
Abstract
While scholars have highlighted how science communication reifies forms of structural inequality, especially race and gender, we examine the challenges science communication pose for religious minorities. Drawing on the disproportionate magnitude of COVID-19-related morbidity on Israel’s Ultra-Orthodox Jews, we examined their processes of COVID-19 health decision making. Survey results show that both religious and health-related justifications were common for personal decisions, yet a disparity was found between the ways social distancing guidelines were perceived in the general education context compared with the religious context, signaling the importance for inclusive models of science communication that account for religious sensibilities and state-minority relations.
Keywords
COVID-19, Religion, and Ethnic Minorities
As the COVID-19 pandemic shifted from East Asia to Europe and then to North America, the public media began reporting the disproportionate effects of the pandemic on minority groups. The American Centers for Disease Control and Prevention (CDC) noted that while “The effects of COVID-19 on the health of racial and ethnic minority groups is still emerging . . . data suggest a disproportionate burden of illness and death among racial and ethnic minority groups” (CDC, 2020). In the United Kingdom, an official report by Public Health England (published in BBC News on June 2, 2020; Nagesh, 2020) stated that “Black people are almost four times more likely to die of COVID-19, according to the Office of National Statistics, while Asians are up to twice as likely to die.” From the CDC to The New York Times to the BBC, the painful question resonated loud and clear: “Why are more people from BME 1 backgrounds dying from coronavirus?” (Butcher & Massey, 2020).
In response to these alarming data, amplified by the killing of George Floyd, which generated renewed public commitment to “Black Lives Matter,” researchers have put forward a variety of interpretations for the disparities in health equity. It has been argued that the pandemic exposes and reifies existing disparities in health care that are linked to structural inequalities. The CDC report indicated that “The conditions in which people live, learn, work and play contribute to their health. These conditions, over time, lead to different levels of health risks, needs and outcomes among some people in certain racial and ethnic minority groups” (CDC, 2020). Growing scholarship in the field of social epidemiology and public health have called for better data collection which includes socioeconomic information as well as race and ethnicity to better understand health equity and inform public health agendas and resource allocation (Bauer, 2014; Chen & Krieger, 2020).
The disproportionate effect of COVID-19 on minorities has also prompted the field of science communication to rethink the analytical tools employed to examine science communication among ethnic and racial minorities. On June 12, 2020, the standing committee on advancing science communication of the National Academies of Sciences, Engineering and Medicine devoted a special webinar to “The Role of Science Communication in Addressing the Disproportionate Effects of COVID-19 on Vulnerable Populations.” This debate is grounded in a decade of research that has highlighted various disparities in science education and communication (Bolger & Ecklund, 2018; Feinstein, 2017; Feinstein & Meshoulam, 2014). Even though there has been rapid growth in science information, access to science-related information and public engagement with science are still inequitably distributed (Canfield et al., 2020). In a recent manifesto arguing for a model of inclusive science communication, Canfield et al. argued that “as a result of science communicators’ cultural and epistemological tunnel vision, their efforts tend to benefit specific (e.g., affluent, college-educated, non-disabled) audiences.” Dawson (2019) commented that “to continue with business as usual is to be complicit in practices that uphold and exacerbate racism, class discrimination, sexism, and other forms of oppression” (p. 170).
Although these studies have highlighted the ways science communication reifies existing forms of structural inequality, while primarily focusing on race, gender and disabilities, the particular challenges posed by science communication for religious minorities have received less attention. While the study of science and religion has flourished over the past two decades, it has mainly focused on conservative, White protestants (Bolger & Ecklund, 2018). In consequence, the focus on the perceived conflict between religious teachings and science, and particularly on evolution, has dominated literature and public discourse on science-religion conflicts (Bolger & Ecklund, 2018). These studies also tend to amplify theological tensions while endorsing a “conflict narrative” (Evans & Evans 2008) that primarily characterizes people of faith in stark opposition to science (Carlisle et al., 2019; Chan, 2018; Elsdon-Baker, 2015). For example, researchers have argued that some religious groups do not seek out scientific knowledge because they are opposed to the all-encompassing veracity of science (Allum et al., 2014). Others suggest that Americans operate either religious or scientific epistemologies (O’Brien & Noy, 2015), reflecting the perceived conflict between science and religion in U.S. society (Ecklund, 2010). While these studies have tended to solely focus on theological tensions, Bolger and Ecklund (2018) recently suggested to pay attention to issues of bias and authority. For example, scholars have shown that conservative Protestants are not skeptical of science per se, but rather of scientists and their authority over truth (Bolger & Ecklund 2018; Evans, 2011).
The move from conceptual conflicts focused on theology and belief has also inspired scholars to push for studying ordinary religious people’s religious attitudes, views, and behaviors, instead of constantly focusing on religious leaders and elites (Evans, 2011, Evans & Evans 2008; Falade & Bauer, 2018). By focusing on everyday attitudes and behaviors, scholars have documented how science and medicine are embraced selectively, especially in cases when they can mirror and bolster communal norms. Assisted reproductive technologies, for example, has been passionately embraced through creative processes of “koshering medicine” (Ivry, 2010), as reproductive technologies enhance Jewish and Muslim prenatal ideals (see Inhorn & Birenbaum-Carmeli, 2008).
Whereas scholarship has mainly focused on strategies of integration of science in formal-educational or experimental settings among religious minorities (Asghar et al., 2014; Piew Loo, 2001), the naturalistic context of science communication has rarely been addressed (Jones et al., 2019; Jones et al., 2020). To put it simply, none of these studies have attempted to respond to the key question: How do religious minorities engage with/and learn about science in their everyday lives? Is conventional public health messaging effective when dealing with a minority population with specific cultural practices and religious beliefs? And, what are the limits of receptivity of science and health advice among specific minority groups?
COVID-19 provides a unique opportunity to pursue this line of exploration. In the study reported here, we explored the ways Ultra-Orthodox Jews in Israel learned about the pandemic and examined their COVID-19–related decision-making. In Israel, at the height of the pandemic in March to June 2020, Ultra-Orthodox (Haredi) Jews accounted for 40% to 60% of all coronavirus patients at four major hospitals, even though they make up only 12% of Israel’s population (Eligon et al., 2020; Waitzberg et al., 2020). Researchers have attributed this disproportionate effect to overcrowding and large families as well as a variety of socioreligious factors (e.g., Waitzberg et al., 2020). Here, we draw on studies in science communication to shed light on the particular types of science communication and decision making that characterize COVID-19-related decision making among Israel’s Ultra-Orthodox Jews. We argue that science-related communication and decision making is negotiated within and through many actors and systems of “local” knowledge, since both scientific knowledge and socioreligious frameworks serve as “cultural and epistemological tunnels” of COVID-19 interpretations, attitudes, and behavior (Canfield et al., 2020; Goldberg et al., 2019). While scholars have argued that individuals operate either religious or scientific epistemologies (O’Brien & Noy, 2015), we demonstrate how both religious and health-related rationalizations interact in the ways Haredi men and women make COVID-19-related decisions. The findings make a strong case for the importance of religious-sensitive science communication.
Education, Media, and Communication in Israel’s Haredi Community
Haredim (Ultra-Orthodox Jews), who are often referred to as an enclave with strict social and cultural boundaries, account for roughly 12% of Israel’s population (Israel Central Bureau of Statistics [ICBS] 2018; Sivan, 1995; Stadler, 2009). Haredi men and women live in accordance with the teachings of the Hebrew Bible (Tanakh) which have been reinterpreted through a voluminous body of rabbinic literature, commentary, and rulings over the centuries. Haredi Jews can be distinguished from Progressive, Conservative, and Religious-Zionist Jewish streams by their self-protective stance and avoidance of secular education and professional training. In practice, the Haredi sector consists of multiple groups, each with its own religious leaders (rabbis), teachings, and rites. This population can be loosely divided into Lithuanian yeshiva-based (Torah learning) communities, Hasidic dynasties, and Sephardi Haredim (who trace their origins to the Iberian peninsula, North Africa, and the Middle East). Differences aside, all Haredim are easily identified by their more or less uniform dress code: black hats and dark suits for men, and similarly colored ankle-length skirts, long sleeves, and head coverings or wigs for women (Taragin-Zeller, 2014, 2015).
Among Haredim, religious knowledge is prized over institutional formal learning and informal learning. Research has emphasized the importance of the Haredi formal schooling system, leading to what Friedman (1991) termed a society of learners. Haredi society venerates religious Torah learning as the main pathway to piety for men, while marginalizing other activities, including employment (Hakak, 2012; Stadler, 2009; Stadler & Taragin-Zeller, 2017; Taragin-Zeller, 2017). Historically, Haredim in Israel have acquired varying levels of autonomy from national curriculums and regulation (e.g., Perry-Hazan, 2015), which enable them to disengage from subjects that pose challenges to their inner-communal worldviews and lifestyles. For this reason, the Haredi community has developed its own educational system that is made up of segregated K-12 schooling for boys and girls, followed by an extensive network of institutions of higher religious study for men.
Very broadly speaking, Haredi schools aim to prepare youngsters for their gender-specific roles in society—males as religious scholars, and females as breadwinners and domestic caregivers. For this reason, STEM (science, technology, engineering, and mathematics) subjects are sparsely taught in Ultra-Orthodox schools (Manny-Ikan & Rosen, 2013). Haredi female pupils usually study math and science (termed the Wonders of Creation) up to the age of 15 years, since women are expected to navigate the non-Haredi world as wives, mothers, and the main breadwinners. The Haredi education system raises boys, on the other hand, to be Torah scholars, who need little formal science or math education. Thus, most male students do not learn science beyond fifth or sixth grade (ages 11-12 years; Manny-Ikan & Rosen, 2013).
In the past, Israel’s efforts to introduce basic scientific learning into the curricula were repelled by political pressure. However, over the past two decades, minimal core studies have been gradually introduced via a number of school reforms (Katzir & Perry-Hazan, 2019). However, the science literacy gap between Haredi and secular education continues to grow. Currently, many Haredi groups, and especially their leadership oppose national testing, which makes it impossible to conduct comparative assessments. In 2018, national tests (Meitzav) that included 110 Haredi schools, indicated a gap of 48.5 points between Haredi girls and their secular counterparts in language and math literacy, Haredi boys were 70 points behind their secular counterparts in language literacy and 90 points behind in math literacy (Ilan, 2018).
Haredim have their own sectorial press, that provides Haredi-filtered news, so as not to “contaminate” the Haredi home and protect their right “not to know.” Soon after the founding of the State of Israel in 1948, leaders of the Agudat Yisrael Haredi political party established Hamodia, which was followed by three more Haredi daily newspapers, each oriented toward different groups of Haredim. Rabbinic representatives “censor” the news, making sure to comply with religious standards as well as standards of modesty which prohibit images of women. Since the 1980s, commercially orientated independent Haredi media have emerged, which pose a challenge to the monopoly of the Haredi press (Cohen, 2012). The Haredi press does not have a designated section for science, so science-related information typically appears in the technology or health sections.
Even though there is still disapproval of internet use among Haredi leaders, in 2018 49% of all Israeli Haredim reported that they used the internet (Malach & Cahaner, 2019). The emergence and popularity of online media and their ubiquity have underscored their benefits for everyday life, entertainment, services, and commerce. Thus, in spite of virulent resistance among Haredi leadership, for almost two decades, the Haredi community in Israel (and the United States) has witnessed a sharp increase in the number of Haredi news websites alongside traditional print newspapers (Cohen, 2012; Golan & Mishol-Shauli, 2018). Today, there is a handful of Haredi news websites (e.g., Kikar Shabbat and B’Hadrei Haredim), which report uncensored information, and one also shows pictures of women. The other influential sector of Haredi-targeted news is radio channels, which are all broadcast by men. Haredi radio shows are one of the most influential routes into the Haredi home, since no Haredi TV channels exist.
Haredim and COVID-19
The first case of COVID-19 in Israel was confirmed on February 21. Beginning on March 11, the Israeli government put forward an increasingly restrictive set of social distancing measures, culminating in a full lockdown by March 19. The number of infected cases rose rapidly during the last week of March, resulting in 6,092 confirmed cases by the beginning of April. Throughout the second half of March, when the data collection for this study took place, the Israeli media were overwhelmingly focused on the virus, reported daily on its rapid spread and the measures the Ministry of Health was putting forward to monitor and contain the spread of the pandemic in Israel. This “state of national emergency” is the backdrop for this study.
During this state of emergency, Haredi Jews were slower to adhere to social distancing guidelines than other groups in Israeli society (Waitzberg et al., 2020). This reluctance has been attributed to various theological, cultural, and political causes. Some have blamed inner-communal media outlets for not reporting the dangers sufficiently, whereas, others have pointed to the ways social distancing disrupts the core of Jewish life which is based on religious obligations performed in the presence of other Jews. Like other religious groups who have struggled with social distancing guidelines, Haredi Jews found it very hard to close places of worship, which constitute the heart and the very essence of Haredi Judaism. Prayer, boys’ Torah study houses, and women’s ritual immersion in a Mikveh, 2 cannot be simply moved to Zoom.
By the end of March, the epidemiological disaster was undeniable: There were significant clusters of infections in Haredi neighborhoods, 40% to 60% of all coronavirus patients at four major hospitals, even though they make only 12% of Israel’s population (Eligon et al., 2020). The first member of the government to be infected, the Haredi Minister of Health Yaakov Litzman and his wife, tested positive for the coronavirus on April 2, after being spotted praying at a synagogue, when Israel was already under lockdown.
It is important to note that Haredim are not one unified group, and there were indeed many Haredim who practiced social distancing and complied to public health guidelines. Yet Haredi reluctance to social distance, together with their large households (seven children on average) and low socioeconomic levels (ICBS, 2018; Taragin-Zeller, 2019a, 2019b, in press), all contributed to the impact of the pandemic on Israel’s Haredi community. The first Israeli city to be declared a “restricted zone” was the city of Bnei Brak, the heart of Israel’s Haredi communities. This aggravated the existing gap between Haredim and other sectors of Israeli society, with non-Haredi groups distancing themselves physically to avoid becoming infected.
In Israel, the most well-defined and prominent minority groups are Haredim and the Arab population (both Muslim and Christian). Although the government was slow to recognize the need to tailor their messaging to both communities, by the beginning of April the Ministry of Health created a Haredi-targeted campaign to provide Haredim with information about COVID-19 that was presented in Haredi-acceptable religious and cultural frameworks. 3 As Passover approached, they also tailored instructions to the Haredi community, which was later implemented for Muslim Arabs during Ramadan starting at the end of April. To prevent large infection (similar to the one caused during Purim celebrations on March 8 and 9), for the week-long Passover holiday (April 8-15) the government enforced a 3-day nationwide lockdown in Jewish cities to further contain the spread. As some parts of Israel’s Arab society have features in common with Israel’s Ultra-Orthodox Jews (mainly, low socioeconomic status and an intense social and communal life), in the context of COVID-19, the disproportionate effect was most striking among Israel’s Arabs and Haredim (Waitzberg et-al., 2020).
On May 4, a gradual easing of lockdown restrictions was approved by the government, which primarily involved on the lifting of the 100-m limit on travel from one’s home together with a gradual shift back to school and work. By May 20, the beaches and museums reopened and group prayer was allowed for up to 50 participants. Yet at the time of this writing (August 2020), a second wave has materialized in Israel. As new hotspots emerge all over the country, the disproportionate effect of infection among Israel’s ethnic and religion minorities continues. The current study focuses on the disproportionate effect of the pandemic on Israel’s Haredi communities to examine engagement with science and health that characterizes COVID-19-related decision making among religious minorities.
Method
The aim of the current study was to explore the interactions between science knowledge and personal health decision making in the context of COVID-19 among Haredi Jews in Israel. An online questionnaire was administered to collect participants’ stances regarding culturally specific COVID-19–related dilemmas. We gathered educational and demographic background information, and then asked the participants to read five COVID-19–related dilemmas that incorporated a potential conflict between health considerations and religious norms. 4 Each respondent was asked to report their solution to each dilemma that corresponded best to their own attitudes, and then explain why.
Research Tool
The questionnaire (Supplemental Appendix, available online) was based on earlier science literacy research tools that use everyday scenarios (Shauli & Baram-Tsabari, 2019). It was constructed around five real-life culturally specific dilemmas, and included measures of general science knowledge, knowledge about COVID-19, and demographics.
Culturally Specific COVID-Related Dilemmas
Dilemmas were designed to assess how Haredi men and women make COVID-related decisions amid changing guidelines. To give one example: the major Jewish festival of Passover took place during the month of April, at the height of the outbreak in Israel. Typically, the celebration entails a 7-day festival, beginning with a large family meal on the first night, usually including the entire extended family. In a typical Haredi family, where a nuclear family has an average of seven children (ICBS 2018), this could easily involve 20 participants or more. The Ministry of Health took extreme measures in April to prevent extended families from celebrating together by enforcing a 3-day nationwide lockdown for the duration of the holiday. However, at the time of data collection (March 17-27) no such guidelines were in place, and few if any would have predicted it. The dilemma as formulated in the questionnaire was as follows: “Imagine that Passover is next week. Your whole extended family is expected to celebrate the Seder together at your house. Will you still hold the Seder, including with older members of the family despite COVID-19?”
Then, respondents were asked to indicate how confident they were with their decisions, the reasoning or rationale for their decisions, and who they would consult for advice. 5 The other dilemmas in the questionnaire dealt with communal prayer, Torah study at seminaries, and wedding attendance when one should be in self-isolation.
Knowledge About COVID-19
Knowledge about COVID-19 was measured based on the response to the following question: A number of Israelis returning from trips abroad were told to go into quarantine for two weeks even though they had been out on the street for more than a week before the rule was put in place. In your opinion, why would going into quarantine a week later help stop the spread of the virus?
General Knowledge About Science
Scientific knowledge was measured on three close-ended questions which covered factual knowledge, grasp of statistics, and procedural knowledge. These questions were taken from the U.S. National Science Foundation Battery, a widely used research tool to assess public understanding of science (National Science Board, 2018). These questions were followed by one open-ended question: “Why is it a better way to test the drug this way?” One point was given for each correct answer. For the open-ended question, respondents scored one point for a scientifically logical explanation (e.g., “Because there is a control group”). The highest potential score was 4.
Demographic Variables
The demographic variables included self-reports of gender, age group, place of residence, occupation, highest level of completed formal education, all as multiple-choice items.
Content Validity
Content-related validity of the research tool was established nonstatistically using expert professional judgment, who addressed domain specification, content universe and sample, item development, item wording, and format. The questionnaire benefited from the constructive feedback of 10 science communication and science education specialists, three of whom had a specific expertise in religion, with particular knowledge of Haredi society.
Cognitive Validity
We gave six Haredim (three women and three men) a draft of the questionnaire and asked them to fill it out. The main feedback was that they were worried that Haredim would feel that they were being singled out as a group. Given the tension related to science education in Israel, they suggested we add another sentence that explicitly stated that this questionnaire was part of a larger survey that did not only focus on Haredim. They also suggested that the demographic question about level of education should correspond to the Haredi system (elementary, Yeshiva) rather than the secular grade system (elementary school, middle school, and high school education).
Pilot
A pilot version was tested on a sample of 10 respondents purposely sampled to check culturally specific sensitivity. The questionnaire was subsequently modified for clarity based on their feedback.
Data Analysis
Respondent’s Justifications for Their Stance on Culturally Specific COVID-Related Dilemmas
A codebook was developed that included the following categories: (1) Justification theme (Table 1, intercoder reliability κ = .895). In case of multiple justifications, up to three different themes were coded. (2) Spontaneous reference to sources of authority (Table 2, intercoder reliability κ = .893). The coding process was conducted by two coders and a reliability test was run for 10% of all answers (50 answers for each dilemma). Based on the codebook, we developed additional variables:
Response quality (0-5): The quality of justifications was based on (1) providing a justification, (2) the number of health- or science-related arguments, and (3) reference to a relevant information source, using manual content analysis.
Percentage of health-related and religion-related claims: For each respondent, we calculated the proportion of health-, medicine-, and science-related justifications, and religious justifications (Table 1) out of the total number of justifications. Scores could range from 0 to 1.
Coding Scheme and Distribution of Respondents’ Justifications for Their Stance on Culturally Specific COVID-Related Dilemmas.
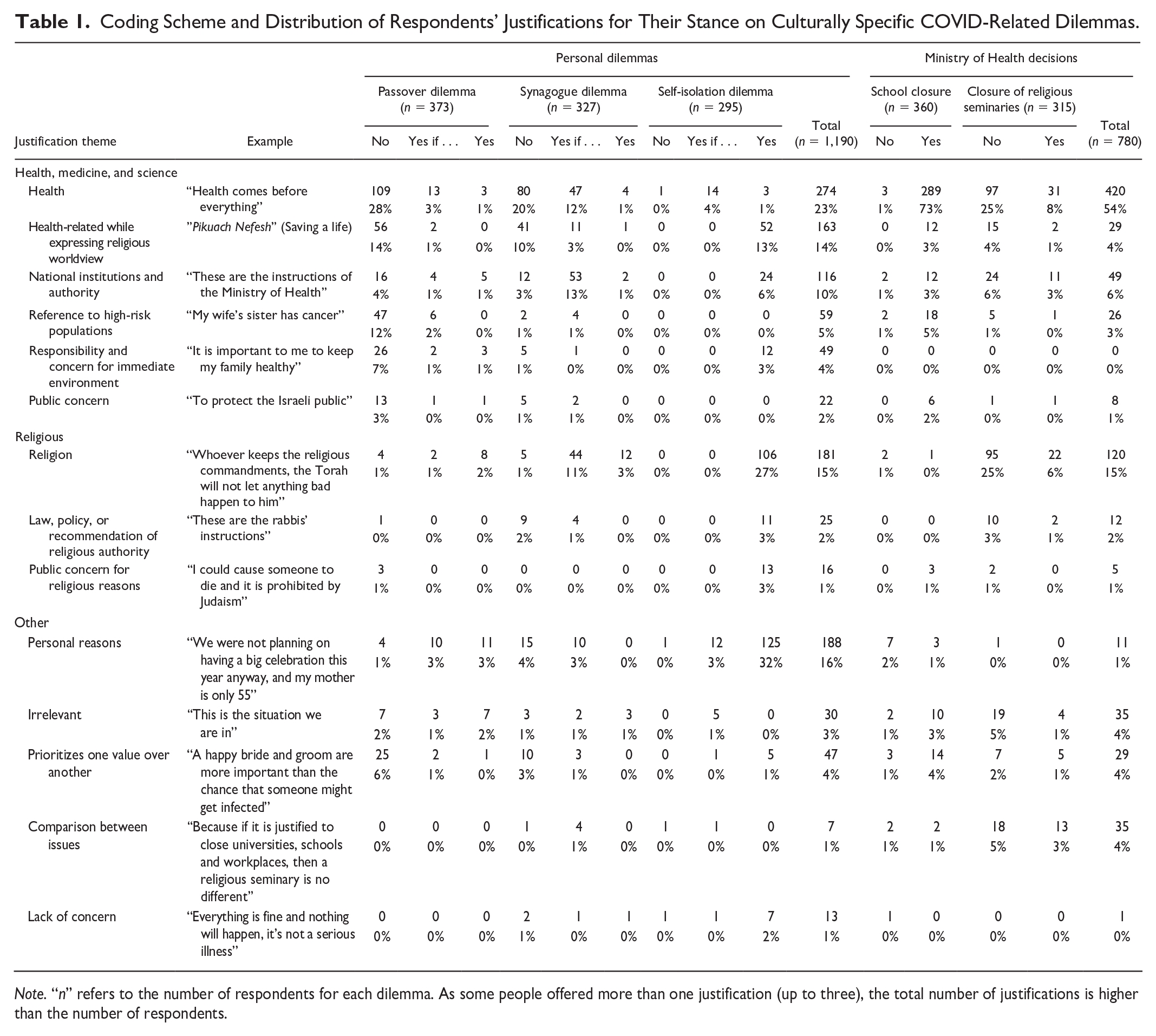
Note. “n” refers to the number of respondents for each dilemma. As some people offered more than one justification (up to three), the total number of justifications is higher than the number of respondents.
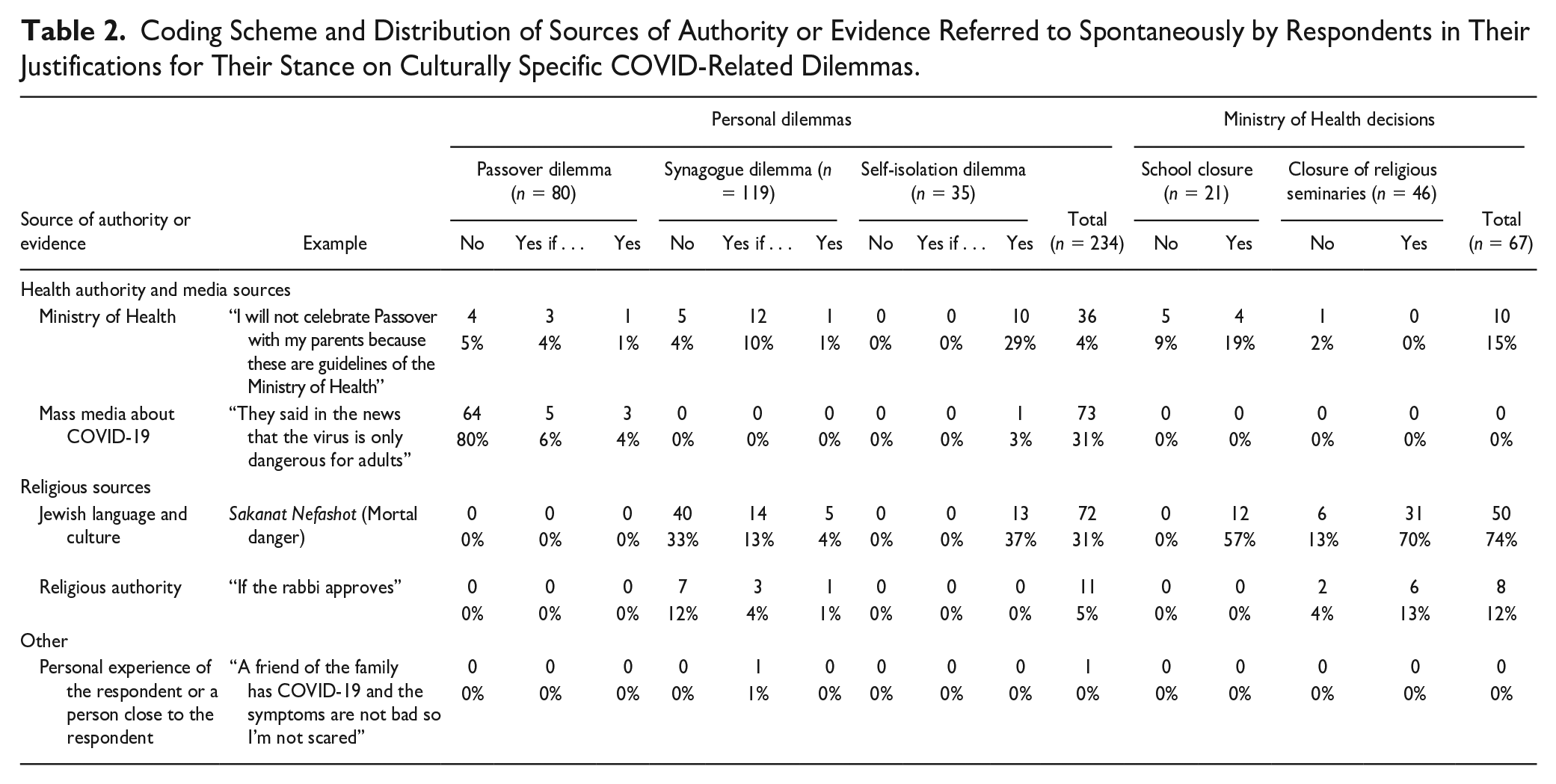
Coding Scheme and Distribution of Sources of Authority or Evidence Referred to Spontaneously by Respondents in Their Justifications for Their Stance on Culturally Specific COVID-Related Dilemmas.
Knowledge About COVID-19
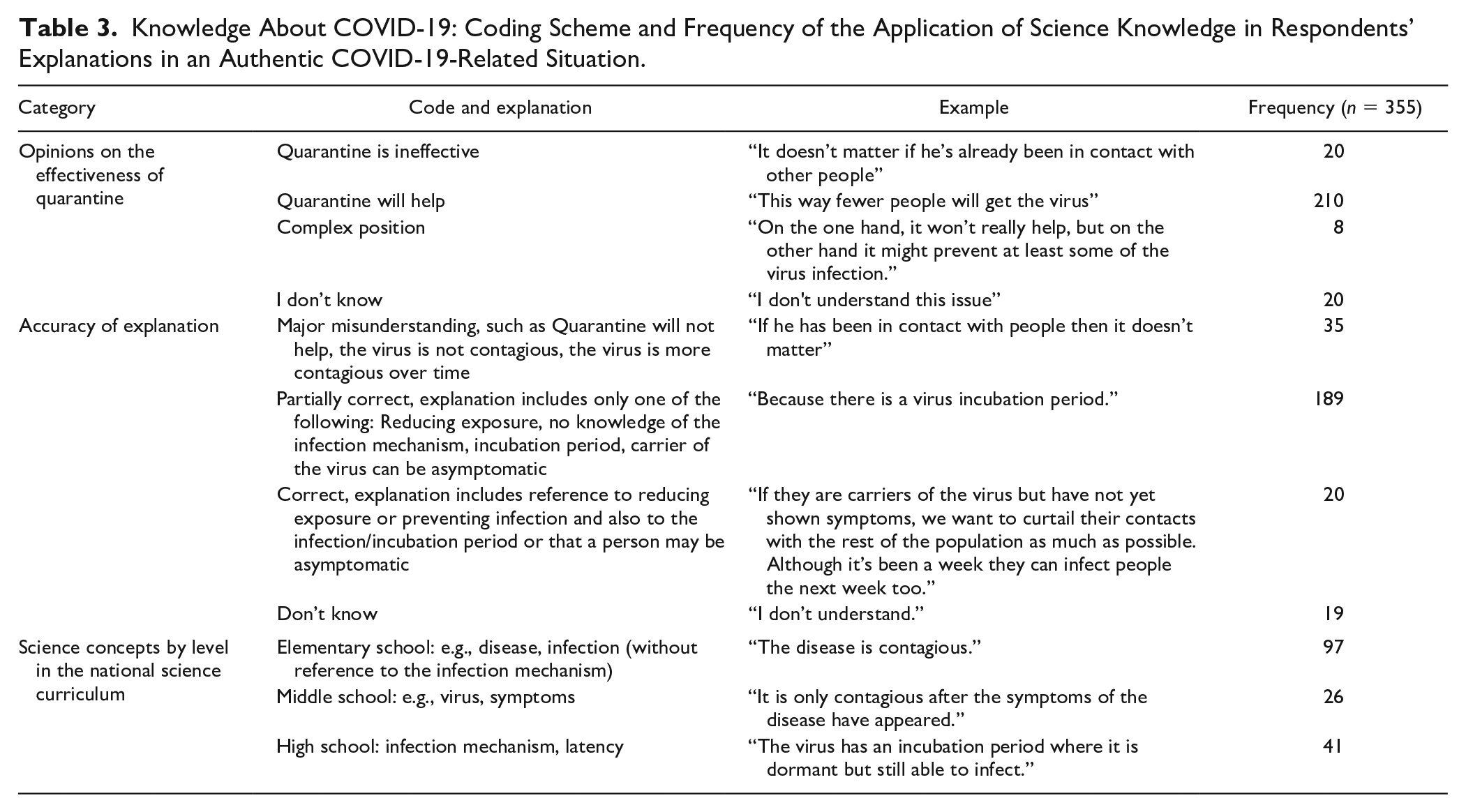
An open question about the efficacy of quarantine was used to assess knowledge about COVID-19. Based on PISA’s definition of scientific explanation we evaluated the application of scientific content knowledge to interpret and explain phenomena (OECD, 2017), using the following categories (Table 3): (1) respondent’s position regarding the efficacy of quarantine (intercoder reliability κ = .804), (2) correctness of the answer (intercoder reliability κ = .822), and (3) number and level of scientific concepts used. The concepts were characterized according to author’s protocol (Laslo & Baram-Tsabari, 2020), which is based on the inclusion of scientific concepts in Israeli science curricula for elementary, middle, and high school. One point was given for each elementary concept, two for each middle school–level concept, and three points for each high school–level concept. The scores for knowledge about COVID-19 ranged from 0 to 16 (mean = 2.7).
Knowledge About COVID-19: Coding Scheme and Frequency of the Application of Science Knowledge in Respondents’ Explanations in an Authentic COVID-19-Related Situation.
Sources of Information
Two dilemmas (Passover, home quarantine) had an additional follow-up question of “Whom would you consult?” Respondents could check as many responses as applicable from the seven listed: health-related sources (physician, internet website of the Israel Ministry of Health or local health services, internet website of a research institute or university), religious sources (Rabbi, Rebbetzin, or search for a Jewish law responsa online), friend or family member, or a general online search. Based on the open answers in the “other” category, two additional sources of consultation were added: mass media and “I would not consult anyone.”
Statistical Analysis
The effects of the justification type and the stance on the proportions of justifications were analyzed using a mixed-design analysis of variance with a within-subjects factor of justification type (health- or religious-themed) and a between-subject factor of stance (No; Yes; Yes, if). The differences in the proportions of health- and religious-themed justifications for each type of stance were analyzed with paired t tests.
The association between the type of educational institution (schools, universities, or religious seminaries) and respondents’ stance on closing them was tested with Pearson’s chi-square test. Generally, the associations between two continuously measured variables were calculated by Pearson correlation coefficients.
Sample
Participants were recruited by the market research firm Eskaria, an online panel with particular expertise in conducting surveys among Hebrew-speaking Haredim who are internet users. In total, 552 participants completed the questionnaire. Of these, 33 participants were removed from the analysis because they did not self-identify as Haredim and another five were removed for completing the questionnaire too quickly (<100 seconds). Average completion time for the remaining 514 respondents was 33 minutes and these were retained in the analysis.
Even though the sample was not selected randomly, in terms of representativeness, the sample was similar to the general population in most categories. Almost all respondents had studied in an Ultra-Orthodox elementary school (95.7%) and their marital status was similar to the high marriage rates in the Haredi population (83% married). Yet the sample included more women (56.1%) than men (43.9%) 6 and participants were more educated than the Haredi average 7 : 35% had a high school diploma (compared with 14% in the general population), 40% had completed a professional training course (compared with 29% in the general population), 24.5% had or were completing a BA degree (compared with 20% in the general population). In terms of employment, whereas 56% of the Haredi men in the sample worked (compared with 57% in the Haredi population), almost all the Haredi women worked (96%, compared with 76% in the Haredi population).
The religious affiliation of respondents was also very similar to the general Haredi population, with the exception of slightly more Lithuanian men and women (38.2% vs. 29% in the general population). The sample also included men and women who were more exposed to Internet use and smartphones than the general Haredi population (e.g., 56.4% used nonkosher smartphones (without any filtering) or had two mobile devices (compared with 37.5% in the general Haredi population). The survey was launched on March 17 and closed on March 28, 2020. The study was reviewed and approved by the Institutional Review Board at the Technion–Israel Institute of Technology (Approval No. 2020-028).
Methodological Limitations
Several limitations should be considered when interpreting the results. First, not all Haredim use the internet. Before COVID-19, only 50% of Haredi men and women reported using the internet. However, as COVID-19 spread, internet use among Haredim continued to rise. While it is hard to arrive at a definitive number, Israeli media has reported various estimates, the highest claiming that Haredi internet use jumped to 90% (Walman Israel, 2020). Even though this number signals a clear-cut change, this survey reflects only those who responded to an online survey, a methodological limitation that must be taken into consideration. In addition, it is much more difficult to contact more elderly Haredim through an online survey. The survey company made a concerted effort to reach elderly participants, but only 1% of the participants were older than 60 years. In addition, there were more responses to the multiple-choice questions than the open-ended questions (an average of 398 responses compared with 334).
While the questionnaire was being circulated, social distancing guidelines were continuously changing. Anxiety amid constant change prevailed. It was within this dynamic context that participants completed this survey. More specifically, the religious seminaries were closed by the Israeli government 24 hours after this survey was launched. To take this into consideration the questionnaire language was modified slightly and this change was accounted for during the analysis.
Results
First, we detail the results by dilemma, and then discuss the cross-cutting findings.
Part 1: Personal Decision Making
Passover Dilemma
The first dilemma asked participants to state how they would hold their celebratory family dinner for Passover given the stringent social distancing guidelines. Of those responding (n = 436), the vast majority of the respondents (54.5%) said they would not celebrate with their extended families, 13.6% reported they were unsure. An additional 8.8% of respondents said they would celebrate as usual, and 8% reported they would celebrate with their extended family under certain conditions (e.g., only if social distancing rules can be abided by). In their responses, participants typically stressed the importance of Passover, and especially the festive Seder night, despite rising infection rates and health guidelines: The Seder night is a special event, and an important one, and we can’t let the elderly be by themselves, but we don't know where infections come from. We are still young, and if we get sick we will get better, please God, but we can’t take a chance like that for our amazing Grandma. (Shoshana,
8
age range = 25-29 years)
The respondents’ decision-making rationalizations were classified into 11 types (Table 1), in order of prevalence: (1) health-related justifications—31.9%; (2) reference to high-risk populations—14.6%; (3) health-related justifications linked to religious language and culture—12.7%; (4) prioritization of one justification over another—7.6%; (5) showcasing responsibility and care for immediate environment—7.4%; (6) reference to personal reasons—6.6%; (7) reference to law and public policy guidelines—5.9%, lack of concern—5.3%; (8) public concern—3.8%; (9) religious reasoning —2.5%; (10) public concern while referencing religious discourse—0.6% (11) reference to public law or health authority recommendations from rabbinic authorities—0.2%.
Synagogue Dilemma
The second dilemma had to do with prayer attendance given government restrictions that limited groups to a maximum of 10 people. In Orthodox Judaism, Jews have an obligation to pray three times a day. While individual prayer is often recited, there are particular prayers that necessitate a quorum of 10 men
9
(minyan). Throughout the week, Haredi Jews typically try to attend group prayer but also pray individually at home when they have work obligations or for personal reasons. However, the majority of Haredi Jews attend group prayer at communal synagogues every weekend on the Sabbath (Saturday). In addition, Haredi interpretations of Jewish law stress this obligation to men. Even though some Haredi women attend synagogue, which varies among different communities, Haredi men attend group prayer (Friday night, Saturday morning, and Saturday afternoon). Based on this pattern of Haredi prayer, we asked the following question: The International Association of synagogues has limited numbers of group worship to a maximum of ten people, but the head of Maaynaei Hayeshua hospital has asked the public not to go to synagogues at all. What are you going to do this Shabbat?
Of those responding (n = 434), 44% said they would not go to the synagogue at all. An additional 40.8% responded that they would go to the synagogue and/or send their husband and children to the synagogue only if the attendant made sure there were not more than 10 attendees. 9% responded “Other,” and 6.2% responded that they would go to the synagogue and/or send their husbands and children to the synagogue in any case. The synagogue dilemma elicited tensions, such as “There is no way to pray inside a building and adhere to social distancing. We need to follow the Ministry of Health’s guidelines” (Avraham, age range = 18-24 years). Many compared the obligation to pray with the religious obligation to stay safe, stating that “Praying is a religious obligation, but so is Pikuach Nefesh!” (“You shall safeguard your lives”; Meir, age range = 35-39 years).
The decision-making rationalizations, as rank ordered in Table 1 were (1) health-related justifications—30.8%, (2) reference to law and public policy guidelines—15.4%, (3) religious reasoning—14.3%, (4) health-related justifications linked to religious language and culture—11.5%, (5) reference to personal reasons—5.9%, (6) showcasing responsibility and care for the immediate environment—5.6%, (7) prioritization of one justification over another—3.5%, (8) reference to high-risk populations—3%, (9) reference to public law or health authority recommendations from rabbinic authorities—3%, (10) public concern—1.9%, (11) comparison between different situations—1.1%, (12) lack of concern—1.1%.
Self-Isolation Dilemma
During the pandemic, the Israeli government directed all returning Israelis or tourists to spend 14 days in isolation. We devised a culturally specific self-isolation dilemma that conflicts with attending the wedding of a family member. In Judaism, marriage is valued highly and going to weddings especially among members of one’s extended family is very important. The participants were asked what they would do in the following scenario: “Suppose you just got back from New York last week, and you are feeling great. Your cousin is getting married tomorrow night. Will you adhere to home isolation guidelines?”
Of those responding (n = 395), 91.6% indicated that they would adhere to quarantine guidelines. 7.6% participants stated they would only partially adhere to the guidelines. 0.8% participants admitted they would not follow the guidelines, and would go to the wedding. Of all the responses, most of the participants were concerned they would infect others, for example, “I don’t think I can take on the responsibility of making others ill, in case I am ill” (Sarah, age range = unknown).
We divided their decision-making rationalizations into 11 types (Table 1): (1) public concern—36.2%, (2) health-related justifications—27.9%, (3) reference to public law or health authority recommendations—12%, (4) health-related justifications linked to religious language and culture—6.5%, (5) reference to personal reasons—5.8%, (6) public concern while referencing religious discourse—3.2%, (7) showcasing responsibility and care for immediate environment—2.5%, (8) prioritization of one justification over another—1.47%, (9) reference to high-risk populations—1.1%, (10) comparison between different situations—1.1%, (11) lack of concern—1.1%.
Participants spontaneously referred to different sources of authority to justify their position on personal decisions (Table 2). Out of the 234 people who referred to sources of authority in their open-ended responses, the five most common were (1) Ministry of Health—15.4%, (2) mass media—31.9%, (3) Jewish language and culture—30.8%, (4) religious authorities—4.7%, (5) personal experience—0.4% (Table 2). These findings solidify our overarching argument regarding the dual usage of both religious and health- and science-related discourses and authority.
Part 2: Conformity to Health Guidelines
School Closure Versus the Closure of Religious Seminaries
The first three dilemmas pitted health guidelines against religious norms, and explored how individual Haredi men and women would make COVID-19-related decisions. The two next dilemmas examined the attitude of Haredim to official guidelines from the Ministry of Health that were put forward during the pandemic, shortly before the survey was administered. At two different points on the questionnaire we asked respondents to express their opinions on two decisions made by the Israeli Ministry of Health: “Do you think the Israel Ministry of Health’s decision to close all schools and universities was right?” and “Do you think the Israel Ministry of Health’s decision to close all religious seminaries was right?”
Whereas most respondents agreed that the decision to close all schools and universities was correct (94.9%), only 23.2% of the respondents agreed with the decision to close religious seminaries (Figure 1). There was a significant association between the type of educational institution and whether or not respondents agreed with the Ministry of Health’s decision, χ2(1) = 6.6, p = .01. An odds ratio indicated that the odds of respondents’ agreement with the Ministry of Health’s decision were 54 times higher if they were asked about the closure of schools and universities than if they were asked about the closure of religious seminaries (Table 4).
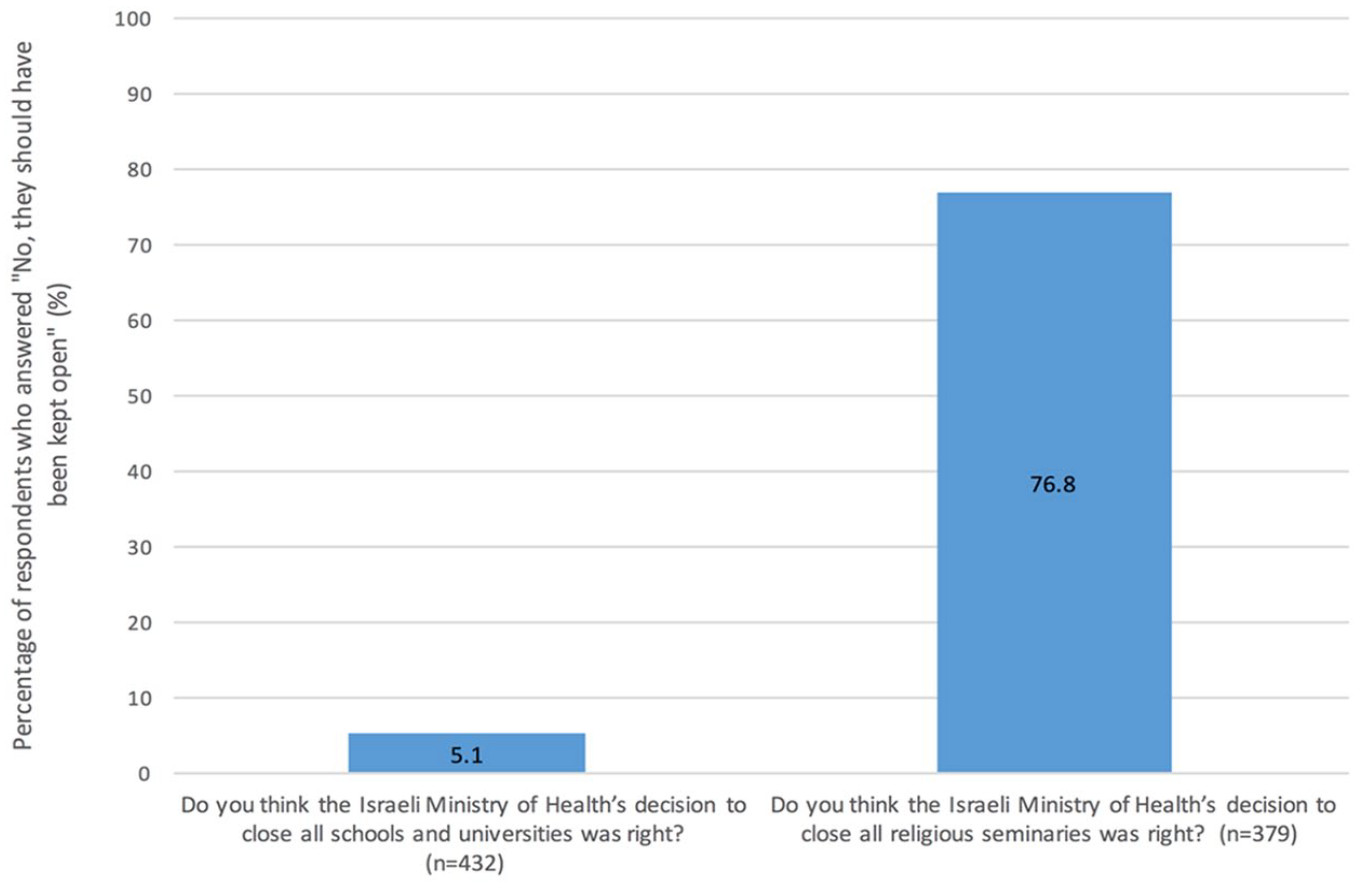
Stance regarding closure of schools versus religious seminaries. The percentage of respondents who agreed with the Ministry of Health’s decision to close all schools and universities, compared with the percentage of respondents who agreed with the Ministry of Health’s decision to close all religious seminaries.
Cross-Tabulation of Respondent’s (n = 378) Agreement With the Ministry of Health’s Decision to Close All Schools, Universities, and Religious Seminaries.
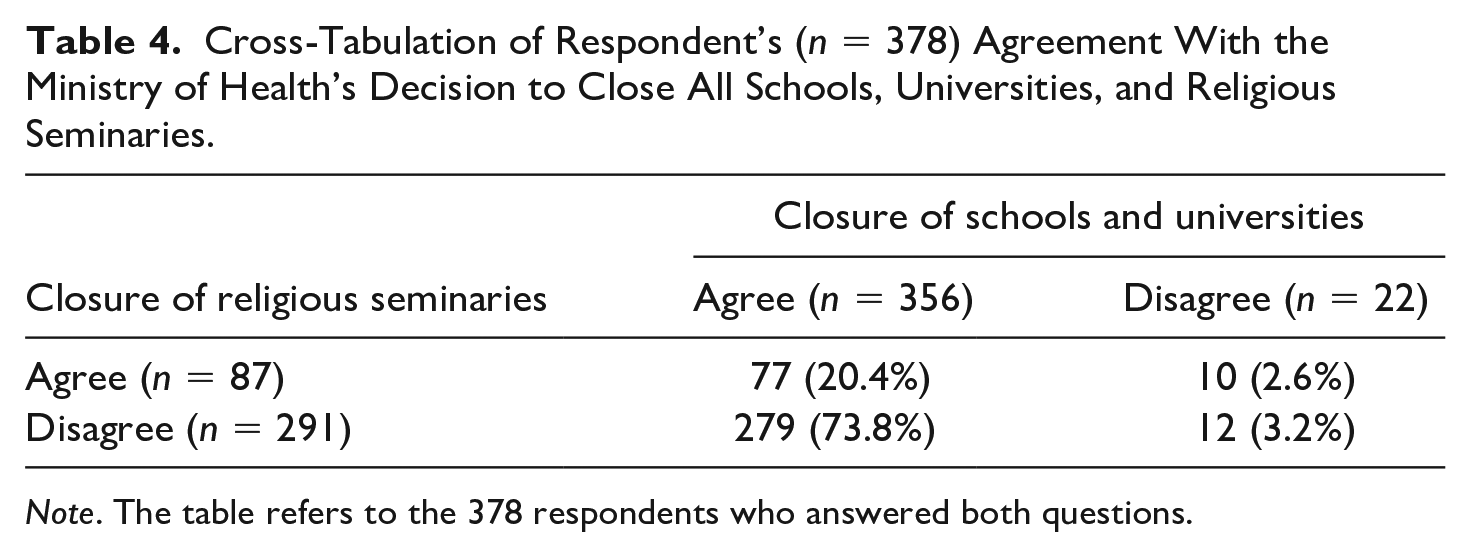
Note. The table refers to the 378 respondents who answered both questions.
For example, Rachel (age range = 20-24 years) said, “Torah study is what preserves the nation,” or as Miriam put it: “There is real danger, so yes, we should close but with a heavy heart. It is so hard. Because Torah study saves and sustains us” (age range = 20-24 years). Those who rejected the closure of religious seminaries often compared Torah study with other institutions that remained open during the pandemic, especially the army. For example, “Religious seminaries and the army are the same . . . it is a home and there is no reason to send them home. They can maintain the guidelines there!” (Rivka, 25-29 years). While the comparison to the army may come as a surprise, this is actually a common comparison among Haredim. As analyzed at length in the “Discussion” section, Haredim are constantly critiqued for their exemption from compulsory military service which also challenges their fulfillment of the duties of all Israeli citizens. The frequent comparison between army and Torah study typically supports Haredi logic that Torah study spiritually sustains Israeli society (see, Stadler, 2009).
The disparities between these two opinions are striking, signaling a gap between the ways Haredi men and women perceive social distancing in the context of general education versus their view of the ways social distancing guidelines should be applied in the religious context. There was also a clear association between level of conformity to the guidelines put forward by the Ministry of Health and the source of authority the participants stated they would consult for advice. The more respondents reported that they would consult with religious authorities, the more their level of conformity with state guidelines decreased. By contrast, the more respondents reported that they would consult academic sources, the more their level of conformity with state guidelines increased.
Participants spontaneously cited different sources of authority to justify their positions (Table 2). The breakdown in percentages of the 67 people who referred in their open answers to sources of authority were as follows: (1) Ministry of Health—14.9%, (2) mass media—0%, (3) Jewish language and culture—74.6%, (4) religious authorities—11.9%, (5) personal experience—0% (Table 2). These findings reflect a preponderant reliance on religious language and culture for justifications for these dilemmas. Since the number of participants who responded to this question was low, statistical analysis was impossible but it resonates with the other findings that men and women who accept the Ministry of Health’s logic refer less often to religious sources than those who do not.
Cross-Cutting Findings: Which Variables Are Associated With Conformity?
After reviewing the responses to each of the dilemmas and their justifications separately, we analyzed the level of conformity with health guidelines across the three culturally specific COVID-related dilemmas: (A) Passover dilemma amid social distancing: Will you be celebrating together with the whole family, including elderly family members? (B) Synagogue dilemma amid social distancing: Will you be going to pray in a synagogue? (C) Self-isolation dilemma: Will you self-isolate while your cousin is getting married?
The proportion of health- and religious-themed justifications was associated with the respondents’ stance (Figure 2): Conformity with health recommendations and guidelines were mainly justified through health-, medicine-, and science-related rationalizations, whereas disregarding health recommendations was associated with greater reliance on religious justifications.
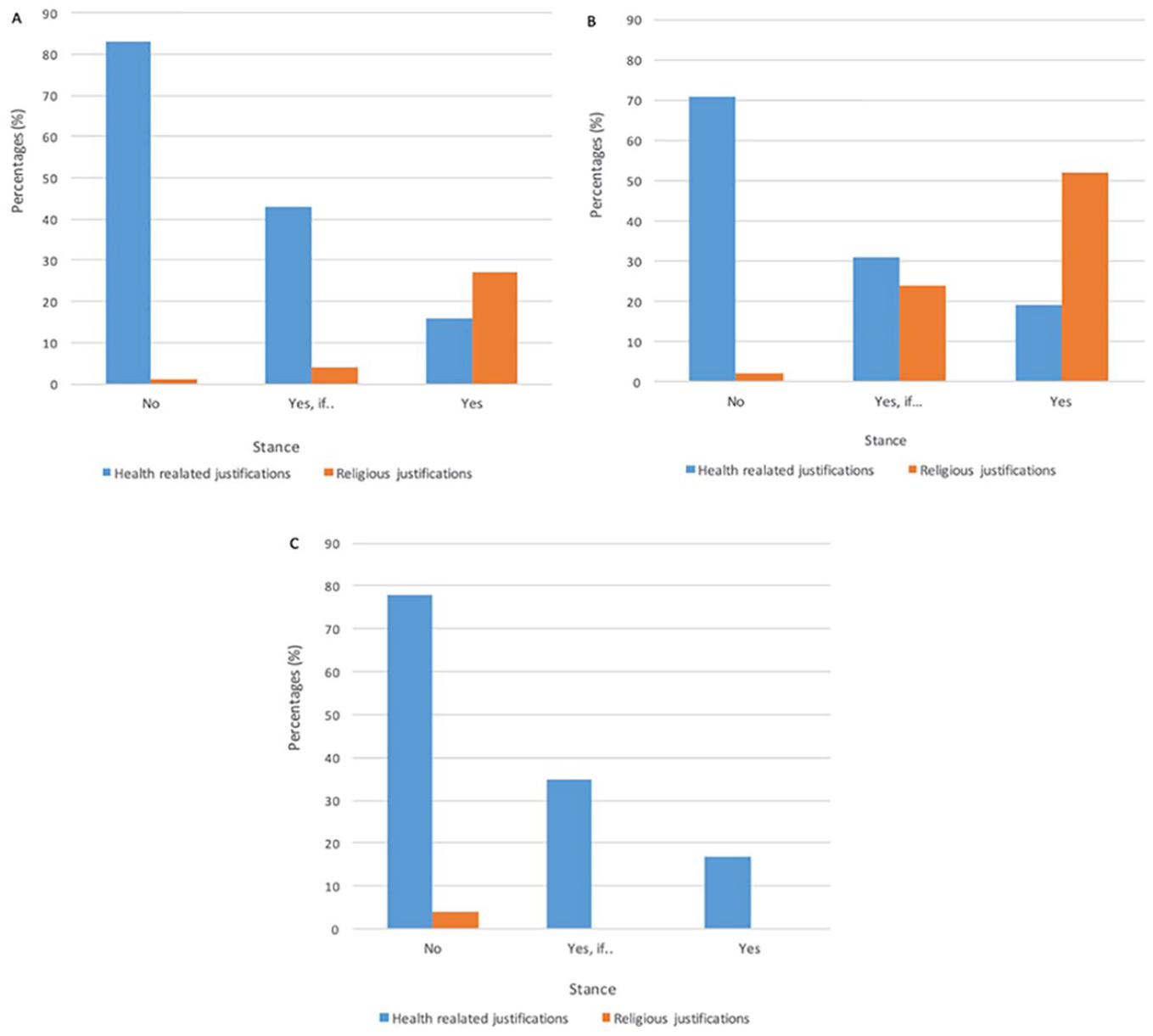
Proportion of health- and religious-themed justifications on culturally specific COVID-related dilemmas, conflicting health considerations and religious norms. (A) Passover dilemma amid social distancing: Will you still hold the Passover Seder, including with older members of the family despite COVID-19? (B) Synagogue dilemma amid social distancing: Will you be going to pray at a synagogue this Sabbath? (C) Self-isolation dilemma: Will you abide by the quarantine guidelines while your cousin is getting married?
This pattern was apparent in all three dilemmas. For the Passover dilemma, main effects of justification type, F(1, 319) = 117.77, p < .001,
For the Synagogue dilemma, main effects of justification type, F(1, 303) = 8.41, p = .004,
For the Self-isolation dilemma, main effects of justification type, F(1, 307) = 24.51, p < .001,
Compliance with health recommendations on the three personal dilemmas was also associated with choice of information sources (Figure 3). Participants who tended to comply with health regulations chose significantly more qualified academic sources (physician, website of scientific research institute, University, Ministry of Health website; r = .168, p < .05), whereas religious sources (rabbis, religious forums on the Internet) were associated with lower compliance on average (r = −.25, p < .05). Notwithstanding this trend as shown in Figures 2 and 3, both sources of “authoritative knowledge” were consulted in the participants’ COVID-19–related decisions.
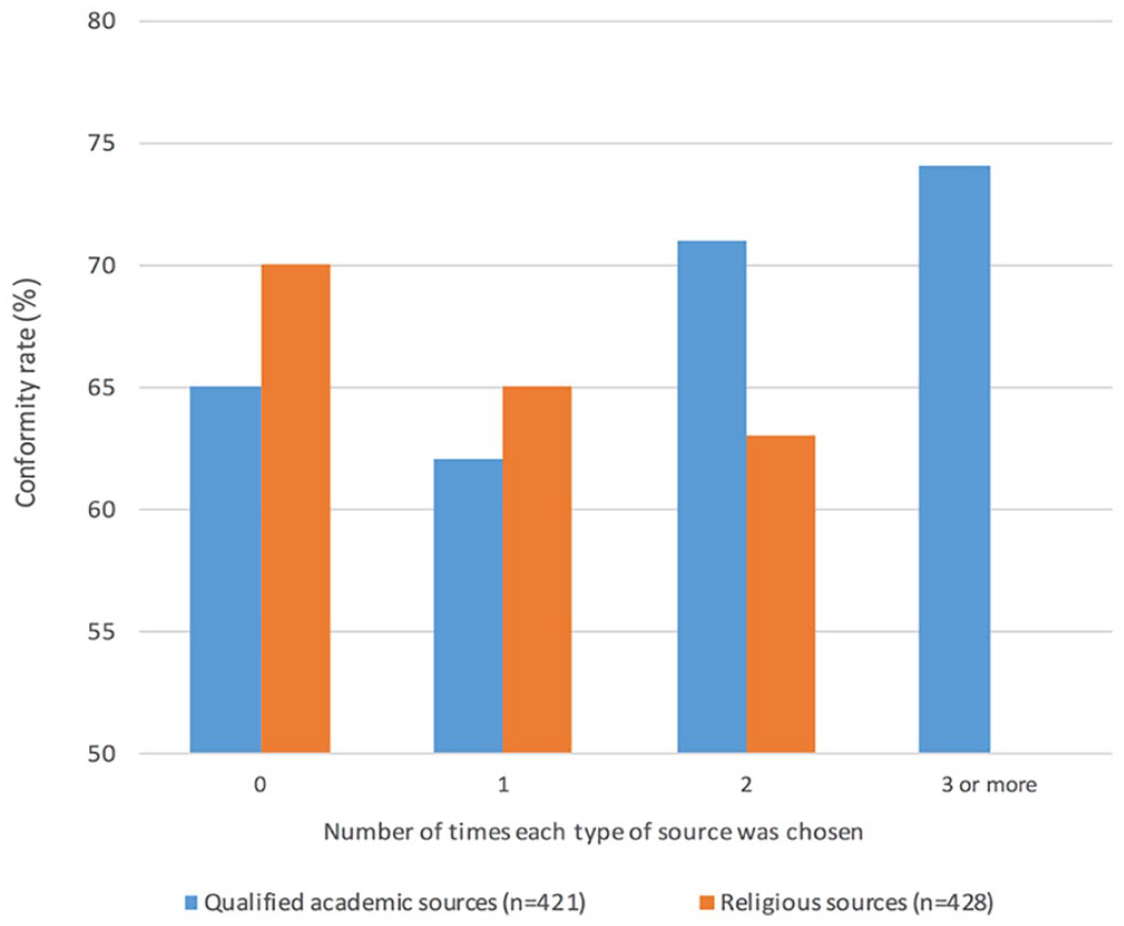
Conformity with health recommendations in personal decision making (Passover, Synagogue, and Self-isolation dilemmas) as a function of reported sources of information.
Respondents’ level of compliance was not significantly associated with age, gender, or level of education. It was weakly correlated with the (1) residential location in that—men and women residing in Haredi cities were less likely to comply with health guidelines (r = .152, p < .01); and with (2) job status contrasting men and women (compared in particular with men who only study in religious seminaries; r = .152, p < .01). In addition, level of compliance was not significantly correlated with knowledge about science or with knowledge about COVID-19. However, it was, significantly correlated with response quality (r = .257, p < .01). Response quality, in turn, was significantly, but weakly, correlated with knowledge about COVID-19 (r = .141, p < .01) and with gender in that women provided better arguments than their male counterparts (r = .154, p < .01).
Discussion
We examined the ways Haredi Jews in Israel engage and make sense of COVID-19-related issues, and their decision making in this context. No significant association was found between levels of education and level of science knowledge and levels of conformity to Ministry of Health guidelines. These echo findings on the relative marginality of science knowledge to everyday decision making (Dalyot et al., 2019; Feinstein & Meshoulam, 2014; Layton et al., 1993; Orr & Baram-Tsabari, 2018; Sharon & Baram-Tsabari, 2020). Although some people are interested in science for its own sake, many engage with science in response to situation-specific needs and tend to be interested in science only insofar as it helps them solve their problems (Feinstein et al., 2013), and when they see it as useful in light of their preexisting commitments and motivations (Feinstein, 2014).
The main findings indicated that Haredi men and women made COVID-19–related decisions that drew on both religious and health- and medical-related rationalizations. Whereas scholars have tended to perpetuate conflicts between science and religion, by examining the ways Haredi Jews engaged and learned about science in their everyday lives, we found that both systems of “authoritative knowledge” (Jordan,1997) were used together during sense-making and COVID-19-related decisions. Whereas many respondents used general health-related justifications, many expressed health-related justifications that were directly linked to religious language and culture, for example “‘You shall take care exceedingly of your lives’ (Deuteronomy 4:15)” (Tables 1 and 2). These findings may be interpreted in two ways. On the one hand, Haredi Jews may adhere to health guidelines because they resonate with religious obligations that emphasize the importance of safety. On the other hand, the use of religious language may simply be a form of expression, the particular terminology Haredi men and women use to express safety concerns. To distinguish between the two would require a qualitative follow-up study. Irrespective of explanation, however, these findings suggest that Haredi men and women have a particular vocabulary to express their justifications for following public guidelines. These findings echo Goldberg et al. (2019), who examined the use of Christian terminology in climate change communications campaigns. They found that “protecting God’s creation” was the leading term used to justify engagement in climate change, suggesting that climate change communication campaigns that use a stewardship appeal may be effective among Christian audiences, for whom this language resonates with existing Christian values.
Researchers have documented the importance of incorporating native languages into scientific communication (Manzini, 2000, Márquez & Porras, 2020). Public health guidelines have been translated into multiple languages in the United States and the United Kingdom, including Yiddish, a language spoken by some Hasidic sects of Haredi Judaism. However, the issue goes beyond translation.
A closer look at the findings suggests that the use of health versus religious justifications was more complex: Compliance with health recommendations for personal decisions (where health and religious norms conflicted) was associated with using more health-related justifications and sources of information than religious ones (Figures 2 and 3). However, there was one particularly striking dilemma in which religious justifications and language dominated: the closing of religious seminaries. When participants were asked what they thought about the Ministry of Health’s decision to close all schools, universities, and religious seminaries, most respondents agreed that the decision to close all schools and universities was correct (94.9%), but only 23.2% agreed with the decision to close religious seminaries. This points to the disparity between the ways public health guidelines are perceived in the context of general education as compared with the ways guidelines should be applied in a religious context (Figure 1).
These findings may be related to a confirmation bias or motivated reasoning, while underscoring the fact that groups can express different opinions depending on their stances with respect to the topic at hand (Kunda, 1990). This phenomenon has been documented in both large-scale survey-based studies (Drummond & Fischhoff, 2017; Kahan et al., 2012), as well as in online discourse analysis (Orr et al., 2016), and in the context of COVID-19-related sports guidelines (Baram-Tsabari et al., 2021). Here we argue that it may also signal a sociocultural gap in sense-making as well as minority pushbacks against state governance.
When the State of Israel was founded Haredi leaders introduced a new form of ultra-Orthodox piety. Unlike Jewish education system in prewar Eastern Europe where only a few gifted young men were chosen to pursue full-time Talmudic studies, all Haredi men were designed for a path of erudite seclusion from the temporal world for the purpose of instituting what Menachem Friedman called a “society of learners.” From that point on, the Lithuanian community took the position that all-male yeshivas would be the only institution capable of defending and preserving the enclave (Friedman, 1991). In the context of the pandemic, even though the comparison between schools and religious seminaries was fairly intuitive, from a Haredi perspective the government decision to close all religious seminaries was perceived as shutting down the heart of Jewish life.
Furthermore, in the Israeli context, the ideal of Torah study remains in direct conflict with “secular” ideals of citizenship. The heated debates in the Israeli parliament reflect how the Haredi religious minority is constantly critiqued for its weak education in secular topics and its exemption from compulsory military service. These divergences pose challenges to the enactment of what is perceived as constituting Israeli citizenship, religion-state relations, and ideological tug of wars in the Israeli Parliament. When the pandemic began to spread in Israel, these tensions also kindled Haredi suspicions of the “true intention” behind the decision to shut down religious seminaries. These suspicions were mirrored clearly in Rivka’s statement above: “Religious seminaries and the army are the same . . . it is a home and there is no reason to send them home. They can maintain the guidelines there!”
Our analysis also draws on recent developments in the study of medical anthropology, which have shown how health care and public health education constitute a “borderland” where religious minorities and the state negotiate each other’s positions, and tap multiple modes of governance (Kasstan, 2019). According to these anthropological critiques, public health demonstrates how particular institutions serve as part of a larger strategy of the state to govern minority groups, which in turn, provoke protective responses from different minority groups (Ecks & Sax, 2005). It is within this state-minority context that “decision-making is negotiated between multiple actors and systems of authoritative knowledge” (Taragin-Zeller, 2019a).
More inclusive communications should thus promote more culturally specific science communication by considering specific communal sensibilities, “local moral worlds” (Kleinman, 2010) and state-minority power relations (Taragin-Zeller & Kasstan, 2020). In May, as more hotspots developed in Haredi neighborhoods, the Israel Ministry of health began a culturally specific science and health section to promote science and health communication on COVID-19, which helped lower infection levels and suggests that more strategic and focused science and health communications may help improve the situation (Waitzberg et al., 2020). However, at the moment of writing (August 2020) the Israeli government decided to put 30 highly infected neighborhoods under closure, mainly Haredi and Arab, to contain the spread. This has exacerbated state-minority tensions as minority groups critique policy makers for constantly singling them out.
Conclusion
Overall, these findings argue for the need to develop better science communication models, which are aligned and resonate with local/communal understandings (Canfield et al., 2020; Goldberg et al., 2019). This article also provides detailed attention to how conventional public health messaging may (or may not) be effective when dealing with a minority population with specific cultural practices and religious beliefs. Based on our findings, we posit that science communicators must incorporate creative strategies to tailor their communications to diverse audiences. For example, translations should be provided whenever possible (Manzini, 2000; Márquez & Porras, 2020) and images should aim to represent as many minority groups as possible (Myers et al., 2019). Second, communication experts should think carefully about the particular medium used to convey messages. For example, many Ultra-Orthodox Jews, as mentioned above, do not have access to the internet, and we must think creatively how to reach them through other venues. Messaging should address and respect the particular challenges and disruptions that public health guidelines pose for minority sensibilities and lifestyles. As demonstrated in this article, the guideline that ultra-Orthodox Jews found most challenging was the closure of religious seminaries. This particular challenge (and the tension it invoked) could have been mitigated if public health messaging conveyed and demonstrated that policy makers acknowledge and understand how challenging this is for Haredi Jews culturally, religiously, and politically. The importance of tailored framing is critical as different framing helps “simplify complex issues by lending greater weight to certain considerations and arguments over others, translating why an issue might be a problem, who or what might be responsible, and what should be done” (Nisbet & Scheufele, 2009, p. 1770; cf. Hellsten & Nerlich, 2008).
Members of minority groups find it easier to follow guidelines when they are put forward by members of their own communities. Therefore, we suggest that when possible, it would be extremely beneficial to have communal representatives of minority groups promote science communications and public health guidelines (see, Wynne, 2006). Alternatively, public communicators can quote or refer to notable members of minority groups, who can serve as communal role models. Finally, it is important to acknowledge that each minority group has different needs and sensitivities, which makes it really challenging (and almost impossible) for any one individual to provide tailored information to diverse populations. To overcome this challenge, we recommend creating a network of consultants who can be called upon when necessary.
In conclusion, the case of Haredi Jews’ response to COVID-19 may serve as a vivid example of the challenges and limitations of communicating science and public health to diverse populations. Over the last 10 years the science communication literature has been pushing for more inclusive models of communication that pay attention to race, gender, and disability. We argue it is time to build another front to align science communication with local understandings of minority groups.
Supplemental Material
Questionnaire_Haredim_in_EnglishESjune28 – Supplemental material for Public Engagement With Science Among Religious Minorities: Lessons From COVID-19
Supplemental material, Questionnaire_Haredim_in_EnglishESjune28 for Public Engagement With Science Among Religious Minorities: Lessons From COVID-19 by Lea Taragin-Zeller, Yael Rozenblum and Ayelet Baram-Tsabari in Science Communication
Footnotes
Acknowledgements
We are grateful to many people for their contributions to this article. First, we want to thank all the research participants who generously shared their time and experiences with us, in midst of a global pandemic. We would also like to thank the anonymous reviewers and the Science Communication editorial team, especially Susanna Priest and Cynthia Coleman, for their support. We thank our colleagues at the Technion and especially Nadia Bordo for her expert statistical advice, and Lea Taragin-Zeller also wishes to thank her colleagues at the Woolf Institute and the Reproductive Sociology Research Group (ReproSoc) at the University of Cambridge for their ongoing support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Israel’s Ministry of Science, Grant No. 3-15724.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.