
Abstract
Little is known about the lived experience of the dyad following a fetal death and the impact on relationships. The purpose of this paper is to explore the dyadic relationship between partners, with health care providers, and with the baby’s memory after birth. This qualitative study utilized hermeneutic phenomenology. The sample included 10 heterosexual dyads from the United States and Canada. All experienced a fetal death between 6 months and 7 years prior to their interviews. The data revealed three themes: (a) The Dyad Relationship: Moving Through the Experience Together; (b) Keeping the Memory Alive: Memorializing the Baby; and (c) Relationships With Health Care Providers: A Spectrum of Caring. The findings from this study provide the beginning knowledge needed to improve the care of dyads who have experienced a fetal death and for future studies to improve care delivery for dyads as their relationships change after fetal death.
Keywords
The experience of fetal death poses several challenges for parents. Following a fetal death, or pregnancy loss that occurs at a gestational age of greater than 20 weeks, dyads must navigate how that loss influences their relationship with each other and the memory of the baby as they grieve the loss (Gregory et al., 2021). One difficulty in adequately caring for families experiencing a fetal death is that it is often completely unexpected. In addition to the death being unexpected, fetal death does not occur frequently, occurring in 6 out of 1,000 live births (Gregory et al., 2021). The risk of fetal death further varies by race and ethnicity. In 2019, the rate of fetal death for non-Hispanic black women was 10.41(out of 1,000 births), and in non-Hispanic Native Hawaiian or Other Pacific Islander (NHOPI), it was 10.03 (out of 1,000 births). Non-Hispanic, White women’s rate of stillbirth was 4.71 out of 1,000 births in 2019 (Gregory et al., 2021).
As less than 1% of pregnancies result in a fetal death, little is known about the lived experience of the dyad following a fetal death and the impact on relationships. What is known related to the dyad experiences presents evidence that this experience may lead to alterations in the strength of marital relationships, difficulty with communication, differing experiences of grief, and limited support from partners (Avelin et al., 2013; King et al., 2021; Nuzum et al., 2018; Tseng et al., 2014). In addition to the marital relationship, another important relationship to understand to care for dyads experiencing fetal death is between the parents and the stillborn baby. Interactions in the hospital such as taking photographs, creating a memory box with footprints or hair, and holding or bathing the infant can help to memorialize the child (Cacciatore et al., 2013; King et al., 2021; Thornton et al., 2019). After hospitalization, King et al. (2021) also emphasized the importance of behaviors like celebrating the infant’s memory with birthdays or speaking often of the baby with other living children.
While beginning knowledge of maternal and paternal experiences with fetal death is available, more research is needed to guide and individualize care of the dyad after loss. The purpose of this paper is to explore the dyadic relationship between partners, with the baby’s memory after the birth, and with health care professionals (HCPs).
Method
To best understand the lived experience of a dyad following a fetal death and their relationships, a research approach utilizing van Manen’s (2017) hermeneutic phenomenology was selected for this study. A hermeneutic phenomenological design was identified as the basis of the study design and analysis as it guides scientists toward a better understanding of the individual experience and its impact on the whole person (Molley et al., 2018). van Manen’s method specifically includes determining a phenomenon of interest, investigating the experience as the individual lives it, and reflecting on the themes through writing and re-writing until the essence of the experience is truly captured. This method required the investigator to balance the data by considering parts as well as the whole which in this study led to viewing the individuals within a couple as a part of the whole dyad as the unit who experienced fetal death and the impact on relationships.
Data Collection Procedure
Prior to data collection, Institutional Review Board (IRB) approval was obtained from a university in the northeast of the United States. Dyads were recruited through regional and international organizations with a mission focused on helping families who have experienced perinatal or infant loss. The organizations shared recruiting materials on their social media and online newsletters and individuals interested in participation reached out directed to the first author. Inclusion criteria required all participants to identify as heterosexual, cisgender, English-speaking dyads who were of a minimum age of 18 years. All interested dyads were additionally required to have experienced a fetal death 6 months to 7 years prior to interviewing. Losses less than 6 months prior were deemed too close to the traumatic event to participate. The upper limit of 7 years was selected as the literature suggests trauma from pregnancy and pregnancy loss can be recalled long term while also acknowledging that time periods beyond 7 years would have had different resources like support through social media available (Beck & Watson, 2016; Takehara et al., 2014; Tseng et al., 2017).
Individuals who identified as lesbian women, gay men, and/or transgender dyads were excluded from participation. Additional exclusion criteria included dyads who had experienced fetal deaths more recently than 6 months ago and those who have gone through over 5 years of fertility treatment. These individuals and couples were excluded because, in becoming pregnant, both lesbian women and gay men and dyads requiring fertility treatments must invest a considerable amount of money and time in fertility treatments to achieve pregnancy. This additional effort, time, and resources can amplify emotions following a pregnancy loss (Hayman et al., 2015; Kim, 2017; Koser, 2019). Similarly, heterosexual dyads who undergo fertility treatment can face psychological distress and increased relationship strain when treatment extends over several years (Bhat & Byatt, 2016; Koser, 2019). Furthermore, the exclusion criteria of gay and lesbian dyads were used as gay men require the use of a surrogate to carry a pregnancy and in a lesbian dyad both partners may have the potential to experience pregnancy loss. The surrogate involved in parenthood for gay men adds an extra personal experience that may alter the grieving process (Kim, 2017). Transgender parents may also encounter complex legal challenges including the failure to recognize an individual’s name and gender, validation of marriages, and protection of reproduction rights through strong policy implementation and for this study were not included due to these possible influences impacting fetal death experiences (de Castro-Peraza et al., 2019).
Semi-structured interviews were conducted with each member of the dyad individually over Zoom. Data collection continued until saturation occurred, which was 10 dyads (20 individuals). The interviewer followed van Manen’s (2017) method using minimal questions in an interview guide, allowing participant responses to guide follow-up questions, and periods of silence or pauses followed by reframing last thoughts to elicit the lived experience of the phenomenon. Interview audio was recorded and transcribed promptly via Zoom by the primary investigator to enhance trustworthiness. Participants were not compensated for their participation.
Analysis
The primary and secondary investigators closely adhered to van Manen’s steps to consider the lived experience as shared by the participants as a whole, analyzed each line of the transcript thoroughly and iteratively, and identified repetitive thoughts and ideas. DeDoose®, an application for analyzing qualitative and mixed-methods data, was used to conduct data analysis (Salmona et al., 2020). In fitting with van Manen’s method, the primary investigator re-read the transcripts, then using coding methods including descriptive, in vivo, and emotion coding, the primary and secondary investigators performed the first round coding (Saldaña, 2021). The second round coding was then performed after half of the data were analyzed which decreased the initial coding list from 179 codes to 3 major themes that emerged from the data to answer the question, “what is the lived experience of relationships in a dyad following a fetal death?”
During the second cycle of coding, a review of shared codes across dyads within DeDoose® was performed to confirm that the analysis was reflective of the lived experience of the dyad and not the individual (Saldaña, 2021; van Manen, 2017). This confirmed that thematic representation was shared across male and female participants of the dyad. The evidence provided support that the experience being described was that of the dyad and not exclusive to one partner. Differences between the individual members of the dyad were explored as reflective of the shared lived experience.
Rigor, Trustworthiness, and Reflexivity
Maintaining standards of quality is pivotal to enhancing the trustworthiness of qualitative research (Stenfors et al., 2020). Data were first analyzed by the primary investigator and their dissertation chair followed by review by two additional committee members. Furthermore, member checking consisted of sending results to four participants for review, all of whom reported they agreed with the seven major themes after having the opportunity to provide feedback (Forero et al., 2018).
The primary investigator is a labor, birth, and postpartum nurse and has cared for dyads experiencing fetal death. As such, this led to and informed the phenomenon being chosen. During analysis as included in van Manen’s (2017) method, bracketing was performed to displace the investigator’s own beliefs while following his six activities.
Sample Demographics
Of the 10 dyads, 90% (n = 9) were married and 10% (n = 1) were divorced at the time of interviews. The currently divorced dyad was married at the time of the fetal death. The mean age in years at the time of the study was 37.2 with a range of 30 to 46 (n = 20). The mean age at time of loss in years was 33.7 with a range of 28 to 39 (n = 20). At the time of the interviews, the mean time elapsed since loss in years ranged from 6 months to 7 years with a mean of 3.3 years. The mean for number of pregnancies prior to loss was 1.4 (0-3). The mean for number of pregnancies after the loss was 1.5 (0-3). The mean number of living children was 1.9 (1-3). The mean gestational age at time of loss in weeks was 30.7 with a range of 21 to 39.5 weeks.
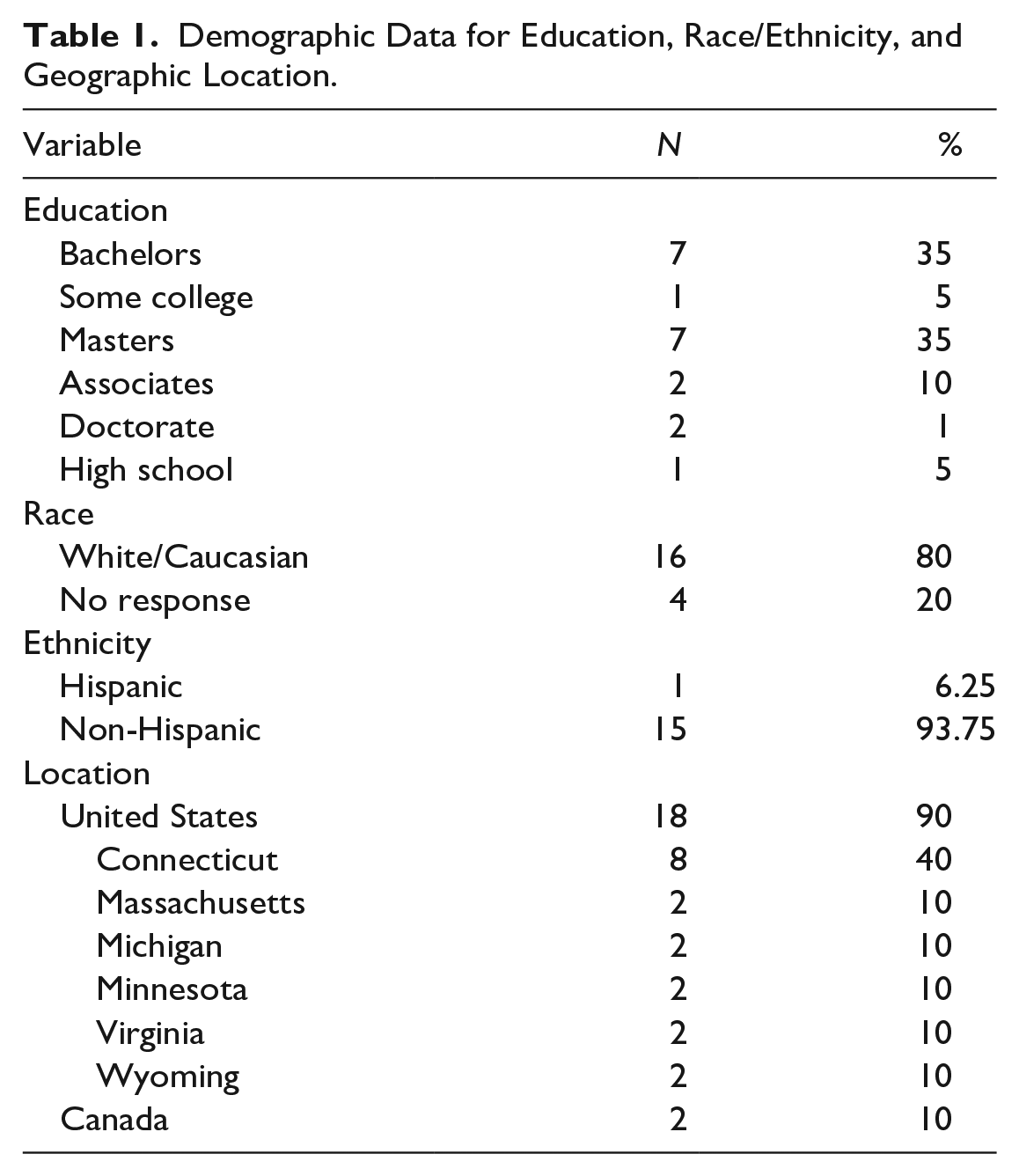
The sample demographics included national and international representation, with most of the sample (n = 9) reporting residence in the United States and 10% (n = 1) resided in Canada. Of the U.S. participants, 40% (n = 4) of dyads resided in Connecticut and the remaining sample (n = 5) were from either Massachusetts, Michigan, Minnesota, Virginia, or Wyoming. Of those who provided their race and ethnicity (n = 16), 100% were White/Caucasian and 93.75% were non-Hispanic. One participant identified as Hispanic. The participants in this study sample were highly educated. Notably, 10% (n = 2) had completed a high school degree or some college, 45% (n=9) had an associate or bachelor’s degree, and 45% (n = 9) had a master’s or doctoral degree. Demographic data are summarized in Table 1.
Demographic Data for Education, Race/Ethnicity, and Geographic Location.
Results
Three themes, each with subthemes, emerged during data analysis that described the lived experience of the dyad following a fetal death pertaining to experience in relationships. The themes were: (a) The Dyad Relationship: Moving Through the Experience Together; (b) Keeping the Memory Alive: Memorializing the Baby; and (c) Relationships With Health Care Providers: A Spectrum of Caring. In the following, the themes are discussed with representative quotes. Themes and subthemes of the participant experience of relationships are presented in Table 2.
Themes and Subthemes of Participant Experience of Relationships.

Theme 1: The Dyad Relationship: Moving Through the Experience Together
A major theme that emerged about relationships was the dyadic relationship and how they experienced their grief and healing together. All the dyads described periods that were challenging due to differences in grief expression followed by a shared journey that resulted in a stronger relationship. While each dyad member had their own grief trajectory and response, all the dyads remarked on the relationship with their partner as a pivotal piece of their healing. One participant described the uniqueness of this shared experience, “I just couldn’t imagine going through life with anybody else . . . we just truly have been through the depths of hell, and we came out of it together.”
Subtheme 1: Variations in Grief
This subtheme recognized that, while there is a common lived experience of fetal death among dyad members, there are variations in grief between everyone. Participants described ways in which societal expectations and timing of healing influenced differences in their experiences. Many male participants reported a need to be “strong” or wanting to “fix things” which affected their outward expression of grief. Several female participants shared they felt their husbands experienced that, too.
A male participant reported, “I was trying to be strong, for the kids and her, but I was worried about her. . . I felt I couldn’t let it get me too bad . . . I probably held it in,” another male reported feeling “a little bit of disconnect about how the grief affects us too.”
Female participants recounted how their expressions of grief varied and that nursing advice focused on societal expectations. One participant shared that hospital staff told her husband during the birth that “you need to be the support system for her, and you need to be you know tough.” Another female reflected and shared “I was much more like emotional, and he was more like, like instrumental in like, do, like doing things.”
Subtheme 2: Navigating the Experience
This subtheme described how individual experiences after the fetal death had differences related to the gender roles around the birth. Female participants reported their physical experiences after the birth influenced their grief and included reminders of the baby they lost. One female expressed, “My body thought I had a baby . . . so experiencing my milk coming in. Not only was emotionally difficult but, but physically very, very painful.” Another woman recounted that, “6-8 weeks after was probably the hardest mentally for me, that was like right around the time . . . my period came back.”
For some of the male participants, their experience differed due to lost hope of a relationship with their son. One participant remembered how “it hadn’t gotten to the point where I had even felt him kick . . . But I had that like excitement of [having] a son.” Another recounted that for him, “mourning the loss of like, my son as he was not like, of all the possible things made it, made it an easier process for me.”
While there were individual experiences the dyad had to interpret as they navigated grief, there were several things that because they had each other made things better. Participants shared that their partners were instrumental to the healing. One female participant shared her husband was her “rock through all this. He’s amazing.” Similarly, a male participant recounted that even after experiencing this he “couldn’t imagine going through life with anybody else. [She] truly understands me to the core, more so than she did even as when we set our I do’s.”
Subtheme 3: Perception of the Partner’s Experience
An interesting subtheme that emerged as the participants were interviewed individually was the partner’s perception of the other’s experience. Each participant reflected on what they thought their partner’s experience was which described the dyad response in a unique light. Participants shared they felt the partner was often forgotten by others and that they wished they understood more about the partner’s grief experience. Many participants remembered the imbalance of support and said, “there’s a lot more resources that are given to the mother. Fathers, fathers are very much, um, I wanna say ignored” or “I really do feel sorry for the fathers, because I think the emphasis is always put on the mothers.” In addition, male participants reflected that the physical experiences of pain and reminders of birth that their wives endured were difficult to comprehend. For example, one male recalled that his wife’s experience was “the same experience I had multiplied by X. I don’t know what the X is. But it was a much more horrific version of what I experienced.”
Subtheme 4: For Better or Worse
This subtheme explored the ways the relationship shifted during the period after a fetal death. Dyads described the initial difficulty, then periods of improved communication, and ultimately for many a strengthened relationship. Examples of this were one participant who shared it “hard for us, both when the other didn’t like grieve the same way” or how a different participant’s partner experienced a lot of “anger” which was “not going to bring him back . . . it’s just going to cause problems with us.” One female recalled their relationship strain and shared that their partner “became extremely anxious and extremely depressed” and how they “were fighting a lot.”
After the periods of difficulty, though, there were positive experiences within the relationship. Many dyads reported their communication “improved” and relationships were “strengthened” following the fetal death. One participant shared “We know each other, a little bit better. And like now our relationship is very, very solid.” Another mentioned that he “would say that that probably would have made us stronger.” Despite the difficulty and immense grief, the dyads experienced, a shared experience united partners that one participant reflected “keeps us close together because we forever have that bond of our child.”
Theme 2: Keeping the Memory Alive: Memorializing the Baby
Overwhelmingly, the dyads reported how maintaining the relationship with the baby was an important part of the experience of pregnancy loss and their healing. That relationship began during the pregnancy and continued through the hospital experience and beyond into their grief journey. A common theme discussed by all 10 dyads focused on the importance of integrating the infant’s memory into their lives as a way of having a relationship with the deceased.
Subtheme 1: Reflecting on the Birthing Experience
Dyads described the delicate balance of wanting to spend as much time as possible with their child but knowing at some point they would need to say goodbye and send the baby to the morgue. This brief period included holding and bonding with the infant. This time with the baby was the only time dyads had to establish a relationship with the physical appearance and feeling of their baby. Unfortunately, for many, their time was limited due to the influence of time on their baby’s appearance. Most dyads kept their baby with them between 6 and 24 hours. Once they decided, it was time to say their physical goodbye in the hospital dyads recounted intense emotional experiences. One participant shared it was “by far the most difficult thing that I’ve ever said in my life. Because I didn’t, I even, even with him not being alive, I could not let [him] go.” Another reflected, “I knew what I was getting into that like dead babies don’t like get better over time.” Her husband remembered, “in total, we probably had six or so hours where we were with him. And then you know we let the nurses take him away, and by that point we were just wrecked.”
Subtheme 2: Honoring the Baby’s Memory
This process honored that the infant was a real member of the family to siblings and a child to the parents. One way the relationship with the baby was maintained included using the child’s name. Many participants shared how using their baby’s name or/and “asking questions” about the child made them feel real and valued. An example of this is a participant who appreciated people who spoke of her son and that “even though he wasn’t full term I held him in my arms, and he looked like my husband. He’s very real, to me.” To honor their baby, some dyads did not change the nursery or create new holiday traditions. One participant shared they kept the nursery “pretty close to where it was for almost a year,” whereas another mentioned at Christmas they “have special ornaments we hang high up on the tree for them.” Another participant reflected how on the birthday they often did “something special that day” and have “done a balloon release” to honor their deceased son’s life and maintain a relationship of his memory.
Others discuss how they light a candle, have special objects that remind them of the infant, or got tattoos to maintain a relationship with the infant. Tangible objects to honor the deceased baby were common to maintain a closeness. One male had their son’s ashes in his bedroom dresser and “tap(s) that every day” to feel close to the child. Others recounted how they have jewelry to remember their child. One participant reflected that she and her husband have necklaces they wear daily. Her necklace has “his handprint and his handprints” and her husband “has a necklace that is a dog tag that has [our baby’s] picture on it.” One male described how their wife also “has a necklace with a little bit of the remains in it the heart of the little handprint or footprint.”
Theme 3: Relationship With Health Care Providers: A Spectrum of Caring
A significant theme that emerged from the data was related to the experience the dyads had in relationship with health care providers following fetal death. Interactions with health care providers were hugely influential at the time of loss and were similar regardless of geographical location. The quality of these interactions had an impact on how the dyad experienced the loss and how they experienced the subsequent grief. Dyads also described the influence of the loss on later interactions and relationships with health care providers. This was often described in relation to future pregnancies and follow-up care.
Subtheme 1: Positive Connection That Carried us Through
Several participants described positive relationships and interactions with health care providers during the time of the loss. These experiences were described as creating a sense of “trust and appreciation.” Some participants described a connection and relationship with a specific nurse or obstetrical (OB) provider who they perceived as “kind,” “compassionate,” and “amazing.” Often these providers were described as serving as an extra source of comfort and strength at a time when it was most needed. One participant recalled “fondly” the experience he had connecting with one nurse, “we both kind of like locked on to her, this is the person in charge.” Another also described, “We were given the most amazing nurse, ever, she was absolutely fantastic . . . She was just like so empathetic and compassionate from the beginning and that meant a lot me.”
In some cases, the positive relationship with the health care provider preexisted the loss experience. Some described encountering the same nurse who had been present at the birth of an older child, “Yes, there was something. Kind of divine intervention in then in that regard because it definitely helped ground the moment I think it, it allowed us to let our guard down a little more, we were comfortable with the people.” One participant also recalled the team calling her own OB to confirm the bad news that their baby had died, “It wasn’t going to change, but just I think we’re on peace of mind, have like our doctor look.” In these cases, participants described a trust in feeling known by the provider which provided a sense of comfort in their experience.
Caring nurses and other health care providers served as a calm and compassionate guide during a time that was chaotic, overwhelming, and filled with emotion. One female participant recalled, “She just cared about my comfort she gave us a nice amount of space to be alone in grief, but also, I never felt abandoned by her it was just a really beautiful art.” Many dyads described the important role that nurse played in helping to make the most of the limited time available to bond with their child. Several families described nurses encouraging them to take pictures of and with their child. In some cases, participants described not realizing at the time that this is something that would later provide great comfort and shared, “they did take pictures and they put them in a memory box . . . I am very grateful they did.” Another also recounted this appreciation of the nurse encouraging pictures, “that was probably one of the best gifts like that nurse ever could have done for us. I wouldn’t have thought to take pictures, and certainly not of a dead baby, but I am so thankful that she did that for us.”
Subtheme 2: Uncaring Providers and Increased Pain
While positive interactions with caring, compassionate health care providers provided great comfort, participants also recalled receiving care from providers who were uncaring. Some participants described interactions that felt rushed or transactional, while others described individual health care providers as “inappropriate,” “terrible,” and “overbearing.”
Some participants reflected upon challenging relationships with health care providers who both rushed them and appeared detached from the participants’ emotions. Almost immediately after receiving the bad news of the loss of their child, participants were forced to make decisions to guide their care and to plan for the management of their child’s remains. For some, caring providers helped to make these decisions manageable, for others a lack of caring contributed to mistakes, miscommunications, and regrets. This is highlighted by one male’s recount of being forced to quickly fill out paperwork right after finding out that his child had died. “I literally just didn’t know . . . what they were handing me . . . I didn’t care, you know the only thing I cared about was what was happening to [my wife and daughter].” Another male also shared how the care received by doctors and nurses further contributed to the pain of his and his wife’s experience, “yeah, the hospital experience, I understand your doctor is going to be kind of detached . . . But at times it’s not helpful. Like from an emotional standpoint.” One female participant described her experience laboring overnight alone under the care of a nurse who seemed both bothered by and callous to her needs. The nurse was notably absent for most of the night and when the female rang to ask for help, there was the perception of impatience, uncaring, and attitude that contributed to added pain. This participant reflected, “It was just like . . . is this really how you treat people when they’re going through something like this?”
Subtheme 3: Change in Health Care Relationships After Loss
The experience of fetal death continued to impact participants’ relationships with health care providers following the initial hospitalization or procedure. Many participants described a change in the dynamic of their expectations in health care encounters and an added need for sensitive and compassionate care. In many cases, these expectations were influenced heavily by those initial relationships immediately following loss. For those who had a positive experience, they were able to develop future relationships with health care providers with an expectation for caring and compassion. For others, who had negative health care experiences, future encounters were clouded by a lack of trust and a sense of needing to strongly advocate for self.
Numerous participants described the desire to have health care providers “read their chart” prior to interacting with them. Participants described encounters during prenatal visits, ultrasound appointments, and with other providers, where the providers’ lack of knowledge of their loss contributed to inappropriate questions, comments, and ultimately added grief. One female recalled a prenatal appointment for care for a pregnancy after experiencing fetal loss where her provider said “oh, didn’t you just have a baby . . . a slight pause, how’s that going,” and I said, “well not too good cause she’s dead.”
Some participants were able to continue to sustain a positive health care provider relationship following the loss. Participants described staying with an OB practice for subsequent pregnancies or returning to the same hospital for a future delivery. The initial experience increased their trust and deepened the connection in these relationships. As stated by one female, “The OB I’m seeing for this pregnancy, is actually pregnant, that the OB who did surgery for my son. And she’s so compassionate and amazing as well.” Providers who knew the participants well and brought to the relationship an understanding of their loss were better able to manage the ongoing grief and at times anxiety that was brought into future pregnancies.
Discussion
This study adds further information about the experience of the partner after a fetal death and an insight into relationship changes bereavement can cause. Fetal death is an experience that is life changing for dyads and these findings echo King et al.’s (2021) in that the emotional pain of losing a child and the juxtaposition of death in a ward surrounded by life is unfair and a pain without reward. As reported in other studies, these findings support the fact that dyadic relationships following perinatal loss may initially experience difficulties but over time result in a stronger bond due to the shared experience (Avelin et al., 2013; Hutti et al., 2015; Paris et al., 2016; Tseng et al., 2017). By viewing the lived experience from the lens of the dyad, variations in grief journeys related to physical differences and societal influences were explored which reflect findings in other literature about males feeling as though they had to be strong (King et al., 2021; Miller et al., 2019). At the time of publication, other studies about couples and their experiences with fetal death did not directly address the perception of the partner’s experience of the death.
Activities such as bathing, taking pictures of, and holding the baby can assist dyads to create a relationship with the deceased baby and provide tangible artifacts to reflect upon to remember that though the child was not born living, they had a meaningful impact on their lives (King et al., 2021; Thornton et al., 2019). Nurses are in a unique position to serve as facilitators in the creation of these memories. As Bakhbakhi et al. (2017) emphasized the importance of providing families time to process the news, counseling patients on how the activities that help create memories of the child should also be provided to individuals as they make decisions about photography or holding the infant. The literature consistently supports the significance of these memorializing activities, a finding that is further reinforced by the participants in this study. Given the importance of nurses’ caring actions in this sample and in the literature, continuing education about care of the dyad during a fetal death should be incorporated into hospital administration requirements for labor and delivery and postpartum nurses (Nurse-Clarke, 2021).
Participants shared how while there were some things done very well by their nurses and providers, there is still room for improvement in health care delivery surrounding a fetal death. Some participants shared how nurses left welcome packets with breastfeeding information and newborn care in the hospital room. Others shared feeling rushed to make decisions regarding the disposition of fetal remains. These examples support the need for standardized approaches to caring for dyads experiencing fetal death with clear guidelines or policies following best practices (Boyle et al., 2020; Leitao et al., 2021; Sousou & Smart, 2015). The findings and existing literature support the need for further research that could identify best practices for nursing interventions in caring for dyads experiencing fetal death, such as a checklist to prepare rooms on the maternity unit to remove triggering pamphlets or photos and a timeline of events to not rush dyads or families off the unit.
There were many strengths to this study. First, the findings of this study provide emerging data about the experience of a heterosexual dyad following a fetal death. As King et al. (2021) discussed there is a need to investigate dyads who are no longer in a relationship, this study includes one dyad who was divorced who’s experiences after the fetal death were like the other participants. Including a dyad who was divorced is a strength of this study as their experience still paralleled the other participants despite their relationship breaking up after the death. Second, some participants in this study experienced pregnancy, fetal death, and perinatal bereavement during the COVID-19 pandemic. This subset of participants provides insight into a growing amount of literature about how the pandemic influenced pregnancy experiences of both normal and high-risk births and pregnancy loss (Cena et al., 2022; Silverio et al., 2021). Third, individual interviews encouraged each partner to share their experience without the influence of the other during their interview and to prevent one participant from talking more than the other which King et al. (2021) reported in their study on couples who experienced stillbirth. Finally, the 10 dyads lived in various states across the United States, and one lived in Canada. This diverse geographical representation showed that, despite differing locations, the lived experience included several shared similarities.
Limitations
Weaknesses of this study include the demographics. The sample was homogeneous and almost entirely white, non-Hispanic participants. As discussed in the background, this population is least likely to experience this phenomenon with 4.71 out of 1,000 live births resulting in fetal death, whereas people of color are about twice as likely to experience fetal death (Gregory et al., 2021). The sample was also homogeneous in that all but one dyad was still married after experiencing fetal death. Evidence suggests that parents who experience parental bereavement are at an increased risk for disruption to their relationships and divorce than the non-bereaved (Bolton et al., 2014; October et al., 2018). This sample is therefore not completely representative of the population at large who experience fetal death and parental bereavement which can limit the transferability of the findings.
In addition, only heterosexual dyads were included in the sample which is also not entirely representative of the population of childbearing individuals and their partners. The authors, however, recognize that stories exist of fetal death in same-sex and transgender couples that are important to investigate in the future. Finally, sampling from dyads only and not individuals impacted the sample as there were interested women who were not able to participate as their partners were not interested.
Conclusion
Dyads experiencing fetal death require compassion, empathy, and support from diagnosis through the bereavement period. The findings of this study suggest that there are individuals and dyads who have experienced this traumatic and unique type of loss that are willing to share their stories to help others and memorialize their baby. Many participants once the interviews were complete shared that they were grateful for the interest in this phenomenon and for the investigator’s desire to hear about their story and baby. The findings also support the need for further investigation into the experience of individuals, dyads, and families who have lost a child to fetal death.
Footnotes
Acknowledgements
I would like to acknowledge Dr. Amy Smith and Dr. Nancy Dluhy for their guidance during my doctoral dissertation from which this manuscript was derived.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.