
Abstract
A primary role in infant parenting is feeding, and this role undergoes a significant transition when introducing complementary foods (CF), with important long-term health implications. Understanding the influences on parental decision-making around timing the introduction to CF can help health care providers provide parents with effective support for feeding; however, the factors that influence parental decision-making have not been recently reviewed in the United States. To determine influences and information sources, this integrative review examined the literature from 2012 to 2022. Results indicated that parents are confused and distrustful of inconsistent and changing guidelines around CF introduction. Instead, developmental readiness signs may be a more appropriate way for practitioners and researchers to support parents in appropriate CF introduction. Future work is needed to evaluate interpersonal and societal influences on parental decision-making, as well as to develop culturally sensitive practices to support healthful parental decisions.
Introduction
All parents are faced with the challenge of navigating the transition from breast or bottle feeding their infant to introducing them to complementary foods (CF). Not only is providing age-appropriate nutrition a key aspect of their role as a parent, but they must also consider the important long-term implications of this period for their child’s health and nutrition. Introduction of CF too early may be associated with obesity, allergy risk, and picky eating (Morgan et al., 2004; Shim et al., 2011; Weng et al., 2012), and late introduction of CF also has adverse effects such as poor nutrition and an increased risk of feeding problems (Coulthard et al., 2009). Parents deciding when and how to introduce CF to their child encounter challenges such as changing professional guidelines and conflicting advice between providers and family/friends. Understanding the influences on parental decision-making around CF introduction can aid in the development of resources that reduce parental stress and improve infant health outcomes.
Feeding: A Parenting Role
Parents assume many responsibilities when they have a new infant. One of the most essential early parenting roles is feeding their infant to ensure they survive and grow (Slaughter & Bryant, 2004). In fact, much of parents’ interactions with their infant in the first year are centered around feeding (Hofferth & Sandberg, 2001; Negayama et al., 2012). Because feeding has important health implications for the infant, parents may feel anxiety and stress around their infant’s feeding (Fletcher et al., 2017; Howe et al., 2019; Sleigh, 2005). This stress can continue throughout the first year as the parent’s and infant’s roles and relationships around feeding change.
Parenting Through Feeding Transitions
A major shift in the parental feeding role is the introduction to CF. CF, or complementary feeding, refers to the introduction of foods other than breast milk or formula to an infant (also known as the introduction to solid foods). Parents navigating the transition to CF encounter decisions about when and how to introduce CF to support their infant’s feeding skills and nutrition. For example, parents must make decisions at every mealtime about what, when, and where to offer CF (Satter, 2000). Further, feeding is a relational endeavor, and this is only emphasized during the transition to CF as parents and infants renegotiate their roles in feeding (Henton, 2018; van Dijk et al., 2012, 2018). Critically, the parent’s initial decision about when to start CF with their infant can have long-term effects on the infant’s health and eating skills (e.g., Palmer & Makrides, 2012; Spill et al., 2019). Therefore, parents face an important initial decision about when to introduce CF, as well as downstream implications and decisions, during this critical shift in their feeding role as a parent.
Given the importance and complexity of the introduction to CF, parents actively seek information about how to navigate this transition with their infant. For example, parents of low-risk infants report using sources like health care providers, the internet, friends, and their own upbringing to gain information about the introduction to CF (Boulanger & Vernet, 2018; A. L. Garcia et al., 2019; Moore et al., 2012; Walsh et al., 2015). In addition, multiple family members may offer their varying opinions on the best way to introduce CF, potentially creating conflict and stress for parents during mealtimes (A. L. Garcia et al., 2019). With this growing volume of input, parents are confused by mixed information across sources and desire more support (Begley et al., 2019; Moore et al., 2012). Parents may be stressed and challenged by navigating this transition given the overwhelming and conflicting information.
Current CF Recommendations
Both parents and health care providers may look to professional medical organizations for guidance on navigating the transition to CF. Currently, the Centers for Disease Control and Prevention (CDC), the American Academy of Pediatrics (AAP), and the Dietary Guidelines for Americans recommend that parents introduce CF to their infants at around 6 months of age and explicitly state that they do not recommend introduction before 4 months (AAP, 2020; CDC, 2019; United States Department of Agriculture [USDA], 2020). These guidelines are based on research touting the risks of introducing CF too early due to an increased long-term risk of obesity, allergies, and picky eating as well as short-term nutritional deficits (Gingras et al., 2019; Morgan et al., 2004; Palmer & Makrides, 2012; Shim et al., 2011; USDA, 2020) or too late due to influences on oral motor skill development, infant food repertoires, and feeding problems (da Costa et al., 2017; Emmett et al., 2018; Simione et al., 2018; Spill et al., 2019). Based on these risks parents must strike a balance of introducing CF within a narrow time frame to reap the optimal benefits for their infant.
It may not be surprising that parental feeding practices often do not match the clinical ideal. In the United States, a recent CDC report stated that 31.9% of parents introduce CF before their infant reaches 4 months of age (Chiang et al., 2020). High rates of early introduction have been observed in other developed countries as well, including Great Britain, Italy, and Australia (Costantini et al., 2019; Scott et al., 2009). Given the long-term health implications for infants, public health interventions have attempted to address this discrepancy. For example, in 2022 the United Kingdom launched an initiative to educate families around when and how to introduce CF (Department of Health and Social Care, 2022). However, in the United States, updated supports for parents are lacking. Notably, the AAP has a “Healthy Active Living for Families” project for obesity prevention in children. However, it is informed by parent interviews from a single U.S. city in 2010 and 2011 and does not focus on the introduction to CF specifically (Radecki et al., 2012). Current U.S. guidelines and interventions do not appear to be influential in parental decision-making around CF introduction. Therefore, to effectively support families in navigating this transition it is essential to identify the most up-to-date factors and information sources parents are using to inform the introduction to CF.
Existing Work
Given the importance of the introduction to CF, multiple researchers have summarized literature on this topic. However, the existing reviews have focused on a specific methodology (e.g., only qualitative studies) and/or factor (e.g., cultural norms; A. H. Garcia et al., 2016; Spyreli et al., 2021). By limiting the research by these criteria, the potential applicability is lessened. In contrast, this integrative review examines quantitative, qualitative, and mixed methods literature together to holistically examine parental decision-making related to introduction to CF. Further, other comprehensive reviews have focused on specific geographical regions (e.g., developing countries), but none have focused on the United States. Given the probable influence cultural and societal factors can have on parental decision-making, we examine the United States specifically to address the gap in the literature regarding this country, with a focus on implications for future interventions.
Guiding Framework
The Social Ecological Model (SEM) is a theoretical framework that can guide the organization and synthesis of the factors influencing parental decision-making around CF introduction to provide guidance for developing successful health interventions (Glanz & Bishop, 2010). Importantly, SEM recognizes that influences on parental decision-making are layered and multifaceted, including individual, interpersonal, community, and societal levels. The individual level refers to factors about the parent and their beliefs, knowledge, and attitudes, as well as characteristics like race, educational attainment, and weight (McLeroy et al., 1988). The interpersonal level refers to influences from the parent’s relationships, such as their interactions with extended family, friends, and health care providers, but also the reciprocal relationship between them and their infant. At the community level, the parent may be influenced by broader factors like social institutions and the setting in which they live. The societal level represents more global influences, such as the economic climate, the parent’s cultural norms, and health care policies.
SEM was chosen as a guiding framework for this work because it acknowledges the multiple spheres of influence in an increasingly connected world. Today parents making health care decisions for their infant are exposed to broad influences through the internet and social media (Pretorius et al., 2019). SEM considers this broad network to evaluate the importance and interaction between spheres of influence. In addition, SEM has been used extensively around parental feeding decisions, such as parental decision-making around breastfeeding (Dunn et al., 2015; Reeves & Woods-Giscombé, 2014; Roll & Cheater, 2016) and infant feeding among immigrant women in Australia (Joseph et al., 2019). SEM is appropriate as a theoretical framework for this work due to its acknowledgment of broad influences as well as its prior use in feeding-related work.
Aims
Parental decision-making around feeding their child, particularly at the time of introduction to CF, has important implications including risks associated with nutrition, obesity, and feeding problems. Parents are faced with a shift in their feeding role and multiple spheres of influence and are seeking support around these transitions. Understanding the current influences on parental decision-making can provide evidence for designing effective interventions to aid parents and reduce stress. The purpose of this review is to provide a modern, integrative synthesis of the available literature in the United States to address the following aims:
To synthesize the recent empirical evidence on parental decision-making around introducing CF.
To identify the factors that influence parental decision-making around when to introduce CF.
To understand parental needs around making decisions about complementary feeding.
Methods
We based our methods on those described by Whittemore and Knafl (2005) for integrative reviews, incorporating both experimental and non-experimental research to understand factors that contribute to parental decisions for introducing CF. In addition, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement (Page et al., 2021) to guide the organization and writing of this review.
Eligibility Criteria
Studies were included if they (a) were conducted in the United States, (b) utilized qualitative, quantitative, or mixed methods research methods, (c) examined parental decision-making, perceptions, or influences regarding introduction of CF, (d) included at least some infants aged 0 to 24 months, and (e) were published as full-text articles in the English language. Studies were excluded if they (a) did not report any factors or did not connect factors to initiation of CF, (b) only examined CF outcomes related to nutrition or hygiene, (c) only reported health care providers’ perspectives, or (d) were published as commentaries or reviews. Interventions were also excluded to avoid bias around influences on introduction.
Information Sources and Search Strategy
A health sciences librarian searched through the final search date of May 26, 2022 in the following databases: PubMed, Cumulative Index of Nursing and Allied Health Literature Plus with Full Text (EBSCOhost), and Scopus (Elsevier). After some initial pilot searches, we opted to use two search strategies. Both strategies included a combination of subject headings and keywords. The first strategy included these four key concepts: infants, caregivers/parents, solid foods, and decision-making. The second strategy included these five key concepts: infants, caregivers/parents, solid foods, factors, and the United States. To be more comprehensive, we did not include terms for the United States in the decision-making strategy because many studies that occur in the United States do not state so in the titles or abstracts. However, we found that quantitative studies around associated factors for CF make use of national or regional data sets and do indicate a U.S. location in the abstract, and therefore this was included in the second strategy. The searches were filtered to English language and to publication dates of 2012 to 2022. This date filter was applied due to the advent of social media. The complete, reproducible search strategies can be found in the Supplemental material.
Study Selection
We used Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org) to complete the screening and data extraction processes. Two researchers independently screened the titles and abstracts of all references for eligibility criteria and resolved conflicts through discussion. We repeated the process for the full-text screening stage.
Risk of Bias Assessment
Two researchers independently assessed the quality of the studies using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018). We chose this tool due to its flexibility in assessing qualitative, quantitative, and mixed methods research. We assessed each included study for two items: (a) clear research questions and (b) collected data that address these questions. Then, each included study was assessed on five design-specific criteria. Overall agreement between raters was 83.25%. We resolved discrepancies around quality assessment through discussion.
Data Extraction and Data Synthesis
We created a data extraction template within Covidence that included the following information: article title, first author, publication year, study aim, study design, participant type, age range of infant participants, inclusion and exclusion criteria, number of participants, cultural group (if applicable), research instruments, percentage of infants introduced to CF by age, factors associated with and not associated with timely, early, and late introduction of CF, sources of information, other key findings, and implementation tips. We excluded missing or unclear data from the data extraction tool.
Two researchers independently extracted data for each study. We resolved discrepancies through discussion. We examined three subgroups based on the population studied: (a) studies that sampled on a national level and/or with no specific sub-population (hereafter referred to as the general sample), (b) studies that sampled by a parental or infant health characteristic, and (c) studies that sampled by race, ethnicity, or socioeconomic status. Within each subgroup we examined three categories: (a) age of introduction to CF, (b) factors associated and not associated with age of introduction, and (c) sources of information. We created data displays for each subgroup and organized using the SEM (Figures 1-3). We extracted themes both within and between subgroups.
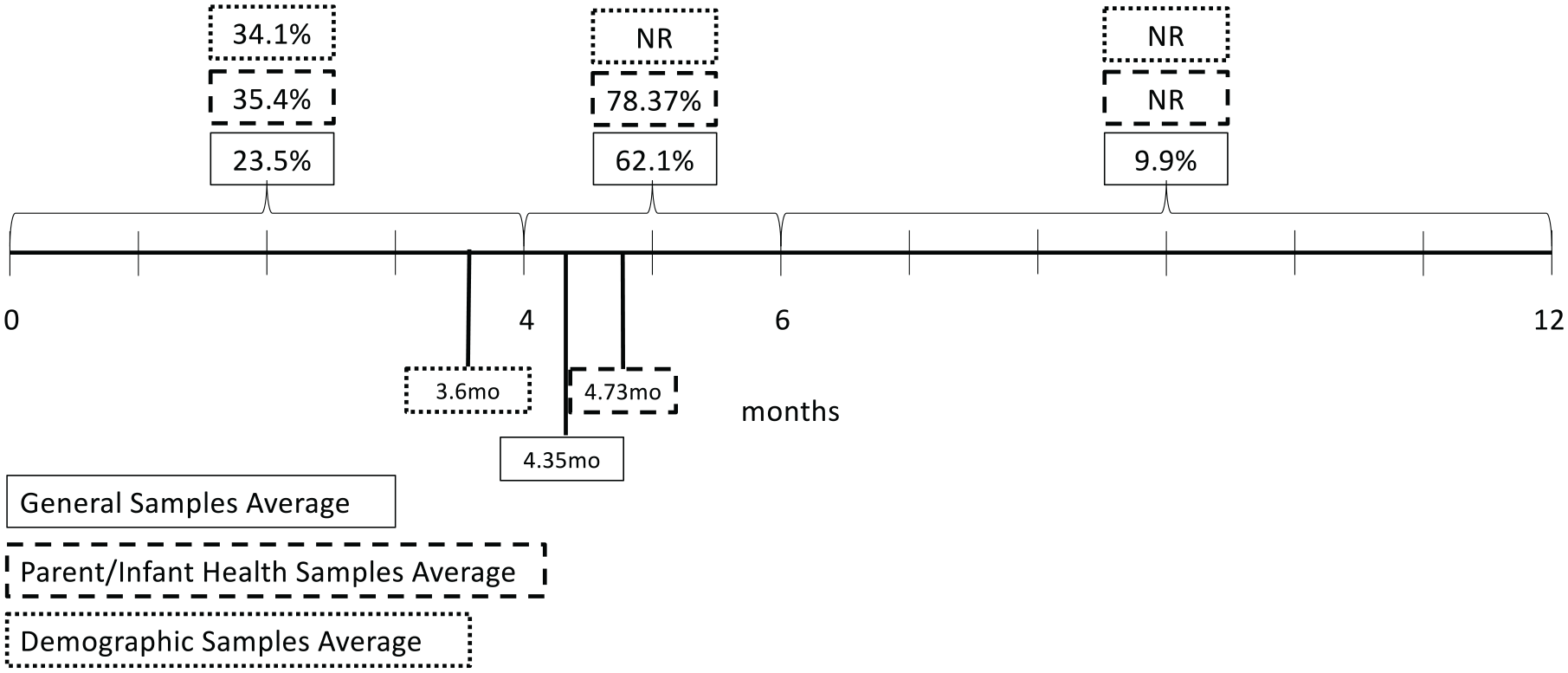
Average percentage and age of infants introduced to complementary foods by subgroup.
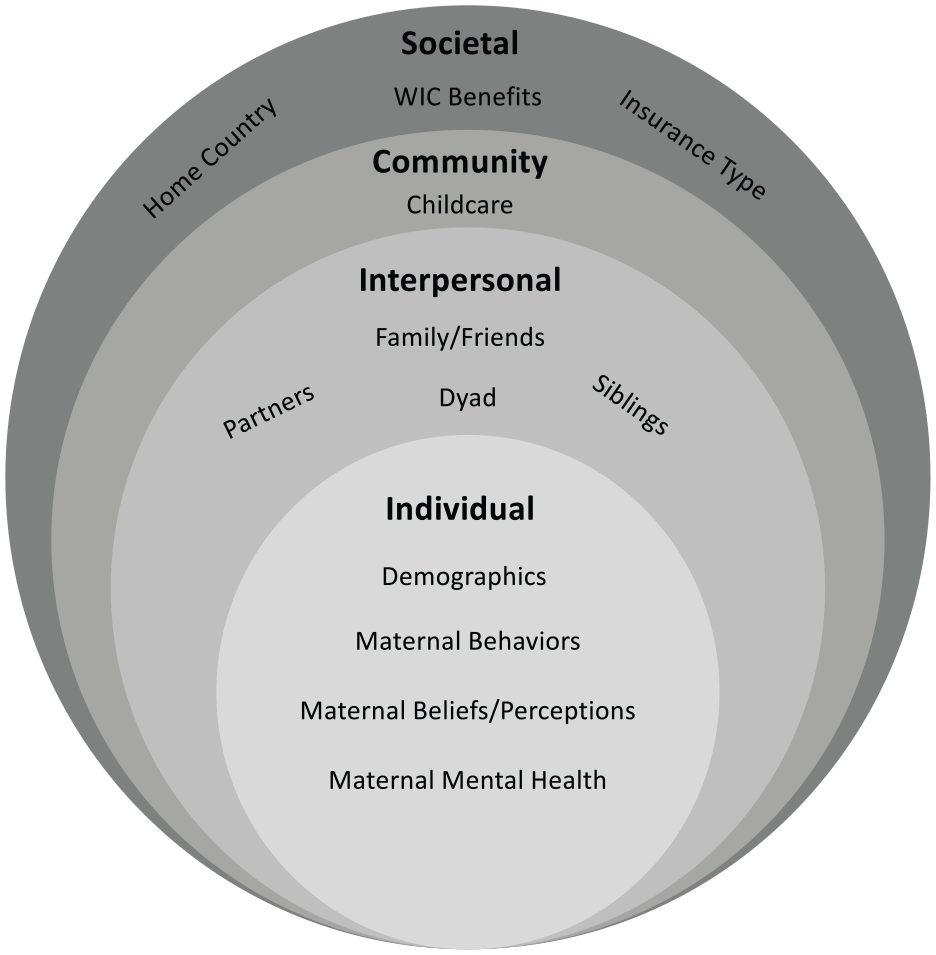
Factors influencing CF introduction.
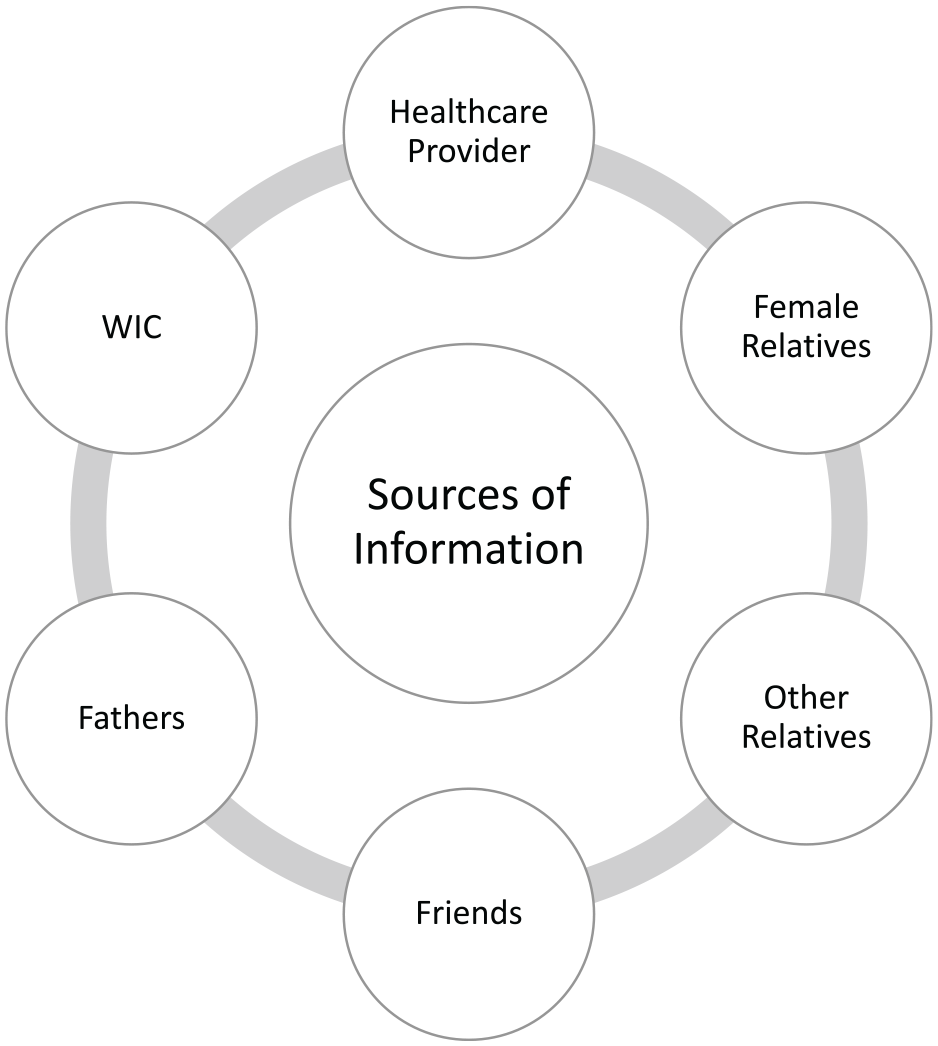
Sources of information about CF introduction.
Results
Study Characteristics
The flowchart of the screened and included studies is shown in Figure 4. A total of 29 studies met eligibility criteria and were included in the final review. See Tables 1 to 3 for study characteristics. The quality of the studies was assessed using the seven MMAT criteria. No studies were excluded on the basis of poor quality; all studies rated fulfilled at least five of the seven quality criteria and none of the deficits were deemed severe enough to disqualify a study from exclusion. Having a representative sample and having a low risk of nonresponse bias were most commonly missing.
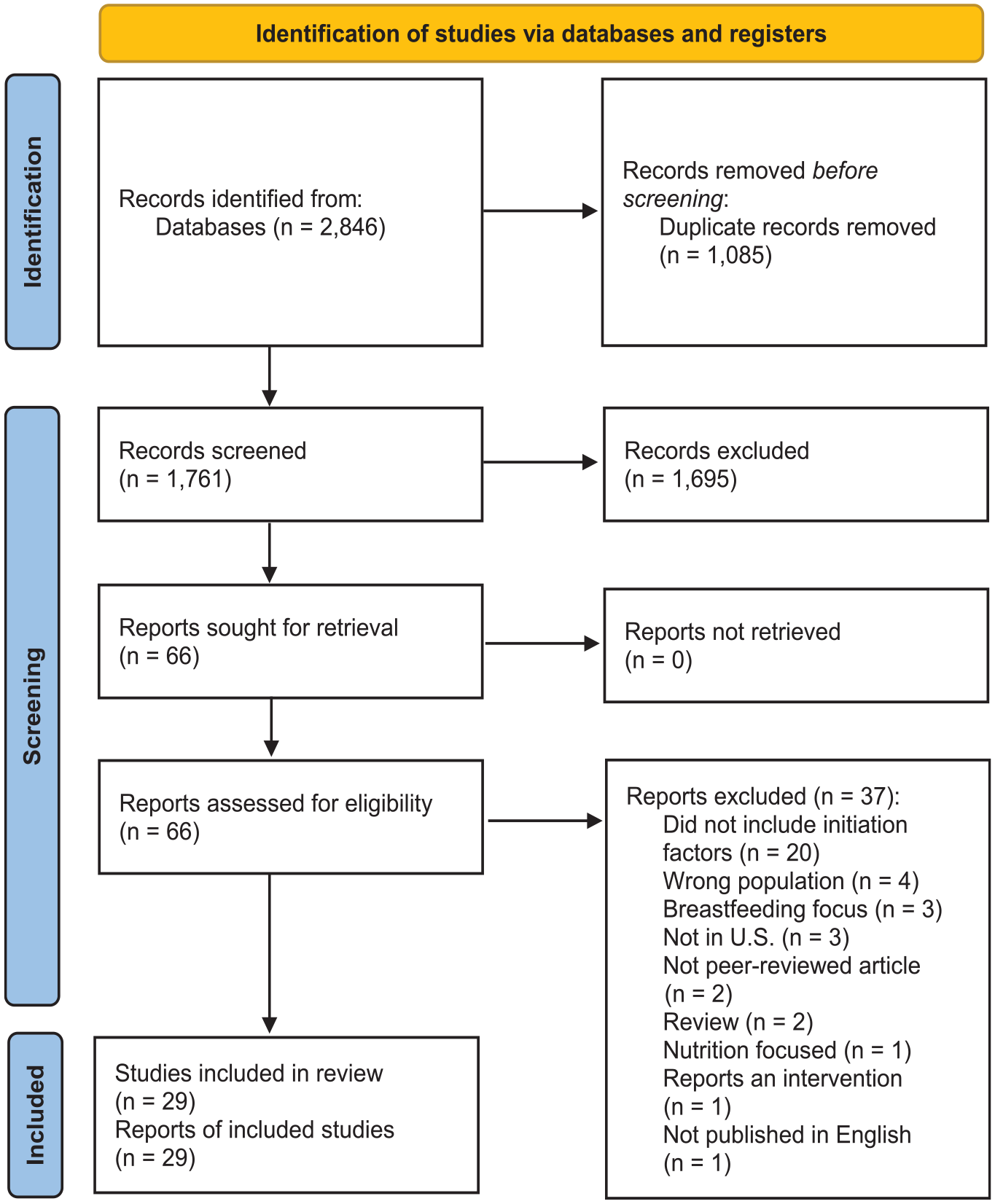
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Study Characteristics—General Population Studies.
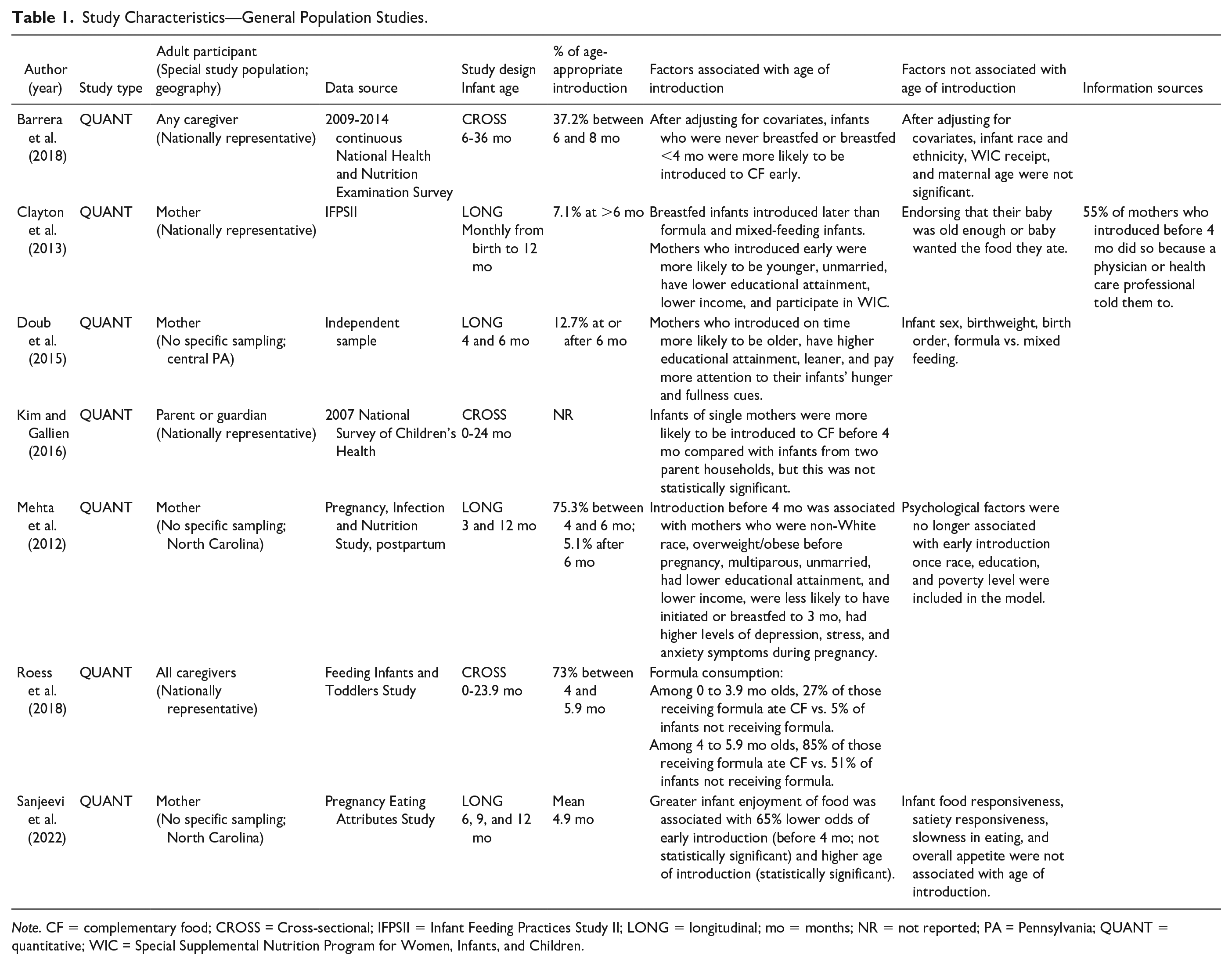
Note. CF = complementary food; CROSS = Cross-sectional; IFPSII = Infant Feeding Practices Study II; LONG = longitudinal; mo = months; NR = not reported; PA = Pennsylvania; QUANT = quantitative; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
Study Characteristics—Parent/Infant Health Characteristic Studies.
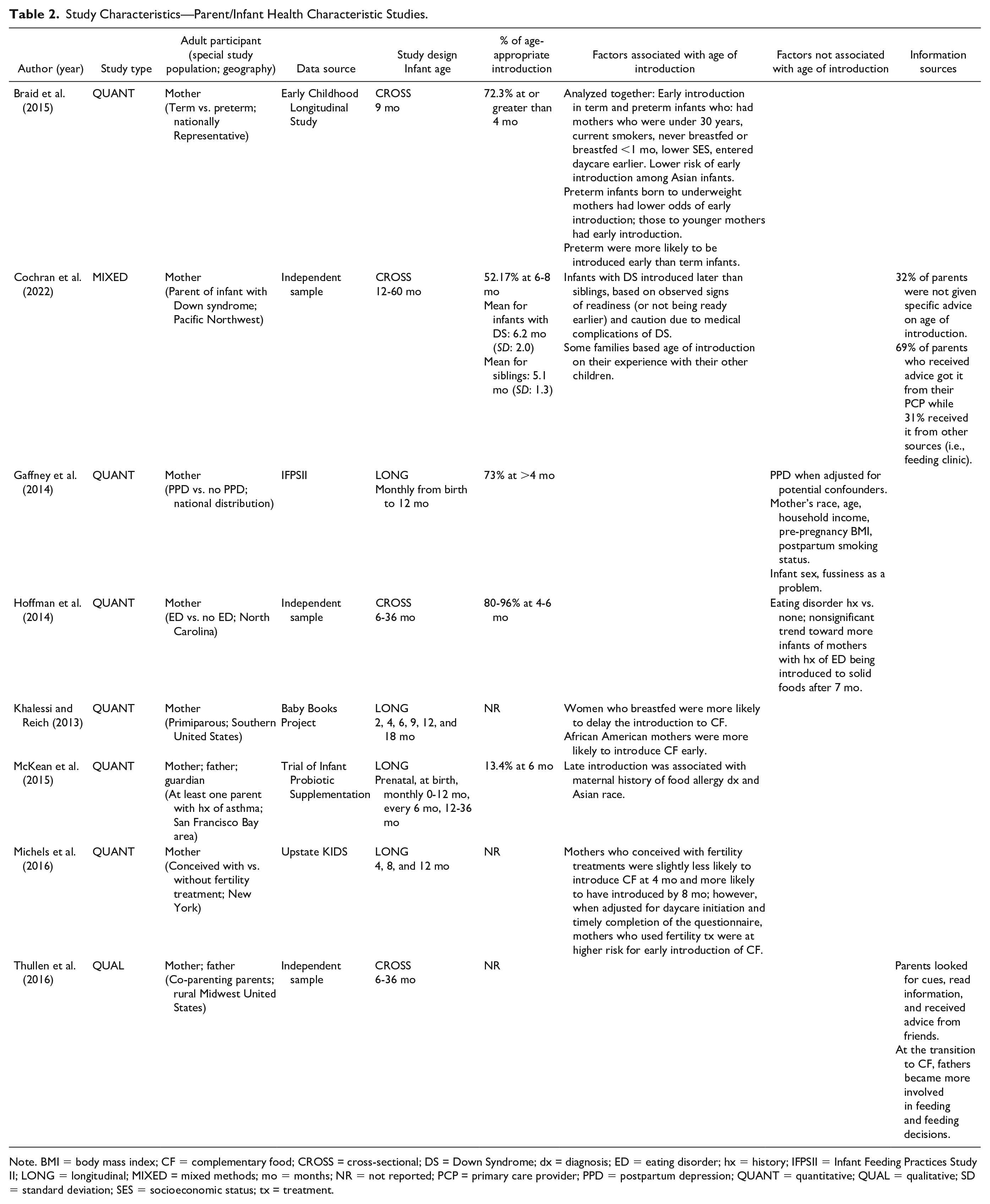
Note. BMI = body mass index; CF = complementary food; CROSS = cross-sectional; DS = Down Syndrome; dx = diagnosis; ED = eating disorder; hx = history; IFPSII = Infant Feeding Practices Study II; LONG = longitudinal; MIXED = mixed methods; mo = months; NR = not reported; PCP = primary care provider; PPD = postpartum depression; QUANT = quantitative; QUAL = qualitative; SD = standard deviation; SES = socioeconomic status; tx = treatment.
Study Characteristics—Race, Ethnicity, and SES Studies.
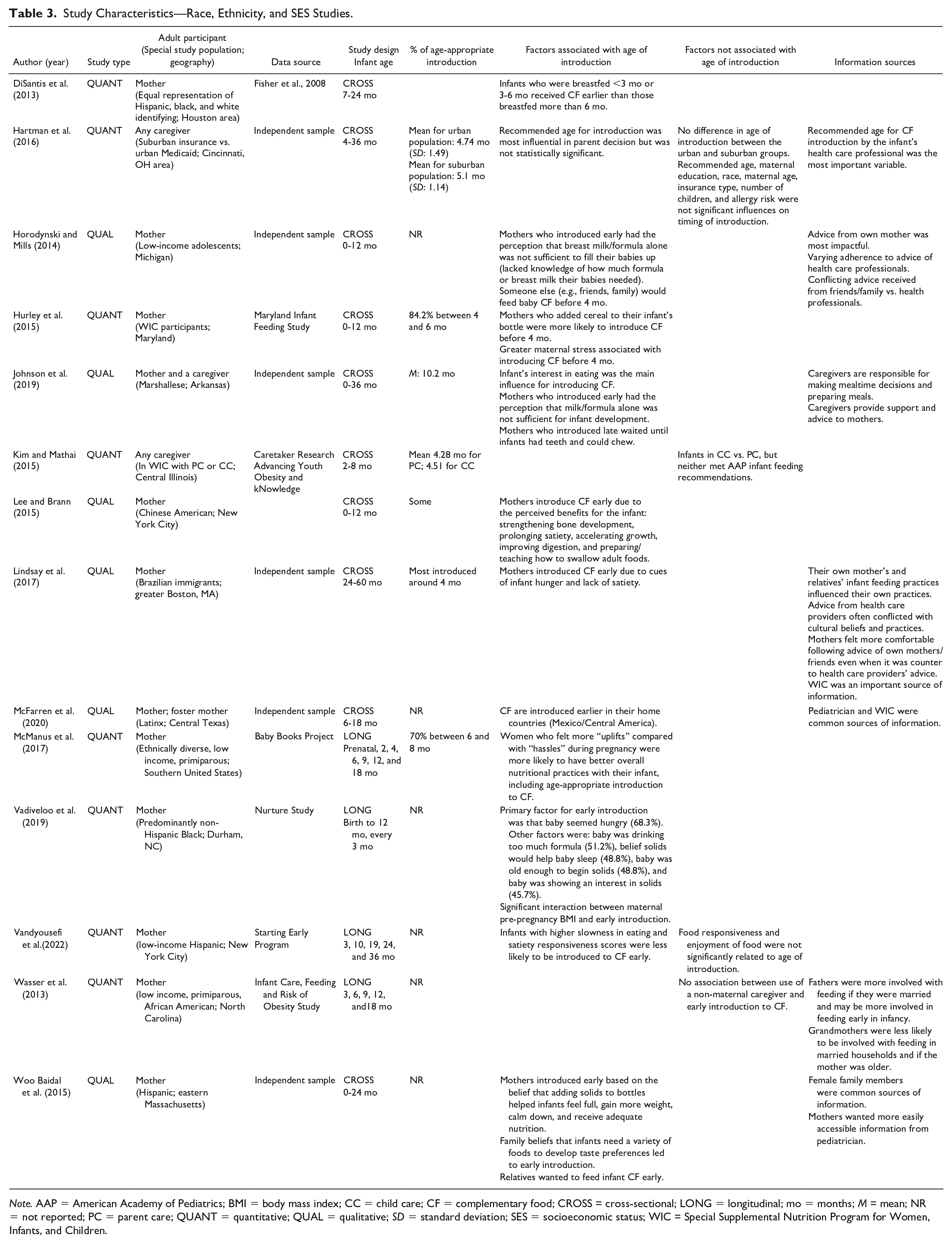
Note. AAP = American Academy of Pediatrics; BMI = body mass index; CC = child care; CF = complementary food; CROSS = cross-sectional; LONG = longitudinal; mo = months; M = mean; NR = not reported; PC = parent care; QUANT = quantitative; QUAL = qualitative; SD = standard deviation; SES = socioeconomic status; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
The majority of studies targeted specific populations within the United States including a particular racial, ethnic, or socioeconomic group (Table 3) or a particular maternal or infant health characteristic (Table 2). Most studies sampled only mothers, although six sampled caregivers or guardians, one sampled co-parenting mothers and fathers (Thullen et al., 2016), and one sampled pairs of mothers and caregivers (Johnson et al., 2019). Six studies utilized nationally representative samples (Barrera et al., 2018; Braid et al., 2015; Clayton et al., 2013; Gaffney et al., 2014; Kim & Gallien, 2016; Roess et al., 2018), but most studies (23/29) recruited from a single geographic area. Geographic regions of the United States were not equally represented with more studies taking place in the Northeast and the South.
Of note, Clayton et al. (2013) and Gaffney et al. (2014) both utilized the same sample (the Infant Feeding Practices Study II). However, Gaffney et al. (2014) limited their sample to matched individuals with and without postpartum depression (PPD) and therefore both studies were included and analyzed as unique studies. Khalessi and Reich (2013) and McManus et al. (2017) both utilized samples from the Baby Books study but used different exclusion criteria; therefore, the samples utilized for data analysis were different and these studies were also independently analyzed.
Age of Introduction to CF
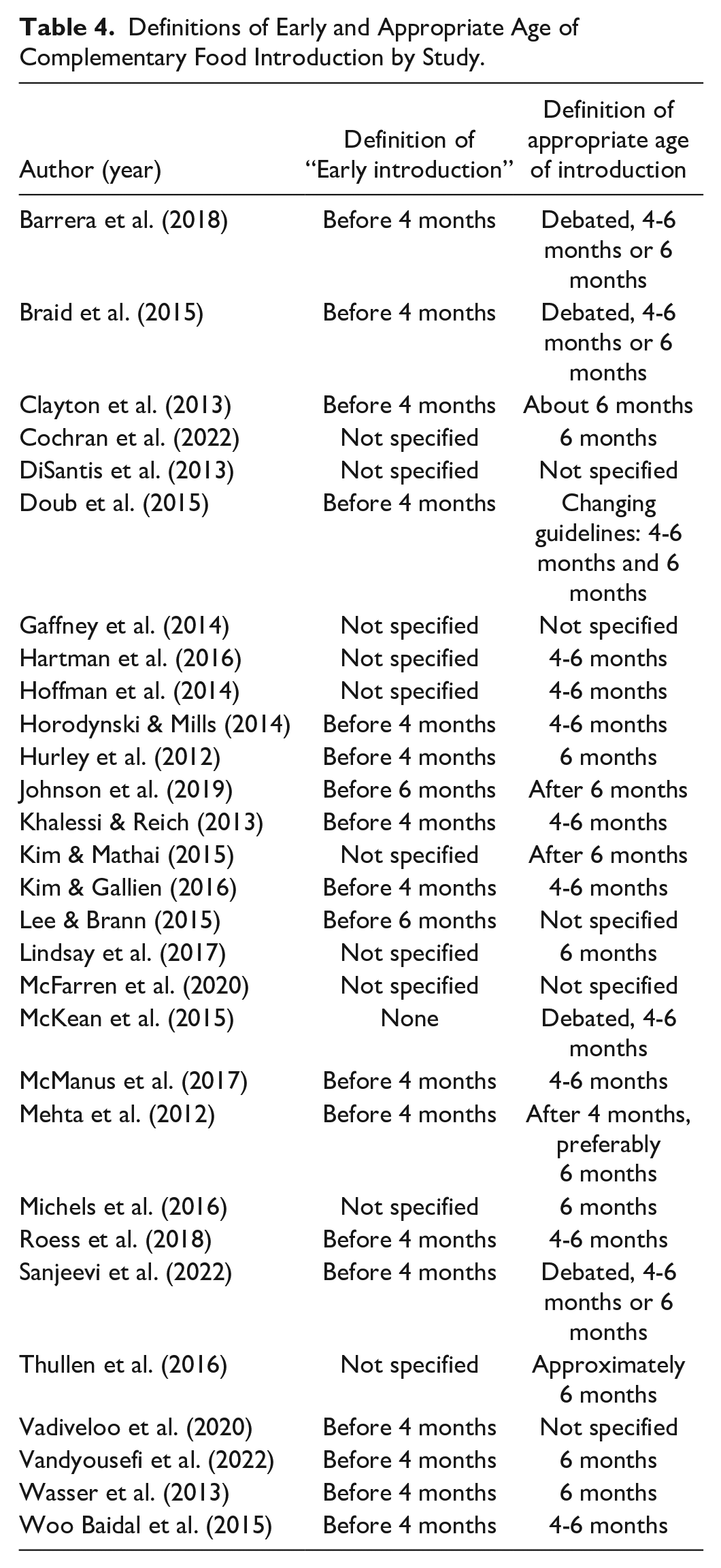
The first category examined across subgroups was the age at which infants were introduced to CF. First, it is important to note that the definition of the appropriate age to introduce CF varied across studies (see Table 4). However, despite the inconsistency in defining an appropriate age to introduce CF, most studies agreed that introducing CF before 4 months was early.
Definitions of Early and Appropriate Age of Complementary Food Introduction by Study.
Overall, across subgroups, most infants were introduced to CF between 4 and 6 months of age, with an overall mean age of introduction of 5.3 months (SD: 2.1 months) across studies that reported an average age of introduction (see Figure 1). Specific sub-populations may be at particular risk of introducing CF before 4 months and broadly, rates of introduction prior to 4 months were high (M: 29.6%; SD: 18.6%). For example, a majority of preterm infants (64.5%) were introduced to CF before 4 months adjusted age (Braid et al., 2015). In contrast, only 4.6% of infants with Down syndrome and 7.0% of infants whose parents had a history of food allergy were introduced to CF before 4 months (Cochran et al., 2022; McKean et al., 2015). While introduction after 6 months was rarely defined or measured, it was rare, with an average of only 9.6% of infants introduced at 6 months or later. However, introduction after 6 months was common among a Marshallese (from the Marshall Islands) sample living in Arkansas where CF was introduced at an average of 10.2 months by mothers and 11 months by caregivers (Johnson et al., 2019).
Factors That Influence Age of Introduction
Across studies, there was little consistency in the variables examined in relation to the age of introduction to CF; therefore, themes across subgroups are presented together below according to the SEM framework.
Individual level
The majority of studies reported on individual level influences on the age of introduction to CF (Figure 2). These included maternal characteristics (e.g., weight, age, education), infant characteristics (e.g., race, sex), maternal beliefs and perceptions about the infant and feeding, and maternal behaviors (e.g., breastfeeding, smoking). The race, ethnicity, and socioeconomic status (SES) subgroup tended to focus on maternal beliefs and perceptions, whereas the other samples focused on maternal and infant characteristics and feeding patterns. However, several themes emerged across subgroups, as described below.
Demographics
There were several maternal demographic characteristics that were associated with age of introduction; however, these associations were inconsistent across populations. Specifically, maternal educational attainment, maternal age, maternal weight, and family income were associated with age of introduction in some samples, and not significantly associated in others (Barrera et al., 2018; Braid et al., 2015; Clayton et al., 2013; Doub et al., 2015; Gaffney et al., 2014; Hartman et al., 2016; Hoffman et al., 2014; Mehta et al., 2012).
Infant characteristics were infrequently reported. Infant sex and birthweight were not associated with age of introduction (Doub et al., 2015; Gaffney et al., 2014). Preterm infants were more likely to be introduced to CF before 4 months, while infants with Down syndrome were introduced to CF later than their siblings (Braid et al., 2015; Cochran et al., 2022).
Race was inconsistently associated with age of introduction. Of note, some studies examined the infant’s race, others examined mother’s race. Infant race was not associated with age of introduction in a national sample, but Asian infants were more likely to be introduced to CF later in a combined preterm/term sample (Barrera et al., 2018; Braid et al., 2015). Maternal race was not associated with age of introduction in a sample of mothers with and without PPD (national sample) or in an urban and suburban sample from Ohio (Gaffney et al., 2014; Hartman et al., 2016). However, in a community sample in North Carolina, non-White race was associated with earlier introduction to CF (Mehta et al., 2012) and African American race was associated with earlier introduction in a sample of diverse, primiparous mothers in the Southern United States (Khalessi & Reich, 2013). In a cohort of parents with a history of allergy in the San Francisco Bay area, maternal Asian race was associated with later introduction to CF (McKean et al., 2015).
Maternal behaviors
Several studies examined dyadic behaviors that may be related to CF introduction. Never breastfeeding, breastfeeding for shorter periods (less than 3 or 4 months), and/or formula feeding were consistently associated with a greater chance of introducing CF earlier and this was true of national, general, preterm/term, diverse, and primiparous samples (Barrera et al., 2018; Braid et al., 2015; Clayton et al., 2013; DiSantis et al., 2013; Khalessi & Reich, 2013; Mehta et al., 2012; Roess et al., 2018). Maternal smoking was associated with earlier age of introduction in the combined term/preterm sample but not associated with age of introduction in the with/without PPD sample (Braid et al., 2015; Gaffney et al., 2014).
Maternal beliefs and perceptions
Maternal beliefs and perceptions as reasons for introduction before 4 months were most commonly explored among the race, ethnicity, and SES samples. A common reason for introducing CF earlier was the belief that milk was not enough for the infant’s growth and development and/or a perception that the infant was hungry and/or not satisfied by milk or formula alone (Horodynski & Mills, 2014; Johnson et al., 2019; Lee & Brann, 2015; Vadiveloo et al., 2019). These beliefs and perceptions were noted among low-income adolescents, Marshallese mothers and caregivers, Chinese American mothers, Brazilian immigrant mothers, non-Hispanic Black mothers, and Hispanic mothers (Horodynski & Mills, 2014; Johnson et al., 2019; Lee & Brann, 2015; Lindsay et al., 2017; Vadiveloo et al., 2019; Woo Baidal et al., 2015).
Maternal mental health
Maternal mental health status was inconsistently associated with CF introduction. Maternal stress was associated with earlier introduction among Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) recipients and experiencing more positive experiences in pregnancy was associated with later introduction in a primiparous sample (Hurley et al., 2015; McManus et al., 2017). However, in a general sample, maternal stress, anxiety, and depression in pregnancy were not associated with age of introduction when race, education, and poverty level were controlled for (Mehta et al., 2012). There were no observed differences in age of introduction among mothers with an eating disorder history or those with PPD (Gaffney et al., 2014; Hoffman et al., 2014).
Interpersonal level
Few studies examined variables at the interpersonal level, but those who did examined the influence of partnered relationships, family and friends, and siblings, as well as the parent’s relationship with the child. In three general samples, being unmarried was associated with earlier introduction (Clayton et al., 2013; Kim & Gallien, 2016; Mehta et al., 2012). In addition, low-income adolescents noted that friends or family would often be the ones to decide to feed their infant CF before 4 months (Horodynski & Mills, 2014) and a sample of Hispanic mothers reported relatives wanted to feed their infant CF before 6 months (Woo Baidal et al., 2015), pointing to the influence of family and friends on earlier introduction to CF.
The influence of having more than one child varied. For example, having more than one child was associated with earlier introduction in a sample of North Carolinian mothers (Mehta et al., 2012) but number of children was not associated with age of introduction in a Ohioan sample (Hartman et al., 2016). Mothers of infants with Down syndrome initially based the age of CF introduction on when they did so with their other children. However, they then also used signs of readiness observed in their infant, which overall resulted in a later introduction than siblings (Cochran et al., 2022).
Parent awareness of and responsiveness to infant cues was sometimes associated with age of introduction. For example, observing that their infant was interested in eating was associated with earlier CF introduction among Marshallese and non-Hispanic Black samples (Johnson et al., 2019; Vadiveloo et al., 2019), but was not associated with age of introduction in a national sample (Clayton et al., 2013). In a national sample, mothers who paid attention to their infant’s hunger and fullness cues were more likely to introduce CF between 4 and 6 months (Doub et al., 2015) and mothers of infants with Down syndrome observed signs of readiness to decide when to introduce CF (Cochran et al., 2022). Marshallese mothers and caregivers often delayed introducing CF until their infant had teeth and could chew (Johnson et al., 2019).
Community level
The only variable examined at the community level was child care use. Earlier age at daycare introduction was associated with an earlier age of introduction to CF among a combined term/preterm sample (Braid et al., 2015). However, having non-maternal child care did not significantly change age of introduction among neither a WIC sample nor a primiparous African American sample (Kim & Mathai, 2015; Wasser et al., 2013).
Societal level
Few studies examined the influence of societal characteristics on the age of introduction. Latinx mothers reported that CF was introduced earlier in their home country than was practiced in the United States, but these mothers often followed U.S. practices based on advice from their pediatrician (McFarren et al., 2020). In two nationally representative samples, receiving WIC benefits was associated with introduction before 4 months in one sample but not associated with age of introduction in another (Barrera et al., 2018; Clayton et al., 2013). In addition, there was no statistically significant difference in age of introduction between an urban Medicaid and suburban private insurance population (Hartman et al., 2016).
Overall, there was little consensus across the full spectrum of studies. Maternal demographic variables, mental health, and infant cues resulted in mixed findings. Breastfeeding practices (never or less time breastfeeding) and beliefs about how well milk or formula satisfied the infant were consistently associated with earlier introduction to CF.
Information Sources
Sources of information about when to introduce CF were primarily explored in qualitative studies (Figure 3). The influence of a health care provider, such as a pediatrician, was cited across studies as a common source of advice (Clayton et al., 2013; Cochran et al., 2022; Hartman et al., 2016; Horodynski & Mills, 2014; Lindsay et al., 2017; McFarren et al., 2020). Friends and family, particularly female relatives like the mother’s own mother, were also frequently cited (Horodynski & Mills, 2014; Johnson et al., 2019; Lindsay et al., 2017; Thullen et al., 2016; Wasser et al., 2013; Woo Baidal et al., 2015). However, it was not uncommon for the advice of friends and family to conflict with that of a health care provider (Horodynski & Mills, 2014; Lindsay et al., 2017). In these instances, the weight placed on different sources of information varied by population. For example, Brazilian immigrant mothers felt more comfortable taking the advice of friends and family over that of a health care provider (Lindsay et al., 2017). Similarly, low-income adolescents received conflicting advice from health care professionals and family members and reported the advice from their mothers was ultimately most impactful. (Hartman et al., 2016; Horodynski & Mills, 2014). Alarmingly, in a nationally representative sample, Clayton et al. (2013) reported that 55% of mothers who introduced CF before 4 months did so at the recommendation of a health care provider. Finally, WIC was cited among Latinx and Brazilian immigrant mothers as valuable sources of CF information (Lindsay et al., 2017; McFarren et al., 2020).
Recommendations for Intervention
A consistent theme across studies was the need for clear, consistent, evidence-based guidelines on the appropriate age to begin CF (Barrera et al., 2018; Braid et al., 2015; Cochran et al., 2022; Hartman et al., 2016; McKean et al., 2015). This was in part due to the confusion among parents and providers about the best age for CF introduction (Barrera et al., 2018; Hartman et al., 2016; McKean et al., 2015). In addition, providing families culturally sensitive counseling, acknowledging maternal beliefs, and helping families establish and reach goals around infant feeding were recommended (DiSantis et al., 2013; Doub et al., 2015; Kim & Mathai, 2015; Lee & Brann, 2015; Lindsay et al., 2017; McFarren et al., 2020; McKean et al., 2015). Given the influence family members can have on feeding decisions, using intervention methods appropriate for both mothers and family members was suggested (Johnson et al., 2019; Wasser et al., 2013; Woo Baidal et al., 2015). Methods for disseminating information about CF to families included counseling during well-child visits, motivational interviewing, text messaging, social media, print newsletters, home visits, the internet, and/or parenting groups (Horodynski & Mills, 2014; McFarren et al., 2020; Woo Baidal et al., 2015). In addition, mental health support, provider training, and screening were recommended practices to support parents in introducing CF appropriately (Cochran et al., 2022; Hurley et al., 2015; McKean et al., 2015; McManus et al., 2017). There were also suggestions made that were specific to the population studied. Most notably, guidelines specific to the needs of preterm infants and infants with Down syndrome were recommended to help providers guide families (Braid et al., 2015; Cochran et al., 2022). Mothers who are obese or overweight were also included as a population that would benefit from tailored intervention (Mehta et al., 2012; Vadiveloo et al., 2019).
Discussion
There is little consensus around factors that influence parental decision-making around CF introduction. Inconsistent definitions around early and appropriate introduction of CF also exist in the literature, making it difficult to identify factors that could be addressed to support families. In addition, studies examining family/interpersonal, community, and societal factors that could influence the timing of CF introduction are lacking, leaving a gap in understanding. The literature is consistent in its call for culturally centered care and clarified guidelines for special populations, such as infants with prematurity or genetic syndromes, to support families with this transition.
Parents often received conflicting advice from health care providers and family/friends. On one hand, parents distrusted the recommendations of health care professionals because of changing and inconsistent guidelines. This is a valid concern—the guidelines have changed in the last 10 years. Prior to the 2012 AAP guidelines, introduction to CF any time after 4 months was considered appropriate. Therefore, families with multiple children may have received different advice from health care providers depending on their children’s birth years and families with multigenerational living arrangements may receive outdated advice from family members. In addition, the CDC and AAP currently recommend CF introduction, “around 6 months of age” but also recommend exclusive breastfeeding up to 6 months, which can be contradictory (AAP, 2020; CDC, 2021). Inconsistency in the recommended age to start CF was also observed among the studies examined in this review, possibly because while all included studies were published at or after 2012, the data were, at times, collected prior to the 2012 guideline change. Given the changing guidelines, health care providers desire, and would benefit from, additional training on CF introduction, particularly in light of a national sample that found 55% of mothers who introduced CF before 4 months were advised to do so by a health care professional (Clayton et al., 2013; Cochran et al., 2022; Samady et al., 2020). In addition, inconsistency in defining appropriate, early, and late introduction limited the ability to compare rates of introduction across studies and populations in this review. Therefore, we endorse the suggestion made by numerous studies calling for improved clarity and consistency of guidelines, to the benefit of parents, health care professionals, and researchers.
Despite the inconsistency, most infants across studies and samples were introduced to CF between 4 and 6 months of age. Based on the above recommendations, this may or may not be appropriate from a public health standpoint. However, it is agreed that the rates of introduction to CF before 4 months are still too high in the United States. This review found that across studies an average of 29.6% of infants were introduced to CF before 4 months. Rates of early introduction were particularly high among a sample of those who conceived with and without fertility treatments (59.1% and 61.7%, respectively), preterm infants (64.5% introduced before 4 months adjusted age), infants of single mothers (37.1%), WIC recipients (36.5%), and non-Hispanic Black mothers (31.7%). Nationally representative samples reported a range of 16.3% to 40.4% of infants were introduced to CF early. Early introduction can have important long-term health implications such as higher rates of obesity, allergies, and picky eating (Fewtrell et al., 2003; Gingras et al., 2019; Morgan et al., 2004; Pluymen et al., 2018; Shim et al., 2011). Therefore, continued efforts from health care providers to reduce the rates of early introduction are warranted.
One way to reduce rates of early introduction to CF is through public health interventions, which would intervene on factors that influence when parents introduce CF to their infants. Based on the findings of this review, both breastfeeding status and maternal beliefs influenced the age of introducing CF and are also likely to be influenced by family/interpersonal factors. Breastfeeding is hypothesized to be linked to age of introduction because breastfeeding mothers may be more committed to healthful feeding practices or may have a greater awareness of infant cues (DiSantis et al., 2013; Khalessi & Reich, 2013). Alternatively, maternal beliefs around the insufficiency of milk for growth could result in both breastfeeding cessation and early introduction to CF. When mothers believed that their infant was no longer satisfied by breast milk or that breastmilk wouldn’t be sufficient for their continued development and growth, they introduced CF to support these goals. Numerous studies have described efforts to improve breastfeeding rates (e.g., Segura-Pérez et al., 2021) and these efforts should be continued as they may have unintentional positive consequences for introducing CF appropriately, particularly when they address maternal beliefs about the nutritional quality of breast milk. Specifically, primary care providers, like pediatric nurse practitioners and pediatricians, can offer support and counseling to parents to continue breastfeeding when appropriate, as well as information about age-appropriate introduction of CF.
Gaps and Future Directions
This review highlights the need for additional research efforts focused on the introduction to CF from diverse perspectives. For example, from the lens of the SEM framework, most of the research has focused on variables at the individual level. Further, even at the individual level there is little consistency in the factors examined, making it challenging to compare findings across populations. While most studies examined some maternal demographic characteristics, the characteristics chosen and how they were defined varied. In addition, other individual-level factors like beliefs, knowledge, infant characteristics, and maternal mental health were inconsistently incorporated into statistical models. Future research would benefit from more consistent examination of factors across study populations.
In addition to deficits at the individual level, the interpersonal level received surprisingly little attention given the overwhelming research on the impact family members can have on breastfeeding (e.g., Ogbo et al., 2020). In those that reported it, health care professionals and friends and family were the most common sources of information about introducing CF (Clayton et al., 2013; Cochran et al., 2022; Hartman et al., 2016; Horodynski & Mills, 2014; Lindsay et al., 2017; McFarren et al., 2020; Thullen et al., 2016; Wasser et al., 2013; Woo Baidal et al., 2015). However, there was often conflict between the advice of health care professionals and friends or family, with mothers relying on friends or family because they understood their cultural beliefs and practices (Horodynski & Mills, 2014; Lindsay et al., 2017). The influence of family members may only be increasing with the increasing rates of multigenerational households in the United States (Cohn et al., 2022). Therefore, health care providers, like pediatric nurse practitioners and pediatricians, would benefit from discussing familial and cultural practices and beliefs for introducing CF with families (Dickin et al., 2021). Within a culturally sensitive mindset health care providers can then assist families in incorporating healthful practices, such as delaying introduction to CF past 4 months, while honoring cultural traditions, such as specific foods that families value introducing first. Finally, this review was narrowed to the preceding 10 years to account for the influence of the internet and social media; however, these resources were seldom inquired about in the included research. Given the growing influence of social media on a variety of parenting behaviors, future inquiry into the impact of social media on CF patterns is warranted (Doub et al., 2016; Griauzde et al., 2020; Kallem et al., 2018; Pretorius et al., 2019). This can be integrated into research that examines the community and societal levels to inform researchers and practitioners about the broader factors influencing parental decision-making around CF introduction.
Before interventions to support parents can be developed, defining appropriate guidelines is critical. One area with a dearth of evidence that is not addressed in current AAP or CDC recommendations is the late introduction of CF. Late introduction to CF (after 9 or 10 months) can lead to feeding problems, oral motor delays, and picky eating (Cameron et al., 2012; Coulthard et al., 2009; Emmett et al., 2018; Northstone et al., 2001). However, in the reviewed articles, the number of infants who were introduced to CF any time after 6 months of age were reported as one group. By doing this, critical differences in age of introduction are washed out. For example, Johnson et al. (2019) found that Marshallese mothers didn’t introduce CF until an average of 10.2 months, an important effect that could be missed by averaging across a sample. Therefore, late introduction, and why parents decide to delay introducing CF, should be carefully measured in future studies.
When deciding when to introduce CF, the CDC and AAP state that it is appropriate to do so around 6 months based on the infant’s developmental readiness signs. However, only one of the studies reviewed reported on parental awareness, understanding, or use of signs of developmental readiness for CF in their decision-making process. Specifically, only parents of infants with Down syndrome referred to developmental readiness as a factor in their decision-making (Cochran et al., 2022). Developmental readiness may be more important than the specific age an infant is introduced to CF (Chung et al., 2014). Therefore, future research should examine parents’ knowledge of and identification of infant developmental readiness signs at the age of CF introduction and how this relates to long-term outcomes to offer a more accurate and individualized look at the impact of age of introduction.
Finally, while most studies excluded populations of infants with medical complications, those studies that reported on infants with health complexities emphasized the need for guidelines specific to these populations, which currently do not exist (Braid et al., 2015; Cochran et al., 2022; Elfzzani et al., 2019; Liotto et al., 2020). The lack of specific guidelines puts infants at risk because high-risk infants may not follow the same developmental timeline as other infants and may exhibit different readiness cues, making deciding when to introduce CF challenging for families and health care providers (Cochran et al., 2022). The lack of guidelines also puts parents at risk because parents of high-risk infants already experience greater feeding-related concern and the lack of clarity can add stress to this transition (Howe et al., 2019). Future research should develop evidence-based guidelines around introducing CF to high-risk infants to guide practitioners and families in successfully introducing CF.
Limitations
This study has several limitations. First, we may have missed relevant articles due to our search strategy and our selected databases. Specifically, we only included studies that directly related influencing factors to parental practices. Therefore, studies that examined factors more broadly were not incorporated into this review but could be used to inform future studies. Second, our review includes studies that ranged in quality and rigor. Some included studies were not generalizable to larger populations, which should be considered when applying to future work. However, these studies do add valuable information specific to sub-populations that can be applied to future targeted interventions. In addition, the representation of regions of the United States was varied and therefore was not compared in this study. Future reviews may consider whether varying geographical regions of the United States contribute to CF practices. Finally, there was variation in the definitions of early and appropriate introduction to CF across studies, as well as some studies that did not clearly define these concepts. This made comparison across studies challenging. Future studies should include clear definitions and mirror current guidelines so that studies can be directly compared.
Conclusion
Parents experience a shift in their parenting role when they navigate the transition to CF. This review highlights how guideline inconsistency can make it more difficult for parents to know what is the best course of action around introducing CF. Focusing on developmental readiness cues, rather than a specific age of introduction, may yield more appropriate practices. Specifically, a focus on developmental readiness allows for more flexibility based on the infant’s individualized developmental progression (such as that needed for high-risk infants) and the family’s cultural traditions, both of which have been identified as gaps in current approaches. Future research should examine developmental readiness cues alongside interpersonal, community, and societal factors that may be influencing healthful practices around introducing CF. By improving the clarity and consistency of guidance, providers can build trust with families and help them meet their goals for their infant’s eating practices and long-term health.
Supplemental Material
sj-docx-1-jfn-10.1177_10748407231156914 – Supplemental material for Parental Decision-Making Around Introducing Complementary Foods: An Integrative Review
Supplemental material, sj-docx-1-jfn-10.1177_10748407231156914 for Parental Decision-Making Around Introducing Complementary Foods: An Integrative Review by Kelsey L. Thompson, Jamie L. Conklin and Suzanne Thoyre in Journal of Family Nursing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.