
Abstract
There is a lack of knowledge about the successful implementation of family nursing practices. This scoping review maps current knowledge about the implementation of evidence-informed family nursing practices across settings and populations. A systematic search (CINAHL, PubMed, Medline) identified 24 publications, published between 2010 and 2020. We found nurses’ implementation experience to be one of disruption, learning, and moving to new ways of practicing. The implementation resulted in benefits to families and self but was marked by fluctuation and partial integration of evidence-informed family nursing practices into care delivery. Uptake was shaped by various contextual determinants, with barriers mainly at the team and organizational levels. We identified low-quality, tentative evidence that capacity-building strategies coupled with dissemination-educational strategies may enable family nursing practice skills and increase the quality of family care. More rigorous research is needed to build further knowledge about effective implementation. Future implementation endeavors should utilize the evolving knowledge base in family nursing and tailor implementation strategies to contextual barriers.
Keywords
Health care systems across the globe are challenged to better integrate evidenced-based practices into routine care delivery to increase the quality and effectiveness of care (Curtis et al., 2017). Over the last decade, attention has been given to implementation efforts that aim to narrow the know-do gap in health care delivery to patients and their families (Rapport et al., 2018; Wensing & Grol, 2019). Despite these efforts, recent estimates suggest that only about 60% of health care practices are based on research evidence, about 30% is of low value or unnecessary, whereas about 10% is even harmful (Braithwaite et al., 2020). Scientific knowledge of effective implementation processes is necessary to ensure sustainable and cost-effective integration efforts (Dolansky et al., 2017; Wensing & Grol, 2019; Zullig et al., 2020).
For more than a decade, family nurses have pointed to the need to optimize family nursing and care knowledge translation into practice (Bell, 2014; Duhamel, 2010; Duhamel & Dupuis, 2011; Leahey & Svavarsdottir, 2009; van Achterberg et al., 2008). Several knowledge translation research projects have been conducted (Davidson & Zisook, 2017; Duhamel et al., 2015; Kläusler-Troxler et al., 2019; Svavarsdottir et al., 2012). At present, however, there is still a lack of knowledge synthesis about the context, process, and outcomes of implementation efforts that focus on the integration of evidence-based family nursing practices across populations and health care settings.
Background
Proactive engagement of and support for families who are affected by acute health events and persistent illnesses have long been called for (Bell, 2013; Carman et al., 2013; Smith et al., 2020; Wright & Leahey, 1984, 2013). Redesign of health care delivery to encompass an active partnership among patients, families, and health professionals is now the gold standard to achieve better quality and more effective care and to ensure improved health and well-being (Carman et al., 2013; Frampton et al., 2017; Giap & Park, 2021). Nurses who work at the point of care play a key role in engaging family members in care and in supporting patients and families in their individual and family-level self-care and illness management (Kaakinen et al., 2018)
Several reviews have been undertaken to determine the evidence of an active partnership with families, operationalized here as any nursing practices that involve, engage, and support family members and family systems in care delivery and in disease or illness management processes (Chesla, 2010; Giap & Park, 2021; Gilliss et al., 2019; Smith et al., 2020). In the context of persistent illness, a beneficial impact of psycho-educational and relationship-focused family interventions on the individual patient and family member’s mental health has been found (Deek et al., 2016; Hartmann et al., 2010; Hopkinson et al., 2012; Park et al., 2018). Patient’s physical health and self-care ability may also be improved (Hartmann et al., 2010; Hopkinson et al., 2012; Park et al., 2018; Smith et al., 2020). There is also some indication of improved family functioning (Östlund & Persson, 2014; Smith et al., 2020) and reduced health care utilization, such as length of stay (Park et al., 2018). Family engagement practices have also been found to improve patient safety outcomes, such as a reduction in adverse events or a sense of safety and satisfaction (Giap & Park, 2021; Lee et al., 2021; Mackintosh et al., 2020; Park & Giap, 2020).
Despite the mounting evidence and encouraging empirical insights about the usefulness and effectiveness of engaging and supporting families in care during acute and persistent illness processes, integration of family nursing into routine care delivery has been slow and partial (Bell, 2014; Leahey & Svavarsdottir, 2009). While several implementation efforts have been undertaken, there remains a lack of knowledge on how to best integrate family nursing knowledge into practice to ensure the consistent delivery of evidence-informed family nursing care and interventions. No review to date has been undertaken to synthesize current research knowledge on the implementation of evidence-based family nursing practices. Knowledge synthesis research is necessary to build an empirical foundation on family nursing implementation, namely, on implementation barriers and context-sensitive, effective implementation strategies (Bauer & Kirchner, 2020). To contribute to the growing body of knowledge in family nursing implementation science, we undertook a scoping review that mapped the current knowledge on the implementation of evidence-informed family nursing practices into clinical care delivery across settings and populations. The research questions to guide this scoping review were as follows:
Method
Study Design
A scoping review methodology was chosen as the most fitting approach to identify the knowledge landscape about the implementation of evidence-informed family nursing practices. Scoping reviews investigate broad research questions and are particularly useful when mapping a new terrain (Colquhoun et al., 2014; Peters, Godfrey, McInerney, et al., 2015). We used the methodological steps outlined by Arksey and O’Malley (2005) and Levac et al. (2010), which include (a) developing a research question; (b) identifying relevant studies through a comprehensive search strategy; (c) selecting the studies; (d) extracting and charting the data; and (e) and collating, summarizing, and reporting the findings. For the reporting of the scoping review, we followed the PRISMA 2020 guideline (Page et al., 2021) and an extension for scoping reviews (Tricco et al., 2018).
The Model of Implementation Research (Proctor et al., 2009) served as the overall framework to organize the concepts for our scoping review. The model specifies four concepts, namely, the intervention (i.e., the what), the implementation strategies (i.e., the how), the context of the implementation, and outcomes (including implementation, service, and health outcomes). For this scoping review, we defined “evidence-informed family nursing practices” as the intervention. We then focused our analysis on (a) implementation strategies and experiences; (b) the context and how contextual determinants influence implementation and intervention delivery; and (c) the outcomes of the implementation efforts.
Data Sources and Search Strategy
We conducted an iterative search by first identifying key publications based on a rapid electronic data search. In a second step, we developed a detailed search strategy. Searches of the electronic databases, CINAHL, PubMed, and Medline, were undertaken in December 2020. The search strategy included various combinations of the following search terms: (a) “family nursing”, “family systems nursing”, “family centered care”, family focused care”, “family engagement”, “family involvement”, “family support”; (b) “knowledge translation, “knowledge transfer”, “implementation science”, “implementation strategy”; (c) “evidence-based models,” “knowledge”; and (d) “enablers,” “barriers,” “facilitator”, “behavior” and “attitude”. Search terms were a mixture of database-controlled keywords, including MeSH headings, subject headings, and keywords (see Supplementary File 1). Reference lists were also screened for relevant publications.
Study Selection Criteria and Process
Publications were included if they were systematic reviews or peer-reviewed research publications, including qualitative, quantitative, or mixed-methods designs, and had been published in published ≥2010, either in English or German. Hence, studies needed to (a) target nursing care delivery in any setting, clinical area, and population; (b) focus on the implementation of evidence-informed family nursing practices, such as Family Systems Nursing, family-centered care, family engagement practices, or family-focused interventions; and (c) investigate implementation processes or contexts. No restrictions were applied to the investigated outcomes. In addition, the study population needed to include nurses, among others, and/or patients and family members. Non-data-based publications, and those not focusing on the implementation of an evidence-informed family nursing practice, were excluded.
Search results from databases were imported into Endnote to remove duplicates and manage the selection process. No systematic review management system or automation tool was used. First, one reviewer (E.T.) screened all records for eligible studies based on title and abstract. If uncertain, the potential study was included for full-text review. Full texts were then retrieved. Next, two reviewers (E.T. and R.N.) independently assessed full texts for eligibility, classifying them into “include,” exclude,” and “to be discussed.” Discrepancies were discussed among the two reviewers. In case of disagreement, a third reviewer (L.V.) was consulted until consensus was reached, which was the case for all discrepancies.
Data Extraction
Data items were extracted for each study using an extraction template on study characteristics (year, country, and aim); methods (design, theoretical framework, setting, population, data collection, and measures); intervention and implementation information (type of evidence-informed family nursing practices and type of implementation focus, such as strategy or context); and study outcomes by one reviewer (ET) and verified by a second reviewer (RN). We then extracted data according to the constructs of interest (i.e., evidence-informed family nursing practices, implementation strategy/process, context, and outcomes according to Proctor) in an Excel sheet. Next, we displayed extracted data in a mind map to create a preliminary overview of the knowledge landscape. Finally, we extracted qualitative and quantitative data in separate tables for further analysis. Consistent with the scoping review methodology, no study risk of bias or quality assessment was undertaken (Peters, Godfrey, McInerney, et al., 2015; Peters, Godfrey, Khalil et al., 2015).
Data Charting and Synthesis
To analyze and synthesize qualitative insights, we first organized qualitative findings into four preliminary categories that we had identified after a first reading of the extracted data and informed by the Model of Implementation Research, namely, implementation strategy, experience with implementation and integration of evidence-informed family nursing practices, contextual determinants, and benefit/outcomes. Two researchers (ET and RN) then coded the extracted qualitative findings for each category separately, discussed emerging themes, and organized them into overarching themes. Next, the researchers organized the identified contextual determinants influencing and shaping the implementation process and uptake according to different levels of aggregation, mapped them to the domains and constructs of the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009), and assessed whether they were described as enabling, limiting, or both. Finally, one researcher (R.N.) categorized the investigated outcomes using Proctor’s implementation (i.e., uptake, fidelity, cost, sustainability), service (i.e., safety, patient-centeredness, effectiveness), and health outcomes (i.e., symptoms, satisfaction.; Proctor et al., 2009), which was verified by a second researcher (E.T.). As many studies investigated outcomes on nurse characteristics, we added the category “nurse outcomes.” Subsequently, one researcher (R.N.) analyzed the direction of study results and narratively summarized them according to each outcome, paying attention to the type of implementation strategy that was used. Regular analytical meetings were held to ensure a systematic and transparent process. Each analytical step was discussed among the involved researchers, and analytical decisions were made as a team.
Findings
Study Characteristics
The search yielded 857 records of which 636 were retrieved. After removal of duplicates and screening of title and abstract, 116 records remained that were assessed for eligibility based on full text. Twenty-four publications met the inclusion criteria. Reasons for the exclusion of the 92 publications are listed in Figure 1. The rate of concordance between the two raters (E.T. and R.N.) was 72% (n = 84).
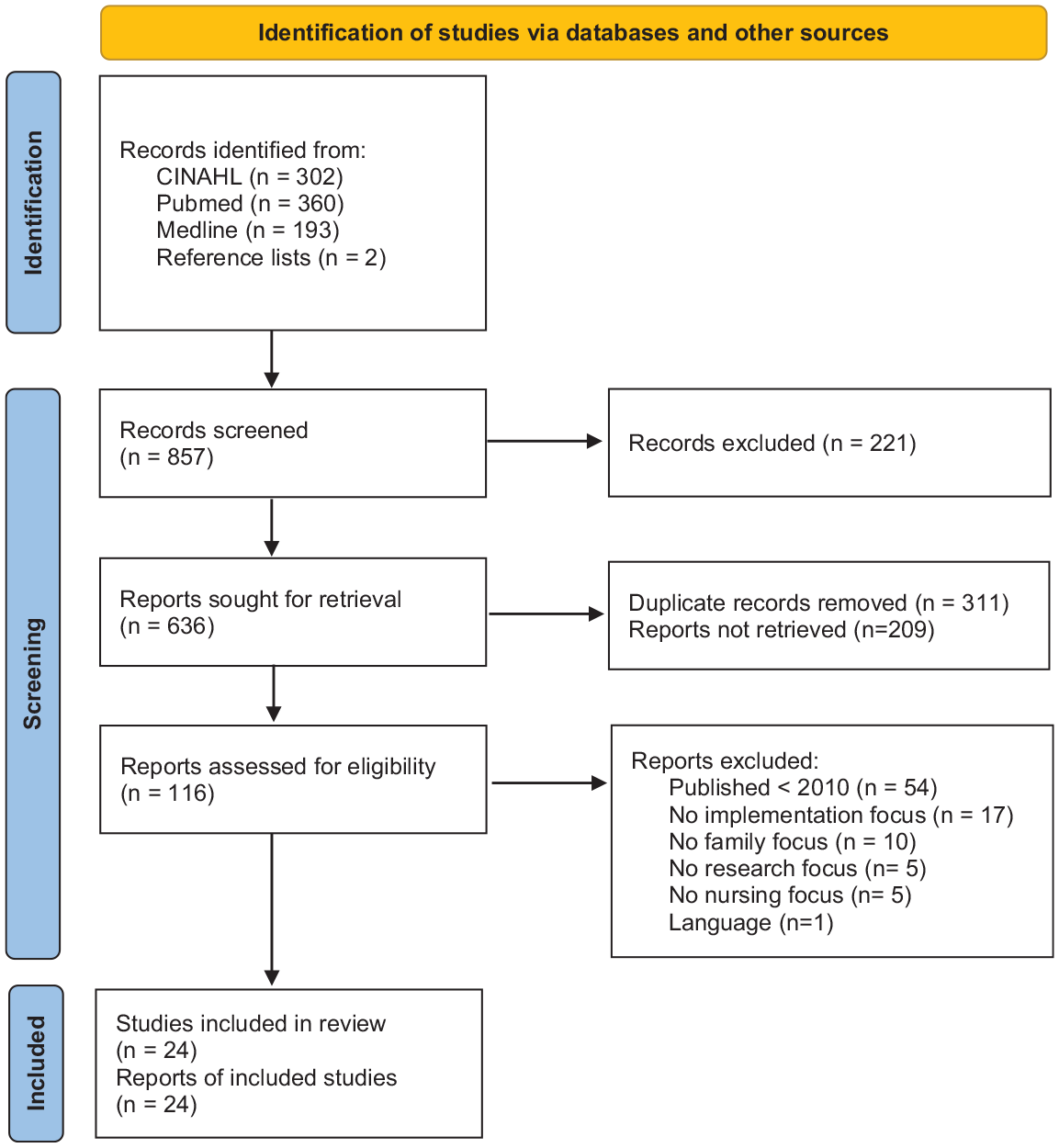
PRISMA flow.
Of the 24 included studies, 11 studies implemented a family-centered care approach (Boztepe & Kerimoğlu Yıldız, 2017; Gomes da Silva et al., 2016; Hamilton et al., 2020; Kleinpell et al., 2019; MacKay & Gregory, 2011; Maree et al., 2017; Mirlashari et al., 2019; Shah-Anwar et al., 2019; Toivonen et al., 2019; Weis et al., 2014; Wells et al., 2014). Ten studies implemented Family Systems Nursing (Beierwaltes et al., 2020; Blöndal et al., 2014; Eggenberger & Sanders, 2016; Naef, Kaeppeli et al., 2020; Naef, Kläusler-Troxler et al., 2020; Petursdottir et al., 2019; Svavarsdottir et al., 2015; Wong, 2014; Zimansky et al., 2018, 2020). Three studies implemented a family-focused intervention program (Antolick et al., 2020; Duke et al., 2020; Wells et al., 2014; see Table 1). Only eight studies reported on the use of an implementation science framework of which five used the Knowledge-to-Action (KTA) Framework. The Consolidated Framework for Implementation Research (CFIR), Promoting Action on Research Implementation in Health Services (PARIHS), and Plan-Do-Study-Act (PDSA) cycle were each used once.
Overview of Included Studies (n = 24).
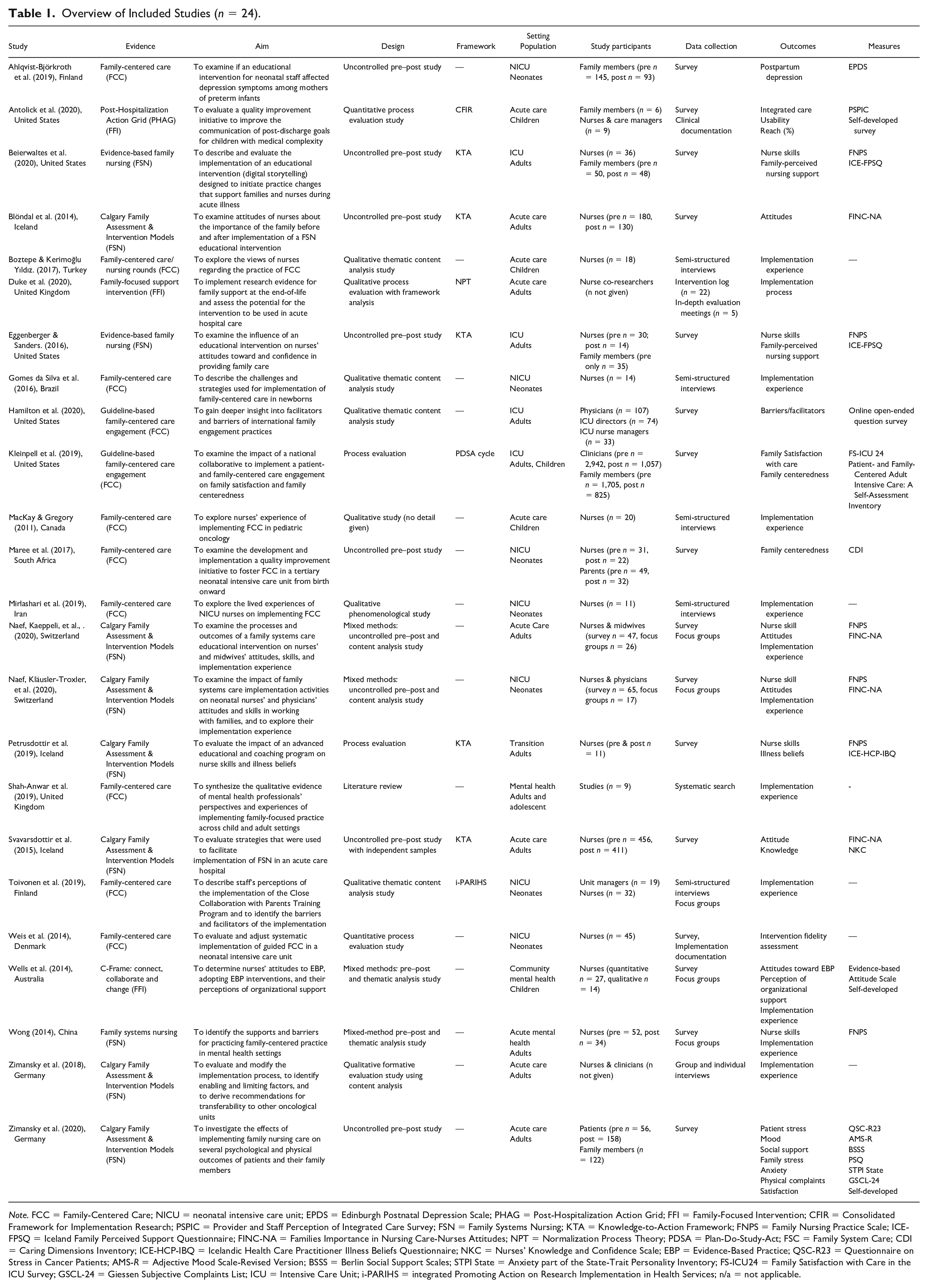
Note. FCC = Family-Centered Care; NICU = neonatal intensive care unit; EPDS = Edinburgh Postnatal Depression Scale; PHAG = Post-Hospitalization Action Grid; FFI = Family-Focused Intervention; CFIR = Consolidated Framework for Implementation Research; PSPIC = Provider and Staff Perception of Integrated Care Survey; FSN = Family Systems Nursing; KTA = Knowledge-to-Action Framework; FNPS = Family Nursing Practice Scale; ICE-FPSQ = Iceland Family Perceived Support Questionnaire; FINC-NA = Families Importance in Nursing Care-Nurses Attitudes; NPT = Normalization Process Theory; PDSA = Plan-Do-Study-Act; FSC = Family System Care; CDI = Caring Dimensions Inventory; ICE-HCP-IBQ = Icelandic Health Care Practitioner Illness Beliefs Questionnaire; NKC = Nurses’ Knowledge and Confidence Scale; EBP = Evidence-Based Practice; QSC-R23 = Questionnaire on Stress in Cancer Patients; AMS-R = Adjective Mood Scale-Revised Version; BSSS = Berlin Social Support Scales; STPI State = Anxiety part of the State-Trait Personality Inventory; FS-ICU24 = Family Satisfaction with Care in the ICU Survey; GSCL-24 = Giessen Subjective Complaints List; ICU = Intensive Care Unit; i-PARIHS = integrated Promoting Action on Research Implementation in Health Services; n/a = not applicable.
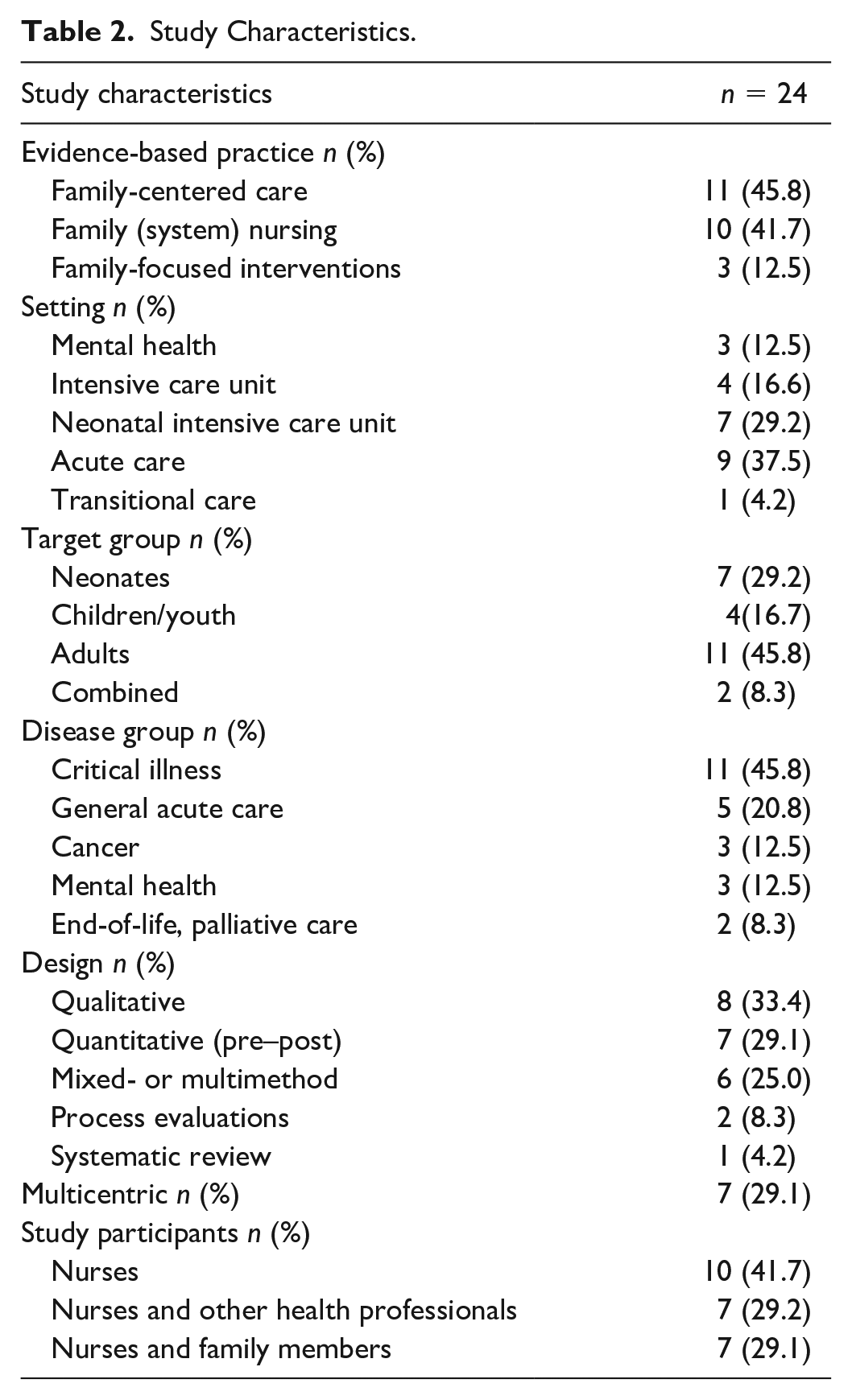
Study characteristics are reported in Table 2. Studies were conducted predominantly in Europe (n = 13), followed by the United States, and Canada (n = 6). A majority of the studies were carried out in acute-critical care (83.3%). Eight studies used a qualitative design, seven were uncontrolled pre–post quantitative studies, six were mixed- or multimethod studies, two were process evaluations, and one was a literature review. Sample sizes in qualitative studies (including qualitative components of mixed-methods studies) were adequate, with a median sample size of n = 20 (interquartile range [IQR] 16–31; minimum 11–max 214) participants. Median sample sizes in quantitative designs included n = 65 (IQR 46.0—115.5; minimum 11–maximum 4,647) participants during pre-data collection, and a median of n = 54 (IQR 30.5–111.5; minimum 11–maximum 1,882) participants for post-data collection.
Study Characteristics.
Implementation Strategies and Experiences
A total of 18 studies specified their implementation strategies. Most implementation efforts entailed an educational component, which was, except for one study (Wong, 2014), combined with the use of a local implementation team or champion/facilitator roles that provided clinical mentoring and supervision (Ahlqvist-Björkroth et al., 2019; Beierwaltes et al., 2020; Blöndal et al., 2014; Eggenberger & Sanders, 2016; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Svavarsdottir et al., 2015; Toivonen et al., 2019; Weis et al., 2014; Zimansky et al., 2018, 2020). Others used a quality improvement methodology that combined feedback loops and local capacity-building strategies (Antolick et al., 2020; Duke et al., 2020; Kleinpell et al., 2019; Maree et al., 2017), and one study did not provide sufficient detail (Wells et al., 2014). Most studies reported using more than one strategy (83%), with a median of three (minimum 1–maximum 5). None reported having tailored implementation strategies to identified barriers. The median duration of the implementation efforts was 8 months (3–24 months, reported by 11 of 18 studies).
Three thematic threads were identified that depicted nurses’ and clinicians’ experience of implementing evidence-informed family nursing practices, based on the findings of 15 studies (Boztepe & Kerimoğlu Yıldız, 2017; Duke et al., 2020; Gomes da Silva et al., 2016; Hamilton et al., 2020; Kleinpell et al., 2019; MacKay & Gregory, 2011; Mirlashari et al., 2019; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Shah-Anwar et al., 2019; Toivonen et al., 2019; Wells et al., 2014; Wong, 2014; Zimansky et al., 2018; see Figure 2).
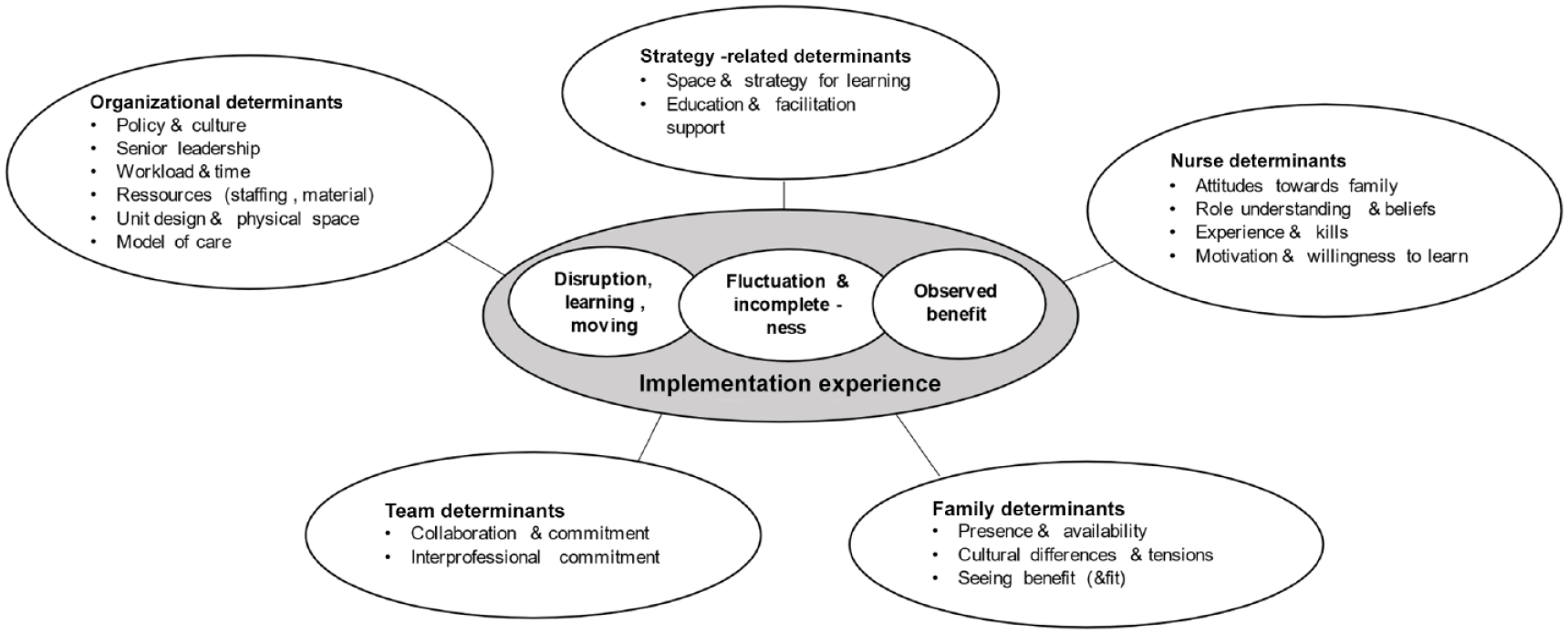
Overview of thematic findings related to implementation strategy and context.
First, implementation entailed disruption, learning, and moving to new ways of practicing with families, which was reported in nine studies (Boztepe & Kerimoğlu Yıldız, 2017; Duke et al., 2020; MacKay & Gregory, 2011; Mirlashari et al., 2019; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Shah-Anwar et al., 2019; Wong, 2014). The introduction of evidence-informed family nursing practices involved the disruption of habitual practices and care processes, as Duke and colleagues (2020) reported: “(It) pulled apart their practice (by) flipping conversations to focus on the family” (pp. 7–8). It required exploring different ways of working with families and a need for conscious learning or unlearning. Nurses were challenged to rethink their role, their view of family, and their understanding of family responses to illness; that is, develop a “new ability to think family” (Wong, 2014, p. 215). The movement toward the use of the evidence-informed family nursing practices became evident in statements such as “family defines who constitutes their members (and) copes in their own ways” (MacKay & Gregory, 2011), “new awareness for family with intentional engagement” (Naef, Kaeppeli, et al., 2020), “parents know their child best, (need to be) near to the child, (and want to) participate in care” (Boztepe & Kerimoğlu Yıldız, 2017), or “offering empathy and create a win-win situation” (Mirlashari et al., 2019).
Second, the implementation process was marked by fluctuation and incompleteness, which was reported in four studies (Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Wong, 2014; Zimansky et al., 2018). Moving to new ways of practicing involved tensions and frictions within teams and the organizational context and was supported by nurse insights about the evidence-informed family nursing practices as feasible and fitting within their clinical area and population served. Studies report that it was not a linear, progressive process but occurred in waves, involving resistance, stand-still, and forward movement. For example, Naef, Kläusler-Troxler and colleagues (2020) found that nurses experienced implementation like a “wheel that moved forward or stood still, depending on the amount of challenges faced in everyday clinical work and organizational context” (p. 7). As a result, evidence-informed family nursing practices were often not fully integrated into routine care after the active implementation efforts were completed. This partial or incomplete (or unfinished) uptake occurred in relation to the intervention’s or model’s core components but also may have pertained to the extent to which eligible families could be reached. Some components tended to be incorporated more readily into practice, such as providing information and advice, or involving families in care (Naef, Kläusler-Troxler, et al., 2020; Wong, 2014). In contrast, family assessment or family-focused intervention strategies were less often or only partially adopted (Naef, Kläusler-Troxler, et al., 2020; Zimansky et al., 2018).
Third, nurses and other clinicians observed benefits in quality of care (Duke et al., 2020; Petursdottir et al., 2019; Toivonen et al., 2019; Wells et al., 2014; Wong, 2014), which encouraged implementation. For example, nurses experienced their work as “more effective” (Petursdottir et al., 2019) and as “enhancing family care” (Duke et al., 2020). They experienced “improved relationships that led to increased collaboration and partnership with families” (Wells et a., 2014) and “deeper understanding and respect for family care” (Duke et al., 2020). They also reported finding their own clinical work to be “more meaningful and satisfying” (Duke et al., 2020; Wong, 2014). One study also reported benefits for families, including “empowerment and self-confidence” (Wells et al., 2014).
Contextual Determinants Enabling or Limiting Implementation
Fourteen studies reported findings about the contextual determinants of implementation efforts (Boztepe & Kerimoğlu Yıldız, 2017; Duke et al., 2020; Gomes da Silva et al., 2016; Hamilton et al., 2020; Kleinpell et al., 2019; MacKay & Gregory, 2011; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Shah-Anwar et al., 2019; Toivonen et al., 2019; Wells et al., 2014; Wong, 2014; Zimansky et al., 2018). We found that implementation was shaped by determinants pertaining to the strategy, individual (i.e., nurse, family), interpersonal (i.e., team), and community or organizational factors (see Table 3).
Contextual Determinants (n = 14).
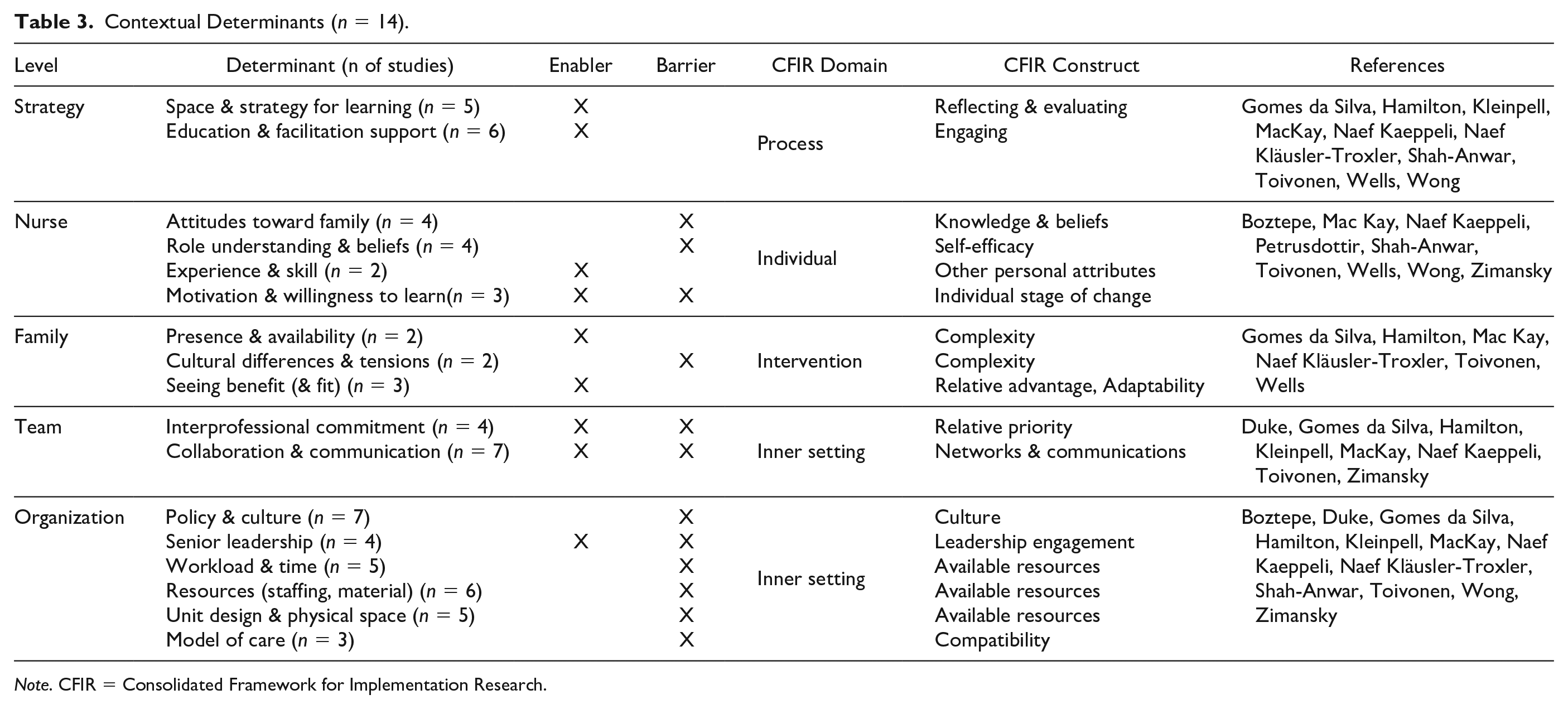
Note. CFIR = Consolidated Framework for Implementation Research.
Strategy-Related Determinants
We identified two enablers pertaining to the implementation strategy. First, strategies were supportive when they created a space for mutual learning and encompassed ongoing opportunities through experiential learning methods and guidance from mentors.
Nurse Determinants
Attitudes, role understanding, and beliefs were most often reported as barriers to the integration of evidence-informed family nursing practices. Motivation and willingness to learn arose as both enabling and limiting factor, whereas clinical experience and skills were predominantly enablers.
Family Determinants
Seeing benefits for the families and self was enabling integration. In terms of family-related determinants, the complexity of family situations played a role, with family presence or availability enabling engagement and support, whereas cultural differences between families and clinicians, or tensions within the family or between the family and clinicians increased the complexity, thereby posing barriers.
Team Determinants
Team-related factors arose as core determinants for successful integration, with their absence stifling implementation efforts. Hence, a shared understanding, commitment, and governance that include all members of an interprofessional team together with participatory models of care delivery were essential success factors.
Organizational Determinants
Organizational level factors were named most frequently (30 codes). Except for leadership, which was also reported to be an enabler, organizational determinants often disabled uptake and in particular long-term integration. Cultural aspects, including policy, and available resources (workload, staffing) were the main barriers.
When matching the identified barriers/enablers to the CFIR, those determinants relating to CFIR inner setting (i.e., organizational context) and process (i.e., strategy) domains were most frequently reported, followed by the CFIR individual (i.e., nurse and other professionals) and intervention (i.e., family) domains. No societal or system-level determinants; that is, constructs within the CFIR outer setting domain were described. It is noteworthy that most implementation strategies were targeting an individual or interpersonal determinants and only a few employed strategies targeting organizational determinants although most barriers were described in the CFIR inner context domain.
Outcomes of Implementation
A total of 15 studies assessed the impact of implementation efforts on outcomes (see Table 4).
Impact of Implementation Strategies on Outcomes (Quantitative Findings; n = 15).
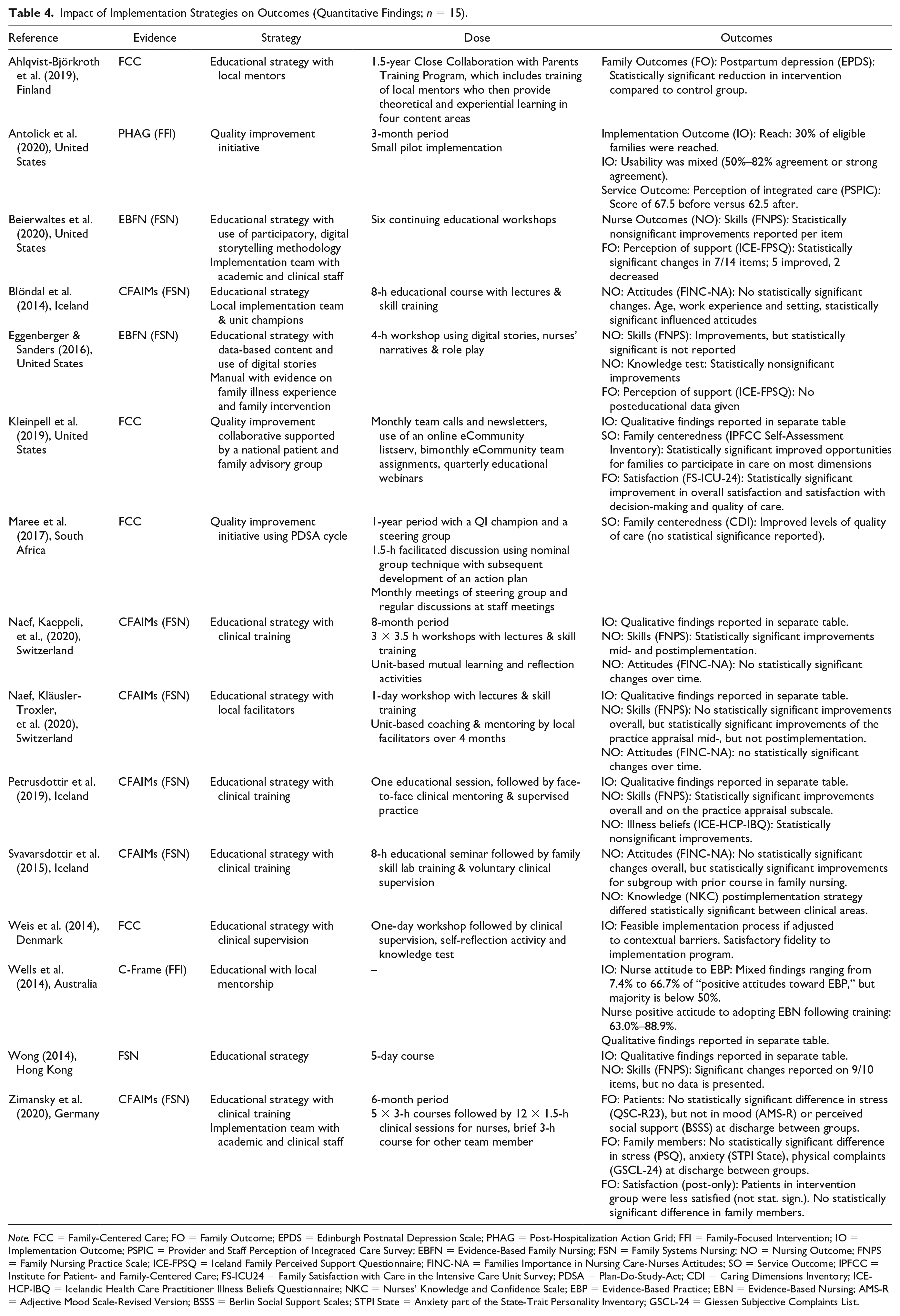
Note. FCC = Family-Centered Care; FO = Family Outcome; EPDS = Edinburgh Postnatal Depression Scale; PHAG = Post-Hospitalization Action Grid; FFI = Family-Focused Intervention; IO = Implementation Outcome; PSPIC = Provider and Staff Perception of Integrated Care Survey; EBFN = Evidence-Based Family Nursing; FSN = Family Systems Nursing; NO = Nursing Outcome; FNPS = Family Nursing Practice Scale; ICE-FPSQ = Iceland Family Perceived Support Questionnaire; FINC-NA = Families Importance in Nursing Care-Nurses Attitudes; SO = Service Outcome; IPFCC = Institute for Patient- and Family-Centered Care; FS-ICU24 = Family Satisfaction with Care in the Intensive Care Unit Survey; PDSA = Plan-Do-Study-Act; CDI = Caring Dimensions Inventory; ICE-HCP-IBQ = Icelandic Health Care Practitioner Illness Beliefs Questionnaire; NKC = Nurses’ Knowledge and Confidence Scale; EBP = Evidence-Based Practice; EBN = Evidence-Based Nursing; AMS-R = Adjective Mood Scale-Revised Version; BSSS = Berlin Social Support Scales; STPI State = Anxiety part of the State-Trait Personality Inventory; GSCL-24 = Giessen Subjective Complaints List.
Implementation Outcomes
Quantitative assessment of implementation outcomes was undertaken in three very small studies with 6 to 45 participants (Antolick et al., 2020; Weis et al., 2014; Wells et al., 2014). Antolick and colleagues (2020), in their pilot evaluation of a family-focused discharge planning process for children with medical complexity, found that 30% of eligible families were followed up, of which 28% completed the discharge planning process. Provider-perceived usability was mixed (n = 6). Weis and colleagues (2014), reporting on a systematic implementation process for introducing guided, family-centered care and communication in the neonatal intensive care unit (NICU), reported protracted and partial uptake, with about half (55%) of nurses completing the training (n = 45). Finally, Wells and colleagues (2014), analyzing the implementation of a strengths-based, solution-focused, and evidence-based family-focused intervention in community mental health, found high acceptability (92.6%) and willingness to use the evidence-based interventions (100%; n = 27) but did not report on the actual results of the implementation efforts. Overall, assessment of implementation outcomes was very limited, and reporting was of moderate to poor quality.
Nurse Outcomes
Nurse outcomes, such as skills (n = 6), attitudes (n = 4), and knowledge (n = 3), were the most frequently investigated type of outcome (n = 8 studies; Beierwaltes et al., 2020; Blöndal et al., 2014; Eggenberger & Sanders., 2016; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Svavarsdottir et al., 2015; Wong, 2014). Educational strategies, coupled with clinical supervision, training activities, or local champion roles, improved nurse’s skill in working with families (as measured with the Family Nursing Practice Scale; Beierwaltes et al., 2020; Eggenberger & Sanders, 2016; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019; Wong, 2014) and reached statistical significance in half of the studies (Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Petursdottir et al., 2019). Nurses’ attitudes toward families, as assessed with the Families’ Importance in Nursing Care—Nurses’ Attitudes, did not change because of these implementation efforts (Blöndal et al., 2014; Naef, Kaeppeli, et al., 2020; Naef, Kläusler-Troxler, et al., 2020; Svavarsdottir et al., 2015). Findings on nurses’ knowledge are very limited and nonsignificant (Eggenberger & Sanders., 2016; Svavarsdottir et al., 2015). They unanimously focused on the implementation of family nursing knowledge or Family Systems Nursing in a variety of clinical settings, most often in acute-critical care, and used the same or similar outcome measures.
Service Outcomes
Services outcomes, including the level of family-centeredness (Kleinpell et al., 2019; Maree et al., 2017) or integrated care (Antolick et al., 2020), were obtained in three studies. Two studies, which focused on the implementation of a family engagement or family-centered care practices in intensive care unit (ICU), using quality improvement strategies coupled with local capacity building (Kleinpell et al., 2019; Maree et al., 2017), found an increase in family-centeredness. Kleinpell and colleagues (2019), in their multicenter study that included almost 4,000 adult ICU clinicians (pre n = 2,924, post n = 1,057), identified statistically significant improved opportunities for families to participate in care on most of the assessed dimensions. Improved levels of family-centeredness in NICU were also found by Maree and colleagues (2017) from both nurses’ and parents’ perspectives, but the small sample size did not allow for statistical testing. One study pilot-implemented a family-focused discharge planning process for children (Antolick et al., 2020) and was unable to show improvements in staff-perceived care integration, which may be due to the very small sample size. Conclusions on service outcomes remain predominantly based on the largest study included in this scoping review (Kleinpell et al., 2019), which suggests that capacity-building strategies might be potentially effective in improving the intended service outcome, that is, family-centered engagement practices.
Family Health Outcomes
Family outcomes, including perceived nurse support (Beierwaltes et al., 2020; Eggenberger & Sanders, 2016), families’ satisfaction with care (Kleinpell et al., 2019; Zimansky et al., 2020), and mental health outcomes (Ahlqvist-Björkroth et al., 2019; Zimansky et al., 2020), were measured in five studies. Two small studies in adult ICU (Beierwaltes et al., 2020; Eggenberger & Sanders, 2016) investigated families’ perception of cognitive and emotional support received by nurses. One study found statistically significant improvements in half of the items measured (Iceland Family Perceived Support Questionnaire), with two showing a decrease in family-perceived support (Beierwaltes et al., 2020), whereas the other study did not provide post-implementation data (Eggenberger & Sanders, 2016).
The multicenter study in adult ICU (Kleinpell et al., 2019) found a statistically significant increase in families’ satisfaction with care as measured with the well-established FS-ICU-24 (Family Satisfaction with Care in ICU: pre mean 85.2 vs. post mean 86.3 out of a score ranging from 0 to 100, p < .05). In contrast, Zimansky and colleagues (2020) were unable to demonstrate an increase in family member satisfaction, using a self-developed tool, following the implementation of Family Systems Nursing in cancer care. The same study was also unable to identify a difference in family member stress, anxiety, or physical complaints when comparing an independent pre- and post-sample of 122 family members in total (Zimansky et al., 2020). In contrast, Ahlqvist-Björkroth and colleagues (2019) were able to demonstrate a reduction in maternal postpartum depression (change of 2.54 points in depression score, p < .001) following an educational implementation strategy introducing family-centered care (Close Collaboration with Parents) in the NICU. Overall, findings on family outcomes are modest and mixed and difficult to interpret, given the uncontrolled nature of study designs, mostly small sample sizes, and variety of measures used.
Discussion
This scoping review of 24 publications stemming from 14 countries identified nurses’ implementation experience to be one of disruption, learning, and moving to new ways of practicing, which resulted in observable benefits to families and self. However, it was marked by fluctuation and partial uptake of evidence-informed family nursing practices in routine care delivery. Uptake was shaped by various contextual determinants, which were more often perceived to be barriers than enablers, particularly at the organizational or inner context level. We identified low-quality and very tentative evidence that capacity-building strategies coupled with dissemination-educational strategies may be beneficial to enable nurse skills and family-centered care delivery.
The findings of individual studies included in this review were quite homogeneous in terms of implementation experience, identified barriers/enablers, and investigated outcomes, which increases the credibility of the synthesized findings in this review. The included studies focused most often on acute-critical care settings. Interestingly, we found few cultural variations although studies from 14 countries were represented in this review. One reason may be that the majority stemmed from Western cultures of which one included international data (Hamilton et al., 2020). Our findings are also in line with a recent global study on ICU family engagement, which found few differences across countries (Naef et al., 2021). However, methodological limitations make it difficult to draw reliable conclusions. Small sample sizes and uncontrolled designs mean that the knowledge gained regarding the impact of implementation strategies on outcomes is provisional at best. Most studies were monocentric. Only about half used an implementation science theory or model to guide their implementation processes, and none reported tailoring implementation strategies to previously identified barriers to implementation. The knowledge-to-action model (Duhamel, 2017; Graham et al., 2006)—a process model used to guide implementation process—was most often used, particularly in research-to-action projects in family systems care based on the Calgary Family Assessment and Intervention Models (Shajani & Snell, 2019; Wright & Leahey, 2013). Several studies used some form of stakeholder engagement or participatory methodology, which is key for tailoring implementation strategies to the local context (D. H. Peters et al., 2017; van Rooijen et al., 2021), but descriptions of the strategy design or clear operationalization were often not given. To build a body of knowledge around family nursing implementation, the use of implementation science knowledge, including theory, is important and should be enhanced (Esmail et al., 2020; Lynch et al., 2018; Nilsen, 2015).
Implementation Process
Integration of evidence-based working with families arose as a complex, fluctuating, and multifaceted process of change at different levels—it involved disruption, learning, and changing ways of seeing and doing things and is determined by individual, team, family, and organizational factors. The complexity of implementation and the bidirectional interaction of implementation strategy with contextual determinants has been previously stressed (Baker et al., 2015; Nilsen & Bernhardsson, 2019; Powell et al., 2019), suggesting that an adaptive, iterative process is necessary to ensure full integration of a new, evidence-informed practice. We observed high variability in terms of type and number of implementation strategies, which is in line with a review focusing on the implementation of nursing guidelines (Spoon et al., 2020). Educational strategies tend to be the most frequently used implementation strategy when attempting to integrate new knowledge of evidence-informed practices, but their effectiveness in achieving the desired changes remains unclear (Gutiérrez-Alemán et al., 2021).
Facilitation roles were the second most often used implementation strategy. Facilitation and the use of champion roles have been previously found to be key strategies for achieving practice change (Albers et al., 2020), and some studies within nursing found them to be promising (Dahl et al., 2018; Lessard et al., 2015; Seers et al., 2018). Strategies combining local capacity-building and creating opportunities for an ongoing process with feedback loops were also used, but many did not evaluate their effectiveness, except for one large study, which identified a positive impact on staff-perceived family-centeredness of the service and family-reported satisfaction with care (Kleinpell et al., 2019). Overall, strategies were poorly defined and operationalized, and none reported a tailoring process, that is, deciding on, matching, and adapting implementation strategies to previously identified or known contextual barriers in the given practice environment, which is a well-known challenge in implementation (Baker et al., 2015; Powell et al., 2019). Within implementation science, tailoring implementation strategies to context is considered a key factor for achieving successful integration of evidence-based intervention in routine care (Colquhoun et al., 2017; McCullough et al., 2015; Pfadenhauer et al., 2017).
Outcomes of Implementation
Among the assessed outcomes, nurses’ clinical competencies were most often measured, whereas implementation outcomes, as suggested by Proctor and colleagues (2009), were rarely evaluated. Some studies, however, provided qualitative insight into the uptake and reach. Our review found that integration is often partial in terms of components and reach, suggesting that some components of the evidence-informed intervention, practice, or programs were not, or not consistently taken up. For example, while family-centered engagement practices were often taken up, specific family assessment and intervention processes that were offered in form of (additional) family conversations, were not at all or not regularly delivery.
Some studies investigated service and family outcomes of the implementation effort, yielding a mixed picture. The small database and methodological limitation of included studies make it difficult to draw reliable conclusions. Nonetheless, our analysis showed that educational strategies alone may be insufficient to achieve uptake of evidence-informed family nursing practices. A recent review focusing on educational programs in family nursing that also included four of the studies included in our review found them to be effective in increasing nurse knowledge, attitudes, and skills in the short-term but was unable to assess whether they translated into clinical competence and application in practice (Gutiérrez-Alemán et al., 2021). In our review, we also found increased nurse skills following educational implementation activities but not in relation to attitudes and knowledge. Strategies that combine capacity-building and an ongoing process of feedback and support may be more promising in increasing quality of family care. Overall, there is a lack of methodologically sound research addressing the effectiveness of implementation strategies on implementation, service, and family outcomes, including quality of life and mental health outcomes.
Contextual Determinants
We found that the integration of evidence-informed family nursing practices is influenced by the interplay of implementation-related, nurse-related, family-related, team-related, and organization-related determinants. None of the studies investigated the outer setting domain, that is, the health system and societal aspects influencing family care (Damschroder et al., 2009). While many of the determinants identified may be both barriers and enablers, it is noteworthy the identified team and organizational determinant is perceived only, or mostly, as a barrier. These CFIR inner setting constructs (Damschroder et al., 2009), however, have rarely been targeted by the reported implementation efforts. Team communication and collaboration evolved as key determinants of implementation success. Culture, leadership, available resources, and compatibility with preexisting policies and models of care acted as barriers. Future implementation efforts need to address inner context barriers, in addition to leverage enablers identified in the other domains, such as the process (i.e., strategy), individual (i.e., nurse), and intervention domains. Hence, future implementation efforts should address organizational barriers and tailor implementation strategies to the locally identified organizational and team barriers. A context-specific implementation at the organizational level will be key to enabling successful, initial implementation of family nursing practices, and to develop a support system that will allow sustainability and sustainment of integrated family nursing practices over time (Fleiszer et al., 2016; Shelton et al., 2018).
Limitations
Our review is not without limitations. To map the knowledge terrain of evidence-based family nursing practices, we included a diversity of theoretical constructs underlying family nursing in diverse settings and populations. The heterogeneity of study designs and intervention/practice components together with the diversity of settings and populations require caution when using the findings of our scoping review. In line with a scoping review methodology (Peters, Godrey, Khalil et al., 2015), no quality appraisal was undertaken. It may be possible that we were unable to identify all eligible studies, despite the use of a systematic and iterative search strategy in two major databases. For instance, we noticed that most included studies were performed in the acute clinical care setting and not within other areas such as community care or mental health care. Despite these limitations, which need to be taken into consideration when transferring findings, this scoping review provides a knowledge map to family nursing implementation on which to build on.
Recommendations for Research and Practice
More implementation research with rigorous designs and guided by specific implementation science theory and evidence is needed to verify our tentative findings and to build further knowledge on how to effectively implement evidence-informed family nursing practices. Better reporting of the evidence- and/or theory-base of the implemented practice is also called for. Knowledge synthesis research about specific family nursing interventions or family engagement practices in distinct settings or populations is necessary. Research insights into the effect of implementation efforts, particularly in terms of implementation outcomes, such as uptake, reach, cost, appropriateness, or sustainability (Proctor et al., 2009) and also on quality of family care and family health outcomes is clearly needed.
The results of this review propose a roadmap for future family nursing implementation projects. Family nursing implementation projects should use the body of knowledge evolving in the field of implementation and family science in three ways. First, use implementation theory to inform and specify the implementation endeavor and its evaluation. Second, tailor implementation strategies to contextual determinants, either by drawing on preexisting knowledge or by analyzing the specific practice environment. Third, use strategies that include capacity-building, facilitation, and participatory approaches and target the “inner context” (team, organizational) factors and not only individual nurse competence and skills.
Conclusion
This scoping review provides an overview of the current state of knowledge around family nursing implementation science. It demonstrates that family nursing practice uptake is fluctuating and partial, hampered by organizational constraints, which are often not specifically targeted through implementation strategies. Family nursing implementation strategies therefore need to target organizational barriers. Capacity-building strategies coupled with dissemination-educational strategies may be most promising to enable nurse skills, ensure consistent family care delivery, and create supportive systems. To further build the family nursing implementation science body of knowledge, systematic reviews focusing on specific aspects of implementation, such as culture, leadership, and resources as key organizational determinants, or the effect of implementation strategies on family health outcomes, are necessary. More research on implementation and knowledge translation efforts in family nursing are also needed to better understand the mechanisms through which sustainable, evidence-informed family nursing practices that translate into improved service and family health outcomes can be achieved and maintained.
Supplemental Material
sj-docx-1-jfn-10.1177_10748407221099655 – Supplemental material for The Implementation of Evidence-Informed Family Nursing Practices: A Scoping Review of Strategies, Contextual Determinants, and Outcomes
Supplemental material, sj-docx-1-jfn-10.1177_10748407221099655 for The Implementation of Evidence-Informed Family Nursing Practices: A Scoping Review of Strategies, Contextual Determinants, and Outcomes by Eva Thürlimann, Lotte Verweij and Rahel Naef in Journal of Family Nursing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.