
Abstract
Black family caregivers of persons with dementia experience high levels of stress that can negatively affect caregiver health outcomes and reduce caregiving capacity. However, Black caregivers tend to report low levels depressive symptoms or other negative health effects. This qualitative descriptive study aimed to identify factors that contribute to resilience among Black family caregivers. Using the rigorous and accelerated data reduction (RADaR) technique to complete thematic analysis, a team of five coders examined transcript data from three focus groups of Black current and former family caregivers (n = 17) of persons with dementia. We identified three primary factors that contributed to caregiver resilience including access to supportive environments, adaptability, and planning skills. Caregiver resistance to reporting depressive symptoms may be attributed to the strong Black woman schema. Findings from this study may be used to develop future culturally responsive interventions that support caregivers and promote family health.
Dementia, a broad category of description for terminal diseases that cause progressive cognitive decline and physical deterioration such as Alzheimer’s disease, vascular dementia, frontotemporal dementia, and Lewy body dementia, affects more than six million families in the United States (Alzheimer’s Association, 2022). Long disease trajectories coupled with progressive disability requiring increasing levels of direct care assistance often leads to emotional distress, financial strain, and general poor health among relatives who serve as primary caregivers (Akhter-Khan et al., 2022; Puga et al., 2022; Sheehan et al., 2020). As a result, fulfilling the role of family caregiver is generally stressful to the individual caregiver and causes strain on the family unit (Mitrani et al., 2006; Robinson-Lane et al., 2022b; von Känel et al., 2020). Racial disparities in dementia related diagnoses, treatment, access to care, and support services significantly adds to the stress and strain on Black families in particular (Alexander et al., 2022; Cothran et al., 2022; Lin et al., 2021; Stevens, 2014). However, Black family caregivers of persons with dementia persistently report lower levels of depression and anxiety relative to caregivers of other racial and ethnic groups (Janevic & Connell, 2001; Liu et al., 2021), perhaps suggesting an increased tendency toward resilience.
Resilience, or the capability to respond more positively than expected to a high-intensity stressor (Angevaare et al., 2020), has been attributed to a variety of individual, cultural, and environmental factors such as adaptability, maintaining a positive approach, high self-esteem, planning skills, and access to supportive environments (Fletcher & Sarkar, 2013; Poe et al., 2023). Although high self-esteem and positive reframing have been commonly noted within the population, particularly among older Black women (Chithambo & Huey, 2013; Hall et al., 2019; Patterson, 2004; Robinson-Lane, 2019), little is known about how other resilience factors may influence the Black caregiving experience. Certainly, religiosity and spirituality have been noted as positive adaptive coping strategies that may facilitate resilience by encouraging positive reframing and providing a supportive environment (Duangjina et al., 2023; Dunn & Robinson-Lane, 2020; Robinson-Lane et al., 2020). Furthermore, within Black families, the dominant role of religiosity and spirituality as important cultural attributes is well documented (Green & Chuang, 2023; Millett et al., 2018; Sisselman-Borgia et al., 2018; Taylor et al., 2013). As noted by Robinson-Lane (Robinson-Lane et al., 2022a), “For many generations, religion has played a central role in Black American culture and communities by facilitating important social connections among members and providing meaning and purpose to lives that are often in distress” (p. 51). However, despite these known characteristics, there remains a dearth of literature examining factors that facilitate, or hinder, resilience among Black family caregivers of persons with dementia. Given the risks associated with caregiving, having a better understanding of resilience factors can lead to more effective clinical interventions likely to facilitate adjustment to the caregiver role and maintenance of both caregiver and familial health. To this end, the following study examined the experiences of Black family caregivers of persons with dementia with the goal of understanding resilience-related factors that may be incorporated into future intervention designs.
Methods
The primary research question, “What characterizes the experience of Black adults providing supportive care to a relative with dementia,” was addressed with focus groups of caregivers using a qualitative descriptive study design. Institutional review board approval for this study was granted by the University of Michigan (HUM00218293). The Consolidated Criteria for Reporting Qualitative Research (COREQ) (Tong et al., 2007) is used to report study findings (see Supplementary Table 1).
Recruitment
Study participants were recruited using study flyers distributed electronically to caregiver networks, through social media platforms (Facebook, Instagram), and within local communities at businesses serving older adults (senior centers, churches, adult daycares). Eligibility criteria included (a) age over 18, (b) ability to speak and understand English, (c) self-identified as Black/African American, (d) relation to a person over the age of 55 that has dementia or evidence of cognitive impairment, and (e) responsibility for monitoring and/or assisting with activities of daily living for the person with dementia.
Data Collection
Eligible and interested participants (n = 21) completed electronic written consent, of which 19 went on to complete a preliminary questionnaire administered through Qualtrics (2020). In addition to basic demographics, caregivers were asked to rate their personal health using items from the Patient Reported Outcomes Measurement Information System (PROMIS®) Global Health Scale Short-Form v1.2 (Hays et al., 2009). Care recipient needs were gauged based upon responses to the Barthel Index of Activities of Daily Living (ADL) (Mahoney & Barthel, 1965; Wade & Hewer, 1987) and the Lawton Instrumental Activities of Daily Living (IADL) (Lawton & Brody, 1969). The Barthel ADL index evaluates ADL needs in 10 areas and is scored by summing responses. Scores range between 0 and 20 with lowest scores indicating very severe disability and highest scores indicating independence. IADLS are similarly scored by examining functioning in eight areas. Scores range from 0 to 8 and lower scores indicate higher levels of dependence. Finally, caregiver social support was evaluated by means of the Personal Resource Questionnaire (PRQ2000) (Weinert, 2003)—a 15 item tool which asks respondents positively worded questions about their perceived level of social support and provides a summary score ranging from 15 to 105 with the higher numbers indicating higher levels of perceived social support.
Participants (n = 19) completing surveys were compensated for their time with US$25 as either a check or Mastercard gift card, depending upon their preference, and assigned to one of three focus groups. Focus group assignments were contingent upon timeframe of survey completion and participant availability. Two participants withdrew from the study and did not participate in the focus groups leaving the total number of focus group participants to 17.
Each focus group (n = 3) consisted of 5 to 6 participants (Group 1 = 6, Group 2 = 6, Group 3 = 5) and took place virtually using the Zoom video teleconferencing platform (Yuan, 2023) over the course of approximately 90 minutes. The primary author (S.R.), a trained Black female nurse scientist with expertise in dementia care management and focus group moderation, conducted all focus group interviews with other diverse team members (F.J., M.T., J.J., and T.Q.) in attendance to make observational notes. A team de-briefing took place after each focus group meeting to review observations.
Focus group participants responded to three basic prompts that elicited naturally flowing narratives about caregiving experiences: (a) How long have you been a caregiver and what’s your relationship to the person with dementia that you are supporting, (b) what challenges have you faced, and (c) what supports have you found useful? Following the interviews, verbatim transcription was completed. Initially, this was done automatically within the Zoom platform; however, an extraordinary amount of data cleaning was needed to make the transcript suitable for analysis. Consequently, transcription of interviews for focus Groups 2 and 3 were completed with REV transcription service (www.rev.com). All transcriptions were compared to recordings, extensively reviewed for accuracy, and deidentified as needed. Focus group participants were compensated US$50 by check or Mastercard gift card depending on their preference.
Analysis
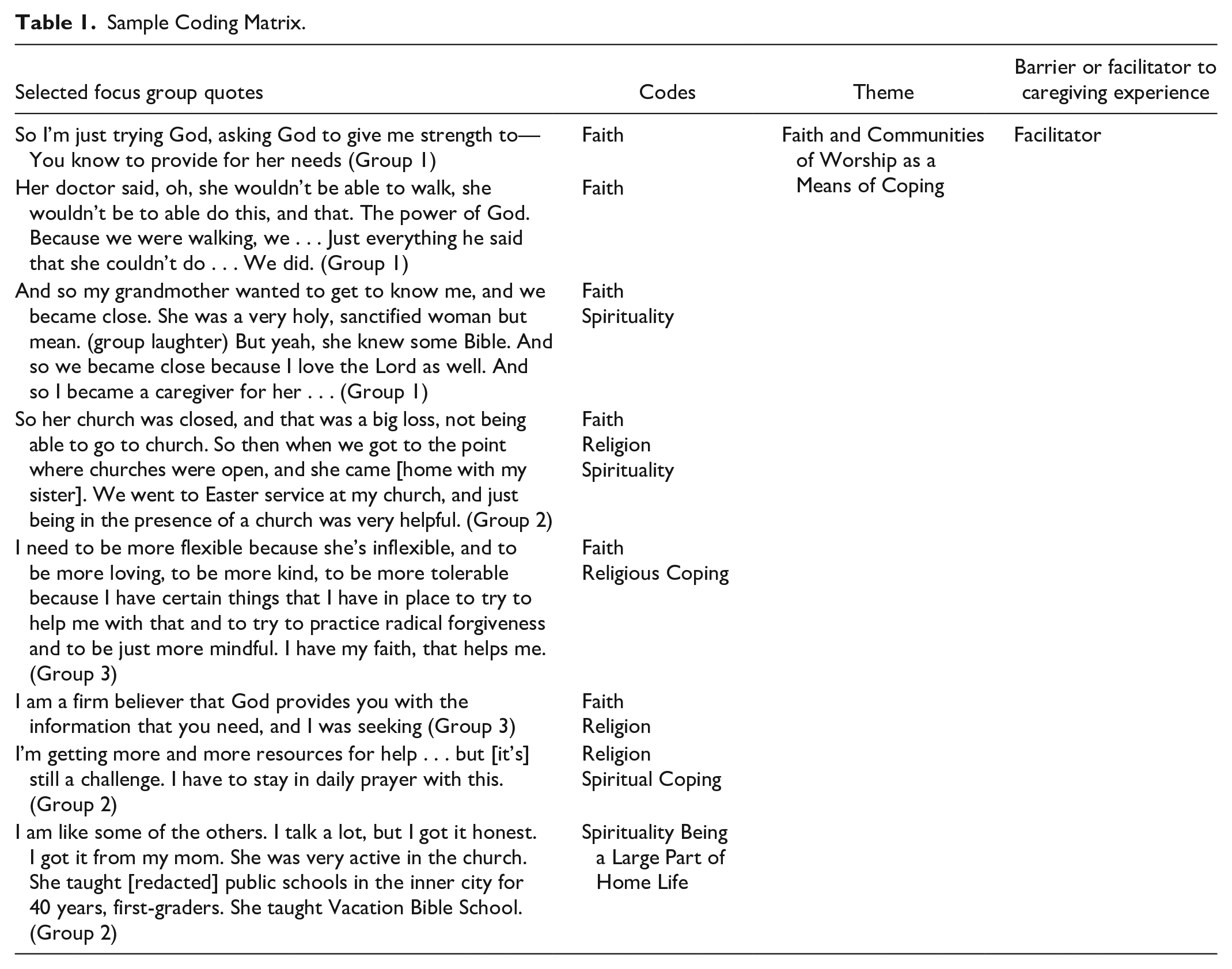
Thematic analysis was completed using the five-step rigorous and accelerated data reduction (RADaR) technique outlined by Watkins (2017). The RADaR technique was selected as an efficient and practical means of collaborative data analysis likely to facilitate intervention design. After ensuring that transcripts from all three focus groups were formatted in the same manner, data tables were created in Microsoft Excel (Microsoft Corporation, 2023) with rows separating individual participant responses and columns used to differentiate interview questions, responses, notes, and codes. A team of five trained coders then identified text responses from participants that highlighted the experience of providing supportive care to a relative with dementia. The selected text was then carried forward into a new reduced data table and open coding was completed by the same team members. Identified codes were then enlarged, printed, and cut for manual axial and pattern coding by the team to identify common themes and clarify coded definitions and relationships until team consensus was reached and data saturation across focus groups was achieved. Final codes were then reviewed and classified as either a barrier or facilitator to family caregiving and considered within the context of resilience (see Table 1 for sample coding matrix). Survey items included on the premeeting questionnaire were analyzed in Microsoft Excel (Microsoft Corporation, 2023) and only included data matched to focus group participants.
Sample Coding Matrix.
Results
Characteristics of Study Participants
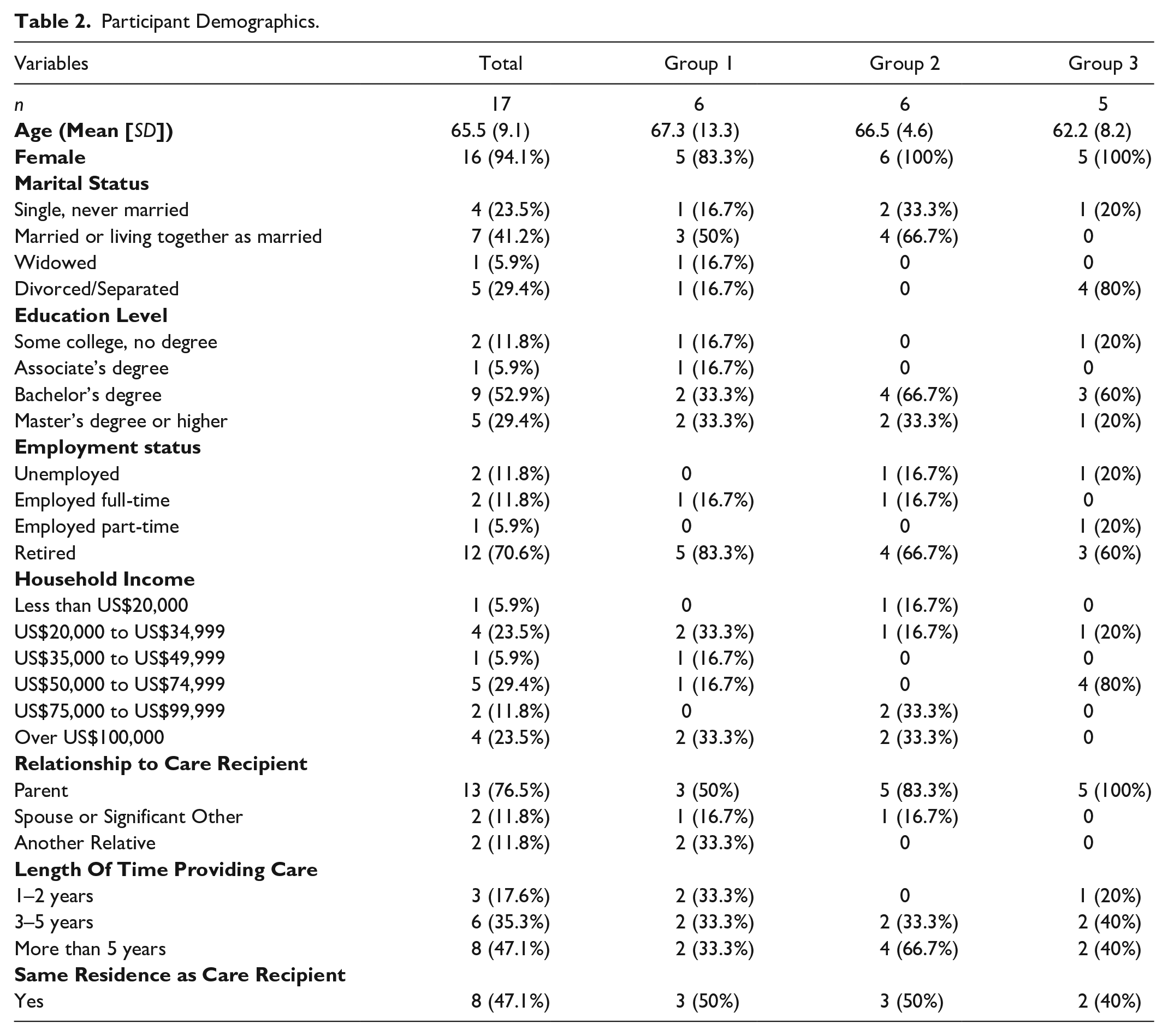
Focus groups participants (n = 17) were primarily women (n = 16) with an average age of 66 (SD = 9.12) who were caring for their parent (76.5%), spouse (11.8%), aunt or uncle (11.8%), for 3 or more years (82.4%). Care recipients were severely disabled as evidenced by an average Barthel ADL score of 10 (out of possible 20) (SD 5.93) and an average IADL score of 1 (out of possible 8) (SD 1.12). When considering their overall health, including mental health, 76.5% of caregivers reported their health as either good or excellent. 35.3% of participants reported sometimes experiencing feelings of anxiety, depression, or irritability over the past week, while 11.8% reported experiencing these feelings often or always. 15 out of 17 participants reported daily pain including 52.9% who reported mild daily pain (pain rating of 1–3 on 0–10 scale), 23.5% who reported moderate daily pain (pain rating of 4–6 on 0–10 scale), and 11.8% who reported severe daily pain (pain rating of 7–10 on 0–10 scale). When rating satisfaction with social activities and relationships, the majority (76.5%) of caregivers rated their satisfaction as good to excellent. Similarly, the average social support score for the group was 87 (range 63–105) indicating strong perceived social support. Other demographic findings are reported in Table 2. Analysis of focus group transcripts revealed seven barriers and three facilitators of family caregiving.
Participant Demographics.
Barriers to Family Caregiving
Participants described barriers to family caregiving included (a) financial challenges, (b) familial expectations and lack of support, (c) managing difficult emotions, (d) dealing with challenging behaviors, (e) dealing with gaps in medical care and supportive services, (f) preventing or managing institutionalization, and (g) adjusting life to be a caregiver.
Financial Challenges
Participants described unexpected financial challenges that made both providing care and getting additional support such as respite from care tasks difficult, despite having insurance. As one focus group member noted, “I think when your parent has an adequate, very sufficient income, these can be a hindrance to maybe getting certain kind of services” (Group 2, transcript lines 584–593). The additional costs of care often made typically anticipated activities like vacations unattainable. As another participant noted, I have to pay—I have to pay people to come to stay here, you know. It’s unfortunate, that’s the way things are. And yeah, I just tend to go with the flow at this point. You know, it is what it is, and I go with it. And the cost of respite care here is like $500 a day. So, for me to go on vacation, it’s like double the money. Unfortunately, you know we do not qualify for any type of assistance. (Group 1, transcript lines 455–473)
Even in instances where care recipients qualified for some services or had the financial means to adequately support themselves, caregivers often ended up with regular out-of-pocket expenses. One participant who regularly drove over 800 miles to manage care for her uncle, the third care recipient she was now responsible for noted, “My grandmother had no money, my mom had no money, so a lot of times you’re paying for things. My uncle has, but he has a lawyer, so that money is his and tied up” (Group 1, transcript lines 639–642). The added expense of care was seemingly more frustrating for caregivers due to the lack of expected support from other relatives.
Familial Expectations and Lack of Support
Although a few caregivers reported working “really well together as a team” (Group 3, transcript lines 345–353) with a sibling or a spouse, most participants expressed disappointment with their siblings and other relatives for their lack of initiative in providing tangible support in caregiving responsibilities. As one participant succinctly noted, “I think that’s the hardest part of the journey—is to understanding—or trying to understand why others, or your siblings or whatever, don’t get it that you need help” (Group 3, transcript lines 303–306). Relatives of caregivers often presumed they were financially benefiting from the aged care recipient or that the services in place were enough. One participant noted, “Sometimes they think you have money when you’re dealing with your relative like . . . (exasperated sigh—lots of agreement from the group) and there is no money” (Group 1, transcript lines 633–635). Another lamented, I have a large family, and you think everyone will pitch in, but it’s like, “She stays with you, you take care of her and just let us know what’s going on.” And just trying to get them to understand that sometimes you need a break—it’s almost like having a baby. (Group 3, transcript lines 289–295)
Participants emphasized the challenges of creating a caregiving team and convincing other relatives to contribute financially or with time and active support. The reluctance to sometimes ask for help and a tendency toward self-isolation were also noted challenges that perhaps pointed to the next noted barrier—managing difficult emotions.
Managing Difficult Emotions
Participants described a range of emotions that characterized their caregiving experiences including joy, stress, sadness, disappointment, anger, gratitude, feelings of depression, emotional burden, and guilt. Although the caregiver’s relationship with their relative affected their feelings, the level of support they received, the care recipient’s behaviors, and the requisite lifestyle adjustments necessary for family caregiving also made a large difference in their emotional experiences. For example, a caregiver who discussed her varied experiences in caring for her mother for 7 years and her husband for three noted, “It was a joy—a joy to take care of my mother, because she was a quiet spirit, and it was a joy to take care of her” (Group 1, transcript lines 209–228). Care responsibilities were split equally with her sister. Conversely, when discussing the care of her husband, a former boxer for whom she managed care alone, she noted that it was, “very, very stressful when he couldn’t take care of himself” but that once her daughter came to assist her, that “some days were very, very stressful—and then some days it was joyful” (Group 1, transcript lines 209–228).
Care recipient health declines and personality changes were common source of sadness. When discussing the dementia progression of a combative aunt, one participant said, everything has really cooled down and she is more compliant. I hate to say that type of word compliant, but she’s always been that fighting person . . . It makes me sad that I don’t see that fight in her no more. (Group 1, transcript lines line 442–451)
Another participant noted that reading about disease progression wasn’t adequate preparation for the emotional experience of watching a loved one decline. She said, “I found that I was getting very depressed during this whole time because I wanted my mom back. I wanted that old person back (Group 2, transcript lines 597–601).
Participants also described emotional fatigue and guilt about feeling burdened with care responsibilities. When discussing the challenges of being a newlywed with a blended family and the added responsibilities of caring for her grandmother in addition to her children and husband, a participant rhetorically asked, “. . . what about me? Am I gonna take care of her for the rest of my life” (Group 1, transcript lines 1204–1209). She went on to describe feeling “guilty,” “horrible,” and “selfish” for considering her own needs (Group 1, transcript lines 1209–1213). Perspective change was mentioned as an important means of managing feelings of guilt and burden. It was noted, “I had to learn it wasn’t what I had to do, it’s what I get to do” (Group 1, transcript lines 1196–1204). However, challenging care recipient behaviors often made emotional self-management difficult.
Dealing With Challenging Behaviors
Participants described various stages of cognitive and motor decline among care recipients that resulted in wandering, insomnia, increased falls, difficulty with decision making, and challenges performing both instrumental (e.g., paying bills, cleaning, preparing food) and basic (e.g., dressing, grooming, toileting) activities of daily living. Confusion, embarrassment, stubbornness, and rejection of care assistance made care delivery both physically and emotionally difficult, and safety a persistent concern. One caregiver recounted, I remember my sister and I were changing the linen on [mom’s] bed thinking innocently, we’ll help straighten up around the house. And we came down and put the linen in the bag, and she went on this rant that I had never seen before. “Who told you to change my linen on my bed? How dare you.” And I had never seen this . . . I had never heard my mother yell at me like that. And some of the language she used, I was like, “Wow.” It really got me. (Group 2, transcript lines 300–319)
The desire of the care recipients to maintain independence and save money sometimes led to exploitation. One caregiver recalled that her stepmother had “befriended this lady, moved her in, and she was unfortunately exploited—because she didn’t want to pay . . . The lady ended up abusing her, giving her a sleep aid” (Group 1, transcript lines 855–864). Another recounted “a so-called church member” who was going to help her aunt and uncle, who ended up getting her aunt to “sign forms to get her house from her for $1” (Group 1, transcript lines 683–692). Care recipient behaviors were not just stressful and emotionally taxing for caregivers, but also made providing care challenging, time consuming, and ultimately more costly. Caregivers noted that gaps in medical care delivery and poor access to supportive services—particularly in the early stages of dementia created additional burden that perhaps could have been avoided.
Dealing With Gaps in Medical Care and Supportive Services
Getting the right medical or supportive care was often difficult for caregivers for a variety of reasons. In the early stages of diagnoses, it was common for care recipients to be guarded about memory issues and/or care needs which meant that caregivers often needed to step into a supportive role in the midst of a crises. For example, one participant recalled receiving a phone call from his aunt’s doorman who informed him, “there’s something going on with your aunt” (Group 1, transcript lines 376–382). This call necessitated out of state travel for a wellness check and then evolved to quickly trying to get necessary services in place. Participants found that identifying appropriate services was difficult “because they’re not really advertised . . . it’s almost like it’s hidden if you’re not in case management or social work” (Group 3, transcript lines 191–198). They also expressed disappointment that information about what to expect and available support services were not readily provided by members of the care team. One care giver noted, You would think that the primary care physicians or someone in the medical field would reach out once they have diagnosed someone with [dementia], or even the pharmacist when they see the medication that you’re getting, that they would have some type of suggestions or information. But I have received nothing from any of that. I’ve even asked the primary care physician about it and they didn’t have a clue, they were like, “Well, you’re on the medication, that’s basically all we can do.” (Group 3, transcript lines 237–243)
Another participant expressed frustration with language use that made it difficult to understand what was happening or what to expect. She recalled, The hardest part for me was at first I didn’t have any patience. And when my mom was repeating herself a lot, I just didn’t have any patience and I would just say, “Well, Mom, I just told you that.” And I felt so bad later on after I was told by her doctor that she [had dementia] because her diagnosis at first was cognitive memory disorder, they didn’t say dementia. (Group 3, transcript lines 314–321)
Even after the diagnosis was clear and more information about available resources was known, participation in support groups and similar educational programming was difficult due to the timing of the offerings. As one participant recalled, I found that when I was really wanting to maybe be a part of a support group, most of them were during the day. Well, if you’re working you can’t go to a support group during the day. So I found that to be a challenge . . . (Group 2, transcript lines 584–593)
Despite the various difficulties caregivers faced with getting the support that they needed at the right time, one area of support they aimed to avoid for as long as possible was nursing home placement.
Preventing or Managing Institutionalization
Most care recipients desired to remain living in their own homes, despite advancing dementia. However, safety and increasingly high acuity care needs did not always make this possible. Caregivers were often concerned about care quality and treatment in long term care communities and aimed to support their relative’s wishes to age in place by preventing institutionalization for as long as possible. Keeping relatives at home often required significant adjustments to work schedules such as early retirement and/or some level of familial support. One participant described her satisfaction with being able to keep her mother at home with her sisters’ support—despite all of them being employed: I have two other sisters, so, we kind of—all of us worked. So we had to kind of deal with that situation, but it worked out . . . we managed to take care of her. We didn’t really want her to go into a nursing home. I saw with my cousin—I felt that there were things that happened when she was initially put in a home where me or my cousin, we were her guardians and conservators; we didn’t have any control over, and I didn’t want anything like that to happen to my mother. So we worked very hard to keep her at home. And when she passed, she was at home. I was with her. (Group 2, transcript lines 264–275)
In instances where institutionalization was necessary, caregivers noted the importance of checking in on relatives regularly and when unexpected. As one caregiver noted, They give you different care when they know somebody’s coming in there—when they know you’re coming in here on a regular basis, and especially with me. They know I was coming at all times of the day. If I woke up in the middle of the night and said I’m coming in there—I’m going. Especially with my mother. (Group 1, transcript lines 980–994)
Caregivers, who found it necessary to place their relatives in long term care often expressed feelings of guilt and sadness. A caregiver who kept her mother home with her for many years before placing her in a nursing home recalled, It was hard for me once she went into the nursing home, I just didn’t feel comfortable going anywhere anymore. So that was difficult actually because I was limited in terms of what I could do because I don’t have any sisters. I don’t have a big supportive family or anything like that, and basically it was just me. (Group 3, transcript lines 323–329)
One thing all caregivers agreed on, regardless of whether they were able to keep their relative at home or not, or had support in care responsibilities, was that being a family caregiver required a significant lifestyle adjustment.
Adjusting Life to be a Caregiver
Focus group participants found it necessary to significantly adjust their lives to accommodate family caregiving. These adjustments often spanned years, included unexpected and regular travel, moves, changes in household composition, and adjusting work hours to accommodate direct care needs. One caregiver recalled, I became a caregiver for my uncle, who lived to be 90, and that was during the time when I was working, so I would stay with him for a while, go and pick up someone like 5 o’clock in the morning to come over and stay with him during the day while I was at work. I would go to work. Then I come out, and I have to take the caregiver [home] that was with him all day home, and then I would go back and take care of him. So it continued like that until he was finally in a nursing home. And he lived in the nursing home for 10 years. (Group 1, transcript lines 259–276)
The availability of support either from other family members or through paid services often influenced whether the caregiver was able to maintain employment. Another caregiver who supported her mother with dementia recalled, I still had a full-time job, and she was still living on her own, which she was able to do probably for over 10 years. But then I had to retire from my job early in order to keep her out of a nursing home and keep her home with me, so that’s how I came into being her caregiver for almost 25 years. (Group 3, transcript lines 19–24)
In addition to managing less disposable income, caregivers described how their care responsibilities necessarily reduced their social activities and vacations. This is partially what led one care giver who noted that she had “a passion for travel” to place her husband in a nursing home. She recalled, “I felt like I worked 40 plus years and I was looking forward to retirement together . . . I still want to move forward with things I want to do for the remainder of the time I’m on earth” (Group 2, transcript lines 72–79).
A factor that seemed to play a significant role in caregivers’ perceptions about life adjustments made for caregiving was the strength and nature of the relationship between the care recipient and the caregiver. Caregivers that described long care trajectories but who were able to recall joyful experiences during that time tended to have strong bonds with their relative prior to their dementia diagnosis versus strained relationships in which care responsibilities were described with resentment. For example, one participant who had a strained relationship with her mother and became a caregiver in her 20s following her mother’s stroke noted, “I was bitter. I’m not gon’ lie” (Group 1, transcript lines 477–480). Despite the many challenges that made adjusting to the caregiver role difficult, there were also factors that made the experience easier.
Facilitators to Family Caregiving
Facilitators of the caregiving experience included (a) faith and faith communities, (b) having a health care connection, and (c) support from local agencies and community programs. Each theme is described in further detail below.
Faith and Faith Communities
Faith and the social support provided by faith communities made a positive difference in the caregiving experiences of many participants. Church was often referenced when caregivers described places where they could get tangible care support or information about dementia care, services, or more. In addition to “relying on friends and church” for support, particularly when finances were a barrier to obtaining care (Group 2, transcript lines 605–614), caregivers also described being able to count on “church members, friends and family” to show up to help celebrate with them when needed (Group 1, transcript lines, 323–328). When speaking of being back in the physical church environment after COVID-related closures, one participant even noted, “just being in the presence of a church was very helpful” (Group 2, transcript lines 340–349). Caregivers also referenced using prayer as a means of coping, finding strength, fostering hope, and seeking providence.
For example, when referencing providing supportive care for her 91-year-old stepmother who she described as “a pistol” and “a firecracker,” one participant noted, “I’m just asking God to give me strength—you know to provide for her needs” (Group 1, transcript lines 151–174). Another recalled, “the power of God” when her mother’s recovery following a stroke far exceeded the physician’s medical prognostication. She recalled, “just everything he said that she couldn’t do—we did” (Group 1, transcript lines 355–365). Even amid despair or disappointment, there was a sense of thankfulness to God. When referencing her mother who died in 2019, another participant noted, “I thank God that God took her before COVID. That would’ve been horrible.” She went on to also thank God for having some help when she was responsible for the round-the-clock care for her mother in addition to raising two teenage children (Group 2, transcript lines 156–166). The idea that “God will not put any more on you than you can bear” (Group 2, transcript lines 721–729) was shared by many participants. In addition to relying on their faith, several participants were also able to rely on their own health care knowledge and connections to get their needs met.
Having a Health Care Connection
Participants described holding a variety of health care roles, and/or connections with health care workers, which helped them to navigate the medical system better and gave them an advantage over other caregivers. As one participant explained, I don’t know, it just feels like you’re left on your own to figure things out. And the people who don’t have a healthcare background, they’re left to really navigate this complicated maze of all of this information and what to do with it. (Group 3, transcript lines 261–269)
This navigation included getting general information about dementia care and being able to identify local service providers. One participant noted, I think by me being a social worker it helped, because I knew, you know, some of the social service agencies, and if I didn’t know I could ask a colleague so that helped because if you don’t know, you don’t know . . . (Group 1 transcript lines 898–904)
Another participant recalled working at a hospital and meeting people there who would recommend “people that would be willing to care give during the day” (Group 2, transcript lines 605–614).
Sometimes these relationships with health care workers developed in the process of receiving care for their relative. In thinking about the social worker who helped her to identify services for use after hospital discharge, including potential nursing homes, one participant recalled, “she said for me to go and check out a number of different places, and then, like I said later on, she was telling me about some other services” (Group 1, transcript lines 1072–1081). One participant even noted having the “personal cell phone number” of her mother’s physician and how “encouraging” it was to be able to “call her whenever” (Group 2 transcript lines 751–755). While these close personal relationships and intimate knowledge proved useful, the support provided from local agencies and programs also made a lasting difference.
Support From Local Agencies and Community Programs
Focus group participants described a wide variety of agencies and community programs that made a difference in helping them to learn more about dementia care or obtaining services that supported their family. These organizations included hospices, home health care agencies, adult day cares, support groups, and community centers. Specific organizations that were referenced included Universal Dementia Caregivers, the Area Agency on Aging, Meals on Wheels, Healthier Black Elders, Veterans Administration, AARP, A Place for Mom, Connecticut Community Care, Program of All-Inclusive Care for the Elderly (PACE), Nurses Improving Care for Healthsystem Elders (NICHE), and the Alzheimer’s Association. It was often a friend or colleague who recommended these programs to the caregivers. As one participant recalled, Somebody invited me to come to the caregivers [support] group again, and so I went back and then I realized I needed to be there. So that is the place where I got information about the dementia and how to care for my mom because I’m not a medical professional at all, my background was in accounting . . . I learned more, really, from other people in terms of what they were going through. That helped me a lot being a part of that support group. (Group 3, transcript lines 131–137)
Despite the emotional and practical hurdles that participants faced when juggling the responsibilities of caregiving, local organizations made a large difference for families by providing essential support.
Discussion
This study illuminates the complex landscape of families caring for a relative with dementia from the perspective of Black adults and identifies characteristics of the experience that contribute to caregiver resilience (see Figure 1). Primary stressors affecting adjustment to the caregiver role included financial difficulties, poor medical support, challenging dementia-related behaviors, unrealistic familial expectations, fears about institutionalization, and incredible time commitments that required major life adjustments. Despite these stressors, caregivers described how supportive environments, adaptability, and planning skills allowed them to manage high-intensity care effectively over long periods.
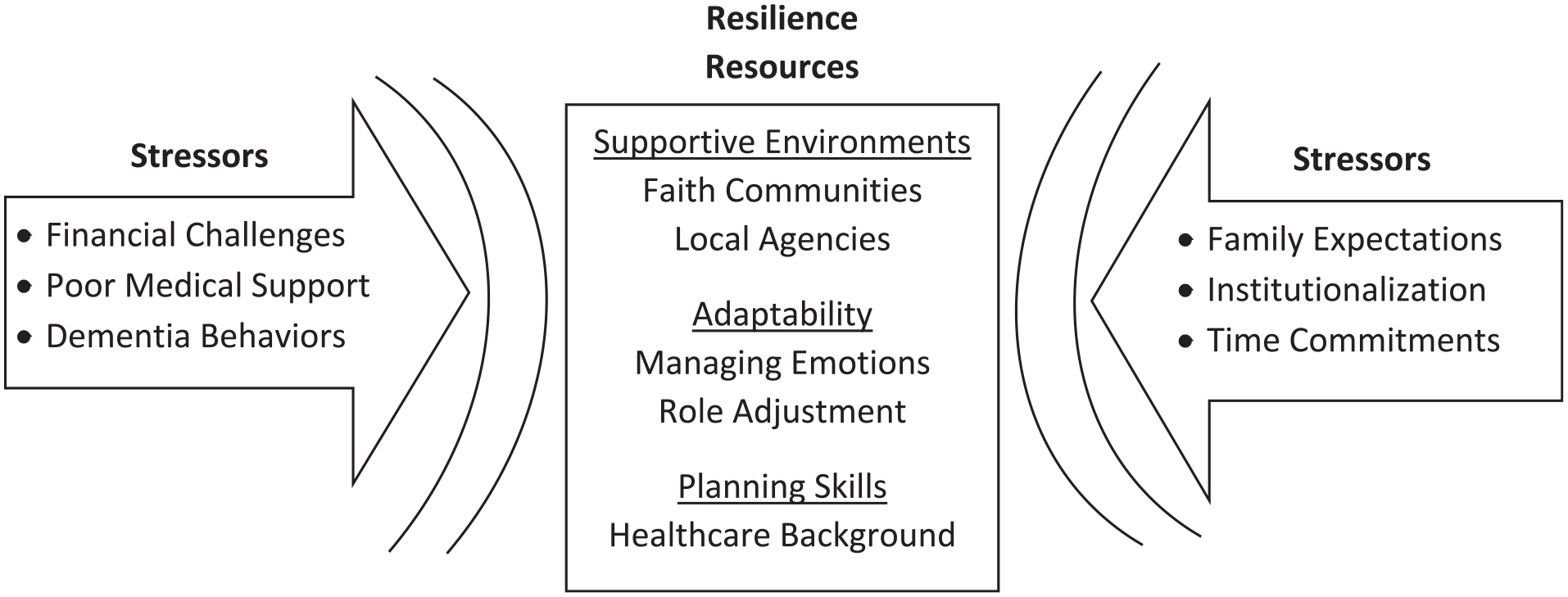
A Model of Resilience in Family Caregivers of Persons With Dementia.
Interestingly, when asked through survey items about their mental health, most caregivers described their mental health as being either good or excellent, yet when describing caregiving experiences, feelings of sadness, isolation, burden, and unease were apparent. Similarly, in survey responses, the majority of participants reported satisfaction with social activities and relationships and strong social support, yet in describing care activities many reported that care tasks limited social engagement, and several noted dissatisfaction with the social support they received. This dichotomy between survey responses and participant verbalizations in focus groups may be related to the cultural trait of remaining positive in the face of adversity that is prominent among older Black women. In other studies, examining Black adults managing challenging health issues or social situations, there have been similar themes identified around positive reframing of negative circumstances (Faronbi, 2018; Monte et al., 2023; Robinson-Lane, 2019) and the role of religiosity in positive reappraisal (DeAngelis & Ellison, 2017; Newlin et al., 2010). The cultural expectations for Black women in particular that center caregiving, maintaining multiple roles, and stress resilience while repressing one’s own vulnerabilities have been described within the strong Black woman schema (Beauboeuf-Lafontant, 2009).
The strong Black woman schema or archetype, often conflated with the superwoman schema, has been characterized as an obligation to: present as strong, suppress emotions, be independent, determined to succeed, and be compelled to help others (Woods-Giscombé, 2010). While the strong Black woman schema centers racial/gender identity and survival despite the odds, the superwoman schema centers gender identity with a focus on achievement (Woods, 2013). Historically, both of these ideals have supported personal and familial survival and thus facilitated adaptation, however, the cumulative effects of unmitigated stress and attempting to mirror expected characteristics can have deleterious effects on both personal and physical health of Black women including limiting the expression of depressive symptoms, psychological distress, poor self-care, and reduced help-seeking behaviors (Holden et al., 2015; Tillman-Meakins, 2017; Woods-Giscombe et al., 2019). It therefore comes as no surprise that chronic health concerns that can affect care delivery such as persistent pain, did not come up as noted challenges among the caregivers in this study despite its frequency of occurrence. It may also be that pain concerns were not a primary stressor, or as Roy (2008) would describe, a focal stimulus, requiring an immediate behavioral response—but nevertheless negatively affecting the overall caregiving experience and the meaning ascribed to it.
Tillman-Meakins (2017) suggests that providing effective clinical support to Black family caregivers that is culturally responsive might entail reframing caregiving as a strength rather than a stressor and then providing strategies that support both caregiver health and their role. To this end, our study illuminated concrete strategies caregivers themselves found effective in managing the caregiving role such as identifying and connecting with supportive communities, being flexible, and using planning skills. The lack of attention to caregiver mental and physical health care concerns also suggests a need for clinicians to advocate for caregiver self-care including identifying and setting attainable self-care goals. A primary obstacle to addressing caregiver health needs in clinical settings is identifying who are family caregivers. This basic demographic data should be included in care assessments and considered in the plan of care with special attention given to the language used to ask about caregiving responsibilities rather than relying solely on self-identification as a “family caregiver”—for many may not relate to this title (National Academies of Sciences & Medicine, 2023). Furthermore, as participants in this study indicated that gaps in medical care and supportive services were a barrier to effective caregiving, additional attention should be given to ensuring that family practice offices, particularly those serving significant numbers of older adults, encourage early family engagement when cognitive deficits are identified and have information readily available about dementia-related support services in the community. Health care systems can facilitate these efforts by ensuring that referral and resource information is accessible within the electronic medical record.
This study also provides important information about structural barriers to family caregiver support such as the need for workplace accommodations supportive of family care, increasing availability of information about dementia-related diagnoses and care needs from health care providers, and increased access to affordable respite and other similar services. Current initiatives like the Recognize, Assist, Include, Support, and Engage (RAISE) Family Caregivers Act are helping to advance these needs through a strategic plan inclusive of recommended federal, state, and community actions (https://acl.gov/CaregiverStrategy). Future research should test the effectiveness of implementing resilience-centered interventions among family caregivers, particularly longitudinally, and examine the effects of caregiver adaptive coping on the family unit. A recent review of resilience interventions by Ferreira and colleagues (2021) suggests that culturally responsive interventions with strong theoretical underpinnings are likely to have the greatest success, while Joyce and colleagues (2018) note the importance of addressing the logistical and cost challenges of face-to-face meetings by exploring virtual options. We suggest that future interventions for family caregivers should also incorporate key resilience resources identified by caregivers including facilitating connections with supportive environments like faith communities and local agencies, supporting the development of planning skills, and providing strategies that support enhanced caregiver adaptability (see Figure 1).
This study adds significantly to the literature on dementia family caregiving and resilience, however there were a few limitations. First, though the data provided by the sample of 17 was sufficient for deep qualitative analysis, including saturation of findings across focus groups, this small number of participants limits the generalizability of findings. Furthermore, while the virtual gathering of our participants allowed us to engage a national sample, our participants were predominantly from the Midwest and Eastern states. Finally, considering that the recruitment strategies included the distribution of flyers at community health programs, sometimes situated in churches, it is of no surprise that several participants were members of church communities. These limitations should be considered when interpreting findings.
Conclusion
Supporting the care needs of a relative with dementia can be incredibly challenging for family caregivers and may result in negative mental health effects and reduced caregiving capacity which can lead to institutionalization of care recipients. However, there are significant culturally relevant factors that seemingly contribute to the resilience of caregivers—and ultimately families. This study highlights those factors and lays the groundwork for future strength-based interventions that center community, faith, and practical wisdom.
Supplemental Material
sj-odt-1-jfn-10.1177_10748407241288606 – Supplemental material for “It Isn’t What I Had to Do, It’s What I Get to Do”: The Experiences of Black Family Caregivers Managing Dementia
Supplemental material, sj-odt-1-jfn-10.1177_10748407241288606 for “It Isn’t What I Had to Do, It’s What I Get to Do”: The Experiences of Black Family Caregivers Managing Dementia by Sheria G. Robinson-Lane, Florence U. Johnson, Marie Jeanne Tuyisenge, Jada Jackson, Tasneem Qurashi, Priya Tripathi and Bruno Giordani in Journal of Family Nursing
Footnotes
Acknowledgements
This work would be impossible without family members willing to share their stories. We thank you.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging [K01AG065420].
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.