
Abstract
Although family-centered care (FCC) has been widely studied in pediatric settings, research focusing on families of children with medical complexity is limited, especially regarding parental perspectives in the Canadian context. This study explored how mothers of children with medical complexity conceptualize FCC. A qualitative approach was employed, using semi-structured interviews for data collection. Purposive sampling was used to recruit 19 mothers of children with medical complexity (aged 0–18 years) residing in British Columbia, Canada. Five key themes emerged: (a) Meeting families where they are; (b) Understanding family roles, responsibilities, and preferences; (c) Recognizing that family needs are dynamic and require ongoing reassessment; (d) Encouraging open communication and feedback; and (e) Acknowledging that the health of the child and parents is inextricably linked. Findings provide insights to guide policy and best practices for this population, who represent some of the highest users of pediatric health care services in Canada.
Keywords
Since the deinstitutionalization movement in the 1960s, caregiving responsibilities have increasingly fallen on parents and family members to meet the needs of children with disabilities (Dunn, 2003). Yet family members and caregivers are a significant and undervalued resource in our health care system and society at large. These informal caregivers contribute approximately 5.7 billion hours each year to caregiving, but are insufficiently supported by health and social service systems (Canadian Centre for Caregiving Excellence, 2022). In response to advocacy efforts from family members to recognize their role and improve care for their children both inside and outside the home, policies and standards promoting family-centered care (FCC) were created (Kuo et al., 2012).
Despite the use of the term FCC for over four decades and its being considered the gold standard of care in pediatrics, there remains a lack of conceptual clarity regarding this term (Al-Motlaq et al., 2019). FCC has been broadly defined as “an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families” (Institute for Patient- and Family-Centered Care, 2018, para. 1). On the other hand, FCC has also been defined as an organized system of medical, education, and social services provided to families that facilitates coordinated care across systems (Perrin et al., 2007). While there is a lack of consensus regarding the definition of FCC, there is considerable agreement on key principles which include: (a) support for each member of the family; (b) communication with the child and family about treatment goals and plans; (c) ethics and shared decision-making; (d) relief of pain and other symptoms; (e) continuity of care; and (f) grief and bereavement support (Truog et al., 2006).
Our current understanding of FCC has been shaped and informed by research from both health care professionals’ and parents’ perspectives. Early studies examining views of health care professionals found that although the majority tend to agree that FCC is important, they were less supportive of increasing family participation, particularly related to administering medications, explaining procedures to the child, and accompanying them to the treatment room (Daneman et al., 2003). In contrast to these findings, more recent studies assessing the perspective of health care professionals have emphasized the importance of collaboration and partnership with parents and family members (Heidari & Mardani-Hamooleh, 2020; Wong et al., 2023).
Family nursing has been recognized as playing a pivotal role in the implementation of FCC by addressing the needs of the entire family unit and ensuring their active participation in decision-making (Bell, 2013). However, while formal policies and standards for FCC have been established, the personal beliefs and practices of health care providers remain a critical factor influencing whether and how FCC is realized in practice (Bell, 2014). For example, the literature indicates that despite some consensus among health care providers in their theoretical understanding of FCC, there is disagreement in regards to its application in practice. A qualitative study by Richards et al. (2018) comprised of 22 physicians from neonatal, pediatric, and cardiothoracic intensive care units illustrated challenges to implementing FCC related to shared decision-making and balancing child and family interests. Similarly, a study by Franck et al. (2022) identified a range of issues that both support and impede delivery of FCC, specifically highlighting the need for increased nursing staffing, interdisciplinary expertise, and translators with an informed understanding of disability experiences.
There appears to be less empirical research exploring the perspectives of parents in this area. In one exception, Byczkowski et al. (2016) examined dimensions of FCC that were important to parents in pediatric care. Focus groups comprised of 68 parents revealed eight dimensions of FCC, including emotional support, coordination, eliciting and respecting preferences, timely and attentive care, information, pain management, a safe and child-focused environment, and continuity and transition. Another qualitative study by Terp et al. (2021) examined perspectives of parents regarding FCC in the Pediatric Intensive Care Unit. Findings indicated that although parents generally expressed satisfaction with the care provided during their child’s hospitalization, they perceived a need for greater partnership and collaboration with health care providers. Specifically, parents prioritized being involved in decision-making regarding their child’s care and treatment, and improving communication by focusing on the individual needs and preferences of both the child and the parents. Together, these studies make important contributions by including the perspectives of families. However, unlike emergency care or intensive care units that typically provide acute or short-term interventions, children with medical complexity require ongoing and coordinated care over an extended period.
Research on FCC for parents of children with medical complexity is extremely sparse. One exception is a study by Houlihan et al. (2024), which conducted focus groups across ten U.S. states to understand how parents of children with medical complexity experience health care systems. Parents perceived the meaning of FCC as recognizing their child’s unique strengths and needs, fostering trusting and compassionate relationships with providers, and involving families as equal partners in decision-making. In addition, parents emphasized the importance of emotional support, provider-facilitated peer connections, and creative, coordinated supports that promote both the child’s and family’s well-being. Another qualitative study by Dewan et al. (2024) comprised interviews with 16 parents of children with medical complexity, and found that trust between families and providers was fostered through family-centered practices such as timely interventions, emotional support, honest communication, clear role definition, and responsive crisis management. While this research highlights key elements of FCC, further studies are needed to validate these findings.
The definition and practice of FCC may need to be tailored specifically for families of children with medical complexity. These children often require care across multiple domains, including medical, developmental, social, and psychological aspects (Kuo et al., 2018). Focusing on the perspectives of mothers allows researchers to understand the comprehensive needs of both the child and the family unit. Their perspectives, knowledge, and experiences are invaluable in understanding the impact of the child’s condition on the family, identifying areas for improvement, and designing family-centered interventions. Mothers of children with medical complexity may also have different expectations and perceptions of FCC for a number of reasons. They likely have more frequent interactions with the health care system, greater expertise and knowledge of their children’s complex condition(s), and a higher need for care coordination across the continuum of care (Adams et al., 2019; Canadian Institute for Health Information [CIHI], 2020; Rennick et al., 2019). These factors may shape their perceptions and experiences of FCC.
While there is a breadth of research examining FCC in the pediatric setting, only a handful of studies have explored this topic in families of children with medical complexity. Even fewer studies have explored the perspectives of mothers regarding their perceptions of FCC in the Canadian context. To address these gaps, this study sought to explore the perspectives of mothers of children with medical complexity, providing care at home, on the meaning of FCC.
Method
Study Design
This study was guided by interpretive description, a pragmatic methodology used to provide practical guidance for policy and practice (Thorne, 2016). In the context of qualitative research for applied clinical practice, interpretive description is particularly valuable as it helps researchers identify patterns and themes in subjective responses. This facilitates the exploration of complex experiential questions while yielding practical outcomes that inform clinical understanding (Thorne et al., 2004). Often, research utilizing interpretive description involves integrating a variety of data collection methods to present a comprehensive account of participants’ lived experience. Outcomes of this approach yield valuable insights that can inform both policy and practice. This approach was most suitable for this study as it allowed for an exploration of participants’ understanding of FCC. Ethical approval for the research was obtained from the University of British Columbia’s Behavioural Research Ethics Board (certificate H20-02158).
Setting
The study took place in British Columbia (BC), Canada, a province with a population of approximately 1 million children, providing a unique context for exploring health care and FCC dynamics (Government of BC, 2024). According to a 2015 to 2016 report, there are approximately 802 children with medical complexity per 100,000 in BC (CIHI, 2020). The province has a single tertiary pediatric hospital situated in Vancouver, located in the southwestern corner of the province, serving as the hub for most outpatient medical specialties. In 2018, BC Children’s Hospital provided services to approximately 7,800 children with medical complexity (Government of BC, 2023). Twenty percent of these families resided outside of the Metro Vancouver area, requiring them to travel to this hospital to access the highly specialized services required for their child. This study focused on the experiences of families providing care for their children with medical complexity at home.
Participants and Recruitment
A purposive sample was recruited through a number of strategies. First, we recruited from the sample pool of a cross-sectional survey conducted with families of children with medical complexity in the Summer of 2020 (Baumbusch et al., 2022), which assessed the impact of public health measures and access to services for this population. Recruitment for the survey was conducted through social media networks, including a private Facebook group dedicated to families of children with medical complexity and traditional print media. Survey participants submitted their responses through an online survey platform of the host institution and were able to indicate their willingness to engage in future qualitative research. To ensure a diverse sample, characteristics of survey respondents were examined based on sociodemographic responses to identify groups that are often underrepresented in this population, such as individuals residing in rural/remote areas, non-white individuals, and men, and individualized invitations were sent. Second, we posted recruitment materials in the private Facebook group again in the Summer of 2022 to capture families who may not have participated in the survey.
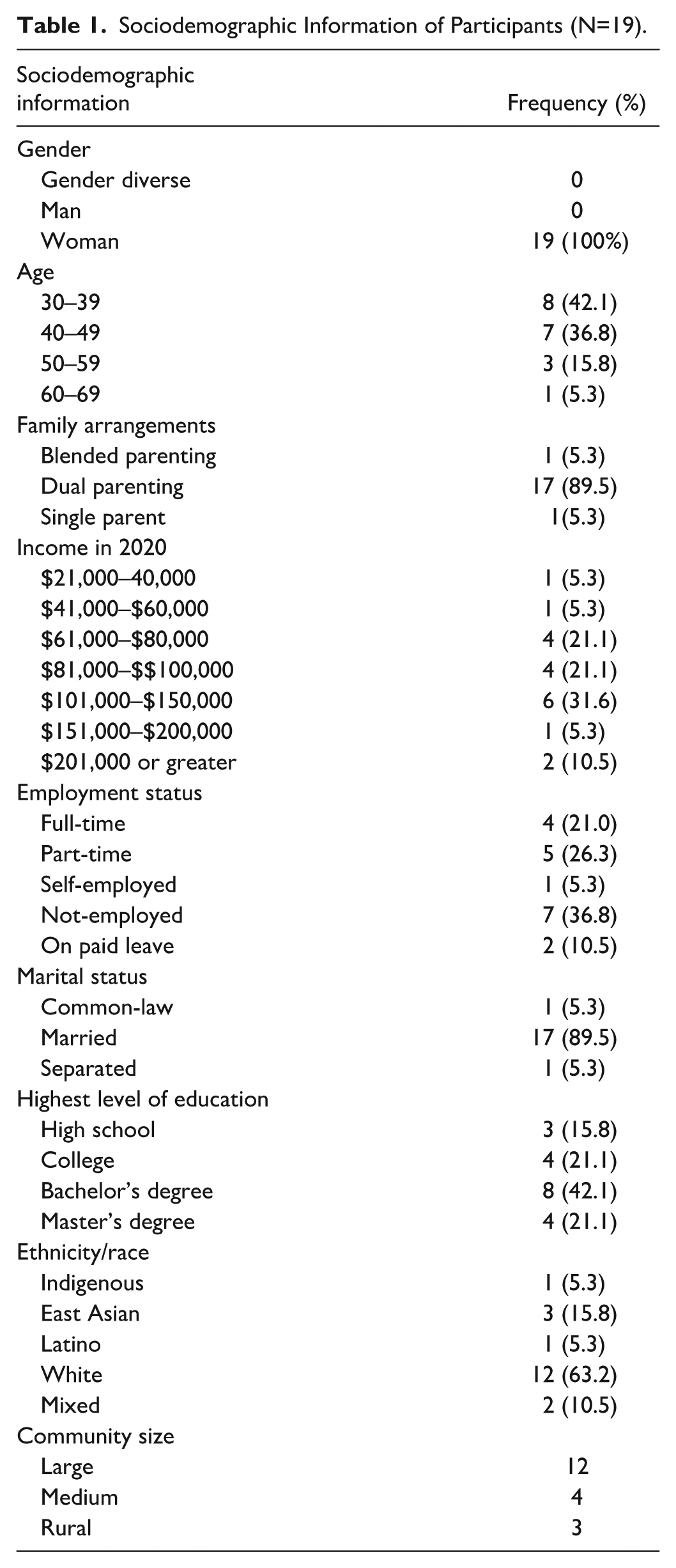
Potential participants were screened prior to enrollment in the qualitative portion of the study to ensure they met the inclusion criteria. The total sample included 19 mothers of children with medical complexity. This study defined medical complexity as encompassing children and youth with a wide range of conditions who typically share four key characteristics: complex chronic conditions, functional limitations, high health care utilization, and a high need for caregiving (Berry et al., 2013; Cohen et al., 2011). The inclusion criteria specified that participants were: (a) a parent/caregiver of at least one child with medical complexity aged from birth to 18 years at the time of survey completion; (b) co-residing in the same household as the child with medical complexity; (c) living in BC, Canada; and (d) fluent in English. To facilitate their active involvement, participants were offered the opportunity to have their child care expenses covered and were also given honoraria as compensation. The confidentiality of all participants was safeguarded by using a participant code when reporting the findings. Sociodemographic information of participants (Table 1) and participants’ children with medical complexity (Table 2) is provided.
Sociodemographic Information of Participants (N=19).
Sociodemographic Information of Participants’ Children With Medical Complexity (N=19).
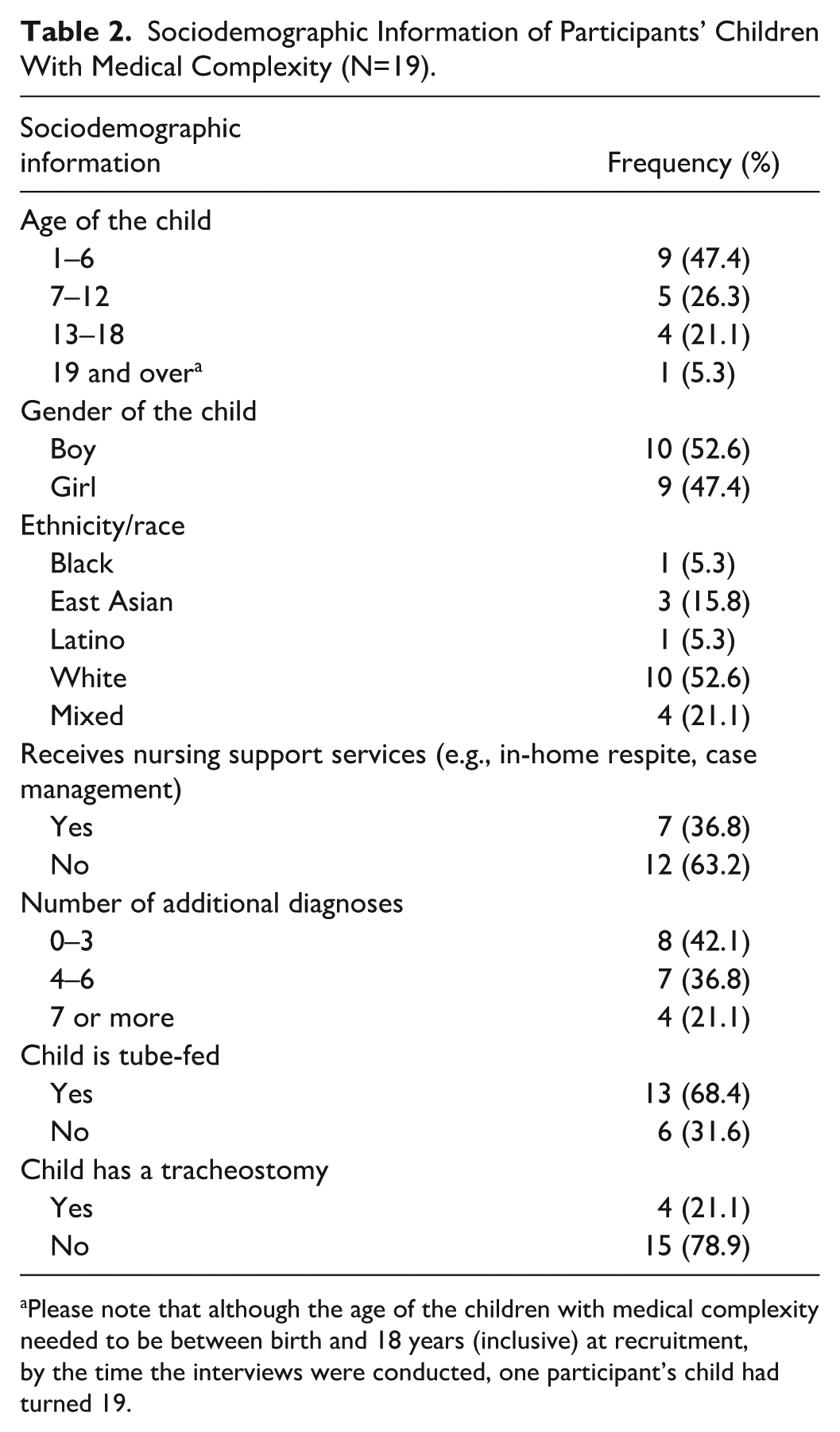
Please note that although the age of the children with medical complexity needed to be between birth and 18 years (inclusive) at recruitment, by the time the interviews were conducted, one participant’s child had turned 19.
Data Collection
From July to November 2022, virtual interviews were conducted with participants via Zoom. All interviews were conducted by VF, who is a PhD-prepared researcher with advanced qualitative research skills. Before beginning the interview, participants granted their consent for the recording of their interview sessions on video. The interview guide was collaboratively developed and adapted by researchers and community partners. These partners, identified through community connections and past research collaborations, included a pediatrician, a social worker, a leader from a nonprofit organization that supports families of people with disabilities, and parents of children with medical complexity. Their input and feedback helped ensure the interview guide accurately reflected families’ lived experience. The interviews had varying durations, ranging from 27 to 60 minutes, with an average length of approximately 45 minutes. The interviews covered various topics, including caregiver experiences in accessing services and support, such as medical services and allied health therapies. In addition, participants shared their perceptions of FCC by answering the interview question, “What does FCC mean to you and your family?” Sociodemographic data, such as family income and race, were also collected to describe the study cohort.
Data Analysis
Each interview was transcribed verbatim, and identifying information was removed. After that, the transcript was uploaded to NVivo 12, a data analysis software facilitating qualitative data management, organization, coding, and analysis. In an iterative process involving three team members (VF, JB, and KK), the codebook was developed. Initially, one team member (KK) reviewed a subset of three transcripts and identified initial codes, which were then reviewed and confirmed by the other two authors (VF, JB). Through consensus building, codes were added, revised, and finalized once it was established that no new codes were being identified, and team members applied them consistently. As the analysis progressed, codes were collated to capture emerging themes and patterns, providing meaningful insights into mothers’ experiences and perspectives. The analysis and interpretation of the data were shared with all co-authors to ensure their input and feedback were integrated.
To enhance the study’s trustworthiness, we utilized Lincoln and Guba’s (1985) criteria to assess and ensure credibility, dependability, and transferability. For credibility, we ensured our understanding of participants’ responses by confirming and comparing their responses across interviews. To address dependability, we collected raw data, maintained memos, and documented the iterative development of the codebook. Regarding transferability, we generated thick data through in-depth interviews, and in the Findings section, we present direct quotes to demonstrate the richness and depth of the information obtained.
Findings
Five themes capturing conceptualizations of FCC were identified, including: (a) Meeting families where they are, providing choices, and engaging them in decision-making to ensure care aligns with their needs and values; (b) Delivering meaningful support by understanding family roles, responsibilities, and preferences; (c) Recognizing that family needs are dynamic, evolving over time, and require continuous reassessment; (d) Building a responsive care network by assessing family readiness and capacity while encouraging open communication and feedback; and (e) Acknowledging that the health of the child and parents are inextricably linked, making family psychosocial screening and psychoeducation essential to providing holistic care. These themes were perceived as significant elements of FCC for families of children with medical complexity. Mothers emphasized the importance of informed decision-making and having a variety of options and choices when it comes to treatment and therapy options for their child. Mothers expressed the need for professionals to understand family dynamics and preferences to tailor care plans that align with their daily routines and values. Families highlighted the evolving and dynamic nature of their needs and appreciated when professionals re-evaluate and adapt care plans over time. Mothers viewed FCC as a collaborative effort, where shared responsibility between health care providers and caregivers led to the best outcomes for the child and family. Finally, families sought compassionate and holistic care that addressed not only their child’s physical health needs but also the emotional and mental health needs of the entire family unit.
Theme 1: Meeting Families Where They Are, Providing Choices, and Engaging Them in Decision-Making to Ensure Care Aligns With Their Needs and Values
Mothers consistently highlighted the importance of engaging parents and families in all stages of decision-making. This entailed more than just sharing information, but also presenting them with a range of choices and options, including the pros and cons, to assist them in making informed decisions. For example, one mother shared:
[Family-centered care] means consulting with families about policies, decisions, and programs that impact them. Parents need choice and to be involved on every level. Family engagement should be included, we should be at the table where those decisions are being made. And only then will you know what families need. (P07, 38-year-old mother)
Mothers reflected on their family’s journey and navigating the medical system over the years. These parents often emphasized the need for professionals to acknowledge the initial shock, unfamiliarity, and unpreparedness many families experience, especially at the beginning, and tailor information in ways that address this. One mother explained:
It’s very rare to find a family that has experience in the medical system before they become a caregiver. We’re not talking about family-centered care when the family doesn’t even know what’s going on or doesn’t understand even though they are the caregiver and case manager for that child. (P08, 40-year-old mother)
Theme 2: Delivering Meaningful Support by Understanding Family Roles, Responsibilities, and Preferences
The need for professionals to consider the unique characteristics of the family, such as their culture, number of children in the household, housing, language, and access to child care, was frequently mentioned by mothers. Understanding the family’s strengths and weaknesses, including where there are gaps and supports needed, and providing resources to address their specific situation were perceived as critical for delivering FCC. To illustrate this, one mother was quoted as saying:
It means taking our whole family into account and looking at the whole picture of what our family is. We have a newborn baby, a little sister, my husband works. So when people ask things of me in therapy appointments I have a lot going on and absolutely no support. I don’t have childcare. It means asking if something is doable for our family or what other people can do to support us to make it easier, to make it work. (P02, 37-year-old mother)
Furthermore, apart from taking into account family characteristics and dynamics, another mother emphasized the significance of recognizing the expertise of caregivers and encouraging their input and involvement in discussions regarding their child’s care. Gaining insight into a family’s day-to-day life, preferences, and individual circumstances can help optimize the quality of care provided in the home. For example, one mother articulated:
[Family-centered care] is including everybody in the discussion. It’s thinking about a family’s specific circumstance. Our daughter is non-verbal so we are her ears, her heart, her everything. So relying on the people that care for her in a full-time environment is what I think of when I think of family-centered. It is also including the dynamics and the circumstances within the family unit, so that we can operate as best as possible under a unique set of circumstances. (P03, 48-year-old mother)
Theme 3: Recognizing That Family Needs Are Dynamic, Evolving Over Time, and Require Continuous Reassessment
Mothers frequently addressed the common misconception that families’ needs are static in nature. Rather, they highlighted the fact that family needs are dynamic, change over time, and even fluctuate across different seasons. For example, during the winter months, children with medical complexity may be particularly vulnerable to illnesses such as Respiratory Syncytial Virus (RSV). One mother shared:
To improve services, you have to look at where families are at—which changes. What we needed four years ago is different than what we need today. Families should be able to dictate how [nursing] hours are used and where hours are used. It involves actually centering the family and asking what supports they need in this season and how can we fill in the gaps. Our financial situation has changed over time. My son’s ability to take care of himself has changed. (P04, 33-year-old mother)
The need for consistent and ongoing evaluation of family needs over time was also apparent when mothers described how accumulating out-of-pocket costs for therapies, medications, and equipment impacted their capacity to support their child at home. Furthermore, mothers also shared how their child’s physical, emotional, and psychological needs changed over time, directly impacting the services and supports they require. One mother explained:
I mean, her health has changed over time, our financial situation has changed over time, and my son’s ability to take care of himself has changed. He was three when he came home from the hospital and he’s 10 now. So there feels less of a need to be doing all the little details for him. Um, so yeah everybody’s needs have changed. (P04, 33-year-old mother)
Theme 4: Building a Responsive Care Network by Assessing Family Readiness and Capacity While Encouraging Open Communication and Feedback
Mothers voiced their frustration with professionals who had burdened the parents with overwhelming responsibility regarding their child’s care. An important distinction was made that empowering the family does not mean shifting all accountability to parents, but rather it involves assessing their readiness and capacity to provide care and offering support and resources where needed:
When they talk about family-centered care I have to correct them. Where they’re talking about empowering the mom, she is meant to do all of the nappy changes and whatever. But also, she’s traumatized and there’s a reason she’s in the ICU right now with her baby. So let’s not dump all the responsibility on a mom in the middle of this. It shouldn’t be like this expectation that it’s all on you now because you know how to do it once or whatever. (P04, 33-year-old mother)
These mothers often emphasized that FCC not only goes beyond defining the roles of the parents but also of other members of the child’s care team so that they feel adequately supported. According to these mothers, FCC involves having a network of support that is open to communication and values parent feedback and opinion:
I think family-centered care means being supported by a network and told who your network is and making sure that you’re given context for your network. [It’s] where the family is the captain of this network and all the different people who are gonna help your family have permission to talk to each other and work together to help the situation. Trusting and knowing what the family is saying and having the family guide the process. Family-centered care is a continued conversation and being asked how would you like to get this report after this appointment? Do you want it mailed to you because you’re having a problem with the e-system? The biggest part around family-centered care is not feeling rushed and being given enough time for questions. (P14, 37-year-old mother)
Theme 5: Acknowledging That the Health of the Child and Parents Are Inextricably Linked, Making Family Psychosocial Screening and Psychoeducation Essential to Providing Holistic Care
It was common for mothers to share how caregiving responsibilities and the lack of support had contributed to mental health challenges, particularly anxiety emerging from the moment of their child’s diagnosis. These mothers highlighted the need for counselors and therapists with specific training and experience in working with this population to address their worries about the future and daily challenges:
With a child who has terminal illness, it is kind of unavoidable to have mental health issues, I think. Like from the moment of diagnosis, the shock of that, too, the restructuring of how your whole life is or how you thought it would be. It just comes with a lot of anxiety, worry about the future, about a child who’s vulnerable in society and how she’ll be treated. So I really want a counsellor who kind of already knows a little bit about what it’s like to be a caregiver parent. (P07, 38-year-old mother)
While a number of mothers acknowledged various benefits of counseling and therapy, they also understood that when someone is in a state of survival, they are unable to engage in therapy or personal growth work effectively. One participant compared it to teaching swimming lessons to a drowning person without providing immediate support and rescue. In these situations, mothers need support and space for personal healing before they are able to fully engage in the therapeutic process:
Therapy itself takes work. But if you are just surviving, you can’t take that work on or take it on seriously. It’s like telling the drowning person, let’s start the swimming lessons now. That’s very helpful while you’re standing there on the shore and looking at me. But how about jumping in and supporting me because without somebody doing that, I am not gonna be learning how to swim. I first need to recover from drowning. (P05, 47-year-old mother)
Participants also highlighted the need to support the mental health of all family members, including parents and siblings. Beyond counseling and therapy, mothers emphasized the need for practicing self-care and spending quality time with the other children and their spouse to improve mental health and well-being:
[Family-centered care] means looking at the whole person and not just health and if the child is okay. It’s asking how the mental health of everybody in the family is, the Mom, Dad, siblings. We don’t necessarily need counselling five days a week or even once a week or regularly. It’s more, do I have time to shower today? Have I had one-on-one time with my other kids? Does the husband and I get dates every once and a while so our marriage is still functioning and intact? (P04, 33-year-old mother)
Discussion
This study explored maternal perspectives of what FCC means to them. Five themes capturing conceptualizations of FCC were identified, including: (a) Meeting families where they are, providing choices, and engaging them in decision-making to ensure care aligns with their needs and values; (b) Delivering meaningful support by understanding family roles, responsibilities, and preferences; (c) Recognizing that family needs are dynamic, evolving over time, and require continuous reassessment; (d) Building a responsive care network by assessing family readiness and capacity while encouraging open communication and feedback; and (e) Acknowledging that the health of the child and parents are inextricably linked, making family psychosocial screening and psychoeducation essential to providing holistic care. Similar to previous research on families in the general pediatric population (Terp et al., 2021; Truog et al., 2006), families prioritized informed decision-making and considered the needs of all family members. The current research has extended these findings by identifying these aspects as key elements of FCC in families of children with medical complexity. Mothers in this study perceived FCC to involve an open dialogue with health care providers about various options and choices that align with the family’s values and preferences. In addition, they emphasized the importance of presenting information sensitively and empathetically, taking into consideration the initial shock and unfamiliarity that comes with their child’s diagnosis.
While previous studies (Byczkowski et al., 2016; Truog et al., 2006) have identified continuity of care and follow-up as an important element of FCC, specifically after acute medical visits, our findings have demonstrated that this is particularly critical for families of children with medical complexity given the child’s health status as well as the vulnerability of the family to burnout over time. While research has acknowledged the need for a holistic approach in FCC (Pozniak et al., 2024), less focus has been on how needs evolve and change over time. Adopting a developmental perspective can shed light on the dynamic nature of family needs throughout different life stages and provide insights into tailoring support and intervention accordingly.
The finding that mothers perceived shared decision-making as a key element of FCC is strengthened by previous research (Heidari & Mardani-Hamooleh, 2020; Truog et al., 2006; Wong et al., 2023) but extends this work by examining the perspectives of caregivers. Exploring the perspectives of mothers has provided unique insights into how they envision their role as caregivers. While historically medical professionals have been viewed as experts in their child’s care (Stewart et al., 2024), the present findings indicate that mothers want to be engaged in an equal partnership with care providers. Our findings also suggest that this is facilitated by open communication that acknowledges and values parent expertise. Consistent with this, previous research by Giambra et al. (2024) found that specific communication behaviors (e.g., listening thoughtfully to caregivers, providing encouragement to ask questions, and being active participants) helped reduce caregivers’ uncertainty about the child’s condition and strengthened their ability to manage care at home. Therefore, it is recommended that pediatric complex care programs implement policies that actively seek input from caregivers regarding their health care experiences, support services, and FCC. In addition, creating transparent processes for families to raise concerns and track the resolution of issues will help drive system improvements.
The importance of emotional and mental health support when delivering FCC for this population cannot be understated. Consistent with previous research on families of children with medical complexity (Heidari & Mardani-Hamooleh, 2020; Truog et al., 2006; Wong et al., 2023), it was not uncommon for mothers in the current study to experience mental health challenges such as posttraumatic stress disorder, anxiety, and depression at some point. Parents of children with medical complexity are also particularly prone to caregiver burnout due to the long-term nature of their child’s medical needs and navigating the complexities of the health care system (Donohue et al., 2018; Lindström et al., 2010; Teicher et al., 2022). In light of these findings, health care providers should prioritize early psychosocial screening to identify caregivers at risk and provide psychoeducation to help prepare families for the emotional demands of caregiving (Knafl et al., 2017). Previous studies have suggested that health care professionals refer parents to peer support networks, where they can share experiences, access helpful resources, and build coping strategies through mutual support (McCrossin & Lach, 2023). The present findings also illuminate mothers’ desires for support in improving their mental health and overall well-being. In addition to counseling and therapy, FCC practices that offer respite to allow parents to spend quality time with each other and siblings, as well as opportunities for self-care, are vital. Ensuring flexibility in services and programs that enable family members to engage in activities beyond caregiving that enhance their mental health is essential for effective delivery of FCC and for the long-term health and well-being of children with medical complexity and their families (Sneddon, 2017).
Family nursing has a pivotal role in the implementation of FCC. Based on our findings, we have created a checklist for clinicians to consider when working with families of children with medical complexity (Figure 1).
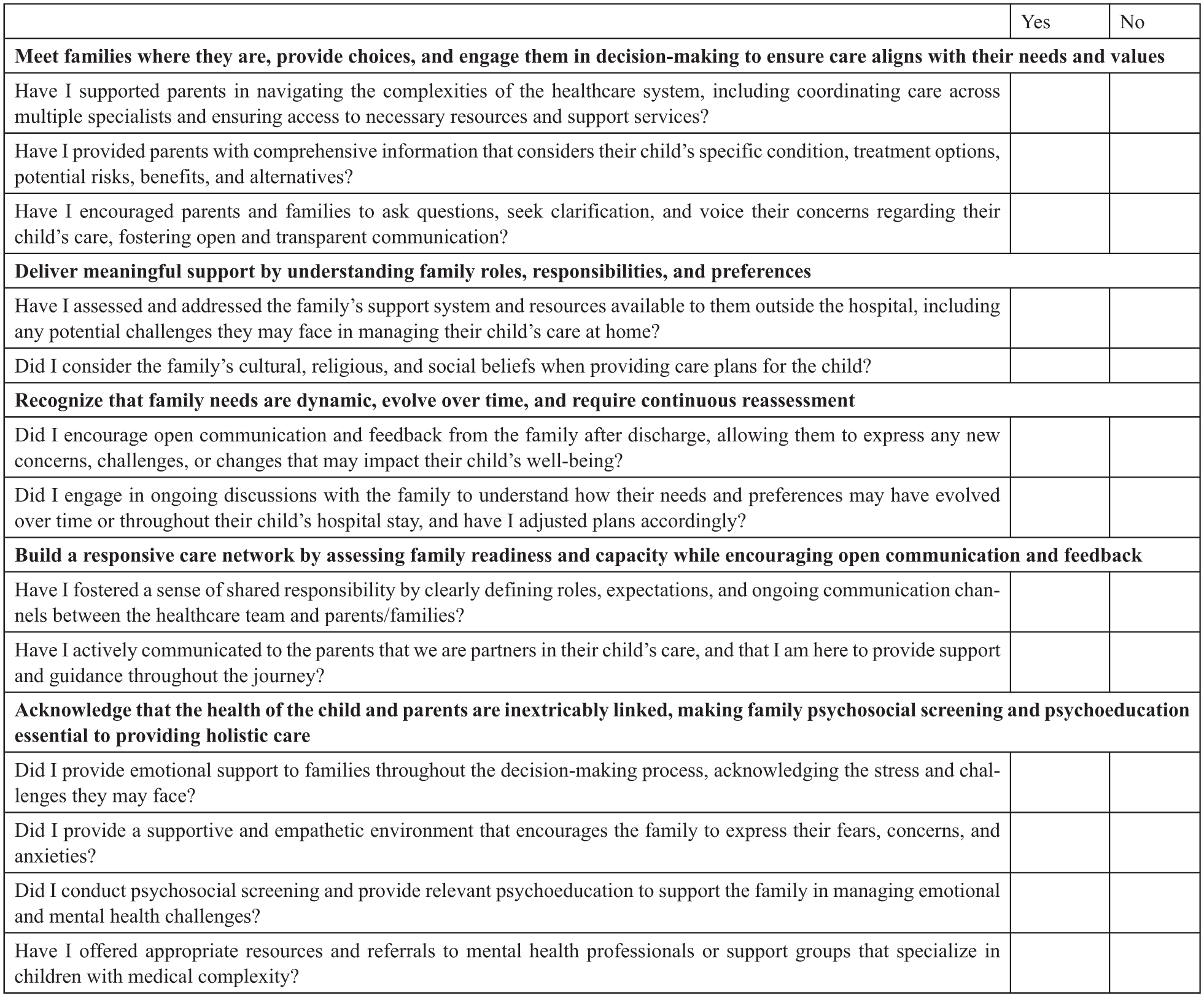
Checklist for Professions to Enhance Family-Centered Care for Children With Medical Complexity.
For each domain, we have included reflective questions. The checklist can also be used as part of team rounds or debriefing on a particular case. Nurse educators can use the checklist as part of their teaching, both with students and as part of professional development sessions, around FCC. Nurses in administrative and leadership positions have a particularly important role in ensuring that the domains of FCC with this population are embedded into policies and procedures that encourage clinicians at the point-of-care to be attentive to the areas that are valued by families.
Several limitations should be taken into consideration when interpreting the findings of our study. First, the vast majority of participants were white women who were fluent in English, reflecting a common trend in this field of research. However, future studies must make greater efforts to include diverse participants, such as men, gender diverse individuals, and those who speak minority languages other than English. Second, the cross-sectional nature of our research hinders a comprehensive understanding of the fluctuating and changing service and support needs of families of children with medical complexity. Longitudinal studies are required to gain deeper insights into these evolving needs over time. Finally, future research should aim to recruit more families from rural and remote areas, as the few participants in our study described distinct barriers, including geographic isolation, a scarcity of service providers, and prolonged wait times for essential supplies and equipment, all of which have important implications for FCC.
Conclusion
A substantial body of research exists examining perceptions of FCC among health care professionals and parents of children in the broad pediatric setting. However, the perspectives and experiences of FCC may differ for families of children with medical complexity due to parents’ intensive caregiving and frequent interactions with complex support systems. To address the lack of research in this area, the current study sought to explore conceptualizations of FCC among mothers of children with medical complexity. The following themes were perceived as significant elements of FCC: (a) Meeting families where they are, providing choices, and engaging them in decision-making to ensure care aligns with their needs and values; (b) Delivering meaningful support by understanding family roles, responsibilities, and preferences; (c) Recognizing that family needs are dynamic, evolving over time, and require continuous reassessment; (d) Building a responsive care network by assessing family readiness and capacity while encouraging open communication and feedback; and (e) Acknowledging that the health of the child and parents are inextricably linked, making family psychosocial screening and psychoeducation essential to providing holistic care. Findings contribute valuable insights to inform policy and best practice guidelines for serving the unique needs of this population, who are among the highest users of pediatric health care services in Canada.
Footnotes
Data Availability
The data supporting the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Canadian Institutes of Health Research.
Ethical Approval and Informed Consent
All procedures conducted in this study adhered to the ethical standards of the institutional research board, as well as the 1964 Helsinki Declaration and its subsequent amendments. Informed consent was obtained from all participants included in the study.
Author Biographies
![]()