
Abstract
Benefit finding is a concept that represents finding positive changes or benefits through difficult experiences. To map the currently available studies on benefit finding and growth among family caregivers of individuals with mental illness, we conducted a scoping review based on methodological frameworks. A systematic search for studies published in English was conducted using MEDLINE, PsycINFO, PsycARTICLES, CINAHL, and PTSDpubs from inception to August 2023. After screening, 21 articles were included in the review. Of these, 11 studies were cross-sectional studies, 7 were qualitative studies, 2 were mixed-methods studies, and a randomized controlled trial (RCT). Family caregivers experienced various positive psychological changes, such as becoming compassionate/tolerant and resilient, stronger family bonds, change in perspective on life and hope, acquisition of knowledge and coping strategies, and leveraging their experiences and appreciation by others, following various struggles and negative changes. Some indicators of benefit finding and growth, such as positive personal traits, positive reappraisal, good relationships with patients, and social support, were also revealed. The quality assessment demonstrated an acceptable level of quality in most studies, with a few outliers. Future longitudinal studies would reveal the mechanism of benefit finding and growth among family caregivers of individuals with mental illness.
Introduction
As one in every eight people lives with mental illness, approximately 970 million people around the world live with mental illness, placing it as one of the most significant factors causing the disease burden (WHO, 2022). With the increasing prevalence of mental illnesses, more family caregivers experience a burden. Caregiver burden can be defined as the multifaceted strain perceived by the caregiver from caring for a family member or a loved one over time (Liu et al., 2020). For family caregivers of individuals with mental illness, caregiver burden is high, as it includes not only the impact and consequences on their own mental health but also dealing with the patient’s psychiatric symptoms and behavior, in addition to changes in daily life (Cham et al., 2022). According to the work by Ntsayagae et al. (2019), they face different challenges from other caregivers of long-term conditions in that they sometimes feel strong anxiety as patients may become aggressive or have suicidal ideation. Family caregiving of individuals with mental illness may also strain family relations and other coping resources, which can be felt more acutely in situations where community rehabilitation resources are lacking and stigmatized. This results in feelings of powerlessness, higher levels of stress, lower quality of life, and lower attitudes and care for individuals with mental illness (Cham et al., 2022; Sustrami et al., 2023).
The development of positive psychology has revealed that difficult events may also serve as catalysts for positive changes. Despite the negative impacts of caregiving, many earlier studies reported that family caregivers of chronic illnesses, including cancer, stroke, and brain or spinal cord injuries, experienced positive psychological changes due to struggling with difficulties (Lin et al., 2022; Ma et al., 2023; Mei et al., 2022). Benefit finding (BF) is defined as finding positive changes or benefits through negative experiences in adversity as a cognitive adaptation process with a positive reappraisal coping strategy, including meaning-making (Lechner, 2021; Tennen & Affleck, 2002). BF reflects psychological well-being and psychological adjustment despite a stressful event, as it facilitates positive emotions and behaviors (Zhao et al., 2023).
Other related concepts include posttraumatic growth (PTG) which is defined as positive psychological changes that occur because of the struggle with a traumatic life crisis that threatens one’s safety, identity, and future (Tedeschi & Calhoun, 2004). It is accompanied by significant challenges for one’s resources, including the fundamental components of how a person understands the world, their place in it, and assumptions, such as the world’s benevolence, controllability, and predictability. PTG manifests in five domains: greater appreciation of life and changed priorities, strengthening relationships, bolstering personal strengths, openness to new possibilities, and spiritual development (Tedeschi & Calhoun, 2004).
Previous studies have pointed out some differences between BF and PTG. BF includes broader and less-specific positive changes than PTG, and does not assume the occurrence of trauma as a precondition (Applebaum et al., 2021). In addition, BF can be experienced as a positive re-evaluation of the circumstances in the shorter term, whereas BF may be experienced after a longer period of rumination and restructuring following trauma (Tedeschi & Calhoun, 2004). Despite such differences, these terms are often used almost synonymously as benefit finding and growth (BFG) in publications because they conceptually overlap, with the context of “meaning-made constructs” in the Meaning-Making Model (Liu et al., 2021). In addition, several similar concepts, such as perceived benefit and stress-related growth, are included in BFG, although the differences among these concepts are still under discussion.
Because BFG enhances psychological adaptation to adversity, it has attracted attention among health care professionals, especially nurses (Kritikos et al., 2021). However, to the best of our knowledge, there are no systematic reports on BFG in family caregivers of individuals with mental illness. It is important to explore how earlier studies on this theme have been conducted to understand how family caregivers of individuals with mental illness can experience BFG, and how it can be facilitated. Therefore, this study aimed to systematically map and summarize currently available studies on BFG among family caregivers of individuals with mental illness.
Method
This scoping review process followed the methodological frameworks of Arksey and O’Malley (2005) and a reworked one by Levac et al. (2010). It also referenced Joanna Briggs Institute (JBI) methodology for scoping reviews (Peters et al., 2020). Based on these guidelines, this study comprised five principal phases: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting of the data, and (5) collating, summarizing, and reporting the results. Unlike systematic reviews, scoping reviews do not require quality assessment of the study. Nevertheless, it is recommended, as non-assessment of quality in scoping reviews may limit the usefulness of the review findings (Abeasi et al., 2023; Shortland et al., 2024). Therefore, we incorporated this information into our review. Guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018) were used to develop and review the final protocol, which was registered prospectively with the Open Science Framework (https://osf.io) on November 20, 2023 (Registration: DOI 10.17605/OSF.IO/6XYG3).
Stage 1: Identifying the Research Question
The specific research questions addressed in the current scoping review were as follows: (a) What is currently known about BFG among family caregivers of individuals with mental illness, including its phenomenon and presence? and (b) What are the relevant factors of BFG among family caregivers of individuals with mental illness?
PCC Framework
This study used the participants, concept, and context (PCC) framework recommended by JBI methodology for scoping reviews (Peters et al., 2020) to guide the selection of relevant studies and ensure alignment with these research questions.
Participants
This review focused on studies in which the participants were family caregivers of any age. The diagnoses of mental illnesses vary, with the exception of dementia, developmental disorders, and intellectual disabilities. Family caregivers with any relationships, such as grandparents, parents, siblings, children, grandchildren, relatives, and non-blood-related families, who provided unpaid care for individuals with mental illness were included, regardless of treatment status or whether they lived together at the time of the survey.
Concept
This review targeted the concepts of BFG, that is, BF, PTG, and other similar terms that represent positive psychological changes as a result of difficulties in caregiving.
Context
To provide a comprehensive and broader understanding, the context was not restricted to any particular geographical location or publication year.
Stage 2: Identifying Relevant Studies
To adapt a broad approach that is comprehensive enough to identify applicable literature, an initial search strategy (Arksey & O’Malley, 2005), which was later refined in light of early results, was used. As the JBI guidelines also suggested (Peters et al., 2020), this first step began with a limited search of two databases to analyze text words found in the retrieved papers with a focus on the title and abstract. Keywords or index terms were also analyzed. The second step involved conducting another search using all index terms identified in Step 1. The search was performed across all the databases used in the scoping review.
Initial Search
The first author conducted an initial search of MEDLINE (Ovid) and CINAHL (EBSCOhost) to determine the text words found in the retrieved papers based on the research question. Keywords or index terms were reviewed to generate the search terms. Subsequently, a search strategy was developed in consultation with an experienced medical librarian. This started with MEDLINE (Ovid), as the subject heading definitions are well organized and developed. Medical subject headings (MeSH), and free-text keywords and phrases were developed based on synonyms and terms. The final version of MEDLINE (Ovid) was converted into each subsequent database.
Searching Across Five Databases
After an initial search with analysis of the results and revision of MEDLINE (Ovid), the final version was converted to the following five databases: APA PsycINFO (Ovid), PsycARTICLES (Ovid), CINAHL (EBSCOhost), and PTSDpubs (ProQuest). As database varies in how the subject headings are indexed, the search terms were modified according to each index term in each database. Gray literature was not searched in this study because the focus of this scoping review was to map peer-reviewed published literature that would likely influence this theme.
Stage 3: Study Screening and Selection
Based on the PCC framework, the inclusion and exclusion criteria were determined as follows.
Inclusion Criteria
Original peer-reviewed articles regarding BFG among family caregivers of individuals with a variety of mental illnesses, which were published in English in academic journals, were included. It involved qualitative, quantitative, or mixed-methods studies published from inception to August 31, 2023. We included studies that aimed to describe BFG, even if negative psychological changes were also a focus. Regarding quantitative studies, articles that used scales to assess BF, PTG, or other concepts of positive psychological changes were included.
Exclusion Criteria
Articles that mostly focused on family caregivers’ difficulties and needs rather than BFG, those that focused on the role of care provision, and participants who were bereaved families were not included. Regarding types of publication, books, handbooks, book chapters, dissertations, commentaries, letters, editorials, and proceedings were excluded. Regarding study design, reviews, systematic reviews, meta-analyses, and study protocols were also excluded.
Study Selection
Search results from each database were imported into EndNote (Clarivate Analytics), a reference management software where duplications were removed and citations were managed in the succeeding screening. After removing duplicates, the articles were exported to Rayyan (https://www.rayyan.ai), a review management system for screening articles.
The results of an initial pilot test of the independent screening of titles and abstracts were used to iteratively revise and finalize the screening criteria. After confirming the consistency of screening, a first-round screening of titles and abstracts was independently conducted by pairs of reviewers. Any differences between the two reviewers regarding eligibility for full-text review were resolved by a third reviewer. Subsequently, full-text screening of all potentially eligible papers was conducted as a second-round screening by paired independent reviewers; any differences regarding whether the paper should be included in the analysis were discussed and determined by the research team. As recommended in the work by Levac et al. (2010), all authors were involved in the process of decisions regarding the inclusion/exclusion of articles. The reasons for excluding papers in the full-text review stage were documented and reported in a PRISMA-ScR flow diagram (Figure 1).
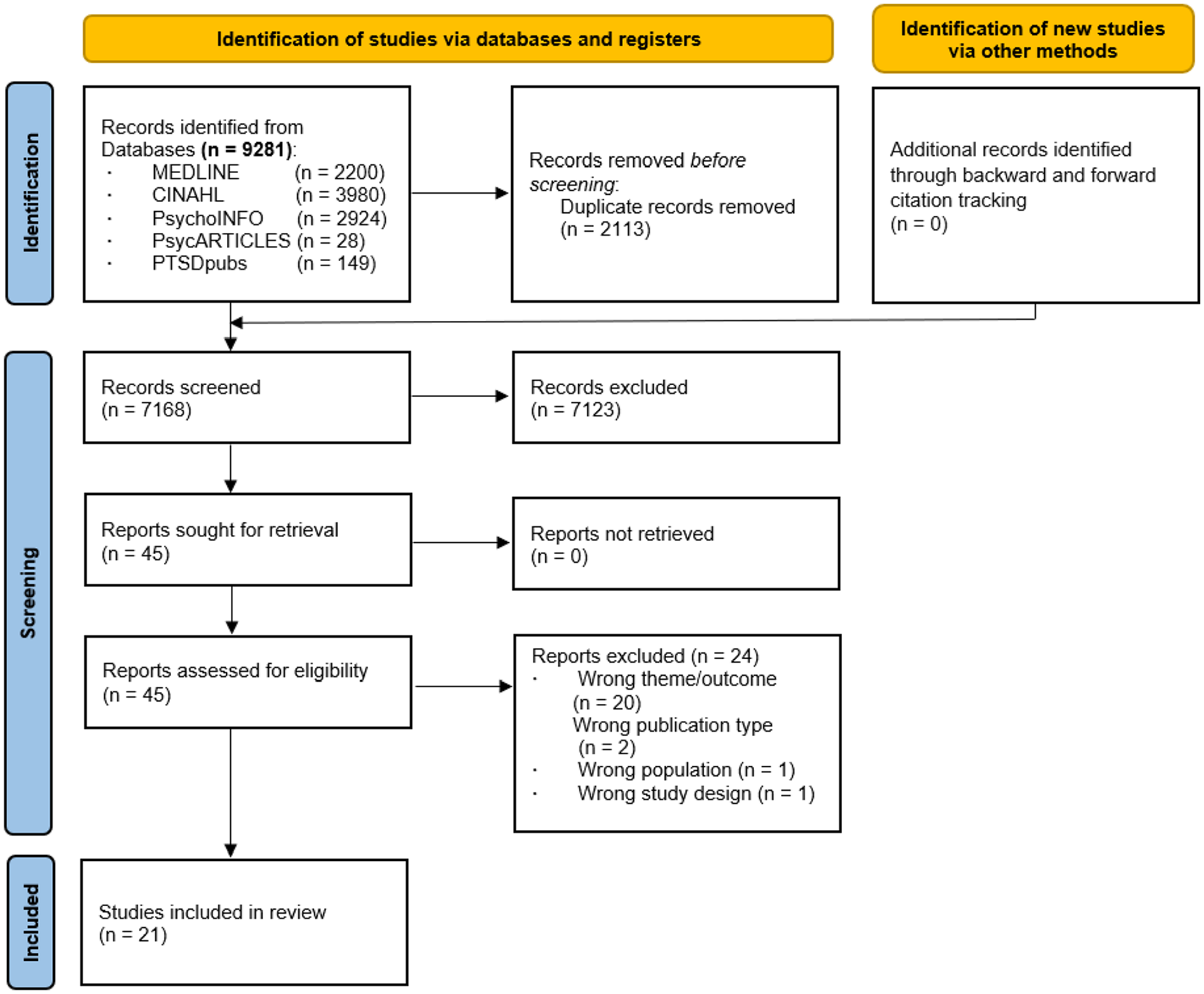
PRISMA Flow Diagram in This Study.
Finally, forward and backward citation tracking was completed to prevent the possibility of excluding the articles concerned as much as possible. Forward citation tracking was performed on all included studies using Web of Science. Backward citation tracking, which involves searching the reference lists of all included studies, was implemented for possible additional articles.
Stage 4: Charting the Data
The data charting process was guided by the methodological frameworks of Arksey and O’Malley (2005) and Levac et al. (2010), and by the JBI methodology for scoping reviews (Peters et al., 2020). It also complied with the recommendations of PRISMA-ScR (Tricco et al., 2018). A data charting form using Microsoft Excel for the extracted information from the included articles was developed by the first author. After a pilot test, the authors agreed on the key elements to be extracted in this scoping review and confirmed that the approach to data extraction was consistent with the research questions and aims of this study.
The following information was collected from the selected studies: title, authors, year of publication, journal, country where the study was conducted, aim of the study, study design, lived experience involvement of family caregivers, sample size, demographic information of family caregivers (gender, age, relationships with individuals with mental illness, education, financial status, employment status/school attendance, caregivers’ own psychological condition, and cohabitation), duration of mental illness and experience of hospitalization of the patients, method of assessing BFG, analysis, and main findings. Two data collection records for each article were compared, and the final decision was made through discussion in the research team.
Stage 5: Collating, Summarizing, and Reporting the Results
As synthesis approaches such as thematic synthesis to reinterpret qualitative evidence are not consistent with the intention and process of scoping reviews, to go beyond basic descriptive analysis is not recommended (Munn et al., 2018; Pollock et al., 2021). In line with this recommendation, we summarized and collated the identified preliminary themes and findings in each study to map the available evidence and existing knowledge gaps.
Quality assessment forms were used to extract relevant data for appraisal. CASP Qualitative Studies Checklist (Critical Appraisal Skills Programme, 2018), Checklist for Analytical Cross-Sectional Studies by JBI (2020), Mixed-Methods Appraisal Tool (Hong et al., 2019), and CASP RCT Checklist (Critical Appraisal Skills Programme, 2018) were used for qualitative studies, cross-sectional studies, mixed-methods studies, and RCT, respectively. After assessment by pairs of independent reviewers, any discrepancies in the quality assessment were discussed to reach a consensus. No studies were excluded because of lower appraisal because such studies can still have useful and informative data.
Results
A literature search yielded 7,168 peer-reviewed articles after removing duplicates. The initial screening involved reading titles and abstracts, which identified 45 articles that potentially met the eligibility criteria. Among them, 21 peer-reviewed articles met the eligibility criteria.
Characteristics and Methodology of the Studies
These 21 articles were published between 2002 and 2023 in various journals related to psychiatry, mental health, psychology, nursing, health care, and social science. The terms used for identifying BFG included BF, growth, personal development, positive appraisal, PTG, rewards, stress-related growth, stress-related personal growth, and traumatic growth (Table 1). The studies were performed in various countries, with the majority from the United States (n = 5), Australia (n = 4), and Turkey (n = 4). In all articles, there were no studies that elaborated the Patient and Public Involvement (PPI) procedure in designing the study, acquisition of the data, or interpretation of the results. However, there were a few studies in which one of the authors had a family member who had experienced mental illness (Klages et al., 2020; Reynolds et al., 2022), and which held focus group discussions among caregivers, mental health professionals, and grassroots separately from interview to provide an in-depth understanding of the lived experiences of caregivers (Dijkxhoorn et al., 2022).
Summary of Study Characteristics and Key Findings.

Note. PTG = posttraumatic growth; PTGI = Posttraumatic Growth Inventory; SRGS = stress-related growth scale.
Of the 21 articles identified, 6 were qualitative studies describing the experiences of psychological changes related to BFG, in family caregivers of individuals with mental illness. Another qualitative study was conducted to explore the experiences of family caregivers through a specific intervention. Two studies with a mixed-methods design mainly focused on the qualitative analysis of the caregivers’ BFG experiences. The sample sizes of the qualitative and mixed methods studies ranged from 7 to 60 participants. These studies conducted interviews with family caregivers to explore comprehensive psychological changes, including the BFG processes and negative changes.
Among the 12 quantitative studies, in addition to an RCT, we found 11 observational studies with a cross-sectional design, with main analyses of t-test (n = 2), correlation analysis including regression analysis (n = 7), and mediation analysis (n = 2). In all quantitative studies (n = 12), the Posttraumatic Growth Inventory (PTGI; n = 7), 15-item Stress-Related Growth Scale (SRGS; n = 4), and Experiences of Caregiving Inventory (n = 1) were used to assess caregivers’ BFG. Notably, 11 quantitative studies assessed BFG as concepts of PTG or stress-related growth using scales that only asked about positive changes. The remaining study, which used the Experiences of Caregiving Inventory, asked about changes in both positive and negative manners (Toohey et al., 2016). The sample sizes ranged from 52 to 666 in the 12 quantitative studies.
Characteristics of the Participants and Patients in the Studies
The age of the family caregivers ranged from 16 to 85 years. Regarding information on family caregivers, 13, 9, 8, 7, and 13 out of 21 studies described the level of education, employment status/school attendance, financial status of family caregivers, caregivers’ psychological condition, and cohabitation with individuals with mental illness, respectively. Among 21 studies, the proportion of working caregivers ranged from 25% to 100%. The proportion of caregivers who lived with patients at the time of the survey varied across studies. For illness-related information of the patients, 5 and 6 out of 21 studies described the duration of mental illness and whether they had ever hospitalized or not, respectively. These 6 studies showed that most patients had experience of hospitalization.
Struggling in Life Which Lead to BFG Among Family Caregivers
Qualitative and mixed-methods studies revealed that family caregivers of individuals with mental illness experienced negative changes, such as perceived stigma and a sense of isolation (Dijkxhoorn et al., 2022; Reynolds et al., 2022; Tranvåg & Kristoffersen. 2008; Veltman et al., 2002), caregiving burden, and the loss of opportunities (Bauer et al., 2012; Dijkxhoorn et al., 2022; Reynolds et al., 2022; Sin et al., 2008; Tranvåg & Kristoffersen. 2008; Veltman et al., 2002), family dysfunction (McCormack et al., 2017; Sin et al., 2008), health problems (Bauer et al., 2012; Sin et al., 2008; Tranvåg & Kristoffersen. 2008), concerns about system issues including lack of care and information (Klages et al., 2020; Tranvåg & Kristoffersen. 2008; Veltman et al., 2002), in addition to other negative feelings and emotions. However, through the process of coping with such difficulties, they eventually found growth or positive gains.
Aspects of BFG Among Family Caregivers
Qualitative and quantitative studies identified aspects of BFG among family caregivers: becoming compassionate, tolerant, and resilient (Bauer et al., 2012, 2013; Dijkxhoorn et al., 2022; McCormack et al., 2017; Reynolds et al., 2022; Sin et al., 2008; Veltman et al., 2002), stronger family bonds (Bauer et al., 2013; Reynolds et al., 2022; Sin et al., 2008; Veltman et al., 2002), change in life perspective (Bauer et al., 2013; Veltman et al., 2002) and new hope for living together with patient (McCormack et al., 2017; Tranvåg & Kristoffersen, 2008), acquisition of knowledge and coping strategies (Bauer et al., 2013; Veltman et al., 2002), agents for change for improvements in mental health care, and appreciation by others for their caregiving (Bauer et al., 2013; Klages et al., 2020).
Indicators of BFG Among Family Caregivers
Indicators of BFG were revealed as follows: optimism (Balaban et al., 2017; Mackay & Pakenham, 2011), extraversion and openness (Balaban et al., 2017; Morton et al., 2014), conscientiousness (Balaban et al., 2017), religiousness (Balaban et al., 2017; Morton et al., 2014; Özates et al., 2022), coping (Balaban et al., 2017; Morton et al., 2014; Toohey et al., 2016; Wu et al., 2021), appraisal, positive reframing and meaning-making (Abraham & Stein, 2015; Mackay & Pakenham, 2011; Morton et al., 2014), resilience (Ergün et al., 2018; Wu et al., 2021), balanced priorities for caregiving and good relationship with patients (Gurcuoglu & Durmaz, 2022; Leith et al., 2017; Mackay & Pakenham, 2011; Sanders & Szymanski, 2012; Stein et al., 2020), lower self-care attitudes (Stein et al., 2020), and social support and support group (Balaban et al., 2017; Bauer et al., 2013; Gurcuoglu & Durmaz, 2022; Leith et al., 2017; Morton et al., 2014; Özates et al., 2022; Wu et al., 2021). Higher education (Gurcuoglu & Durmaz, 2022) and absence of patients’ substance abuse (Abraham & Stein, 2015) were also identified as indicators of BFG. No consistent results in quantitative studies have been found regarding the association between psychological distress and BFG (Gurcuoglu & Durmaz, 2022; Özates et al., 2022).
Quality Assessment of the Studies
CASP Qualitative Studies Checklist (Critical Appraisal Skills Programme, 2018) showed the number of “Yes” grades in 10 items ranged from 6 to 9 in seven qualitative studies. All studies failed to declare that the relationship between the researcher and participants was adequately considered. Out of 11 cross-sectional studies, 9 studies showed five or more “Yes” grades in eight items of Checklist for Analytical Cross-Sectional Studies by JBI (2020), though there were two outliers which included only two or three “Yes.” Two mixed studies had 10 or 11 “Yes” grades out of 17 items of Mixed-Methods Appraisal Tool (Hong et al., 2019), whereas an RCT study showed 6/11 “Yes” in the CASP RCT Checklist (Critical Appraisal Skills Programme, 2018).
Discussion
In this scoping review, 21 studies described BFG among family caregivers of individuals with mental illness. They experienced various positive psychological changes, such as becoming compassionate and resilient, stronger family bonds, changes in life perspective and new hope, acquisition of knowledge and coping strategies, agents for change for improvements in mental health care, and appreciation by others for their caregiving. Some indicators of BFG, such as positive personal traits, positive reappraisal, good relationships with patients, and social support, were also revealed.
Most aspects of BFG revealed in this study, such as becoming compassionate, tolerant, and resilient; stronger family bonds; and changes in perspectives on life and hope, were similar to those in other studies of family caregivers of individuals with physical illnesses, including amyotrophic lateral sclerosis, stroke, type 1 diabetes, and cancer (Kennedy et al., 2022; Mei et al., 2020; Pierce et al., 2019; Song et al., 2024). This suggests that these changes are prevalent regardless of the type of care provided or the challenges unique to the illness characteristics that families experience. Future research should explore how these dominant elements of BFG eventually lead to quality of life and well-being among family caregivers of individuals with mental illness.
However, the acquisition of knowledge referring to decreased stigma, and agents for improvements in mental health care seem to be specific features of this population, considering that mental illness is a highly stigmatized illness. Given that a previous study showed that patients with mental illness also recognized an increased understanding of mental illness as BFG (Chiba et al., 2014), it appears to be found in people who become deeply involved with mental illness, whether they are patients or caregivers. Recognizing the importance of improving mental health services, which are not necessarily adequate, and taking action will help make use of one's own experiences in society. Therefore, these BFG may substantially lead to more active participation and support for better treatment and mental health care.
Although paying attention to their own healthy lifestyles has been reported as BFG in family caregivers of individuals with life-threatening or worsening illnesses (Mei et al., 2020; Song et al., 2024), it was not dominant in family caregivers of individuals with mental illness. This shows that families caring for patients with life-threatening or worsening illnesses recognize the importance of being physically healthy and alive, while it is not necessarily common for families caring for patients with non-life-threatening mental illnesses.
Theoretically, coping, including positive reappraisal, is regarded as a part of the BFG process (Lechner, 2021). Consistent with the findings of previous empirical studies on family caregivers of patients with mental or physical illnesses (Li et al., 2023; Liu & Sun, 2024; Milios et al., 2022; Phillips et al., 2022), it was also shown to correlate with BFG in family caregivers of individuals with mental illnesses. Although some interventional studies for family caregivers of individuals with Alzheimer’s disease or physical illnesses (Cheng et al., 2019; Fu et al., 2020; McAndrew et al., 2023), and for people with mental illness (Chiba et al., 2015) have been empirically demonstrated coping can enhance BFG, future research on family caregivers of individuals with mental illness is needed to clarify how it can contribute to BFG.
The association between social support and BFG in this study was consistent with the findings of earlier studies on family caregivers of patients with developmental disorders and other mental illnesses (Brand et al., 2014; Slattery et al., 2017). Family caregivers of individuals with mental illness tend to feel isolated due to stigma and find it difficult to deal with various symptoms (Labrum & Newhill, 2021). Therefore, formal and informal social support, including various services and peer support, should be effectively provided, not only for the patients but also for family caregivers. Such social resources would contribute to balanced priorities for caregiving and good relationships with patients, as shown by the indicators of BFG in this review.
BFG is experienced as part of a sequence of changes resulting from caregiving, including negative changes and difficulties, which is in line with the findings of earlier studies on family caregivers of physically ill patients (Kennedy et al., 2022; McAndrew et al., 2023). Given that positive and negative changes can coexist (Malhotra et al., 2024), the quantitative assessment of BFG as part of a comprehensive psychological process may be a future consideration. Although most quantitative studies have assessed BFG using scales with options for only positive changes, earlier studies have suggested that assessing both positive and negative changes can be more valid, reducing response bias and psychological burden (Boals & Schuler, 2018; Chiba et al., 2020).
In this review, 11 out of 12 quantitative studies used a cross-sectional design, except for one RCT. Given that some studies did not show high quality, future longitudinal studies with rigorous designs are clearly needed to examine the causal relationships between related variables and BFG. In addition, the inclusion of lived experience perspectives in the research teams was not prevalent among the studies. Future studies may be implemented in collaboration with family caregivers, as this is a way of validating their experiences of BFG, obtaining insights into the findings, and harnessing its potential for future research.
Clinical Implications
As the International Family Nursing Association (IFNA, 2017) Position Statement on Advanced Practice Competencies for Family Nursing declared, advanced practice competencies in family nursing include facilitating awareness, supporting family strengths, and assisting them in identifying opportunities for growth and change. Since mental illness tends to require long-term care, recognizing and assessing not only negative changes but also BFG that family caregivers experience is of great significance in family nursing. This would help nurses understand family caregivers holistically, enhance family strength, and provide support to help them overcome their difficulties.
Limitations
This study has two key limitations. First, including only studies written in English and excluding non-academic or gray literature might omit relevant studies, causing important findings to be missed. Second, family caregivers were not involved in this scoping review process due to the incipient stage of the research in this field, while frameworks by Arksey and O’Malley (2005) and by Levac et al. (2010) proposed a sixth optional phase as consultation with stakeholders. Subsequent research that overcomes these limitations may bring about an even broader consolidation of research findings and deeper insights. However, despite these limitations, this study is noteworthy enough because it is the first scoping review to address BFG among family caregivers of individuals with mental illnesses, and it systematically and comprehensively mapped and summarized currently available studies.
Conclusion
In this scoping review, a total of 21 studies were identified which described BFG among family caregivers of individuals with mental illness. They experienced various positive changes, such as personal growth, change in perspective on life and hope, stronger family bonds, and acquisition of knowledge and coping strategies as BFG, following various struggles. Some indicators of BFG such as positive personal traits, positive reappraisal and coping, good relationship with patients, and social support were also revealed. Future longitudinal and interventional studies would reveal the mechanism and effective interventions of BFG among family caregivers of individuals with mental illness.
Footnotes
Acknowledgements
The authors thank Dr. Takeshi Hashimoto at Hashimoto Takeshi Clinic for contributing to the development of the protocol. They also thank Ms. Mariko Tanaka, a librarian at Medical Library at Kyoto University, for providing technical support and expertise in the development of search strategies.
Author Contributions
All authors herein listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors.
Data Availability
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (grant no. 19K11216). It was also partially supported by JSPS KAKENHI (grant nos. 23H03196, 22K10779, and 23K09929).
ORCID iDs
Author Biographies
Chiba, R., Yamazaki, Y., Miyamoto, Y., & Funakoshi, A. (2021). Related changes in personal recovery, benefit finding, and sense of coherence among people with chronic mental illness: A two-wave study. The Journal of Psychology, 155(3), 292–308. ![]()
Kotera, Y., Miyamoto, Y., Vilar-Lluch, S., Aizawa, I., Reilley, O., Miwaw, A., Murakami, M., Stergiopoulos, V., Kroon, H., Gives, K., Kenneydyrae, G., Ronaldson, A., McPhilbin, M., Jebara, T., Takhi, S., Repper, J., Meddings, S., Jepps, J., Simpson, A. J., Kellermann, V., Arakawa, N., Henderson, C., Slade, M. & Eguchi, S. (2024). Cross-cultural comparison of recovery college implementation between Japan and England: Corpus-based discourse analysis. International Journal of Mental Health and Addiction. Advance online publication. ![]()
Funakoshi, A., Miyamoto, Y., Tsuchiya, T., & Tsunoda, A. (2024). Development of the clinical competency assessment scale in child and adolescent mental health nursing. Journal of Psychiatric and Mental Health Nursing, 31(4), 583–595. ![]()
Hirota, M. Chiba, R., Aoyama, S., Hirano, Y., Ichikawa, K., Grenier, C., Fujimoto, H., Yotsumoto, K., & Hashimoto, T. (2023). Individual nurse-led active listening intervention for spouses of individuals with depression: A pre-/posttest pilot study. Journal of Psychosocial Nursing and Mental Health Services, 61(12), 19–25. ![]()
Yoshinaga, N., Thew, G. R., Hayashi, Y., Tanoue, H., Nakai, M., & Clark, D. M. (2024). Translated and culturally adapted internet-delivered cognitive therapy for social anxiety disorder in Japanese clinical settings: Study protocol for a randomized controlled trial. Trials, 25, Article 492. ![]()
Yamanouchi, T., Hiroshima, M., Takeuchi, Y., Swada, Y., Takahashi, M., & Amagai, M. (2018). Factors associated with worsened or improved mental health in the Great East Japan /earthquake survivors. Archives of Psychiatric Nursing, 31(1), 103–111. ![]()
Amagasa, T., Inagaki, A., Suzuki, W., Suzukamo, Y., Nagai, K., Sawada, K., Inadomi, H., Mukaiyachi, I., Anzai, N., Ikebuchi, E., & Niwa, S. (2024). Examining the content validity of the Comprehensive Assessment of Functioning for Mental Illness-Subjective Version (CAMI-S) with reference to the framework of the International Classification of Functioning, Disability, and Health (ICF). Psychiatry and Clinical Neurosciences Reports, 3(3), Article e232. ![]()