
Abstract
This review aimed to identify and synthesize empowering support for the family members of patients in the acute phase of traumatic brain injury hospital treatment. CINAHL, PubMed, Scopus, and Medic databases were searched from 2010 to 2021. Twenty studies met the inclusion criteria. Each article was critically appraised using the Joanna Briggs Institute Critical Appraisals Tools. Following a thematic analysis, four main themes were identified about the process of empowering traumatic brain injury patients’ family members in the acute phases of hospital care: (a) needs-based informational, (b) participatory, (c) competent and interprofessional, and (d) community support. This review of findings may be utilized in future studies focusing on designing, implementing, and evaluating an empowerment support model for the traumatic brain injury patient’s family members in the acute care hospitalization to strengthen the current knowledge and develop nursing practices.
Keywords
Traumatic brain injury (TBI) is functional or structural damage to the brain caused by a sudden external injury. TBI can be classified as a mild, moderate, or severe brain injury. Moderate and severe brain injuries in the acute phase often require hospital treatment (Capizzi et al., 2020). Approximately 5.3 million people in the United States and 7.7 million people in the European Union (G. Liu et al., 2021) suffer from various symptoms and problems caused by a TBI, including impaired attention, difficulty with memory, depression, impulsivity, poor decision-making, aggressive behavior, slowness, fatigue, and mental disorders (Capizzi et al., 2020; Rasmussen et al., 2020). A considerable number of people with brain injuries are below 25 years old, although brain injuries have also increased among older people (Nguyen et al., 2016). After hospital discharge, family members (FMs) are often the primary caregivers for a TBI survivor, offering daily support and executing demanding care procedures (McIntyre et al., 2020). FMs must adapt to this new, unexpected role (McIntyre et al., 2020), and as a result, they often experience difficulties managing the TBI survivor care process (Kivunja et al., 2018), and need empowering support (Sakanashi & Fujita, 2017). Based on the literature, TBIs are a global health problem (Maas et al., 2017), and the number of brain injuries is constantly increasing (Jochems et al., 2021). Therefore, it can be assumed that the number of FMs and caregivers will also increase in the future.
Background
Empowering the FMs of TBI patients has received little attention in nursing science. Most previous studies have focused on the needs of FMs (de Goumoëns et al., 2018; Kreutzer et al., 2018) and the relationships between life satisfaction (Manskow et al., 2017), perceived burden (Doser & Norup, 2016), and the functioning of the TBI patient and FMs after hospitalization. These studies reported FM’s unfulfilled needs in the acute phase of TBI patient care were related to insufficient emotional support, professional support, and involvement with care (de Goumoëns et al., 2018). In addition, research has reported that FMs’ needs do not decrease over time but actually increase (Anke et al., 2020; de Goumoëns et al., 2018). Furthermore, FMs’ feelings of burden (Doser & Norup, 2016) and depression increased and were related to decreased life satisfaction (Manskow et al., 2017), especially in the context of severe brain injury (Rasmussen et al., 2020). Therefore, professionals should recognize and attend to the needs of FMs in the acute phases of TBI to better support and empower FMs in order to prevent these negative consequences for the individual and the family.
Empowerment is a mutual process multidimensional concept that has been defined in several disciplines, including education, politics (Mehta & Sharma, 2014), social sciences (Rubin & Babbie, 2016), psychology (Jones et al., 2011), feminist studies (Rodwell, 1996), and nursing science (Friend & Sieloff, 2018; Wåhlin, 2017). In nursing science, the concept of empowerment has been studied from the perspectives of patients (Ania-Gonzalez et al., 2022), health care professionals (Papathanasiou et al., 2014), and management (Garcia-Sierra & Fernandez-Castro, 2018), but less from the viewpoint of TBI patients and their FMs.
Empowerment has been described both as a process and an outcome (Friend & Sieloff, 2018). Empowerment as a process means offering hope and confidence and encouraging people to promote their well-being, decision-making, and self-management (Chen & Li, 2009). Empowerment as an outcome, in turn, means that the individual feels able to manage and control their situation (Sakanashi & Fujita, 2017). From an empowerment perspective, FMs require support, knowledge, and guidance from the health care professionals during the acute phase of TBI patient hospital care (Sakanashi & Fujita, 2017) to manage the complex, life-changing situation and adapt to it (Kreutzer et al., 2018). Empowerment of FMs requires that the information a health care professional provides is multifaceted and corresponds to the FM’s expectations and needs in a manner that can also benefit decision-making (Sigurdardottir et al., 2015). Qualities such as authenticity, communication, listening, and equality are needed for an empowered mutual relationship between families and health care professionals, with acceptance and support being the key factors thereby creating an atmosphere where FMs can express their feelings and concerns (Wåhlin, 2017).
The key elements of providing empowering support to FMs relate to equal and trustful relationships between the professionals and the FMs (Sakanashi & Fujita, 2017). FMs can develop a positive belief in themselves and the future in this process. Professional competence to support FMs in achieving the skills needed to manage TBI survivors’ care independently after hospitalization and to overcome challenges through guidance and emotional support are also important in the empowerment process. Furthermore, health care professionals must meet FM’s needs and expectations with the knowledge to reach potential empowerment (Funnell et al., 1991; Nygårdh et al., 2012; Wåhlin, 2017).
Previous systematic reviews have examined the experiences, requests for support, and needs of FMs of TBI patients in the hospital (Coco et al., 2011; Oyesanya, 2017; Wetzig & Mitchell, 2017). According to recent studies (de Goumoëns et al., 2018; Doser & Norup, 2016; Manskow et al., 2017), FMs reported that they did not receive enough information, support, and guidance from health care professionals. As a result, FMs experienced a long-term feeling of burden and a reduced quality of life. There is a gap in the available knowledge from the perspective of providing empowering support for FMs in the acute phase of TBI patients’ hospital treatment. Moreover, there is a lack of nursing recommendations and structured care procedures prepared to support FMs in the acute phase of TBI patients’ hospital treatment.
Research focusing on empowering support for FMs in the acute phase of TBI patient care is significant, both for increasing health care professionals’ awareness of FMs’ needs and for improving care procedures to support and empower FMs experiencing the TBI of a loved one.
This systematic review aimed to identify, critically evaluate, and synthesize available evidence of empowering support for FMs in the acute phase of TBI patient hospital treatment, including emergency care, intensive care unit (ICU) care, and inpatient care. Specifically, we wanted to (a) identify factors that contribute to FMs’ empowerment and (b) understand the empowering support from the perspective of FMs of TBI patients. The research question that guided this study was: What is empowering support for the FMs of TBI patients in the acute phase of TBI patient hospital treatment, and what are the influencing factors?
Method
Design
This mixed-methods systematic review explored FMs’ perspective of empowering support in the acute phase of TBI patients’ hospitalization. A convergent integrated design approach was chosen because it enables gathering information about the care procedures that families found helpful and also explored the experiences of FMs to better understand these multifaceted phenomena (Grant & Booth, 2009; Lizarondo et al., 2020). The population, intervention, control, and outcomes format was used for framing the research question (Aslam & Emmanuel, 2010). The literature review was conducted and reported using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021) (see Online Supplementary File 1).
Search Methods
We performed the systematic data retrieval by dividing the research question into thematic entities to define key concepts and construe search terms. We conducted searches in the CINAHL, PubMed, Scopus, and Medic databases; the process also included testing and combining Medical Subject Headings terms. The search strategy with phrases variations is provided in Table 1.
Search Strategies for the Systematic Mixed Methods Review.
An information specialist’s expertise was used to improve the data set coverage and reliability in the data retrieval process. Inclusion criteria were studies involving adults over 18 years old; the patient’s and FMs’ experiences of TBI; and needs of FMs for support during the acute phase of treatment. In addition, the health care professional’s supportive approaches, nursing practices, and nursing interventions from the perspective of FMs’ empowerment were also examined. Furthermore, factors related to empowering TBI patients’ FMs in the acute phases of hospital treatment were included. In order to obtain a more comprehensive synthesis, numerous qualitative, quantitative, RCT, and mixed methods studies were screened. Exclusion criteria included non-traumatic brain injuries, FMs’ experiences and needs of children with TBI literature reviews, medical intervention, rehabilitation, and outpatient care. Data retrieval was limited to peer-reviewed research articles in English. We did not include gray literature in the data retrieval process. The time period included in all database searches was 12 years (2010–2021). Table 2 presents the criteria for inclusion and exclusion of studies in the review.
Inclusion and Exclusion Criteria of the Search Strategy.
Note. PICO = population, intervention, control, and outcomes; TBI = traumatic brain injury.
Study Selection and Data Extraction
The literature selection process proceeded in two phases. The first author (JL) independently carried out report retrieval for the study. In the first phase, duplicates and records marked as ineligible by the automation tool were removed. According to the inclusion and exclusion criteria, two researchers (JL and KC) independently selected studies based on the title and the abstract. Covidence program was used (Kellermeyer et al., 2018) for data extraction. The second phase included reading each study and re-checking whether the study answered the research question and fulfilled the inclusion criteria. Any possible disagreements were discussed with the other members of the research group (TV and HT) to reach a consensus and make the decisions.
Data Analysis
A thematic analysis was used to analyze and synthesize the findings; the review included qualitative, quantitative, and mixed methods designs. The studies were read, familiarized, and coded by forming a narrative interpretation of the quantitative results (Lizarondo et al., 2020; Vaismoradi et al., 2013). Each publication was analyzed to find expressions describing the FMs’ experiences of receiving empowering support in the acute phase of TBI patient’s hospital treatment. Some of these expressions offered by FMs were narratives (e.g., “. . .need for continuity of care. . .so it has all been taken care of and then you can free your time to go to work”), and some were phrases (e.g., “to receive concrete information on the brain injury and its effect on the future at an early stage”), and some were single words (e.g., “. . .empowerment processes. . .”). These meaningful expressions formed a basis for data reduction, categorization, and abstraction. After this, similar reduced expressions were grouped into categories by comparing their similarities and differences. Categories with similar content were grouped as a subtheme with a name that described the content (e.g., information about TBI patients’ health conditions in the acute phase). The subthemes were then grouped into higher-level categories and main themes (e.g., informational support to empower the FMs) (Elo et al., 2014); (see Online Supplementary File 2).
Two reviewers (JL and KC) independently appraised the methodological quality of the studies and performed the quality assessment using Joanna Briggs Institute (JBI) Critical Appraisals Tools: (a) Checklist for Qualitative Research and (b) Checklist for Analytical Cross-Sectional Studies. The JBI critical appraisal checklist includes 10 criteria for qualitative studies and 8 criteria for quantitative studies, addressing the risk of bias in its design, conduct, and analysis (Moola et al., 2020). For each study, two reviewers completed the appraisal step (each reviewer rated each study “Yes,” “No,” “Unclear,” or “Not applicable”). In my opinion, this sentence can be removed here, as it will come up in the next section “Description of Included Studies”. The studies’ strengths were related to a clear description of the research methodology, data collection methods, and data analysis. The inclusion and exclusion criteria of the sample were also clearly described, including the study’s subjects and settings. Weaknesses in reviewed studies related to the lack of description of potential confounding factors and strategies to control them. In total, the selected studies (N = 20) were generally of good quality and were not excluded based on their quality assessment.
Results
Study Selection
At the first stage of the data retrieval process, the number of hits within the search limits was 1500. After removing duplicates and records marked as ineligible, 907 articles remained. Of these, 873 articles were excluded based on the title and the abstract. This selection process resulted in 34 articles. After the full texts were read, 14 articles were excluded. The main reason the interventions were excluded was that they were not nursing interventions; if they were, they did not focus on the acute phase of hospital treatment or provide a perspective of the FMs. Finally, 20 original research articles were selected for review after completing the data retrieval process and the parallel analysis. Figure 1 illustrates the search selection process using a PRISMA flowchart.
PRISMA Flowchart of the Selection of Included Articles (Page et al., 2021).
Description of Included Studies
Table 3 presents the selected research articles and highlights the studies’ characteristics and quality. Overall, the majority of the selected studies used a qualitative design (n = 10): Abrahamson et al., 2017; Adams & Dahdah, 2016; Degeneffe & Bursnall, 2015; Gan et al., 2010; Holloway et al., 2019; Keenan & Joseph, 2010; Kreitzer et al., 2019; Lefebvre & Levert, 2012a, 2012b; and Schutz et al., 2017. A cross-sectional design was used in eight research reports: (Arango-Lasprilla et al., 2010; Calvete & Arroyabe, 2012; Choustikova et al., 2020; de Goumoëns et al., 2019; Dillahunt-Aspillaga et al., 2013; Doyle et al., 2013; W. Liu et al., 2015; and Norup et al., 2015). The remaining studies used a mixed-methods design (n = 2): (Bellon et al., 2015; Kanmani & Raju, 2019).
Characteristics of the Studies Selected in This Review (n = 20).
Note. TBI = traumatic brain injury; ABI = acquired brain injury; BIAF = The Brain Injury Association of Florida.
Qualitative study = Quality score of JBI (Joanna Briggs Institute) critical appraisal checklist, including 10 criteria to assess the methodological quality of qualitative studies. bCross-sectional study = Quality score of JBI (Joanna Briggs Institute) critical appraisal checklist, including 8 criteria to assess the methodological quality of cross-sectional studies.
Most studies were conducted in the United States (n = 7), Canada (n = 4), and the United Kingdom (n = 2). The remaining seven studies were from Australia (n = 1), Spain (n = 1), Finland (n = 11), Switzerland (n = 11), India (n = 11), China (n = 1), and Denmark (n = 1). Most studies focused on FMs’ experiences of empowering support (n = 15). However, five studies discussed the perspective of empowerment more broadly, such as from the perspective of TBI patients and health care professionals.
Synthesis of Results
Data synthesis with an integrated approach was used. Based on convergent results of the systematic literature review, empowering support for FMs in the acute phase of TBI patient hospital care is based on four main themes of the empowerment process: (a) needs-based informational support, (b) participatory support, (c) competent and interprofessional support, and (d) community support (see Figure 2).
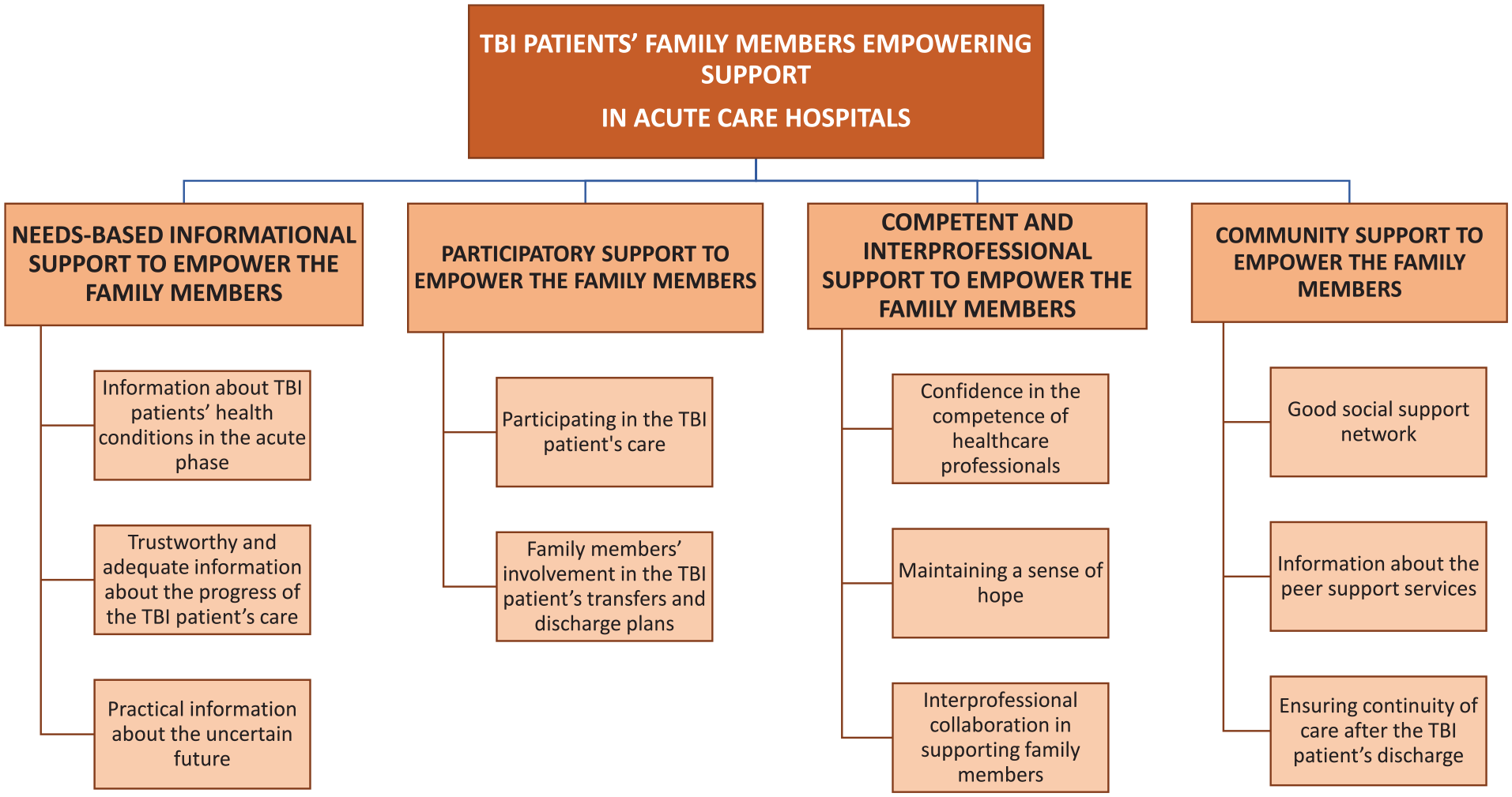
Illustration of Traumatic Brain Injury Patients’ Family Members’ Empowerment in Acute Care Hospitals.
Theme 1: Needs-Based Informational Support to Empower the FMs
The FMs’ most pressing need was identified as a need for information during the acute phase of TBI patients’ hospital care, which lasted throughout the patient’s hospital treatment, from emergency care to discharge (Keenan & Joseph, 2010; Kreitzer et al., 2019; Lefebvre & Levert, 2012a). However, FMs’ needs and ability to acquire information changed over time (Keenan & Joseph, 2010; Lefebvre & Levert, 2012a). For example, during emergency care and intensive care, the members of the family needed information focused on the TBI patient’s health conditions, medical treatment, and recovery (Doyle et al., 2013; Lefebvre & Levert, 2012a; W. Liu et al., 2015). In the inpatient ward, the FMs’ need for information focused more on practical issues and future plans (Keenan & Joseph, 2010; Lefebvre & Levert, 2012a). Although the FMs’ need for information changed over time, to empower the FMs, the information needed be trustworthy, versatile, and consistent (de Goumoëns et al., 2019; Gan et al., 2010; Lefebvre & Levert, 2012b).
Needs-based informational support to empower FMs contained three sub-themes: information about TBI patients’ health conditions in the acute phase, trustworthy and adequate information about the progress of the TBI patients’ care, and practical information about the uncertain future.
Information about TBI patients’ health conditions in the acute phase described the importance for FMs to have an early diagnosis of the patient’s brain injury (Choustikova et al., 2020; Gan et al., 2010). FMs wished to receive factual information about the accident (Keenan & Joseph, 2010), the brain injury, and its effect on the future (Bellon et al., 2015) at an early stage (Kanmani & Raju, 2019). If FMs felt they were receiving too little information from health care professionals, they would seek more information online or from their friends and relatives (Lefebvre & Levert, 2012a). Receiving sufficient information about the symptoms of TBI such as memory disorders (Arango-Lasprilla et al., 2010), emotional problems (Abrahamson et al., 2017), and changes in mood and personality (Adams & Dahdah, 2016; Calvete & Arroyabe, 2012; Gan et al., 2010; Kreitzer et al., 2019), helped FMs to understand, for example, why their relative with TBI displayed changes in behavior (Degeneffe & Bursnall, 2015). In addition, FMs wished to receive information on the TBI patient’s medical care (Doyle et al., 2013; Lefebvre & Levert, 2012a; W. Liu et al., 2015), and they needed reassurance that the patient received all necessary medical care (Gan et al., 2010).
FMs wanted trustworthy and adequate information about the progress of the TBI patient’s care, such as any changes in the TBI patient’s condition, and that all questions were answered honestly (Kreitzer et al., 2019; Lefebvre & Levert, 2012b) and professionally (Keenan & Joseph, 2010). FMs hoped that hospital staff would always be honest with them, even when the patient’s condition worsened. The research demonstrated that honesty was seen as a characteristic of professionalism that promoted the development of a trusting relationship between FMs and health care professionals (Keenan & Joseph, 2010; Kreitzer et al., 2019; Lefebvre & Levert, 2012b). FMs could better understand the purpose of their relative’s care if the information was conveyed in a peaceful environment with sufficient processing time (de Goumoëns et al., 2019). The information also needed to be provided in oral form (Gan et al., 2010; Lefebvre & Levert, 2012b) and written form (Choustikova et al., 2020). In addition, from the empowerment perspective, FMs wished to receive regular patient updates (Keenan & Joseph, 2010; Lefebvre & Levert, 2012b) that were specific to their relative and not based on general statistics and probabilities in order to utilize the information in their decision-making (Keenan & Joseph, 2010).
FMs needed practical information about the uncertain future after the TBI patient had left the ICU and the situation had stabilized (Lefebvre & Levert, 2012a). FMs’ needs for information shifted from damages the accident caused and medical care to planning for the future (Keenan & Joseph, 2010). In the inpatient ward, FMs’ needs focused on receiving sufficient guidance (Choustikova et al., 2020) and support for practical issues such as organizing extended hospital visits and managing financial matters (Abrahamson et al., 2017). At this point, FMs started to realize they had to attend to other obligations such as family (Adams & Dahdah, 2016; Arango-Lasprilla et al., 2010), work, and community life (Keenan & Joseph, 2010). FMs frequently wondered how TBI would affect the patient’s life in the areas of work (Calvete & Arroyabe, 2012), independence (Degeneffe & Bursnall, 2015), family activities (Dillahunt-Aspillaga et al., 2013; Gan et al., 2010; Holloway et al., 2019) and marriage (Lefebvre & Levert, 2012a). FMs also needed support and information about taking care of themselves, for example, by taking a break from the care, problems, and responsibilities (Doyle et al., 2013). In the inpatient ward, FMs were interested in finding out about available services (Kreitzer et al., 2019) and resources (Adams & Dahdah, 2016) to ease their social adaptation as well as to promote the family’s independence and coping after hospital discharge (Lefebvre & Levert, 2012a).
Theme 2: Participatory Support to Empower the FMs
Uncertainty and concern about the patient’s survival increased the FMs’ feelings of powerlessness and, arguably, their need to participate in the patient’s care (Bellon et al., 2015; de Goumoëns et al., 2019; Keenan & Joseph, 2010). To empower the FMs, the professionals must recognize them as an integral part of the TBI patient’s comprehensive nursing process (Degeneffe & Bursnall, 2015). Being close to the patient was the primary way for FMs to participate in the patient’s care (Keenan & Joseph, 2010). However, concretely participating in the patient’s care through the nursing procedures and the patient’s transfers and discharge plans was also important for empowering FMs (Lefebvre & Levert, 2012a; W. Liu et al., 2015; Norup et al., 2015).
This theme included two sub-themes: participating in the TBI patient’s care and FMs’ involvement in the TBI patient’s transfers and discharge plans.
By participating in the TBI patient’s care, FMs reported feeling part of the patient’s holistic care (Calvete & Arroyabe, 2012) and nursing process (Degeneffe & Bursnall, 2015). This, in turn, promoted the FMs’ understanding of the situation and future (Bellon et al., 2015; de Goumoëns et al., 2019) and helped to identify their abilities, to trust in themselves, and their coping process at home (Calvete & Arroyabe, 2012; Lefebvre & Levert, 2012a). In addition to practical duties (e.g., assisting in washing and eating), participating in planning and decision-making were considered essential aspects of inclusion in the patient’s care (Bellon et al., 2015; de Goumoëns et al., 2019). However, just staying at the patient’s side was enough to create a sense of participation (Calvete & Arroyabe, 2012; Kanmani & Raju, 2019). Being at the patient’s side increased FMs’ sense of managing the situation and created an optimistic feeling that their relative’s recovery was progressing (Keenan & Joseph, 2010).
FMs’ involvement in the TBI patient’s transfers and discharge plans was significant for FMs. They wanted to participate in planning the discharge together with the professionals (Lefebvre & Levert, 2012a; W. Liu et al., 2015; Norup et al., 2015) because FMs usually knew better if the patient could cope at home and whether the necessary preparations had been made at home (Abrahamson et al., 2017). Problems with hospital discharges are often related to poor communication, inadequate planning, and abrupt discharges without prior notice to the FMs (Abrahamson et al., 2017). Delays and long waiting times for transport without timely provision of information exacerbated anxiety (Abrahamson et al., 2017) and perceived burden (Kreitzer et al., 2019) among FMs. Proactive discharge planning, identifying differences between units (Keenan & Joseph, 2010), evaluating the FMs’ and patient’s needs, and setting goals together with nursing staff (Abrahamson et al., 2017) reduced the anxiety experienced by FMs (Keenan & Joseph, 2010). It enhanced their preparedness to cope at home (Calvete & Arroyabe, 2012).
Theme 3: Competent and Interprofessional Support to Empower the FMs
The versatile support from health care professionals was one of the essential factors in empowering FMs during the acute phases of the TBI patient’s treatment. To empower the FMs, the health care professionals needed to be competent, listen, and maintain the FMs’ sense of hope throughout the patient’s treatment (Abrahamson et al., 2017; de Goumoëns et al., 2019; Gan et al., 2010; Kreitzer et al., 2019; W. Liu et al., 2015). The nurse’s role was especially significant in empowering FMs because they were often considered to be part of the family (Keenan & Joseph, 2010). In addition, participating in interprofessional collaboration to support FMs was also perceived as a significant factor in empowering families because their needs changed during the different phases of the patient’s hospital care (Choustikova et al., 2020; Keenan & Joseph, 2010; Lefebvre & Levert, 2012b).
This theme included three sub-themes: confidence in the competence of health care professionals, maintenance of a sense of hope, and interprofessional collaboration to support FMs.
The FMs’ confidence in the competence of health care professionals was necessary (Gan et al., 2010) because it increased their feeling that the patient was receiving holistic care (W. Liu et al., 2015). Professionals’ knowledge and skills in caring for the TBI patient demonstrated the staff’s competence. This and communication were the key factors influencing the FMs’ experience receiving empowering professional support (Keenan & Joseph, 2010). It was important to ensure that FMs were able to talk to a doctor at least once a day; otherwise, the FMs experienced disappointment (Calvete & Arroyabe, 2012). In this study, the health care professionals who expressed little interest in involving the family were perceived as leaving the FMs alone with difficult issues. Talking about difficult issues with professionals eased the FMs’ fear, anxiety, and shock (Choustikova et al., 2020). In addition, having a good relationship with professionals allowed the FMs to feel that they were part of the team, the treatment, and the decision-making process (Lefebvre & Levert, 2012b).
Furthermore, good communication and information sharing between FMs, and staff promoted the coordination of care and achievement of shared goals (de Goumoëns et al., 2019). The need for cohesive, consistent, and long-term communication between service providers and between service providers and families was essential for empowering FMs (Abrahamson et al., 2017; de Goumoëns et al., 2019; Kreitzer et al., 2019).
To empower the FMs, health care professionals require good listening skills (Calvete & Arroyabe, 2012), know the family, and communicate with different health care providers (Keenan & Joseph, 2010). FMs wished to be heard more on patient-related issues (Kreitzer et al., 2019) because they felt they had valuable (Lefebvre & Levert, 2012b) and useful (Holloway et al., 2019) knowledge to convey that could prevent the staff from making false conclusions (Choustikova et al., 2020). Especially in situations where the patient had limited communication ability, involving the family was an important factor for the patient’s recovery (Holloway et al., 2019) and the FMs’ adaptation (de Goumoëns et al., 2019).
Maintaining a sense of hope was needed because unexpected news of an accident causes a powerful emotional reaction (Bellon et al., 2015; Keenan & Joseph, 2010) and a sense of powerlessness among FMs (Lefebvre & Levert, 2012a). Uncertain prognosis of the TBI increased the FMs’ need for hope (W. Liu et al., 2015), and they wished for health care professionals to recognize this association (Schutz et al., 2017). Although the FMs wanted truthful information, they also wanted health care professionals to give them hope for the future (W. Liu et al., 2015). Even in cases of patient death, the FMs remained hopeful and focused on minimizing the perceived suffering of the TBI patient (Schutz et al., 2017). This sense of hope gave FMs the strength to ensure their loved ones received the best care possible (Calvete & Arroyabe, 2012). However, FMs need professional encouragement (W. Liu et al., 2015) to maintain a sense of hope (Arango-Lasprilla et al., 2010). Physicians were perceived as being particularly pessimistic (Keenan & Joseph, 2010), emphasizing nurses’ role in maintaining hope and empowerment for the FMs (Schutz et al., 2017).
In the acute phase of hospital care, FMs had many questions (Norup et al., 2015) and challenges (Abrahamson et al., 2017); thus, interprofessional collaboration in supporting FMs was needed (Keenan & Joseph, 2010; Lefebvre & Levert, 2012b). For example, FMs wanted to see a hospital chaplain to discuss and share their feelings (W. Liu et al., 2015) and to meet a social worker to handle financial matters (Choustikova et al., 2020). Many FMs also hoped to meet with a physiotherapist and psychiatric nurse during the acute phase of hospital care (Choustikova et al., 2020). In addition, FMs needed interprofessional support in planning the future to strengthen their sense of control over the new situation at home with the TBI survivors, which usually arose from insecurities FMs experienced due to the potentially progressive nature of TBIs (Gan et al., 2010).
Theme 4: Community Support to Empower the FMs
The findings highlight community support as a fundamental part of empowering FMs. Arguably, it is essential for FMs to receive support from health care professionals, FMs, and friends (Calvete & Arroyabe, 2012; Holloway et al., 2019; Keenan & Joseph, 2010). In addition, the results indicate that peer support services complement the support for FMs and reduce the FM’s feelings of anxiety and fear (Gan et al., 2010; Norup et al., 2015). However, at the end of the patient’s treatment, the FMs hoped the patient’s treatment would continue after hospitalization. Once again, the nurses’ role was emphasized because the FMs hoped that the nurses would coordinate the follow-up care and organize the services. In summary, community support can empower FMs in the long term (Abrahamson et al., 2017; Bellon et al., 2015; Doyle et al., 2013; Lefebvre & Levert, 2012a; W. Liu et al., 2015; Norup et al., 2015).
This theme had three sub-themes: good social support network, information about peer support services, and ensuring continuity of care after the TBI patient’s hospital discharge.
A good social support network meant tangible help was available from friends or relatives, such as when transporting the family to the hospital (Calvete & Arroyabe, 2012) or taking care of the children’s needs (Keenan & Joseph, 2010). However, the mere presence of friends and other FMs (Calvete & Arroyabe, 2012) made the FMs feel they were not alone with all the challenges and thus promoted their feeling of empowerment (Holloway et al., 2019; Keenan & Joseph, 2010). Despite welcoming community support, FMs also wanted health care professionals to address the burden that the number of contacts from relatives caused (Calvete & Arroyabe, 2012). FMs perceived time spent with friends and relatives and answering their questions as cumbersome and stressful. They wanted to have professional guidance (Lefebvre & Levert, 2012a) and support (Keenan & Joseph, 2010) to limit their contacts (Calvete & Arroyabe, 2012).
FMs were interested in obtaining information about different peer support services at the first stage of hospitalization (Norup et al., 2015). Peer support services offer timely and helpful support in a crisis and relevant information on various resources for FMs (Gan et al., 2010). To be empowered, FMs needed to share their feelings (Norup et al., 2015) and experiences (Bellon et al., 2015) with people who had been in the same situation and had faced the same problems. Thus, they could offer suggestions and solutions for arising issues (Gan et al., 2010) and help them prepare for the worst (Arango-Lasprilla et al., 2010). Other people’s stories and experiences about the effects of TBI on family life gave FMs courage (Gan et al., 2010). They made them feel hopeful about the TBI patient’s recovery (Keenan & Joseph, 2010) and the family’s coping (Adams & Dahdah, 2016).
Ensuring continuity of care after the TBI patient’s hospital discharge was critical. At the end stage of the patient’s inpatient care, FMs hoped there was a person who would manage and coordinate the discharge and organization of services (Bellon et al., 2015; Lefebvre & Levert, 2012a; W. Liu et al., 2015; Norup et al., 2015). FMs hoped for a nurse to assume the responsibility for coordinating duties, providing information, and organizing the necessary care meetings and services (Abrahamson et al., 2017; W. Liu et al., 2015) because FMs frequently experienced inequalities in access to services (Bellon et al., 2015; Holloway et al., 2019). Access to necessary support services was crucial for empowering FMs because studies have shown such services promote FMs’ adaptation to their new roles, ease intrafamilial relationships, satisfy families’ long-term needs (Bellon et al., 2015; Gan et al., 2010), and reduce the sense of burden FMs experienced (Doyle et al., 2013).
Discussion
Summary of Findings
The findings of this systematic review outline the factors contributing to the empowering support of FMs while also describing the empowerment support from the FMs’ perspective during the acute phase of hospital care. We have defined the process of empowerment as a dialogical and supportive relationship between FMs and health care professionals, in which the FMs were seen as part of the TBI patients’ comprehensive treatment planning and implementation throughout the acute hospitalization period. Needs-based informational, participatory, professional, and community support were identified as factors of the empowerment process to promote FMs’ empowerment.
FMs are empowered when they have sufficient, concrete, and needs-based information about brain injury, its treatment, and its effect on the future from health care professionals during the acute phase of care. This enabled the FMs to utilize information in their decision-making and hence better process the consequences and effects of brain injury on family activities (de Goumoëns et al., 2019; W. Liu et al., 2015). FMs’ needs for information change in time (Lefebvre & Levert, 2012a) and, according to Keenan and Joseph (2010), decrease by 50% when the patient is transferred from the ICU to an inpatient ward. Later in the inpatient ward, FMs felt more capable of evaluating the progress of the patient’s recovery (Keenan & Joseph, 2010). At this point, it was important for the FMs to become informed about practical factors, such as transport services and managing finances (Abrahamson et al., 2017). From the empowerment perspective, the results support the findings of Wåhlin’s (2017) research, which identified knowledge as an empowerment-promoting tool and receiving information as an integral part of it. However, another point to consider is that the quality of the information and the environment where the information is offered also affects the extent of FMs’ empowerment. The information should thus be tailored to fit the FMs’ needs. The closer the received information and support are to the FMs’ needs, the more potential there is for empowerment (Funnell et al., 1991). In light of this new knowledge, future health care professional education should focus on how to offer guidance, especially from the perspective of the family’s needs (Choustikova et al., 2020). The International Family Nursing Association (IFNA, 2017) has developed advanced practice competencies for family nursing that may be useful for health care professionals working with this population of families.
Participating in the patient’s care and involvement in the patient’s transfers and discharge plans were also associated with empowering FMs (Lefebvre & Levert, 2012a; Norup et al., 2015), as it made the FMs feel they were useful and part of the patient’s holistic care (Calvete & Arroyabe, 2012). This further corroborates previous results (Kivunja et al., 2018; Manskow et al., 2017), although Oyesanya (2017) found that FMs frequently felt they were invading the health care staff’s territory by actively participating in the patient’s care. However, Wetzig and Mitchell (2017) discovered that health care professionals recognized the benefits and significance of FMs’ involvement from the perspective of the TBI patient’s recovery in acute care. The previous results emphasize that participation in patient care has also been essential in empowering the FMs because they are viewed as equal and active partners in TBI patient treatment (Degeneffe et al., 2011; Man et al., 2003; Rodwell, 1996). Thus, health care professionals should actively encourage and guide FMs on how to participate in patient care concretely. In addition, health care professionals should boldly involve FMs in all phases of the patient’s treatment plan and decision-making process to ensure that both the FMs and professionals have up-to-date information on future activities and plans and to allow the FMs to feel that they are a part of the patient’s nursing process (Lefebvre & Levert, 2012b).
Our results also show that FMs need competent professional support as well as interprofessional collaboration to comprehend the trauma (de Goumoëns et al., 2019). Thus, FMs can mourn the damage the brain injury caused; process (Keenan & Joseph, 2010), and manage (Abrahamson et al., 2017) their own emotions, such as fear, grief, anger, and guilt (Calvete & Arroyabe, 2012); and adjust to the new life situation (Lefebvre & Levert, 2012a). Health care professionals, especially nurses (de Goumoëns et al., 2019), played a significant role in supporting the FMs of TBI patients during the acute phase of hospital care (Keenan & Joseph, 2010). Earlier studies have confirmed an equal and trustful communication between health care professionals and FMs can contribute to empowering the latter (Sigurdardottir et al., 2015) and decrease the feelings of burden (Sakanashi & Fujita, 2017) and abandonment (Wåhlin, 2017). The empowered FMs feel emotionally and physically balanced, which increases confidence to act as a caregiver and further supports adaptation to a new situation (Sakanashi & Fujita, 2017). Even though empowerment cannot be handed over (Sigurdardottir et al., 2015), the review shows that nurses should recognize the effect of their support and actions on family members’ long-term capacities and well-being, particularly their coping at home after the TBI patient’s discharge.
In addition, the findings highlight how valuable it is for FMs to obtain support from outside the hospital in the acute phase of TBI patient care, particularly from other FMs, friends, and peers. Furthermore, emotional and financial support from the FMs; work environment was also significant (Gan et al., 2010). Before discharging the patients from the hospital, FMs hoped to establish a single contact point between the family and the health care and social services (Holloway et al., 2019) to provide long-term support based on the FMs’ needs, which change with time (Abrahamson et al., 2017). Undoubtedly, the nurse’s role was significant again because the FMs hoped that the nurses would take responsibility for organizing follow-up and aftercare services (W. Liu et al., 2015). It was essential to ensure continuity of care and access to support services during the acute phase of patient treatment to maintain the FMs’ well-being and ability to cope (Abrahamson et al., 2017) because FMs frequently reported facing a fragmented (Gan et al., 2010) and inconsistent health care system (Kreitzer et al., 2019) after hospital care.
Earlier studies have consistently demonstrated that FMs of TBI patients often experience anxiety, depression, social isolation, and economic disruption after hospital care (Anke et al., 2020; Manskow et al., 2017; McIntyre et al., 2020). Specifically, deficiencies in organizing and ensuring the provision of aftercare services for the family in the discharge phase may cause this. Regarding these findings, receiving incomplete or little information about support services during the patient’s hospitalization also delayed access to them and reduced FMs’ adaptation to their new role and living situation Bellon and colleagues (2015). Therefore, health care professionals must ensure that support services are available for TBI patients before being discharged from the hospital (Abrahamson et al., 2017). Although studies have demonstrated the importance of ensuring and securing the continuity of care for FMs (Bellon et al., 2015; W. Liu et al., 2015), they also show that it has not been recognized as part of the empowerment concept. However, the review revealed that information about support services alone was insufficient to ensure continuity of care for TBI patients and empower FMs.
In summary, FMs experience long and difficult times during a TBI patients’ hospitalization, especially in the ICU. Moreover, FMs have needs during the acute phases of the patients’ care that may have long-reaching consequences, such as feelings of burden, reduced life satisfaction, and depression, if they are not met. The goal of empowering FMs is to promote and maximize the FMs’ ability to manage independently with the TBI patient after hospitalization and to increase FMs’ coping and well-being. Receiving high-quality, sufficient information, participating in the patient’s care and decision-making, holistic support from health care professionals, and ensuring the TBI patient’s care constitute essential elements in the FMs’ empowerment process. Considering these elements when facing FMs during the acute phase of a TBI patient’s care may ease the family’s transition from hospital to home and facilitate adjusting to the new life situation.
However, it should be noted that the FMs’ experiences and perceived needs during the acute phases of care are insufficient sources of information to offer empowering support. Therefore, it is important to define and examine the concept of empowerment in more depth from the perspective of acute care. It would be interesting to determine whether the FMs’ primary information and support needs resulted from the sudden and uncertain nature of the brain injury, the hectic environment of acute care, and the limited resources available to the health care professionals, or a combination of these factors.
Strengths and Limitations
Our systematic literature review was performed systematically and comprehensively, and the data analysis was conducted using original data. The university library information specialist was consulted in the data retrieval process to improve the data’s coverage and reliability. In addition, two researchers performed a literature quality assessment in parallel and independently. This systematic literature review contributes beneficial knowledge on empowering support for FMs of TBI patients during the acute phase of hospital care from the empowerment perspective.
However, this study may have limitations due to the lack of available literature on FMs’ empowerment. Moreover, empowerment is a multidimensional concept, and in this study, it was generally observed on an individual level. However, information about the organizational and community levels would have also provided a more comprehensive understanding of the empowerment process. According to Wåhlin (2017), it is possible that health care professionals need to feel empowered in their professional role in order to empower FMs which was not addressed in this review. Nevertheless, it is notable to understand that it is the health care professionals who form the healthcare organization.
We did not find any clinical trials in nursing that focused on the effectiveness or efficiency of empowering TBI patients’ FMs. Therefore, other aspects of empowerment may not have been identified and may warrant more thorough research in the future. For example, tested interventions can be used to ensure and strengthen the empowerment of FMs, even after hospitalization. Although these findings are based on the perspective of FMs, the results of this study can assist health care professionals in identifying factors that help FMs process and utilize the provided support and information to control new, possibly insecure, situations. Future studies should focus more on the perspectives of health care staff when empowering FMs in acute care to gain a deeper and more holistic understanding of empowerment in the context of TBI patient care.
Conclusion
This study provides a systematic overview of the factors contributing to FMs’ empowerment and describes the empowerment from the FMs perspectives. We can conclude that empowerment in the acute phase of TBI patient treatment consists of an interactive relationship between FMs and professionals, which includes professionals providing comprehensive information and support and ensuring that the patient’s care will continue after hospitalization. Consequently, the process of empowering FMs does not end when the TBI patient’s acute phase ends, but instead continues after hospitalization.
Nevertheless, it is clear that in the future, it is essential to study the concept of empowerment more at the organizational and community levels in the context of acute care and from the perspective of health care professionals. Although this review provides information on the nature of empowering support for FMs of TBI patients during the acute phases of care, this information is derived mainly from qualitative and cross-sectional studies. In the future, clinical trials in TBI nursing aiming to find concrete and effective means to increase and to support TBI patients’ and family’s empowerment are needed. It might prove beneficial for future studies to redirect the methodology and study design toward interventional studies to obtain more comprehensive information on aspects of FMs’ empowerment support in acute care.
Supplemental Material
sj-pdf-1-jfn-10.1177_10748407231171933 – Supplemental material for Empowering Support for Family Members of Brain Injury Patients in the Acute Phase of Hospital Care: A Mixed-Methods Systematic Review
Supplemental material, sj-pdf-1-jfn-10.1177_10748407231171933 for Empowering Support for Family Members of Brain Injury Patients in the Acute Phase of Hospital Care: A Mixed-Methods Systematic Review by Julia Lindlöf, Hannele Turunen, Tarja Välimäki, Justiina Huhtakangas, Sofie Verhaeghe and Kirsi Coco in Journal of Family Nursing
Supplemental Material
sj-pdf-2-jfn-10.1177_10748407231171933 – Supplemental material for Empowering Support for Family Members of Brain Injury Patients in the Acute Phase of Hospital Care: A Mixed-Methods Systematic Review
Supplemental material, sj-pdf-2-jfn-10.1177_10748407231171933 for Empowering Support for Family Members of Brain Injury Patients in the Acute Phase of Hospital Care: A Mixed-Methods Systematic Review by Julia Lindlöf, Hannele Turunen, Tarja Välimäki, Justiina Huhtakangas, Sofie Verhaeghe and Kirsi Coco in Journal of Family Nursing
Footnotes
Acknowledgements
The authors wish to thank the Traumatic Brain Injury Association of Finland for their support, and the Carers Finland and The Finnish Nursing Education Foundation for funding this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Department of Nursing Science, University of Eastern Finland, Carers Finland and The Finnish Nursing Education Foundation. The funders had no role in the study design, in the collection, analysis and interpretation of data, the writing of articles, or the decision to submit for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.