
Abstract
Although the value of family caregivers’ involvement with relatives in long-term care (LTC) is well recognized, tensions remain regarding their role. Such tensions were exacerbated during the COVID-19 pandemic as strict public health measures restricted family access to LTC homes. Using interpretive description, we examined the impact of visitation restrictions on family caregivers’ experiences caring for a relative in LTC between March 2020 and June 2021. In-depth interviews were conducted with 14 family caregivers (five spouses and nine adult daughters) and two key themes were identified. The first theme, “seeking to maintain relational continuity,” illustrates how caregivers sought to sustain connections with residents prior to and during the pandemic. The second theme, “disrupted relational continuity,” highlights the impact of severed relational connections on caregivers’ sense of self and ongoing feelings of loss and anger. Findings call for a trauma-informed approach that recognizes the pervasiveness of trauma for family caregivers and the avoidance of re-traumatization.
Research continues to dispel the myth that family members relinquish their caregiving role when their relative moves into a long-term care home (Backhaus et al., 2020). Rather, families provide a range of instrumental, emotional, and personal care support, thereby facilitating the continued physical and psychosocial well-being of their relative (Gaugler & Mitchell, 2021). In U.S. residential care facilities, older adults receive an average of 65 hrs of care from “informal” caregivers (including family members) per month (Coe & Werner, 2022). Although agreement exists as to the value of family involvement (Puurveen et al., 2018), tensions remain regarding family members’ roles, with their knowledge and contributions both silenced and devalued (Bauer et al., 2014; Baumbusch & Phinney, 2014). Such tensions have only been exacerbated during the COVID-19 pandemic as governments around the world mandated strict response measures to mitigate infection spread and control outbreaks within care homes, including prohibiting visitors and nonessential health care personnel from entering (Low et al., 2021). Although the effects of such measures on residents’ mental and physical well-being have been well examined (e.g., Kaelen et al., 2021; Levere et al., 2021; Mo & Shi, 2020; Stall et al., 2021; Van der Roest et al., 2020), emerging evidence suggests such lockdowns and visitor restrictions have also had considerable impact on family caregivers (e.g., Avidor & Ayalon, 2022; Dupuis-Blanchard et al., 2021; Hindmarch et al., 2021; Ickert et al., 2021; Mitchell et al., 2021). This article seeks to contribute to the growing body of literature examining the experiences of being a family caregiver to a relative living in long-term care during the COVID-19 pandemic.
Background
Recent reviews highlight that while the nature of family involvement in care may change following a relative’s transition to a long-term care home, it does not end (Gaugler & Mitchell, 2021; Puurveen et al., 2018). While spouses and female family members are more likely to be involved than other family members, the role of gender is mediated by relationship, with husbands visiting more frequently than wives and adult daughters more than adult sons (Roberts et al., 2020). Involvement is also higher for family members of residents with dementia (Weimer et al., 2021). Prepandemic, 59% of family members in British Columbia, Canada (the jurisdiction in which this study was conducted), visited at least several times per week, with 18% visiting daily (Office of the Seniors Advocate, 2020a). Similar figures are reported elsewhere (e.g., Verloo et al., 2018; Weimer et al., 2021); however, Puurveen and colleagues (2018) point out that family visitation is fluid and can shift over time, particularly as the physical and psychosocial needs of residents increase.
Family members’ patterns of involvement in care can be characterized as providing hands-on assistance (e.g., at mealtimes and with personal care), overseeing and managing care (e.g., appointments outside the care home, monitoring quality of care), offering socioemotional support (e.g., linking the resident to families and friends outside the care home), and contributing to the sense of community (e.g., engaging with other residents during activity programming and mealtimes; Puurveen et al., 2018). However, Whitaker (2009) cautions against simply categorizing family involvement by visit frequency or the extent to which instrumental tasks are conducted, arguing that this provides a distorted view of family members’ contributions and the meaning of the visits for both families and residents. Whitaker’s (2009) exploration of family involvement in Swedish care homes attends to the relational dynamics in which visits are rooted, highlighting how family visits entail relational representation and nurture relationships beyond the care home, ritualize continuity and coherence through daily routines, and preserve their relative’s identity and dignity.
As evidenced above, when a relative moves into a care home, the role of family members does not shift from that of caregiver to visitor. Classifying family as visitors negates the critical role family caregivers play, highlights the limited comprehension of care relations in long-term care, and reflects the taken-for-granted assumptions about care work, gender, and families (Aronson & Neysmith, 1997; Kemp, 2021). The COVID-19 pandemic and the resulting public health visitation policies have also negated much of the work of the past few decades to shift long-term care from a traditionally focused biomedical approach to a more holistic, person-centered approach (Ickert et al., 2021). Indeed, British Columbia’s public health measures left little, if any, room for families to support their relative’s mental or physical well-being or mitigate social isolation.
An emerging body of literature suggests that the failure to recognize the significance and depth of family involvement has had a profound impact on family members caring for a relative over the course of the pandemic. Avidor and Ayalon (2022) described how, during the first wave of the pandemic, visiting restrictions in Israel led to an abrupt breach between families and residents, in terms of the sudden physical disconnection, disruption to routines, treatment and care, and the disruption of satisfaction with and trust in the care home. Families struggled with the guilt they felt in being unable to remove their family member from care to take them into their own homes, a sentiment echoed by North American caregivers (Dupuis-Blanchard et al., 2021; Mitchell et al., 2021). Feelings of helplessness, frustration, anxiety, fear, and anger are woven through the accounts of caregivers caring for a relative in long-term care in Canada (Dupuis-Blanchard et al., 2021; Hindmarch et al., 2021; Ickert et al., 2021), Finland (Paananen et al., 2021), and the United States (Mitchell et al., 2021; Nash et al., 2021) due to differing ideas of what it meant to be essential, limitations associated with masking and physical distancing, disrupted care routines, understaffing, and limited visiting hours (Ickert et al., 2021; Mitchell et al., 2021). Concerned about the deteriorating health of their relatives, restrictions aggravated families’ feelings of anticipatory grief and the missed opportunities to spend time with their relatives at their end of life (Mitchell et al., 2021; Paananen et al., 2021). Finnish family members, whose relatives could no longer express themselves using words, reported finding the change from being able to physically touch their relative to having to rely on conversation alone, devastating (Paananen et al., 2021). Indeed, phone and video calls were considered a poor substitute for face-to-face visits and especially problematic for those with cognitive and physical impairment (Hindmarch et al., 2021; Ickert et al., 2021; Paananen et al., 2021). Not surprisingly, restricted access to their relatives resulted in increased social isolation and strain for family caregivers as well as decreased quality of life (Hindmarch et al., 2021).
This article seeks to extend this growing body of literature by examining the tensions around the changing relations and roles of family members caring for an older adult living in a long-term care home during the COVID-19 pandemic in British Columbia, Canada.
Method
This study utilized interpretive description (Thorne, 2016) as the methodological approach. Grounded in naturalistic and constructivist theory, interpretive description allows us to move beyond simple description to explore the meanings and explanations of the lived experience of family members caring for a relative in long-term care during the first 12 months of the pandemic. It entails drawing meaning from interpretation among and between participant accounts, enabling both pattern recognition and variance detection (Thorne, 2016). Particularly useful in the nursing and health care profession, interpretive description results in contextualized meaning that yields implications for both practice and policy (Thorne et al., 2004). Ethics approval was obtained from the University of British Columbia Research Ethics Board (H21-00176).
Setting
This study was conducted in Canada’s westernmost province of British Columbia, where the first case of COVID-19 was identified in late January 2020 and a provincial state of emergency was declared on March 18, 2020 (Office of the Seniors Advocate, 2020b). Public health orders closed all care homes to visitors, including families, from March 20, 2020. In July 2020, restrictions were amended to include two distinct visitor categories that remained in place until April 2021 (Mackenzie, 2022). Under the designated visitor category, the same individual was permitted one visit per week for 30 min or less in a common visiting area, whereas as an essential visitor, a family caregiver (theoretically) could visit more frequently and for longer durations. The category into which a family caregiver was placed was determined by the care home operator, who decided whether the threshold for “essential” (e.g., visits for compassionate reasons such as critical illness or end-of-life care, or visits considered paramount to resident’s physical care and mental well-being) was met.
Recruitment and Participants
Convenience sampling was used to recruit participants via social media (e.g., Twitter and Facebook). Inclusion criteria were (a) a family or friend providing support to an older adult living in a long-term care home in British Columbia prior to, and during, the COVID-19 pandemic (i.e., since January 2020) and (b) fluency in English. Upon initial contact from caregivers, H.A.C. screened potential participants and offered additional study information. Following receipt of written informed consent, participants were contacted by email to schedule a time for the interview. Using this approach, we recruited 14 family caregivers.
Data Collection and Analysis
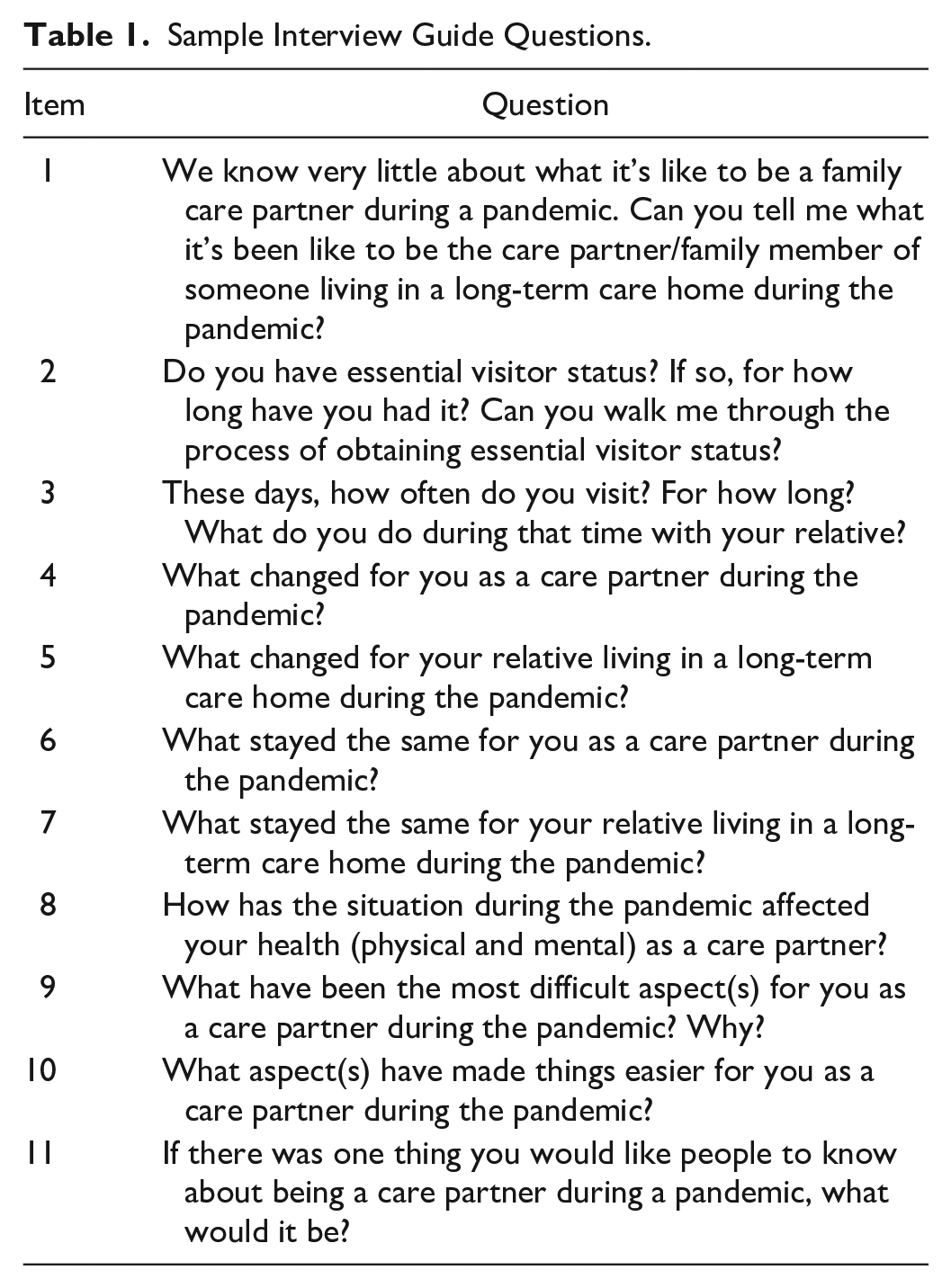
In accordance with interpretive description, data collection and analysis occurred concurrently. Fourteen in-depth, semi-structured interviews were conducted with participants between May and July 2021. Interviews were primarily conducted via Zoom, with the exception of two participants who preferred to be interviewed by phone. Interviews focused on their visitor status (essential or designated), the nature of their visits over the course of the pandemic, the changes they and their relative experienced as a result, and the impact of the pandemic and visiting restrictions on their physical and mental health (see Table 1 for sample interview questions). Sociodemographic data were also collected. Interviews ranged in length from 68 to 117 min (average length 89 min) and were conducted by HAC. All interviews were digitally recorded and transcribed verbatim. Field jottings capturing participants’ body language, reactions, and verbal tone were taken during the interview and expanded into more detailed field notes as soon as possible following the interview to contextualize participants’ narratives during analysis (Silverman, 2015). Field notes also served as a reflective diary to capture emerging patterns and personal responses to the research (Teodoro et al., 2018). Data management was facilitated via NVivo 12 and data collection concluded when no further novel patterns were noted in the data to warrant additional interviews. To ensure anonymity and confidentiality, all participants were assigned a pseudonym and are identified by this pseudonym in the “Findings” section.
Sample Interview Guide Questions.
Data analysis was an iterative, inductive process that facilitated coherent, conceptual description of thematic patterns (Thorne, 2016). Each interview recording was listened to/watched by H.A.C. and S.A.W., and transcripts and field notes read several times to develop a sense of the whole, reflecting upon “What is going on here?” and “What might this mean?” (Thorne et al., 2004). Data were subsequently arranged in patterns that reflected similar properties and were continually assembled and disassembled as relationships between data became increasingly apparent (Thorne, 2016). Biweekly team meetings enabled the interrogation and comparison of data interpretation (i.e., the extraction of thematic patterns and representative exemplars that best reflected specific dimensions of caregivers’ experiences) and ensured internal coherence of the findings.
Credibility was enhanced by documenting the decision process, using an analytic log and practicing reflexivity (Thorne, 2016). Confirmability is supported through the presentation of study methods, transparency of recruitment, and data collection and analysis, with interpretive claims grounded in rich description and verbatim data excerpts (Thorne et al., 2004).
Findings
Of the 14 family caregivers (13 women and one man), nine were adult daughters and five were spouses. Three of the participants had more than one relative living in long-term care. All participants had completed college or a university degree, six were retired, five were employed full-time, two part-time, and one was between work. Participants’ ages ranged from 38 to 87 years, with an average age of 64.2 years. Table 2 summarizes the demographic characteristics of participating family caregivers and their relative living in care.
Participant Demographics.
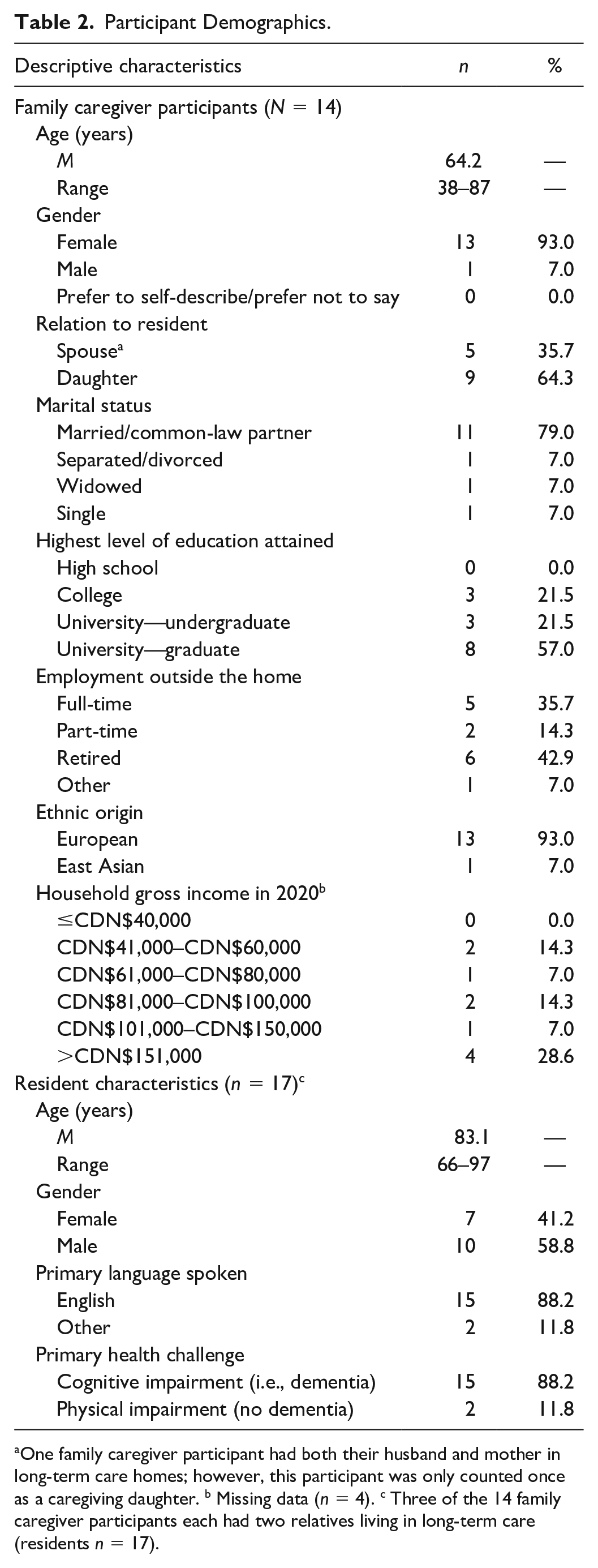
One family caregiver participant had both their husband and mother in long-term care homes; however, this participant was only counted once as a caregiving daughter. b Missing data (n = 4). c Three of the 14 family caregiver participants each had two relatives living in long-term care (residents n = 17).
Two overarching themes were identified as underpinning family caregivers’ experiences of caring for a relative in long-term care during the COVID-19 pandemic. The first theme, Seeking to Maintain Relational Continuity, illustrates how, through involvement in their relative’s care, participating family caregivers sought to sustain preexisting roles and relationships and reaffirm familial bonds both prepandemic and during visitation restrictions. The second theme, Disrupted Relational Continuity, highlights how pandemic visitation restrictions profoundly affected caregivers’ sense of self and identity, resulted in ongoing feelings of loss and guilt, and the differing impact of such disruption on a spouse versus an adult daughter.
Seeking to Maintain Relational Continuity
Participants’ narratives illustrated the limitations they faced over the course of the pandemic as they attempted to maintain the continuity of family relationships as a means of sustaining the identity, sense of self and well-being of the resident, and themselves. They were clear that the specialized support they endeavored to provide was distinct from that provided by care home staff and that such support was vital to their relatives’ health and well-being.
Through their family relationships, caregivers sought to support their relatives’ familial roles—be it mother, father, wife, husband, or grandparent. At issue for the participants was the way in which the support they offered was deemed nonessential during the pandemic:
. . . just because you don’t need feeding, doesn’t mean that visits aren’t essential . . . to me, the role that my family plays in my dad’s life is essential for him being healthy and well. . . I remember feeling angry and disappointed that my mom got designated status, so she could go once a week or once every two weeks, not essential [status] when they were able to go daily or at all meals. Like my mom and dad have been together for over 65 years and were used to seeing each other almost every day. (Deborah, 59-year-old daughter)
For Deborah, her mother’s daily prepandemic mealtime visits recalled a lifetime of togetherness and confirmed the spousal relationship. For other participants, prepandemic activities such as shaving their relative’s face, cutting their hair, trimming nails, wiping their face following a meal, and ensuring hearing aids were functional were expressions of love that upheld residents’ dignity and identity and reaffirmed familial bonds. Although seemingly trivial tasks, their completion offered families a means of demonstrating their caring and an opportunity to share close and intimate contact.
The above acts illustrate the unpaid labor that, prepandemic, not only kept residents healthy and happy but also supported care home staff by freeing time for them to engage with residents. As such, while care staff primarily focus on “bed and body” tasks (i.e., ensuring quality of care), family members focused on facilitating resident quality of life. However, ongoing visiting restrictions compromised participants’ abilities to maintain familial bonds, devalued their ongoing contributions, and dismissed their willingness to support residents during the pandemic:
[the last year has been] something you would never even suspect would happen in your life in terms of being cut off from someone you so frequently support and love and care for. [I] just never had the dialogue inside the facility about exactly what I do every day, you know. I didn’t realize how much I played into his support system until I wasn’t able to be there and finding that nobody even picked up those pieces and understood what those pieces were. Some of them of vital importance. . . The shock for all of us families was witnessing how much those of us who are involved in our loved one’s life, how much we present relief to the system by doing what we do to ensure quality of life. And feeling frustrated and challenged by being called a non-essential visitor. When in fact, you were far beyond a visitor, and you were definitely not non-essential. (Diane, 60-year-old daughter)
Families attended to their relatives’ preferences as best they could during the visitation restrictions; for those with access at mealtimes, bringing in culturally relevant or favorite foods provided comfort to their resident, reminding them of their earlier lives:
I go around mealtime so I can help feed her. And I bring in food that she likes. I do things like sushi konchi because she eats pureed food. . . So I make Taiwanese soups that she used to make and I make miso soups. It’s like comfort food for her. (Ellen, 66-year-old-daughter) The food is excellent and lunch is probably the best meal of the day, in terms of quality. Never had a complaint. But I bring him his favorites. He’s not going to get fresh mango and pineapple and his very favorite, his favorite sweets, his favorite, he likes prawns. I mean certain things that I’m not expecting them to produce or present. (Diane)
For Ellen whose mother’s advanced dementia meant the ability to participate in lengthy conversation had passed, assisting at mealtimes offered a means to share in her mother’s daily life. Mealtimes for families were not just about the quality of the food but about the provision of food that meant something to their relative, which offered comfort and continuity. Bringing in or making their relatives’ favorite foods can be viewed as yet another display of love and caring that was especially helpful in reinforcing familial bonds.
In many ways, the long-term care system views staff and families as interchangeable in terms of their caregiving support, as illustrated by Terra, a 62-year-old spousal caregiver, who relayed how she was denied essential visitor status: “But my husband eats well. He will eat from anybody. And so they [the home] decided I wasn’t necessary. I wasn’t necessary for feeding.” However, when Terra went in at mealtimes to assist her husband, she was not “feeding” him; rather she was “having a meal” with him. Assisting her husband at mealtimes was a social occurrence, one that reaffirmed their relationship, allowed for the continuation of routine of eating together as husband and wife, and offered one of the few remaining points of connection for her and her husband, given his advanced dementia.
One daughter astutely noted that what families do is often misunderstood, likely because the intangibles such as supporting a resident’s sense of self are not readily visible or easily measured, and when something cannot be measured or assigned a specific value, it is often not accounted for within policy or practice. As such, the visitation restrictions set out in the public health orders positioned families as extraneous:
And we were not referred to from the government as caregivers. We were referred to as visitors. So extraneous to the needs of a resident. And that definition itself was wrong and quite cruel . . . (Amy, 49-year-old daughter)
Participants also spoke of the intergenerational dynamics within their families and how their relative was positioned within that dynamic. In many participants’ families, it was not just a lone family member involved in their relative’s care, but rather a network of family members who all played a part in sustaining their relative’s identity and positionality within the family, in addition to their quality of life. Implementing an essential visitor policy in which only one family member was deemed essential negated the key roles of other family members:
. . . the family is an integral part of that resident, if there is a family. And the whole network of what keeps that resident healthy is dependent on this circle of love and care from the family, in addition to what they [care staff] provide. But it’s taken its toll for her because, you know people like her grandchildren, great-grandchildren, my children are all here. And they don’t visit her. They can’t. They have little babies. Before COVID. . . my daughter comes around, she’d bring her baby and her babies and they’re young. She’d bring them to my Oma, that’s how they call my mom. . . and my mom will be sitting there, and you can see, they would try to throw a ball between them and she would try, even though she was not moving, try to catch you know. The kind of joy that I have not seen. (Ellen)
For study participants like Ellen, family involvement was about holding space for the older adult within the structure of their family, something that became much harder during restrictions that prevented family from visiting. In the initial weeks and months of the pandemic, virtual visits (e.g., via Zoom or FaceTime) were offered to families. While most families did not find the virtual visits helpful, some were appreciative of the attempt to help keep their relative involved in their lives:
We missed him. . . being part of our family, and we are thankful for the phone calls. We are thankful for the FaceTime because that helped us feel connected. And the FaceTime, I honestly think was a better value than the window visits because you can bring him into your life, you know what I mean? (Deborah)
However, for residents living with dementia, as well as those who had sensory impairments and difficulties with manual dexterity, virtual communication was fraught with challenges. These residents required staff assistance to manage tablets or smart phones and, when on video calls, struggled to understand that they were visiting in real time as opposed to simply watching a prerecorded video of their family. When staff resources were significantly limited and in-person visits suspended, staff did not have the capacity to accommodate virtual visits, leaving families disconnected:
And then the FaceTime during outbreak was not . . . like my dad’s unit was on lockdown so you couldn’t do FaceTime. So, then the window visits go away when they’re on lockdown, and in-person visits go away when they’re on lockdown, and FaceTime went away on lockdown as well. (Deborah)
The nature of virtual visits also meant that other equally critical forms of communication on which families and residents may have relied were not possible. Amy described the distress she and her mother felt given the limitations of socially distanced visits: “Mom just really wanted to hold our hand. She really needed, desperately needed touch. Touch is extremely underestimated.”
Disrupted Relational Continuity
While participants revealed the importance and challenges associated with attempting to maintain a sense of continuity within family networks, they also identified the direct impact of these relational disruptions on their roles as family caregivers. The intensity of feelings exhibited during the interviews underscores the trauma that remained 17 months after the initial lockdown. Participants described their experiences as “disastrous,” “hellish,” “lonely,” “heartbreaking,” and “hugely frustrating.” Tears and anger frequently accompanied their narratives. As Terra relayed her experience during the initial lockdown of her husband’s care home in the Spring of 2020, she rocked back and forth, rubbing her hands along the top of her legs as tears sprung to her eyes. However, it was not just her body language that reflected the significant trauma the forced separation had on her well-being:
. . . it took away my purpose and my identity. I’ve been a caregiver for so long. I found it quite debilitating. For the first three months when I was entirely locked out of his life, I just kind of curled up and died. . . I found it mentally very hard to cope being separated from him. I think that hasn’t been accounted for—husbands and wives. You don’t separate husbands and wives and you don’t do that when one is sick. That’s half my soul in there and they ripped it from me. . . I was forced out of his life. . . I was obsolete. I was written off. (Terra)
Differentiating the type of kin relationship between the family caregiver and their relative is critical to understanding the distinct experiences of loss, grief, and anger as a result of these relational disruptions. Spousal caregivers like Terra were quick to explain how their relationship differed from that of a parent–child relationship. Gregory, a 78-year-old spouse, spoke of the “liminal space” he occupied. Fearful of being the one to introduce the virus into his wife’s care home, he recounted how he had curtailed his own social interaction and support and how returning home to an empty house after seeing his wife made for an isolated and lonely existence.
For adult daughters, the source of distress was not so much tied to their identity and sense of self but to the sense of abandonment and loss of control they experienced over their inability to maintain relational continuity within their families. There was also a lingering sense of guilt and failure at being unable to deliver the reciprocal care they believed their parents deserved in later life:
I don’t know how many times I said to my husband, “I don’t know what a nervous breakdown looks like, but I think I might be on the brink of one.” . . . And I think the hard part for me is that, you know, my parents lived a healthy, wonderful life and raised—I think—two fairly normal human beings. And they always did the best they could for us. And this is not the best that we could do, is it?. . . (Nicole, 47-year-old daughter)
Not being able to do “the little things” that fostered relational continuity also exacerbated feelings of guilt arising from having placed a parent in care in the first place: “you try to be like the good daughter to justify the guilt that you have, for no longer being able to care for somebody that you love” (Samantha, 38-year-old daughter). Adult daughters likened their parents’ experience to their being “on the moon” or “in prison” given the limited amount of interaction and communication they were able to maintain due to visiting restrictions.
For some participants, being the sole designated essential visitor within the family magnified the weight of caregiving responsibility. As Ellen explained her source of exhaustion, “I am the single point person. The responsibility. . . the burden. It’s so not good to say burden because it’s my mother but it’s a big responsibility. It’s huge.” At times, changes to caregivers’ roles and responsibilities resulted in disruptions beyond the immediate caregiver–care recipient relationship. Nicole highlighted the ripple effect of the challenges she faces given her multiple roles as a daughter, wife, and mother:
I think feeling defeated and tired and exhausted by the whole thing, right? Trying to be a good mom and a good wife and a good everything and not being successful with anything because you can’t, right? Like I just. . . My husband has done so much. And he will because he’s wonderful. But you want to show your kids that this is important. And you know, I’ve said to them, “You know, Mommy’s upset because. . .” and “Mommy’s mad because. . .” I think my 8-year-old gets is. She’ll say, you know, “Yeah, you’re not happy with what’s happening to Nana.” “No, I’m not. I’m not happy. It’s not good enough.” You know, but again, it’s like that whole layer of trying to do everything and feeling like you’re shit at it all. Like we didn’t fail my parents, we didn’t fail my parents, I know we didn’t. But you know, poor Mom.
The guilt and grief woven through the above excerpt underscore the tension adult daughters experienced as they struggled to reconcile the complexity of what they knew on some level to be the system’s failure (to recognize the essential role of family caregivers and the resulting impact on residents’ quality of life), with a sense of personal failure (to fulfill familial roles and expectations). Samantha conveyed a similar sentiment as she explained trying to uphold the relational continuity between her father in care and her 5-year-old son whose visit was canceled due to an outbreak in the home: “I don’t make promises because I can’t keep anything. . . you don’t feel very good as a caregiver.”
At the time the interviews were conducted, wider societal restrictions had begun to ease in British Columbia; however, while other families began to resume some semblance of normalcy and reestablish their relationships and activities, participants’ lives were still circumscribed by the visiting restrictions and ongoing worry about transmitting the virus, which in turn created some bitterness and resentment. Samantha explained,
I don’t care how much news you watch. I don’t care how much social media you consume. You have no idea what happened there and what’s happening there unless you live it. We’re a baseball family and you know, they’re having barbeques for wrap up and we’re like, “We’re not going.” And they’re like, “Well why? You’re allowed.” And I’m like, “My Dad is locked up in a home again because of COVID.”
As Nicole concluded, “. . . I don’t think anybody will ever know the pain and trauma of family members who have lived through this.”
Discussion
Our study findings reveal the profound and deeply disruptive consequences that pandemic visiting restrictions had on the relational continuity of family caregivers with relatives in long-term care homes. As in recent research (e.g., Avidor & Ayalon, 2022; Dupuis-Blanchard et al., 2021; Hindmarch et al., 2021; Ickert et al., 2021; Mitchell et al., 2021), family members highlighted the intense emotionality—frustration, grief, anger, anxiety, and guilt—of their experiences, and the lingering impact of such emotion 17 months into the pandemic. However, the findings also extend the current literature by exploring what visits meant to families, thereby offering a more nuanced understanding of why visiting restrictions had such a traumatic and long-lasting impact.
For participating families, visits with their relative were about reaffirming familial bonds—upholding their relative’s position within the family as a cherished parent or spouse, sharing companionship and intimate contact, and demonstrating their affection and love. Such findings reinforce Whitaker’s (2009) research in which family visits and involvement were conceptualized as representing the marital or parent–child relationship, maintaining continuity and coherence of daily routines, and protecting resident dignity and identity. However, pandemic visitation restrictions designed to mitigate infection spread and control outbreaks within care homes privileged a biomedical approach to care. This in turn curtailed families’ abilities to sustain their relatives’ (and their own) sense of self and identity and devalued families’ role in preserving residents’ quality of life, thereby severely disrupting relational continuity.
The findings also highlight how the roles that family caregivers and care home staff fulfill are not interchangeable. When family members enter the care home, they do so not just to offer hands-on assistance with care tasks (e.g., grooming and/or personal care, mealtime assistance) but to continue their preexisting familial relationship, within which they demonstrate their affection and caring, and reaffirm familial ties and resident identity. As such, families are not there to do the work of staff but to fulfill a unique and meaningful role. Their visits are not simply about the tasks to be performed but about what the performance of the tasks represent: the maintenance of, and attendance to, ongoing familial relationships. For example, the oft-stated rationale behind the denial of essential visitor status for participating families was that staff were able to “feed” their relative, rendering family assistance unnecessary. However, as demonstrated in previous research (Henkusens et al., 2014; Roberts et al., 2020; Whitaker, 2009), the task of mealtime assistance is not just about getting calories in, but about continuity, love, and companionship. Indeed, distinct differences exist with regard to who provides care and the subsequent impact on resident health and quality of life (Verloo et al., 2018). Recent research by Wu and colleagues (2020) found that residents who received eating assistance from family members consumed significantly more energy and protein compared with those residents who were assisted only by staff. The authors attribute this difference to the combination of the psychosocial aspect of having family present at mealtimes and the practical aspect of the dedicated and focused attention needed when providing eating assistance (Wu et al., 2020).
Close relationships and kinship ties have been shown to predict visit frequency as family caregivers seek to continue their relationship with their relative in care (Gaugler & Kane, 2007). The type of kin relationship held between family caregivers and their relative offers additional insight regarding the traumatic impact of pandemic visiting restrictions on relational continuity. Our findings confirm those of existing research (e.g., Pinquart & Sörensen, 2011) that suggest family caregivers should not be considered a homogeneous group, despite the tendency for policymakers to treat them as such. The experiences of spousal and adult child caregivers are substantively affected by their relationship histories and family dynamics (Statz et al., 2021). For spouses, caregiving is often considered an act of love or fulfillment of marriage vows (Statz et al., 2021), and as they uphold their relative’s familial identity, so too is their own role and sense of self reinforced by their relative (Avidor & Ayalon, 2022; Whitaker, 2009). As such, being separated from their relative in care during the pandemic profoundly influenced spousal caregivers’ role identity. As illustrated elsewhere (e.g., Brody, 2004; Stephens et al., 2001), participating adult daughters encountered role conflict and overload as they sought to balance their caregiving role with the competing demands of additional social roles (e.g., mother, wife, employee). Adult daughters spoke of the guilt they experienced at being unable to reciprocate the care received from their parents during childhood, a role that has previously been shown to increase caregiving gratification (Wright & Aquilino, 1998).
Although person-centered care approaches, with their requisite inclusion of the resident, their families and care providers, are increasingly implemented in long-term care settings (Backhaus et al., 2020), our findings highlight the disconnect between care philosophies and practice. Such disconnect has been noted elsewhere; for example, Puurveen and colleagues (2019) noted how, prepandemic, family participation in care conferences was frequently viewed as tokenistic, tempering family caregivers’ ability to advocate for their relative’s care. The experiences of study participants demonstrate the primarily performative nature of family-inclusive care philosophies (see also Hoek et al., 2021; Holmgren et al., 2014; Koster & Nies, 2022) as they were swiftly denied and/or limited in their access to their relatives. With minimal opportunities to advocate for themselves and their relative, participants were left feeling aggrieved and betrayed.
Our findings and others (Avidor & Ayalon, 2022; Nash et al., 2021) suggest that families’ experiences have caused significant trauma, which has in turn only further exacerbated the betrayal, mistrust, and cynicism felt toward care home and health authority administrators, policy makers, and the long-term care system at large (Dupuis-Blanchard et al., 2021; Ickert et al., 2021). Such sustained distrust may lead to a sense of institutional betrayal (Ashana et al., 2020; Lewis et al., 2019; Smith, 2017). Utilizing a trauma-informed approach to care, such as that used in child/youth or adult inpatient settings (e.g., Muskett, 2014), may offer a meaningful way to address the trauma and institutional betrayal felt by families. For example, Kusmaul and Anderson (2018) have adopted this approach to support care home residents experiencing unexpected and/or multiple loss(es) (e.g., death of a spouse and resultant care home placement). The approach is grounded in an assumption of previous exposure to trauma, such that interactions and service delivery center on the prevention/avoidance of retraumatization by adopting a manner appropriate to the needs of the individual. Focused on principles such as safety, trustworthiness, collaboration, and empowerment (Fallot & Harris, 2008), a trauma-informed approach would entail refining policies, modifying practices, and providing additional education/training to staff to ensure a certain sensitivity and responsiveness to family members moving forward.
Study Limitations
Although this study provides an in-depth understanding of the nuances of visitation restrictions on families’ ability to maintain relational continuity during the pandemic, several limitations exist. First, given the challenges of conducting research during a pandemic, a convenience sample was recruited via social media, resulting in the inclusion of participants whose experiences may differ from more infrequent users of social media platforms. Second, although participant demographics reflect the predominance of women’s involvement in caring for a relative in long-term care (Armstrong, 2018), men’s perspectives were limited (i.e., n = 1). Finally, our sample was relatively well-educated, affluent, and English-speaking, with only one family caregiver who identified as an ethnocultural minority. It is important to acknowledge that the social position of families may well have affected their ability to navigate and potentially minimize adverse experiences during the pandemic (e.g., Kong et al., 2010). Hence, future research will want to include a greater diversity of caregiver experiences, including those of immigrant and ethnocultural minority families.
Implications for Practice
Study findings illustrate the importance of acknowledging the variations that exist among family caregivers with a relative in long-term care. Care home administrators, policy makers, and researchers must recognize that the motivations and involvement of spousal caregivers may differ from those of adult children and thus refrain from treating them as a homogeneous group. Similarly, care home administrators and policy makers are encouraged to adopt a “nuanced and compassionate” approach that acknowledges the complexities of family involvement (Mitchell et al., 2021, p. 335), recognizing that family members offer hands-on assistance and socioemotional supports that extend beyond those provided by staff, to preserve resident identity, dignity, and continuity of routine.
We concur with Whitaker (2009) that categorizing family involvement and engagement purely by visit frequency (e.g., daily vs. monthly) or the extent to which hands-on assistance is provided (e.g., grooming, meal assistance, ambulation) does not fully capture family members’ contributions and thus should not provide the basis for determining whether a family member is essential. As such, long-term care providers must work with public health officials to ensure visitation policies adopt a more holistic, person-centered approach that attends to the social and relational aspects underlying familial involvement and ensures a balance between residents’ physical and mental well-being, and infection prevention and control. In recognition of the dynamic and interdependent nature of relational continuity, care home staff are encouraged to ensure that a resident’s social history captures their family dynamics and the extent to which multiple family members may be involved in their care. In turn, such documentation would prove useful for determining which family members are granted entry during subsequent outbreaks.
Given the inefficacious application of virtual communication technologies during periods of lockdown, virtual visits should not be considered the default option during prolonged periods of isolation for residents with sensory and/or cognitive impairments. Rather, care providers and public health officials are encouraged to maximize opportunities for in-person visits through consistently enforced vaccination policies and rapid-testing opportunities (Mitchell et al., 2021). As Hindmarch and colleagues (2021) argue, family involvement/visitation during an outbreak is not simply a dichotomous choice (i.e., close doors or grant access). Rather, it is about mitigating risk while supporting the relational work that family caregivers perform, ideally through the formalization of family roles within long-term care homes and the inclusion of families in policy development (Gaugler & Mitchell, 2021). Finally, care homes are also encouraged to build upon the work of Kusmaul and Anderson (2018) and adopt a care culture and processes that incorporate trauma-informed approaches to ensure family caregivers have the ability to sustain relational continuity without the potential for re-traumatization.
Conclusion
This study sought to understand the experiences of family caregiving in long-term care during the COVID-19 pandemic within British Columbia, Canada. Our findings illustrate the significance of the intangible aspects of family caregiving, in this case maintaining the relational continuity between family caregiver and resident through the confirmation of reciprocal relationships: daughter and parent, husband and wife, grandchild and grandparent. Restrictive visitation protocols put in place at the beginning of the pandemic disrupted and impeded this aspect of family caregiving, resulting in profound distress and trauma among participants who endeavored to uphold their relative’s identity and position within the family while at the same time maintaining their own roles and sense of self. It is clear moving forward that families and care home staff are not interchangeable and that preventing family caregivers from entering care homes during a pandemic disregards the symbolic and ritualistic aspects of relational continuity that is essential to upholding resident and caregiver identity.
Footnotes
Acknowledgements
The authors wish to express their heartfelt appreciation for the family caregivers who gave their time and energy to share their stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided through Dr. Baumbusch’s Canadian Institutes of Health Research Chair in Sex and Gender Science.