
Abstract
A Collaborative Online International Learning (COIL) experience was designed for prelicensure nursing students taking a pediatric course in the United States and in Brazil, to teach family-centered care to develop inclusive, global nursing practices. The purpose of this study is to describe prelicensure nursing student learning of family-centered care concepts facilitated by COIL. For data collection, six focus groups with 37 students were conducted across both universities. Data were analyzed using inductive qualitative analysis by each country separately and as a global team. Major themes included understanding the needs of families of children with chronic conditions as impacted by health systems, assigning meanings to family care of children with chronic conditions, applying concepts of family-centered care and self-reflection. Results suggest COIL is a feasible way for prelicensure nursing students to learn family-centered nursing care by operationalizing concepts, from real experiences and increasing cultural awareness.
Keywords
Background
Family-centered care is a fundamental concept in pediatric nursing, as the care of a child is embedded within a family system that influences all aspects of the child’s health. Key elements of family-centered care involve acknowledging and appreciating the strengths of family diversity, including ethnic, racial, spiritual, social, economic, educational, and geographic differences. By supporting and celebrating this diversity, we can enhance health outcomes and improve the quality of life for families (Institute for Patient- and Family-Centered Care, 2024).
Practicing family-centered nursing care is especially crucial for families whose child has a chronic condition because they face ongoing, complex challenges that significantly impact their daily lives. Certain pediatric conditions require families to make substantial efforts, adapting and integrating their lives with the health care system to facilitate early diagnosis and treatment, prevent disease progression, and mitigate adversities such as disability and death (Morton et al., 2022; Zhang et al., 2023).
Traditionally, family-centered care has been taught within prelicensure pediatric nursing courses. However, there is inconsistency in the best methods for teaching family-centered nursing concepts and limited research on the most effective educational modalities to effectively teach these concepts (Gutierrez-Aleman et al., 2021). A few educators have used standardized actors and simulation to teach undergraduate nursing students about family-centered care. For example, Zimmerman and Alfes (2019) focused on developing a pediatric simulation experience to promote learning of family-centered care, aiming to enhance baccalaureate nursing students’ understanding of the role and perspective of parents within pediatric emergency and general inpatient pediatric nursing settings. Findings from debriefing sessions and student reflections highlighted the experiential value of these simulations in engaging students and teaching family-centered care. Similarly, Fitzgerald and Ward (2019) examined baccalaureate nursing students’ performances in providing family-centered care by using standardized actors in a pediatric-focused simulation, finding this to be an engaging way to teach empathy and family-centered care. Others have recognized the need to teach family-centered care competencies to prelicensure nursing students (Domingo-Osle et al., 2023; Duarte et al., 2024). For example, Duarte et al. (2024) found using validated simulation scenarios an effective and innovative way to teach family-centered nursing care for students.
Today’s nursing students must be equipped with skills to work effectively with families from diverse cultural backgrounds. Research in family-centered nursing education that accounts for global disparities is necessary, given that the burden of chronic pediatric diseases is predominantly concentrated in countries with lower socio-demographic indices (Buckle et al., 2024; Zhao et al., 2024). Given current and future global migration patterns and the profound influence culture has on family beliefs, values, and decision-making, it is essential for educators to identify the best methods for teaching culturally responsive family-centered nursing care through a global lens (Bozkurt & Gazarian, 2024). Furthermore, when educators evaluate different teaching methods, it is crucial to consider approaches that address the complex challenges faced by children and families. Teaching methods should aim to advance health sustainability goals, such as reducing poverty and inequalities, and should prepare future nurses to be adaptable to meet the needs of culturally diverse patients (Bozkurt & Gazarian, 2024; Nkurunziza et al., 2023). Despite the need, there is a lack of research on how to effectively teach family-centered care through the lens of culturally responsive nursing, particularly when considering nurses’ work with families worldwide.
Collaborative Online International Learning (COIL), an emerging teaching modality, offers a distinctive virtual educational experience that enhances students’ cultural awareness through global perspectives. This unique model involves faculty from partnering universities co-creating, co-teaching, and co-evaluating learning activities. Students collaborate in a highly interactive environment and earn credit from their own institutions (State University of New York [SUNY] 2024; Vahed & Levine, 2019). COIL has been shown to be a cost-effective and inclusive way to provide a global experience to all students enrolled in a given course because the experience is virtual and students incur no additional costs to participate (SUNY, 2024). Through synchronous and asynchronous activities, COIL empowers students to learn about and appreciate cultural differences, develop global citizenship skills, and understand how varied health care systems and the role of nurses in different countries impact patient and family experiences with health and illness. By integrating students from diverse backgrounds into a shared virtual classroom, COIL fosters international dialogue and cultural exchange (SUNY, 2024).
A COIL partnership was established between the University of North Carolina at Chapel Hill (UNC) in the United States, and the Universidad de São Paulo (USP) in Brazil. Within the COIL experience, prelicensure nursing students engaged in shared synchronous and asynchronous learning experiences over a 5-week period while exploring families’ experiences with pediatric chronic conditions. Learning objectives for the experience were to (a) apply the nursing process in the delivery of family-centered, culturally responsive nursing care through the care continuum (UNC), (b) identify opportunities for nurses to advocate for pediatric patients and their families to enhance informed decision-making and access to quality health care (UNC), and (c) understand the child, adolescent, and their family in a situation of disease in relation to growth and development, family structure and dynamics, and socio-cultural factors as the basis of care (USP).
The purpose of this study is to describe the experience of nursing students regarding family-centered care of children with chronic conditions through a COIL experience. Our research question was: What are prelicensure nursing students’ experiences and perceptions of learning family-centered care in pediatrics within the context of COIL?
Methods
Procedure
In this study, we used a qualitative research design methodology with focus group discussions. This method offered several advantages. First, focus group discussions gathered rich, detailed data by fostering interactive exchanges, promoting participants’ comfort in sharing openly, comparing experiences, and building upon each other’s ideas. This dynamic format allowed for diverse insights to be shared that might not have emerged in individual interviews or surveys. Second, focus group discussions facilitated real-time clarification, enabling researchers to probe deeper into specific topics as they arose. Third, the format of focus groups emphasized communication and collaboration, mirroring the dynamics of participants’ engagement in COIL experiences. Finally, including students from different cultural and educational backgrounds, such as those from the United States and Brazil, allowed for comparative analysis, helping the researchers to identify common themes and unique international challenges.
At the time of focus group data collection, 532 students had participated in this COIL experience during the current and previous academic year, with 402 coming from UNC and 130 from USP. Following Institutional Review Board (IRB) approval from both universities, study participants were selected through convenience sampling, responding to an email requesting voluntary participation from students enrolled in the pediatric course at their respective university. Focus group discussions were conducted 3 months after the COIL experience ended and 2 months after the course had been completed and evaluated, ensuring that students would be able to reflect on their experiences with some distance and to avoid potential coercion or undue inducement for participation in the research. Written consent forms were completed prior to the start of the focus group sessions.
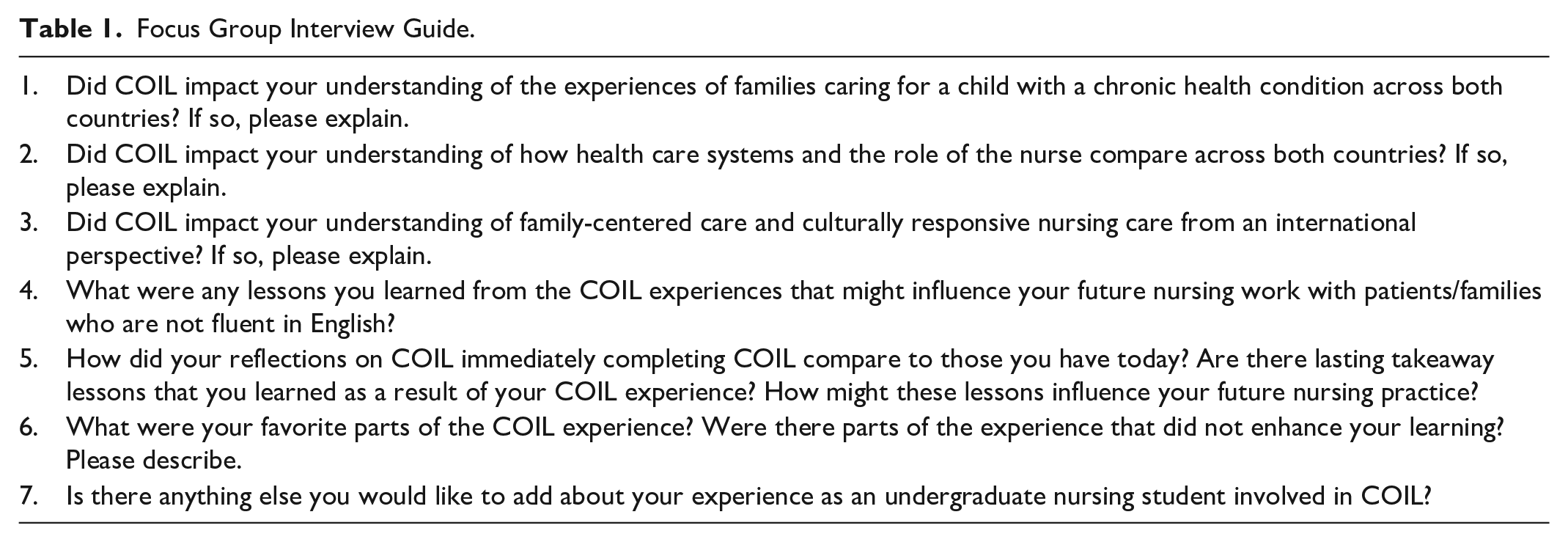
Data collection took place over 6 months in 2023. In total, the study had 6 focus groups with 37 students; 24 of these students were from UNC and 13 were from USP. Each focus group session was designed to facilitate an open and honest discussion related to the students’ experience with COIL and was conducted in the students’ native language. The sessions were held in-person in a private and confidential location convenient for all participants and each lasted approximately 60 minutes. The discussions were guided by a set of predetermined questions, which helped maintain consistency across all groups while allowing for the deep exploration of topics, as shown in Table 1. Participants self-assigned a pseudonym to use throughout the discussion. Data collection involved audio recording and transcribing the focus group sessions verbatim, ensuring a comprehensive capture of the discussions. Strict confidentiality protocols and ethical guidelines were adhered to throughout the study.
Focus Group Interview Guide.
Data Analysis
Data analysis was carried out by two research team members from the United States and three from Brazil, bringing a rich mix of cultural and academic perspectives to the process. Monthly meetings helped researchers from both countries to maintain consistency during the process and ensure reliability for data analysis. We employed an inductive analysis approach. Because focus groups in each country were conducted in the students’ native language (English for the U.S. students and Portuguese for the Brazil students), we began the analysis with reading the transcripts from our own country’s focus groups. Next, we individually assigned first-level coding to meaningful segments of the transcripts, grouping similar codes to identify patterns and relationships. To ensure the reliability of our analysis, we conducted intercoder reliability checks, where multiple researchers independently coded the data and then compared results to reach consensus. Once we had focused on codes and categories within each country, allowing for in-depth, context-specific analysis, we compared and merged our findings from both countries. Through this approach to data analysis, we ensured that the identified themes provided a comprehensive understanding that incorporated insights from both countries. Categories and quotes were translated from Portuguese to English, with analysis of language and semantics, performing translation and back-translation of the content.
Results
Sample
Focus group discussions occurred with 4 groups of nursing students from the United States, each with 5 to 7 students. Two groups were comprised of traditional Bachelor of Nursing (BSN) students (n = 13), whose average age was 22 years old. Of these, 10 had at least one experience with international travel, and 5 were first-generation college students. Two additional focus groups from the United States were comprised of Accelerated Bachelor of Nursing (ABSN) students (n = 11), who had previously earned a bachelor’s degree in a different discipline. These participants averaged 30 years old, all reported experience with international travel, and 3 were first-generation college students. For each of the groups from the United States, the pediatric nursing course took place in their second to last semester of nursing school.
The two cohorts of students (n = 13) from Brazil followed a traditional Bachelor of Nursing Science model, with their pediatric course falling in the fifth or sixth semester and the first semester of clinical in acute setting. The average age of students participating in the focus groups from Brazil was 23 years old. Most were female (N = 10), 7 reported international travel and 3 were first-generation college students.
Qualitative Themes
Following a rigorous data analysis, four central themes emerged. These themes include (a) understanding the needs of families of children with chronic conditions as impacted by health systems, (b) assigning meanings to family care of children with chronic condition, (c) applying concepts of family-centered care, and (d) self-reflection. Table 2 reflects how each theme was developed from organizing subthemes within the data. Participants shared insights about family-centered care throughout the entirety of each focus group discussion, not simply in response to questions directly addressing family-centered care.
Themes, Subthemes, and Exemplar Quotes.
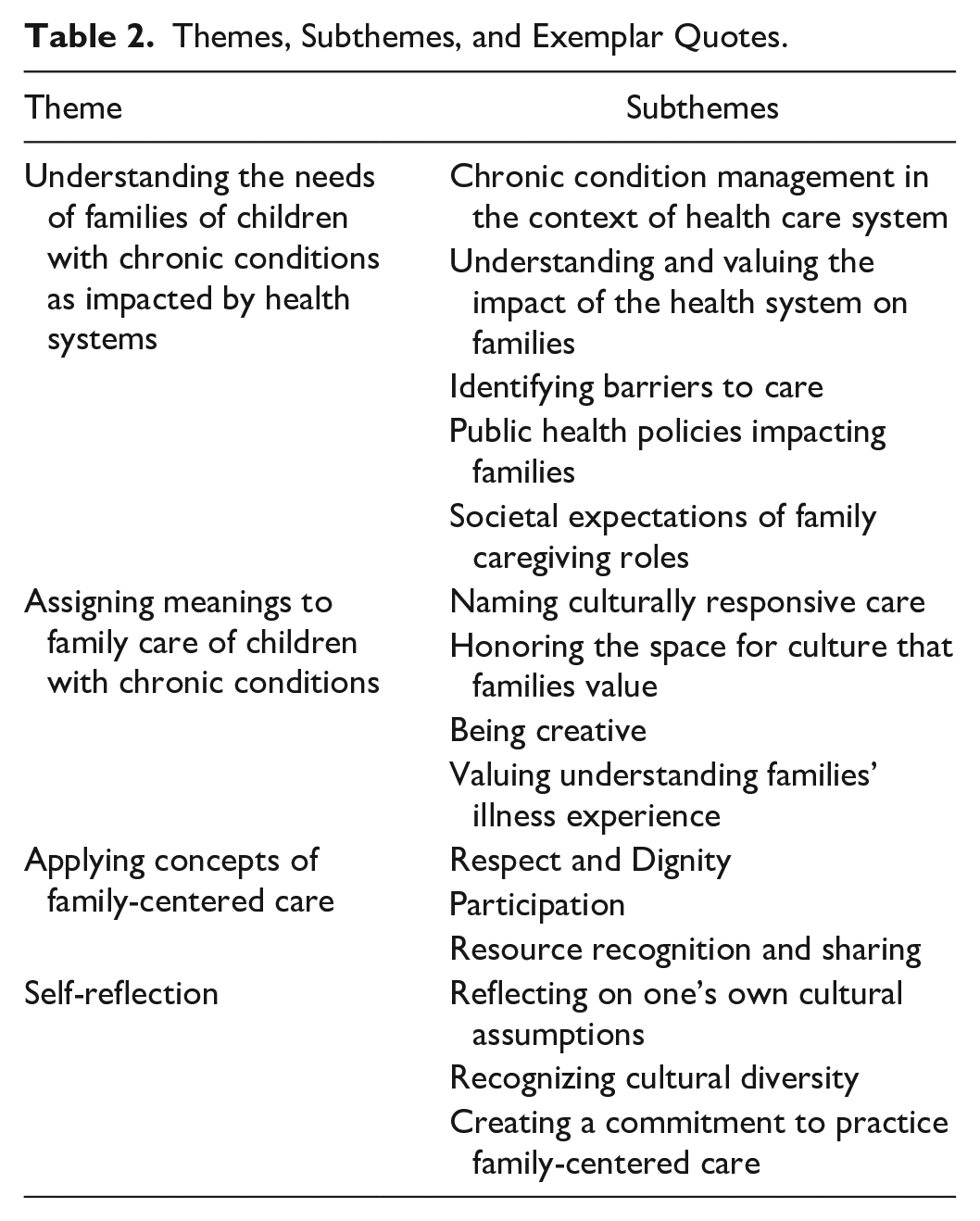
The first theme, understanding the needs of families of children with chronic diseases as impacted by health systems, explores how health systems influence the management and experiences of families with children who have chronic diseases. Key subthemes included: (a) chronic condition management in the context of the health care system, which examined how various health care systems support or hinder the management of chronic conditions in children, (b) understanding and valuing the impact of health systems on families, which recognized the importance of health systems in shaping the experiences and outcomes for families, (c) identifying barriers to care, including obstacles that families face in accessing care and managing chronic conditions, (d) public health policies impacting families, which considered how health policies affect the care and support available to families, and (e) societal expectations of familial caregivers, which explored societal roles and expectations of family members as caregivers within different health systems. Students across all focus groups discussed the impact of health care access on families and the importance of empowering families within these systems. Furthermore, they considered the health policy differences between the two countries and how policy can impact care. For example, when considering the universal health care system in Brazil, one Brazilian student reflected, “it helps us to expand our understanding of the importance, because for us it’s normal, families have access to everything. When you realize that someone else doesn’t think it’s normal, you start to appreciate it.” A student from the United States similarly reflected, [COIL] gave me a good understanding of their health system, our own health system, and how patients and families interact with those health systems—how frequently they engage with them and the knowledge base they have about their chronic condition and how it’s managed.
The second theme, assigning meanings to family care of children with chronic conditions, explored the nuanced understanding and practices of family-centered nursing care for families of children with chronic conditions. The theme included four subthemes: (a) culturally responsive care, (b) honoring the space for culture that families value, (c) being creative, and (d) valuing the understanding of families’ experiences. Culturally responsive care emphasized the importance of providing care that respects and integrates the cultural backgrounds of families, ensuring a personalized approach to nursing. Students emphasized the value of culturally responsive care and were able to name what culturally responsive care looks like in nursing practice. A student from Brazil stated, when you look at a family individually, you have to consider their culture, so I think that’s exactly it, we managed to give a name to something that we always try to do, but it also awakened a bit of a more attentive look of “am I doing this?”
An almost identical statement was made by a U.S. student: learning the word culturally responsive care . . . how to care for each family itself, not only the standard procedures, but what they need, how to help, the support network they have, everything developed for the child’s life. It gave a name to what we were doing, and it makes it easier for us to search, to learn more.
Furthermore, a Brazilian student stated, “[COIL] helped to give a name to what we were doing and made it easier for us to look for it, to learn more.”
The subtheme of honoring the space for culture that families value highlighted the necessity of creating and maintaining spaces where families’ cultural values and practices are respected and acknowledged in the care process. Brazilian and U.S. students alike reflected on the importance of considering each family’s unique cultural context, with statements highlighting the recognition and naming of culturally responsive care as a crucial aspect of their training. They noted that understanding this concept allowed them to seek further knowledge and improve their practice. One student stated [being] culturally responsive is not necessarily with another country, in clinical experiences you can take a patient who doesn’t accept, for example, a transfusion, and his surgery was all planned [. . .] we deal with this a lot daily, various religions, various beliefs.
The subtheme of being creative focused on the need for innovative approaches to meet the unique needs of each family, especially in overcoming challenges such as language barriers and access to resources. Brazilian students highlighted the role of creativity in overcoming barriers and establishing bonds with families, while U.S. students discussed the importance of leveraging available community resources in innovative ways. One student from Brazil stated, I always hear people saying that the special thing about Brazilian nurses is their creativity. So, I think this has become more evident, especially with the language barrier. You have to use other devices and you have to be creative because not only do you have to establish a bond with the person, but if you’re thinking about the family, you need to establish a bond with the whole family so that you can provide good care for that child.
A U.S. student remarked, “[COIL] helped me get creative in terms of what it is that our health care system does offer or that our community does offer that aren’t necessarily quantifiable.” The subtheme of valuing the understanding of families’ experiences recognized the significance of understanding and appreciating the lived experiences and perspectives of families dealing with chronic conditions. One student from Brazil commented, In my COIL group, we discussed once a child has had a transplant, they have to be looked after for life and we were able to address the family issue a lot. We compared their experiences and noticed that there [U.S.] they have a lot of blogs that help families and here [Brazil] we don’t have as much.
Theme three, applying concepts of family-centered care, showed how the concepts of family-centered care were integrated throughout the COIL activity; students reflected on the experience of families in different countries and the responses of professionals and health systems to meet the demands of families. Three subthemes included respect and dignity, participation, and resource recognition. Students valued the diversity of families while discussing care of children in different contexts as a part of respect and dignity. As one of the students from Brazil stated, “[COIL] helped me to emphasize a different perspective for each family, because we become so immersed in the system that we lose this individuality, of each person and each family.” A similar sentiment was reflected in the U.S. focus groups, with one student saying, I think that the COIL experience really reinforced like the idea that family-centered care and culturally responsive care is different for every family . . . there’s lots of diversity and lots of people from all over the world . . . there’s different cultural mashups . . . it looks different for every family. There’s not a one-size-fits-all culture that you can just assign and think that you’re being culturally responsive.
A second subtheme of applying concepts of family-centered care was participation, described as understanding and honoring a families’ autonomy to participate in health care decisions. Students reflected on times when families opted out of care that the health care team recommended or made a decision they did not support. One Brazilian student stated, I realized that sometimes we think we’re offering the best, but for some belief or other reason he doesn’t want it. So, we have to stop and understand our limits, how far we can go. Because people, families have autonomy, right? Dignity and all that, so we also have to stop and think about it and respect it.
A third subtheme, resource recognition and sharing, was seen throughout the focus groups from both countries. This subtheme included students recognizing available resources such as community services, translator services, and technology, while emphasizing the professional’s role in assisting families in obtaining information to access health rights and navigate the health system. Because of the differences in the health care systems between the two countries, students had rich discussions related to resources and access to care. When considering resources within the health care system, one student from Brazil stated, [COIL] showed me to value more what we have available and always show it to families. We don’t always know everything that SUS [the Unified Health System in Brazil] offers or all the rights that this person has, so it helped me to open my eyes to always show and pursue all the rights that families have here [in Brazil].
A similar sentiment was shared by a student in the United States: . . . just knowing that you need to allocate the appropriate resources for case management and social work and that kind of thing to help support these families especially with chronic condition where they might be in and out of hospitalizations and primary care. There’s a lot of pressure put on any family in the U. S. to navigate their care alone . . . I think a system should be in place for everybody but especially for people of different cultures.
Within the U.S. focus groups, there was a great deal of discussion around resource utilization, including how essential translator services are.
The fourth theme of self-reflection highlights the importance of a commitment to continuous learning and self-awareness in providing family-centered care. Although not explicitly introduced in the activity, self-reflection emerged as a fundamental aspect of caring for families. This theme encompasses several subthemes, including (a) reflecting on one’s own cultural assumptions, where students critically examining their own cultural biases and preconceived notions that may impact their care practices, (b) recognizing the importance of cultural diversity, which emphasized the value of understanding and respecting the diverse cultural backgrounds and beliefs of families, and (c) creating a commitment to practicing family-centered care, which focused on the ongoing dedication to integrating family-centered care principles into nursing practice, including the importance of language skills. Students made powerful statements with regards to reflecting on one’s own cultural assumptions. For instance, one student from Brazil stated, there are various beliefs that have a great influence on care, so that we can even rethink some of the prejudices we have . . . I think the culture is here on our side, you know? We have differences, for example. I think it’s very good for us to reflect . . .
A student from the United States similarly stated, I think it’s important to realize that you can be caught up in your own bubble sometimes . . . it’s important to take a step back and really think about where do these people come from and ask them . . . really to understand where they’re coming from in order to provide best care you can.
Students from both countries reflected on cultural diversity as not only being related to what country a family might be from but also their beliefs within their unique culture. Students noted how even a small amount of knowledge about language can help break down barriers and make a family feel more comfortable. A quote from a U.S. student exemplifies this concept: I personally am going to take it as a lesson on myself to try to learn little things in every language . . . so that I can at least say a single word that might make a family feel a little bit more comfortable in that I’m recognizing their culture and their language.
Discussion
Findings from the focus group data indicate that COIL provided an experience to these students which was transformative in learning the principles of family-centered care. The themes developed from the focus group data in many ways mirror the principles of family-centered care developed by the Institute for Patient- and Family-Centered Care (2024). These principles, including dignity and respect, participation, information sharing, and collaboration are similarly reflected in the International Family Nursing Association (IFNA, 2013) position statement on Nursing Education. We found that as a result of the COIL experience, students were not only able to identify these important concepts without being directly taught about them, but also consider how they would apply these concepts in their future nursing practice. In addition, because of their experience with COIL, students were able to reflect on their own cultural assumptions.
It was also apparent that as a result of the COIL experience, students were also beginning to operationalize concepts of family-centered care. This was seen in relation to theme 3 in assigning meanings to family care related to pediatric chronic conditions. Students discussed the importance of placing the child’s chronic condition within the context of the family and their culture. Providing a platform for students to share experiences from different places in the world allows students to learn from other’s experiences engaging in cultural competence as part of family-centered care. Research has shown that using real-life examples has been a promising way to teach nurses to work in multicultural environments (De Castro et al., 2019). Being able to cite examples from both personal and clinical experiences and then share these experiences in an international group setting allowed students to recognize areas in which they are able to practice family-centered and culturally responsive care.
Competences for teaching family-centered care include validating family’s health care experiences, empowering families, recognizing communication, and interactions between family members and health care team, and develop strategies to support families (Meiers et al., 2018). Many of the themes found in our focus group data from the COIL experience are mirrored in these core competencies. Through this COIL experience, students were able to consider interactions both personal and in the clinical setting that help to name these features of family-centered care. From the focus groups, students cited examples such as using a variety of technologies for interpretative services, to help provide high-quality language support and family-centered care. Students also acknowledged the need for creativity and use of research to aid in communication with families. As we continue to consider competency-based learning in our curriculums, COIL provides a space to consider both concepts of family-centered and culturally responsive nursing care.
COIL has been shown in other studies to increase intercultural awareness, a critical component of family-centered care that places the family in the context of their culture and cultural experiences (Malik et al., 2023). In both qualitative and quantitative analyses of COIL experiences, researchers have noted an increase in intercultural awareness and broadened global perspectives related to health care around the world (Jenssen et al., 2024; Niitsu et al., 2023). Findings from our focus group research are similar. Students reflected on policy and health care systems from each country, how these impacted families in their ability to care for their child, and how policies and health care systems impacted their nursing care as well. Students were able to critique the different health care systems in the United States and Brazil, then brainstorm how they could best support families within each unique system. COIL also helped students to recognize that within our global community, families coming from other health care systems may have very different views of health care and as nurses we need to be aware of these differences to be able to support all families. Students acknowledged that health care is continually changing and with these changes come nuances in supporting families. As they begin their nursing careers, students recognized that practicing family-centered care within a health care system will be a lifelong learning endeavor.
Data collection for this study was completed after students had entered the next semester of their nursing program. Because of this timeline, students were able to reflect on their COIL experience and how it influenced their nursing care going forward. One example that surfaced across focus groups was the use of interpretation services. Students recognized the barriers that language differences can cause, not only in reflecting about patient care experiences, but also in interacting with each other during the COIL experience. Other authors have noted language challenges during the COIL experience itself (Matthews et al., 2021; Righetti et al., 2019; Woodley et al., 2023) but not how working through these challenges can inform nursing students when working with diverse families. As such, this represents a new finding.
Swan and Eggenberger (2021) found that for new graduate nurses, learning family-centered care aids in care because it results in increased family trust, increased communication with families, and establishes connections with families. This was central in our theme of applying concepts of family-centered care as well as students reporting feeling empowered to ask specifically about what families may need with regards to care. With further research, we hope to see continued examples of application of family-centered care in the clinical setting.
Given the importance of practicing family-centered care as a part of culturally responsive care, this is an area that warrants continued investigation. There is great potential for COIL as a teaching modality in nursing education as a way to teach family-centered care with a global perspective. The collaborative cross-cultural experience provided by COIL, where students discuss family-centered care in the context of pediatric chronic conditions, is an invaluable teaching tool. COIL continues to be an inclusive, low-cost global experience within baccalaureate nursing education. It will be important to continue to investigate how COIL and family-centered care influence nursing practice of nursing graduates as they enter the workforce.
Limitations
The collaborative international analysis process played a pivotal role in achieving a comprehensive understanding of the data. The participation of researchers from both the United States and Brazil enriched our analysis and bolstered the credibility of our findings. However, we acknowledge certain limitations, including potential biases stemming from cultural differences and the complexities of coordinating and amalgamating research findings. In addition, because student participants volunteered and incentives were minimal, we may have captured the experiences of those most enthusiastic about COIL. Focus groups were conducted 2 to 3 months following the end of the course. The extended time between completion of COIL and focus group discussions, while beneficial in allowing students to be immersed in the next clinical setting and able to reflect COIL experience, may have caused some details of the experience to be forgotten. These constraints underscore the need for continued exploration and refinement in future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the University of North Carolina at Carolina Hill Office of Global Affairs and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq 409190/2023-3).