (Buchanan et al., 2021). Thus, we hypothesize that the following:
Hypothesis 2: Information acquisition will be positively associated with (a) perceived risk, (b) perceived efficacy, and (c) affective response.
The Role of Information Utility and Source Trust
Previous studies focused on the relationship between information exposure and cognitive, affective, and behavioral changes (Johnson & Case, 2012; Kahlor, 2010; Nazione et al., 2021; So et al., 2019; Witzling et al., 2015). As a result, little scholarly attention has been paid to the role of instrumental factors such as opinions about information and source and how those factors impact the health decision-making process after information exposure.
Within the CMIS (Johnson & Meischke, 1993), instrumental factors, including utility of information and character of the information carrier, have been conceptualized as primary factors related to information-seeking behaviors. Utility refers to the relevance, topicality, and ultimate usefulness of the information contained in the medium; character, refers to an individual’s perceived credibility and trustworthiness of information source and channel (Johnson & Meischke, 1993). Instrumental factors are key to determining how individuals process and respond to information (Johnson & Meischke, 1993). Even so, much previous research has formulated pathways from information acquisition to actions without explicitly articulating the role of instrumental factors (Tan et al., 2015).
Reported levels of trust in information source (as one dimension of information carrier character) are related to evaluations of the quality of information (e.g., Johnson & Meischke, 1993; T. D.Lee et al., 2019; Mun et al., 2013), and can influence subsequent information responses (Hou & Shim, 2010). Originally, Johnson and Meischke (1993) proposed that the characteristics of the information carrier, referring to an individual’s perception of its credibility and trustworthiness, affect the perceived utility of information from that source and any subsequent information-seeking behavior. Empirical evidence has also suggested that source trust—as the primary component of source perception—is the key determinant of information acquisition, perceived information utility, and any consequent preventive behaviors (Goodwin et al., 2022; E. W. Lee et al., 2023; Trent et al., 2021; Yang & Liu, 2021). For example, by analyzing survey data from 700 Korean citizens, E. W.Lee et al. (2023) found that trust in government is positively related to perceived information quality. Trent et al. (2021) also demonstrated that trust in government is a major determinant of vaccine uptake in large cities. Thus, we hypothesize that the following:
Hypothesis 3: Source trust will be positively associated with (a) information acquisition, (b) information utility, and (c) preventive behaviors.
While CMIS suggests information utility is an important driver of information seeking, the relationship between the two could be reversed. In this study, we propose that information acquisition from official sources is positively related to individuals’ perceived information utility. More specifically, during COVID-19, people process the utility of pandemic-related information provided by government authorities on the basis of their past information seeking experience. Evidence suggests that compared to COVID-19 information from alternative sources, the information obtained from official sources is more reliable, informative, and useful (Rufai & Bunce, 2020). Hence, individuals may turn to the official sources first to fulfill their own knowledge of the pandemic. When the results of information acquisition provide positive health outcomes (e.g., useful for preventing the virus), citizens are likely to judge that information as having high utility. Therefore, evaluation of information utility may occur after individuals obtain relevant information from government sources in our study context.
Moreover, prior studies have also empirically tested the direct relationship between information utility and individuals’ cognitive and affective responses (Dutta et al., 2010). For instance, using the survey data from 705 respondents in Indonesia, Alamsyah and Zhu (2022) found that higher quality of government information during the pandemic led to higher response efficacy and fewer reported negative emotions. Quality content has also been proposed as a significant determinant of individuals’ self-efficacy (Cassia & Magno, 2021). Taken together, information acquisition from official sources during the pandemic is positively related to information utility, which further triggers individuals’ cognitive and emotional responses. Accordingly, we propose the following:
Hypothesis 4: Information utility will mediate the effect of information acquisition on (a) perceived risk, (b) perceived efficacy, and (c) affective response.
Preventive Behaviors as Responses
In related research, self-protective behavior during crisis is commonly found to be an outcome of perceived risk and perceived efficacy (Witte, 1992). Perceived risk refers to the extent to which one believes they are vulnerable to a disease. Perceived efficacy refers to an individual’s belief about their ability to perform the recommended responses. According to the risk perception attitude (RPA) framework (Rimal & Real, 2003), perceived threat and efficacy play a significant role in explaining individuals’ likelihood of adopting preventive actions. The RPA framework emphasizes the interaction effect between perceived risk and efficacy on health-related outcomes. Health outcomes, including health information seeking, knowledge acquisition, self-protective motivation, and protective behavioral intention, depend on the joint effect of perceived risk and efficacy (Rimal, 2001; Rimal & Real, 2003). RPA drew from the extended parallel process model; consequently, RPA also theorized the effects of perceived risk and efficacy on behavioral outcomes (Shi et al., 2023; So et al., 2019; Witte, 1992). Although the effects of perceived risk and efficacy on behavioral outcomes are well established in the literature, these relationships are essential to our proposed model. Thus, we propose the following hypotheses in the context of the COVID-19 pandemic:
Hypothesis 5: Perceived risk will be positively associated with preventive behaviors.
Hypothesis 6: Perceived efficacy will be positively associated with preventive behaviors.
Theories of risk perception often emphasize cognitive appraisals of risk (e.g., perceived risk and efficacy beliefs) and ignore emotional processes that may affect decision-making (Freimuth & Hovick, 2012; Leppin & Aro, 2009). Recently, communication scholars have begun to shift their attention from cognitive risk responses to affective response as a primary driver of preventive behaviors. For instance, Loewenstein and colleagues (2001) proposed the risk-as-feelings hypothesis, which argues that two interrelated reactions to risk—cognitive and affective responses—function differently in guiding health decisions. In the context of COVID-19, affective response describes the negative emotions (such as fear, anxiety, worry, and sadness) aroused by risk. Affective response may encourage more preventive behaviors by leading to more risk-information exposure (Ford et al., 2023; Li & Zheng, 2022). In line with the risk-as-feeling hypothesis, we hypothesize that the following:
Hypothesis 7: Affective response will be positively related to preventive behaviors.
Method
Participants and Procedures
The survey focused on prevention behaviors during the COVID-19 pandemic. Participants were restricted to those aged 18 years and above. Respondents were recruited by an online survey agency (Rakuten Insight) in Hong Kong. Ethics review approval was obtained from the Human Subjects Ethics Sub-Committee of the Research Committee at the hosting university. All methods were performed in accordance with relevant guidelines and regulations. Two survey waves were conducted with a 14-month interval by an online survey agency in Hong Kong. For the first wave (September and October 2020), data were collected through quota sampling drawn from the 2016 population census data of Hong Kong, based on the distribution of gender, age, and residential area. The Wave 1 survey received 3,190 responses (response rate: 58.8%). The second wave was conducted in November 2021. All participants in Wave 1 were invited to participate in Wave 2, and 68.75% participated again (n = 2,193). Informed consent was obtained before participants began each survey.
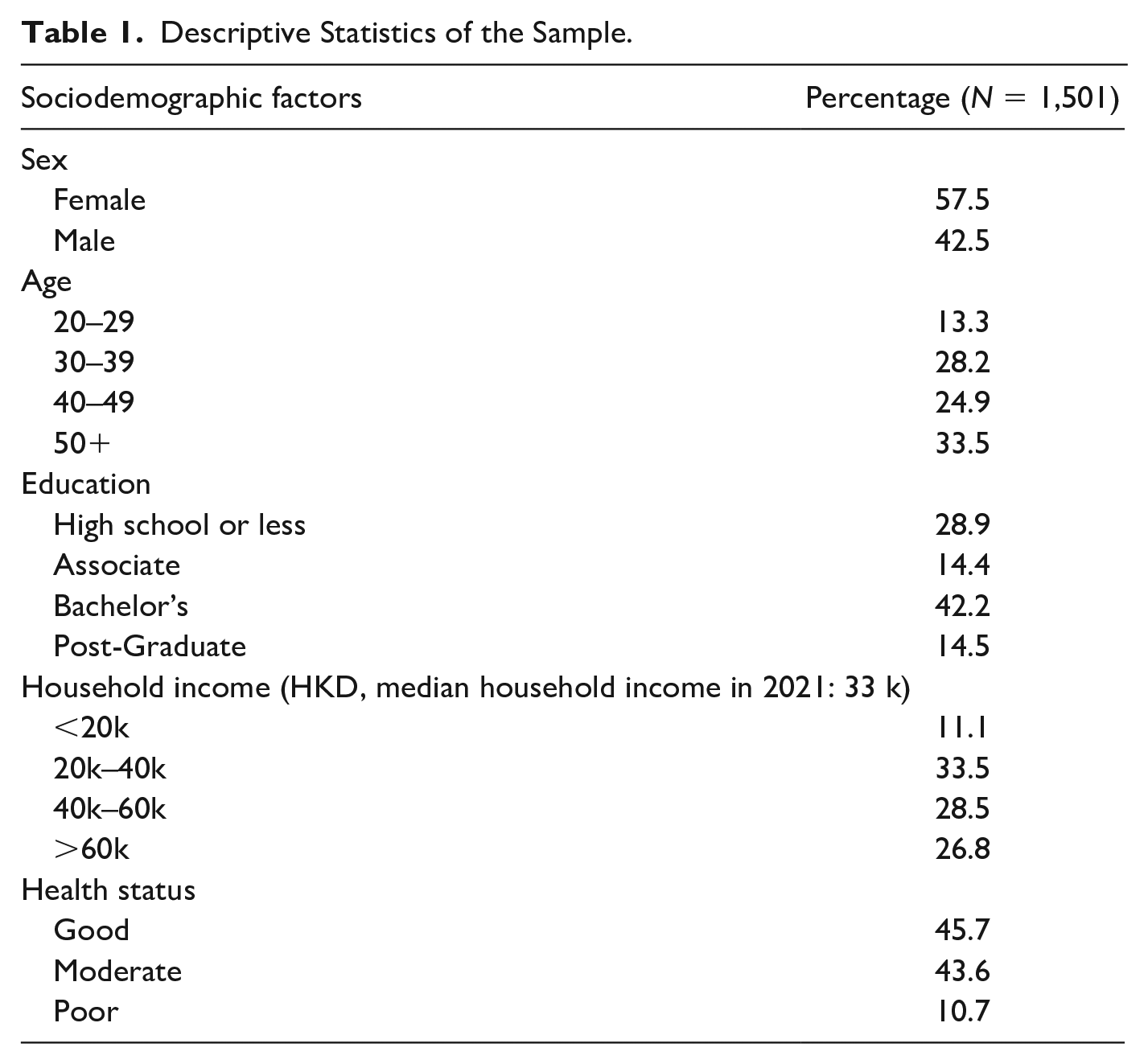
Data cleaning in both waves was conducted prior to analysis. Respondents who failed the attention check question and who finished the entire questionnaire in less than 5 minutes were eliminated (median = 13 minutes). Moreover, we measured respondent demographics in both waves. Those who failed to provide a consistent answer for gender, age, and education level in the two surveys were also removed. Eventually, we analyzed a final complete sample of 1,501 respondents. Although we used quota sampling to collect our first wave data, our sample frame changed because of participant attrition in the second wave. Table 1 shows the descriptive statistics of the sociodemographic features of the studied sample. Compared to the census data, our two-wave sample has more female (χ2 = 14.08, p < .05), middle-aged (χ2 = 235.33, p < .05), higher income (χ2 = 694.96, p < .05), and more highly educated participants (χ2 = 1,384.26, p < .05). Age, gender, income, and education were thus used as control variables in following data analysis.
Descriptive Statistics of the Sample.
A Chinese version of the survey was developed based on previous literature. Translations were performed using standard translation-back-translation procedures (Brislin, 1970). A pilot test with 15 participants was then conducted to test the feasibility of the questionnaire and the survey procedure, such as length of the survey, layout design, readability of the items, and item reliability. Participants were asked to test and comment on the pilot study. Item reliability was acceptable, and participants were satisfied with the survey design.
Measurement
Information Acquisition
Items were adapted from Clayman et al. (2010) and Zhao et al. (2022). Participants indicated the frequency on average per day, in the past 6 months, they had received information about COVID-19 from four government sources (1 = never to 7 = always): HK government, Health Bureau, and Center for Health Protection. Individuals respond differently to information from different sources depending on source credibility, information quality, and behavior intentions ( Y.Hu & Shyam Sundar, 2010). Previous research showed that, during the pandemic, individuals primarily acquired information from official government sources (Tang & Zou, 2021). Thus, to simplify, we focused on information from government sources (Wave 1: M = 4.57, SD = 1.22, α = .87; Wave 2: M = 4.30, SD = 1.26, α = .93).
Information Utility
Based on Johnson and Meischke (1993), utility was measured by four items from the information quality scale (Lee et al., 2002). Participants were asked to what extent they agree that (1 = strongly disagree to 7 = strongly agree) the information about COVID-19 from the government sources was accurate, transparent, up-to-date, and useful (Wave 1: M = 4.37, SD = 1.24, α = .95; Wave 2: M = 4.21, SD = 1.35, α = .96).
Source Trust
Following Johnson and Meischke (1993), respondents were asked to what extent they agreed that the government and health authorities (1 = strongly disagree to 7 = strongly agree) were capable, efficient, confident, and knowledgeable (Wave 1: M = 4.18, SD = 1.35, α = .95; Wave 2: M = 4.17, SD = 1.41, α = .97).
Affective Response
For affective response, respondents were asked to rate their feelings about COVID-19 on a 1 to 7 scale (1 = strongly disagree to 7 = strongly agree): (1) fearful, (2) sad, and (3) worried (Wave 1: M = 4.43, SD = 1.21, α = .88; Wave 2: M = 4.38, SD = 1.21, α = .88) (Ferrer et al., 2016).
Perceived Risk
Perceived risk was measured by four items adopted from previous literature (Ferrer et al., 2016), including “the coronavirus is almost ubiquitous, and the pathogenesis is high,” “there is a high probability of getting infected,” “the COVID-19 mortality rate is high,” and “I have no confidence I can avoid the negative impacts of COVID-19” (Wave 1: M = 4.41, SD = 1.00, α = .80; Wave 2: M = 4.31, SD = 1.05, α = .83).
Perceived Efficacy
Participants were asked to what extent they believe that they can take the following measures to prevent COVID-19: wearing a face mask, sanitizing or washing hands regularly, keeping socially distant, staying at home, and testing for COVID-19 (Wave 2: M = 5.82, SD = 0.91, α = .82).
Preventive Behavior
Following previous studies (e.g., Yang & Cao, 2022), we operationalized COVID-19 preventive behavior as individuals’ level of engagement, ranging on a scale from 1 (=never) to 7 (=always), in the following: wearing masks, staying at home, keeping socially distant, sanitizing or washing hands, and recommending vaccines. Items were averaged to represent overall frequency of preventive behavior (Wave 1: M = 5.12, SD = 0.65; Wave 2: M = 5.10, SD = 0.65).
Control Variables
Demographic variables including age, gender, household income, and education level were included as control variables. Health status may also be associated with information acquisition, psychological response, and preventive behavior (Wang et al., 2021). We therefore adopted health status as an additional control variable.
Analysis
Structural equation models were conducted using the lavaan package in R to test our proposed theoretical model. Our model includes cross-lagged paths between variables measured at two waves. Specifically, for information acquisition, source trust, and information utility, Wave 1 data were used. Perceived risk, affective response, perceived efficacy, and COVID-19 preventive behaviors were measured in the second wave as follow-on behaviors. We also controlled the effect of preventive behaviors measured at Wave 1 in analysis.
First of all, confirmatory factor analysis (CFA) was conducted to test the measurement model with all latent variables. A preliminary analysis on the multivariate normality of the data set was then conducted, with perceived efficacy and source trust nonnormally distributed. To proceed with multivariate nonnormal data, we used the maximum likelihood estimation with robust standard errors (Byrne, 2013). The model fit indices of the CFA, χ2(236) = 1,539.19, p < .001, comparative fit index (CFI) = .96, Tucker-Lewis index (TLI) = .95, root mean square error of approximation (RMSEA) = .06, standardized root mean square residual (SRMR) = .05, all met the suggested criteria ( L. T.Hu & Bentler, 1999). Reliability, convergent validity, and discriminant validity tests were then conducted for the measurement model. Indicator reliability was assessed by examining whether factor loadings on the latent variable were above the threshold of .50 (Appendix A). Construct reliability was assessed using Cronbach’s alpha (CA) values, which established that their values were all above the threshold of .70. Convergent validity was established by examining if the AVE values were above 0.50. The AVE square root of each construct was greater than its highest correlation with other constructs, which supported discriminant validity (Table 2). These results suggested that the measurement model is reliable and valid.
The Correlation Matrix.
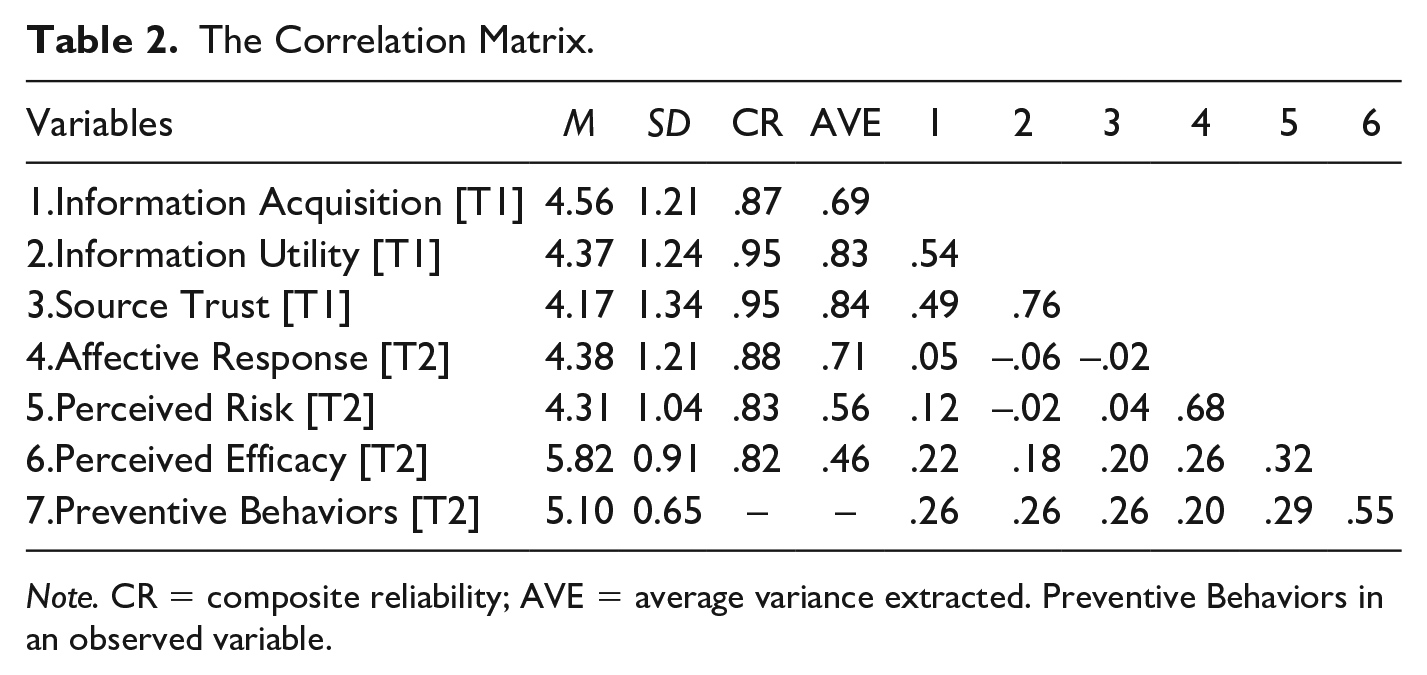
Note. CR = composite reliability; AVE = average variance extracted. Preventive Behaviors in an observed variable.
Next, structural equation modeling demonstrated that the information-response model (controlling for age, gender, income, education, and health status) yielded a good fit: χ2(377) = 2,506.85 p < .001, CFI = .93, TLI = .92, RMSEA = .06, SRMR = .08. This established an acceptable fit between the model and the data.
Results
As can be seen from Figure 2, the direct effect of individuals’ information acquisition from governmental sources at Wave 1 on preventive behaviors at Wave 2 was nonsignificant (β = .01, p = .69), thus rejecting H1. Individuals’ information acquisition at Wave 1 was associated with perceived risk (β = .13, p < .001), perceived efficacy (β = .12, p < .001), and affective response (β = .11, p < .01) at Wave 2, which supported H2(a–c).
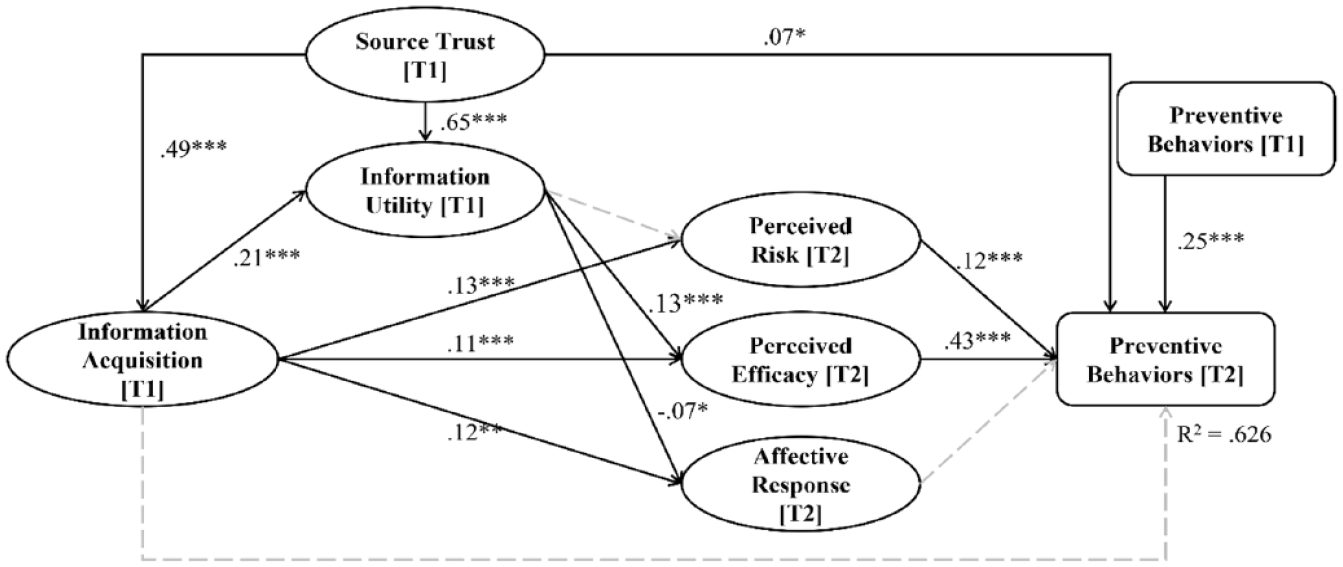
Structural Equation Modeling Results With Standardized Estimates.
In terms of the role of instrumental factors, source trust at Wave 1 was positively associated with information acquisition at Wave 1 (β = .48, p < .001), information utility at Wave 1 (β = .65 p < .001), and preventive behaviors at Wave 2 (β = .07, p < .01), which supported H3(a–c). In terms of H4, information acquisition at Wave 1 was positively associated with information utility (β = .21, p < .001). Information utility at Wave 1 was associated with perceived efficacy (β = .13, p < .01) and affective response at Wave 2 (β = −.10, p < .01). However, its effect on perceived risk was nonsignificant (β = −.03, p = .49). Bootstrapping (n = 5,000) was conducted to examine the mediating role of information utility (H4) in our proposed model. Results demonstrated that information utility mediated the effect of information acquisition on affective response (Β = −.02, s.e. = .01, p < .05, 95% CI = [−.04, −.00]) and perceived efficacy (Β = .03, s.e. = .01, p < .01, 95% CI = [.01, .03]), lending support to H4(a–b).
Finally, in terms of the effect from organism to responses, perceived risk (β = .11, p < .01) and perceived efficacy (β = .43, p <.001) at Wave 2 were positively associated with preventive behaviors at Wave 2, lending support to H5 and H6. However, the relationship between affective response at Wave 2 and preventive behaviors at Wave 2 was nonsignificant (β = .03, p = .63). Thus, H7 was not supported. The total effect from information acquisition to preventive behavior is also calculated, bootstrapping results show a significant effect (B = .05, s.e. = .01, p < .001, 95% CI = [.02, .06]).
Discussion
How can information acquisition from government sources help citizens engage in preventive behaviors that combat COVID-19? Our study identifies potential pathways. Guided by the SOR framework, this study proposed an information-response model to explain the mechanisms (i.e., cognitive, affective, and instrumental) underlying the relationship between information acquisition and preventive behaviors. Results from a two-wave online survey provided empirical support for the proposed model. The following section elaborates several major findings of this study.
Summary of Major Findings
First, we found that although information acquisition at Wave 1 was not directly related to preventive behaviors at Wave 2, its indirect effect through instrumental and cognitive organisms is significant. This underlines that the pathway from obtaining information from official sources to preventive behaviors is complex and dynamic. In contrast with Li and Zheng (2022), which found the direct relationship between the two, our study highlights that obtaining COVID-19 information may create different perceptions and emotions before individuals’ various behavioral changes.
Second, information acquisition at Wave 1 was positively associated with risk perception, affective response, and perceived efficacy at Wave 2. This finding shows how information acquisition from government sources during a crisis can trigger a set of either beneficial or detrimental cognitive and affective responses. Governments might release anxiety-inducing information such as the number of cases per day or city lockdown orders. Such information may enhance perceived risk and affective response (Buchanan et al., 2021). However, if the information is tailored to emphasize the ways in which certain measures or statistics help combat the pandemic, perceived efficacy might be enhanced (So et al., 2019). Therefore, information acquisition outcomes during a pandemic may depend on the types of information that government agencies provide (Xin et al., 2022). This line of research warrants further investigation in future studies.
We further found that risk perception and perceived efficacy were positively related to preventive behaviors while the effect of affective response was nonsignificant. This finding suggests that cognitive perceptions play a more crucial role when people are exposed to an uncertain situation. More specifically, those with high levels of risk perception and perceived information efficacy are more likely to adopt some preventive actions. However, people who experience affective response may prefer to take actions other than strictly preventive ones. For example, several recent studies found that affective response (e.g., anxiety and sadness) is positively related to information avoidance in the context of COVID-19 (Song et al., 2021). In our study, we examine affective response as a single-dimensional construct. Previous studies also suggested the separate role of discrete emotions in health communication (Nabi, 1999). Future studies should thus delve into the role-played by different negative emotions.
Third, we highlighted the important role of instrumental factors (i.e., source trust and information utility). Information acquisition was positively related to information utility, which was further related to perceived risk and increased efficacy. This finding is consistent with the CMIS, indicating that when people perceive information obtained from government sources to be useful, valuable, and relevant to their needs, they have a better understanding of the situation. Consequently, their risk perception is lower, and confidence in the information’s ability to help them combat the virus (i.e., efficacy) increases. Therefore, our findings demonstrated that information utility plays an important role in mediating the effect of information acquisition on cognitive perceptions.
In addition, we found that information acquisition from government sources was positively related to source trust, perceived information utility, as well as preventive behaviors. Government is an important source of COVID-19 information, and accordingly, source trust is essential to ensure that accurate and timely information is disseminated to the public (Wong et al., 2022). Low levels of source trust may lead to uncertainty about the information being conveyed, which leads further to hesitancy to comply with official recommendations. Conversely, those with high source trust perceive information utility to be high, report lower perceived risk, and increased perceived efficacy, which eventually lead to preventive behaviors. Therefore, to promote preventive behaviors during the pandemic, it is important to improve perceived trust of information provided by government sources (Mansoor, 2021).
Theoretical and Practical Implications
This study proposed a new model that maps the linkage from information acquisition to psychological and behavioral outcomes. Referring to the SOR model, our proposed information-response model untangled how information acquisition triggers cognitive, affective, and instrumental perceptions, which further determine behavioral outcomes during the pandemic. Results from the two-wave panel survey lend support to the propositions in the theoretical model. Previous behavioral change models emphasized the role of psychological factors, such as attitude, norms, cognitive and affective responses, and self-efficacy (Wang et al., 2021). However, as our study showed, source and information beliefs played a critical role during the process from information acquisition to behavioral change.
Specifically, our model proposed that source trust and information utility are two major factors associated with information acquisition and health outcomes. When seeking information from official sources, individuals will form a belief about those information sources as well as the quality of the information conveyed, which further influence their perceptions and behavioral outcomes. Our model thus elaborates the pathways between information acquisition and positive health outcomes with a particular emphasis on instrumental factors. The rapid spread of information on the internet via an ever-expanding number of official and unofficial sources led to an “infodemic” that coincided with the pandemic (Zheng et al., 2023). This infodemic is characterized by information overload that includes both accurate information and false or misleading information. 2 The overabundance of fake news mixed with facts can cause the public to mistrust health authorities and undermine the public response to crisis. Our model points out the need to emphasize the trustworthiness of information carriers and the quality of information being disseminated.
Integrating the literature on information management with communication during crises, we tested multiple pathways from information acquisition to preventive behavior. Our primary factors—source trust and informational beliefs—have been firmly established in other areas of risk communication research such as information science (e.g., Mun et al., 2013). Our findings thus have broader implications for multiple fields, such as public health, communication, and information science. A more comprehensive model of information responses combining theories and concepts from multiple domains is necessary for understanding the complex phenomenon of how people make sense of information.
Practically, the results of this study provide direct guidance for public policy. COVID-19 is expected to remain a permanent fixture of the public health ecosystem in many societies, and documented pandemic fatigue is growing worldwide. As pandemic fatigue deepens, individuals’ perceived efficacy is likely to remain high, but risk perception will decrease. The critical effect of trust in government information and information utility has informed our understanding of how source and informational characteristics might influence health outcomes. Exposure to low-quality information may increase worry and demotivate self-efficacy, and consequently diminish preventive behaviors. Ensuring timely and accurate information and cultivating trust in citizens may be a particularly effective approach in coping with COVID-19 or future pandemics.
Limitations and Future Research
When generalizing this study’s results, its limitations should be noted. First of all, although quoted to the population distribution at Wave 1, the study sample consists of more female, middle-aged, higher income, and more highly educated adults than the overall population due to attrition at Wave 2. These sociodemographic characteristics may affect perception and consumption patterns toward information (Wang et al., 2022). Therefore, interpretation of findings from this sample may be limited in terms of its generalizability to the overall Hong Kong population or that of other countries. However, our findings could form the basis for replicating the information-response model to other nationally representative samples.
Second, the two-wave data collected during a 14-month period may not be granular enough to capture the dynamics of individuals’ beliefs and psychological states. For example, individuals’ emotional changes toward pandemic can be more immediate than a 14-month lag. In our model, the affective response measured at Wave 2 was not significantly correlated with information acquisition measured at Wave 1. Scholars have suggested that longitudinal survey may fail to detect an effect if the time interval between the study waves does not match the contextual situation (i.e., the height of the COVID-19 pandemic; Slater, 2007). Alternatively, perceptions about information sources and utility may change more slowly compared with emotional responses. Thus, the choice of an optional time interval for longitudinal study is important for the validity of results and should be calibrated to a study’s other particulars.
Third, our model fit did not fully meet the criteria established by L. T.Hu and Bentler (1999). Researchers have proposed that, in practical application, we ought to acknowledge the significance of fit indices; however, they advise against unwavering dependence on predetermined thresholds (Hayduk et al., 2007). Thus, in this study, we focused on testing our proposed model linking information acquisition to health outcomes. Nevertheless, the model fit may be improved by testing alternative models. In the future, a survey design with multiple stages over a longer time frame might fully capture the dynamic and nonlinear changes of affective, cognitive, and behavioral responses to information acquisition.
Despite the above limitations, this study contributes preliminary empirical data to the existing knowledge of how individuals respond to information acquisition from government sources during the pandemic. Much prior research has relied on cross-sectional data with small samples (Wang et al., 2021). In this study, we collected longitudinal data to ensure that information acquisition temporally preceded the dependent variables. Beyond testing how information acquisition is related to psychological and behavioral responses, we also emphasized the role of instrumental beliefs. Our findings might inform future studies that examine the complex process of information consumption during crisis. Future studies should delve into the information consumption process to sort out the interdependent relationships among various information behaviors such as information exposure, processing, use, and additional seeking to validate the multifaceted instrumental beliefs, such as source credibility and information utility, that we treat here. It should also be noted that these instrumental beliefs are dynamic. Individuals may refresh their beliefs during the information consumption process, which may further determine future information-acquisition behaviors. Thus, more longitudinal studies are needed to untangle the recursive relationship between information behaviors and instrumental beliefs.
Footnotes
Appendix A
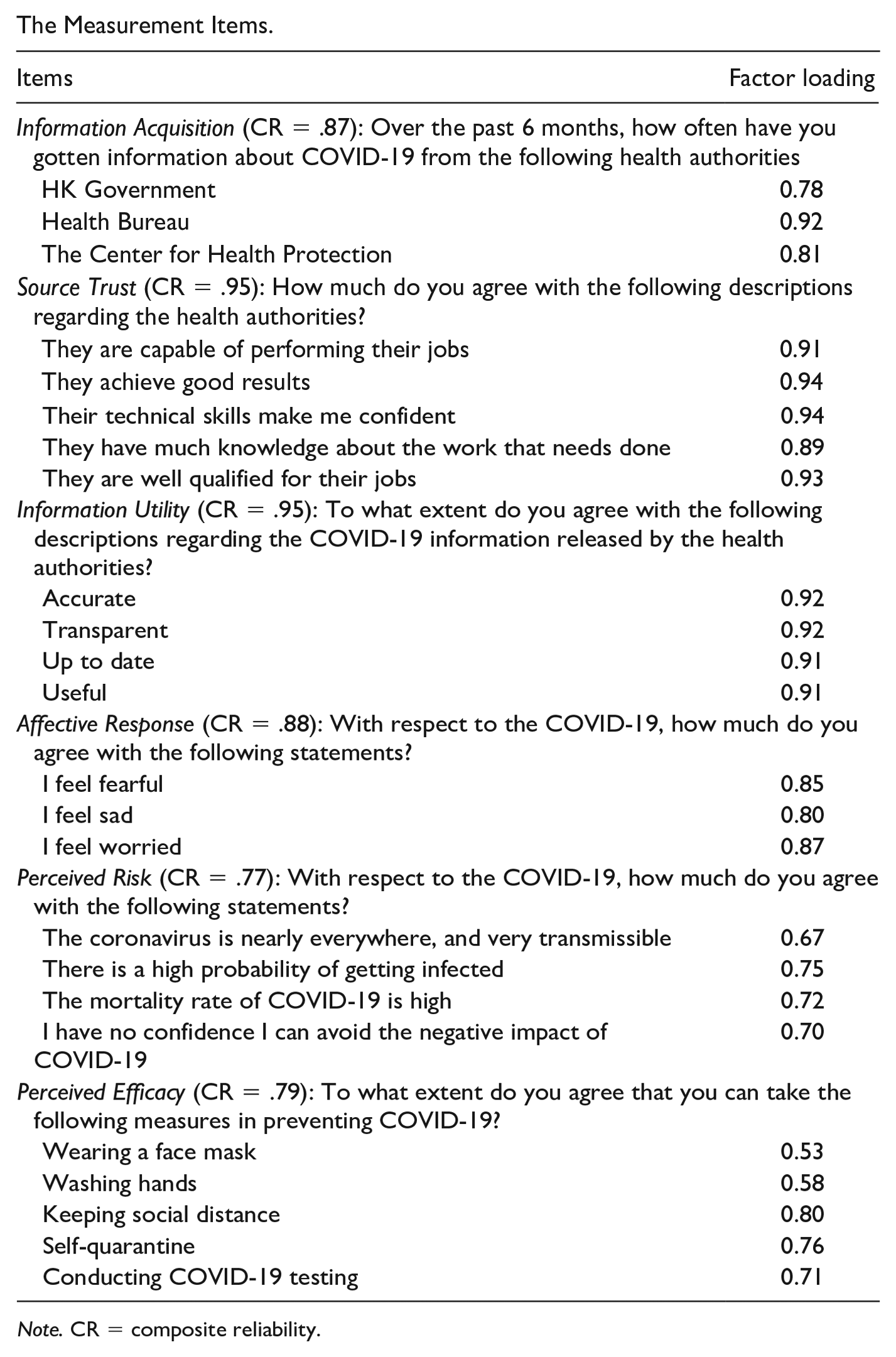
The Measurement Items.
| Items | Factor loading |
|---|---|
| Information Acquisition (CR = .87): Over the past 6 months, how often have you gotten information about COVID-19 from the following health authorities | |
| HK Government | 0.78 |
| Health Bureau | 0.92 |
| The Center for Health Protection | 0.81 |
| Source Trust (CR = .95): How much do you agree with the following descriptions regarding the health authorities? | |
| They are capable of performing their jobs | 0.91 |
| They achieve good results | 0.94 |
| Their technical skills make me confident | 0.94 |
| They have much knowledge about the work that needs done | 0.89 |
| They are well qualified for their jobs | 0.93 |
| Information Utility (CR = .95): To what extent do you agree with the following descriptions regarding the COVID-19 information released by the health authorities? | |
| Accurate | 0.92 |
| Transparent | 0.92 |
| Up to date | 0.91 |
| Useful | 0.91 |
| Affective Response (CR = .88): With respect to the COVID-19, how much do you agree with the following statements? | |
| I feel fearful | 0.85 |
| I feel sad | 0.80 |
| I feel worried | 0.87 |
| Perceived Risk (CR = .77): With respect to the COVID-19, how much do you agree with the following statements? | |
| The coronavirus is nearly everywhere, and very transmissible | 0.67 |
| There is a high probability of getting infected | 0.75 |
| The mortality rate of COVID-19 is high | 0.72 |
| I have no confidence I can avoid the negative impact of COVID-19 | 0.70 |
| Perceived Efficacy (CR = .79): To what extent do you agree that you can take the following measures in preventing COVID-19? | |
| Wearing a face mask | 0.53 |
| Washing hands | 0.58 |
| Keeping social distance | 0.80 |
| Self-quarantine | 0.76 |
| Conducting COVID-19 testing | 0.71 |
Note. CR = composite reliability.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by City University of Hong Kong, grant number 9380119, 7005703.