
Abstract
This article reports the results of a scoping review of research applications of the Family Management Style Framework (FMSF) and the Family Management Measure (FaMM). We identified 32 studies based on the FMSF and 41 studies in which the FaMM was used, 17 of which were based on the FMSF. Both the framework and measure have been used by investigators in multiple countries, with most applications of the FaMM outside the United States. Although the FMSF and FaMM were originally developed for use with families in which there was a child with a chronic physical condition, both have been applied to a broader range of health conditions and to studies focusing on families with an adult member facing a health challenge. Based on our findings, we make recommendations for how researchers can more fully address all aspects of the FMSF.
Published three decades ago (Knafl & Deatrick, 1990), the Family Management Style Framework (FMSF) conceptualized how families with a child with a chronic condition incorporated condition management into daily family life. The FMSF described key elements of family management related to how family members defined their situation, their management behaviors, and the consequences of condition management for family life. Recognizing that these elements might differ across family members, we also pointed to the need to explicate further the elements of family management and identify overarching family management patterns. Research aimed at further developing the framework and identifying patterns of family management was first published in 1996 by Knafl and colleagues.
Building on research on family response to childhood conditions, we continued to refine the framework, publishing two updated versions (Knafl & Deatrick, 2003; Knafl et al., 2012). Based on research evidence, the updated versions of the FMSF added family and family member functioning as outcomes of family management. The most recent version of the framework is displayed in Figure 1, which also highlights the changes made as the framework was developed. These initial conceptualizations of family management were grounded in studies of predominantly North American families in which a child had a chronic physical condition. In 2010 Janice Bell, the editor of the Journal of Family Nursing (JFN), invited the submission of manuscripts for a special issue addressing “New Directions for the Family Management Style Framework” that extended the framework to conditions and/or sociocultural contexts not included in the initial conceptualization. Published in May 2012, the special issue reported studies focusing on family management of serious and life-threatening conditions in both children (Bousso et al., 2012; Rempel et al., 2012) and adults (Beeber & Zimmerman, 2012; Wiegand, 2012), studies completed outside North America (Bousso et al., 2012), and a study of adolescents’ perspectives of family management of chronic conditions (Wollenhaupt et al., 2012).
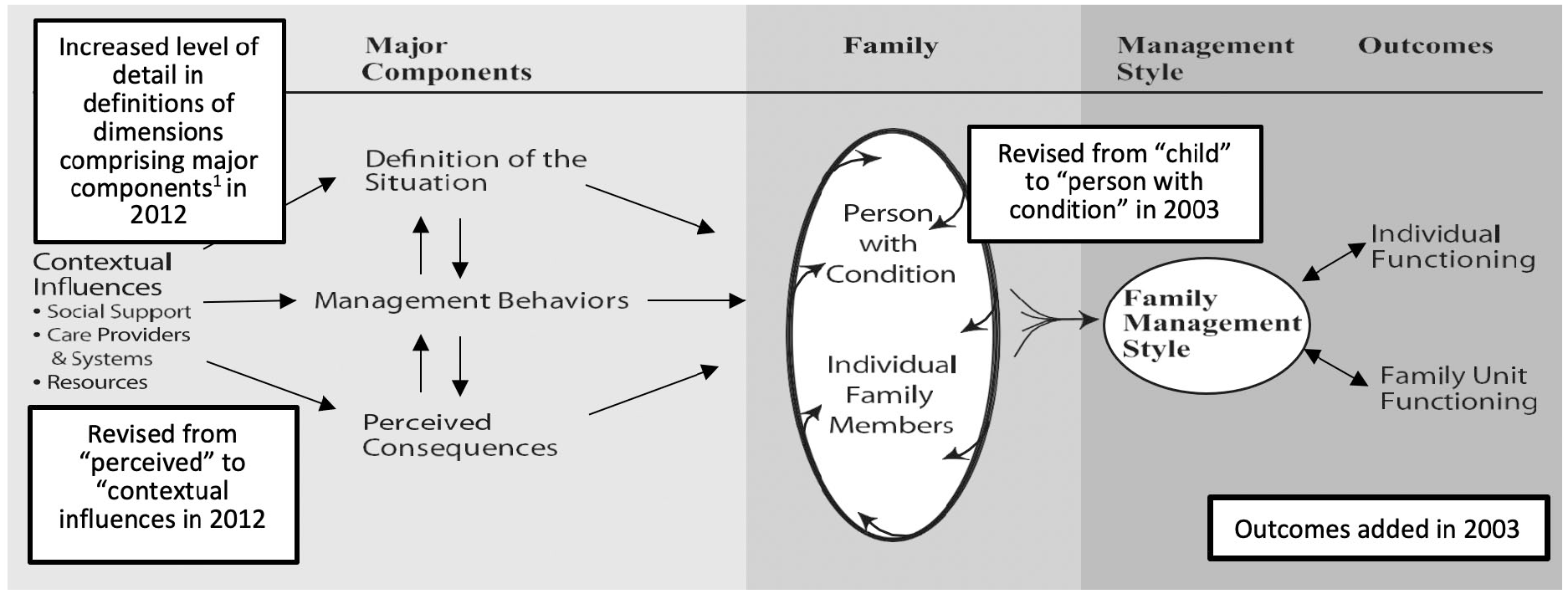
Family Management Style Framework.
In the absence of a measure of family management, early studies applying the FMSF were largely qualitative. We recognized that to examine the association between family management and family and family member functioning, a measure of family management was needed. Funding from the National Institute of Nursing Research supported the work to develop a family management measure. A questionnaire was created with items based on the FMSF; the measure’s psychometric properties were assessed from a study of more than 500 parents with children with varied non-life-threatening chronic physical conditions. Publication of the Family Management Measure (FaMM) included its methodological development and provided evidence of its reliability and validity (Knafl et al., 2011). The measure comprised six separately scored scales (Child Daily Life, Condition Management Ability, Condition Management Effort, Family Life Difficulty, Parental Mutuality, and View of Family Impact) with a total of 53 Likert-type items. Researchers have the option of using all or a subset of the scales. There is no summary score because each scale measures a different aspect of family management. The instructions to the FaMM define family as “those living in your household that you think of as family.” The publication of the FaMM set the stage for subsequent quantitative studies, including investigations directed to examining the relationship between family management and child and family outcomes, as well as identification of patterns of family management.
Although we were aware of ongoing applications of the FMSF and FaMM, we had not systematically tracked the extent of their use. We recognized that such tracking would be useful in evaluating the applicability of both, thereby informing study design and decision-making of future investigators. Our intent in this review was to determine how the FMSF and FaMM have been used in research by examining the aims, sample, and design of published research reports.
We conducted a scoping review of published studies to assess the extent and ways in which the FMSF and FaMM had been used. Following guidelines recommended by Arksey and O’Malley (2005), we identified and screened research reports for inclusion in the sample, extracted the information from the reports needed to address the purpose of the review, and collated and summarized the results. With support from a research librarian based at the first author’s university, we identified articles citing one or more versions of the FMSF and/or the FaMM published through June 30, 2019. Articles were identified through citation searches of the Scopus, Web of Science, and Google Scholar databases. Following identification of all articles citing the FMSF and/or the FaMM, the first author reviewed articles to differentiate research from nonresearch applications of the FMSF and FaMM. Research applications were defined as those in which the FMSF provided the conceptual underpinnings of a research study or secondary analysis or the FaMM was used in the study. In some articles, the framework or measure was cited in a background or discussion section but was not applied in the research being reported. Other nonresearch applications included citations in a review article or publications focusing on theory or methods. Other than tallying the number of such citations, these reports were excluded from further analysis. The co-authors reviewed the research versus nonresearch categorization, with any disagreements resolved through discussion to reach consensus.
The following information was extracted from each study: country where data were collected, study aims, sample (number of families; family members participating), condition(s) included in the sample, and design. For studies based on the FMSF, which aspects of the FMSF (contextual influences, components/dimensions, management style, outcomes) were addressed in the research were noted. For studies using the FaMM, we also noted the conceptual underpinnings and summarized how the measure was used in the study (e.g., independent versus dependent variable) and any data provided on the reliability of the six FaMM scales. Four summaries were completed, one for each of the three versions of the FMSF and one for the FaMM.
The first three authors divided the work of extracting the data from the research reports. As a quality check, the fourth author independently extracted the same information from every fifth article. These checks revealed we were thorough and accurate in the data extractions and only minor corrections were made to the initial extractions.
The analysis was straightforward and included simple listings and counts (e.g., countries where data were collected, conditions studied) and categorization of certain aspects of the study (e.g., aims, design, use of FaMM). The first author did the initial categorizations, which were then reviewed by the co-authors. Any disagreements were resolved through discussion to reach consensus. If more than one version of FMSF was cited in the research report, only the most recent version was counted in the tally.
Results
Final Sample
In Table 1, the breakdown of the 262 published articles citing one or more versions of the FMSF or citing the FaMM is summarized. The FMSF was named as the conceptual grounding in 32 studies and the FaMM was used in 41 studies, 17 of which were based on the FMSF. Each study was counted in one tally only to avoid artificially inflating the number of studies based on the FMSF. Studies using the FaMM and citing the FMSF were tallied under the FaMM. Both the FMSF and the FaMM also were cited in nonresearch articles and research reports where they were not applied but were referenced in the background or discussion sections of the article. These were categorized as “Other Citations.” Eight reports citing the FaMM addressed efforts to assess or adapt it for use with non-English samples. In contrast to the tally for “Published Research Based on FMSF or FaMM,” when reports in the “Other” category included citations to multiple versions of the FMSF, each of these citations was tallied. The rationale for this was that authors were using the citations to support their work, and thought it necessary, in some cases, to cite multiple versions.
Number of Reports Citing the FMSF or the FaMM.
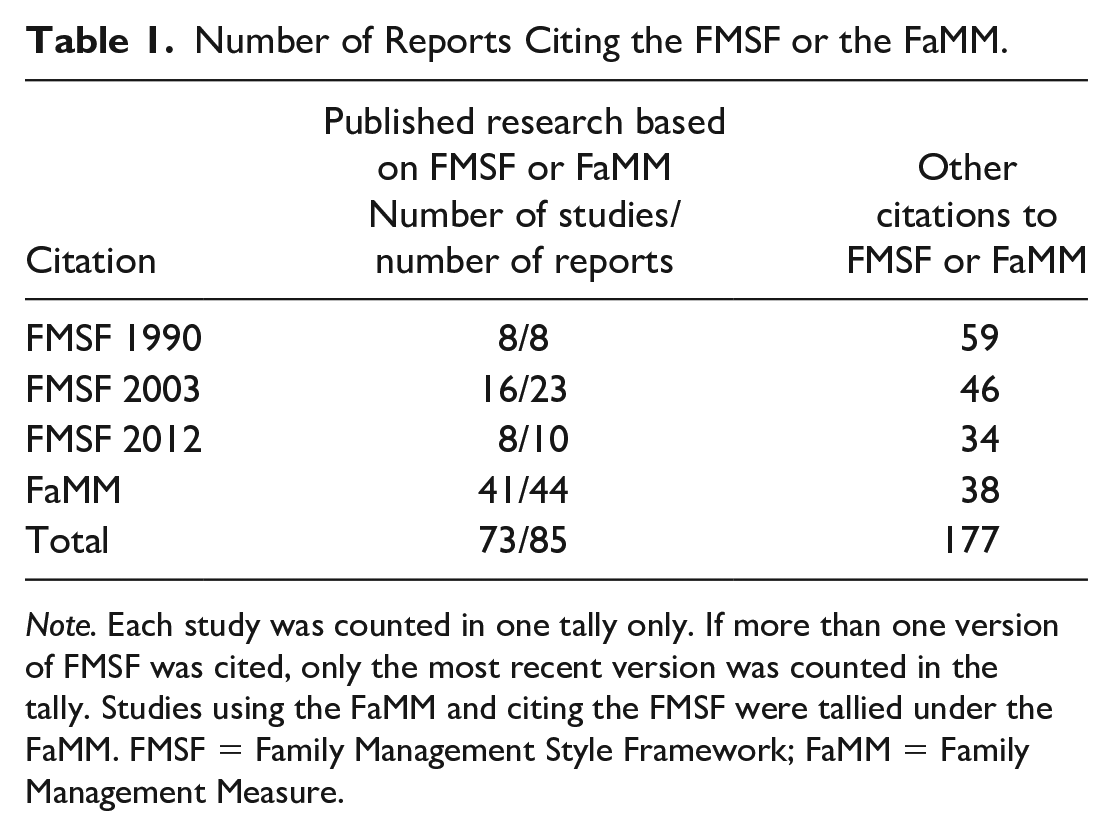
Note. Each study was counted in one tally only. If more than one version of FMSF was cited, only the most recent version was counted in the tally. Studies using the FaMM and citing the FMSF were tallied under the FaMM. FMSF = Family Management Style Framework; FaMM = Family Management Measure.
FMSF
As summarized in Table 2, study participants for most (n = 26/81%) of the 32 studies based on the FMSF were recruited in the United States, although investigators from Brazil, Thailand, and Canada also published study results. The research aims of the studies citing the FMSF were most often descriptive or exploratory such as an early study by Williams (1995) describing the problems and management behaviors used by mothers of daughters with precocious puberty or Turner syndrome. More recently, Estrem and colleagues (2017) applied the FMSF to a study of family management of children’s feeding problems and SanGiacomo and colleagues (2019) described the management challenges reported by mothers of childhood brain tumor survivors. In four studies (Conlon et al., 2008; Knafl et al., 1996; McCarthy & Gallo, 1992; Obrecht et al., 1992), investigators described changes in family management over time. One investigator (Johnson et al., 2014) used the framework to support development of a social script iPad application for children with autism.
Overview of Studies Conceptually Grounded in FMSF.
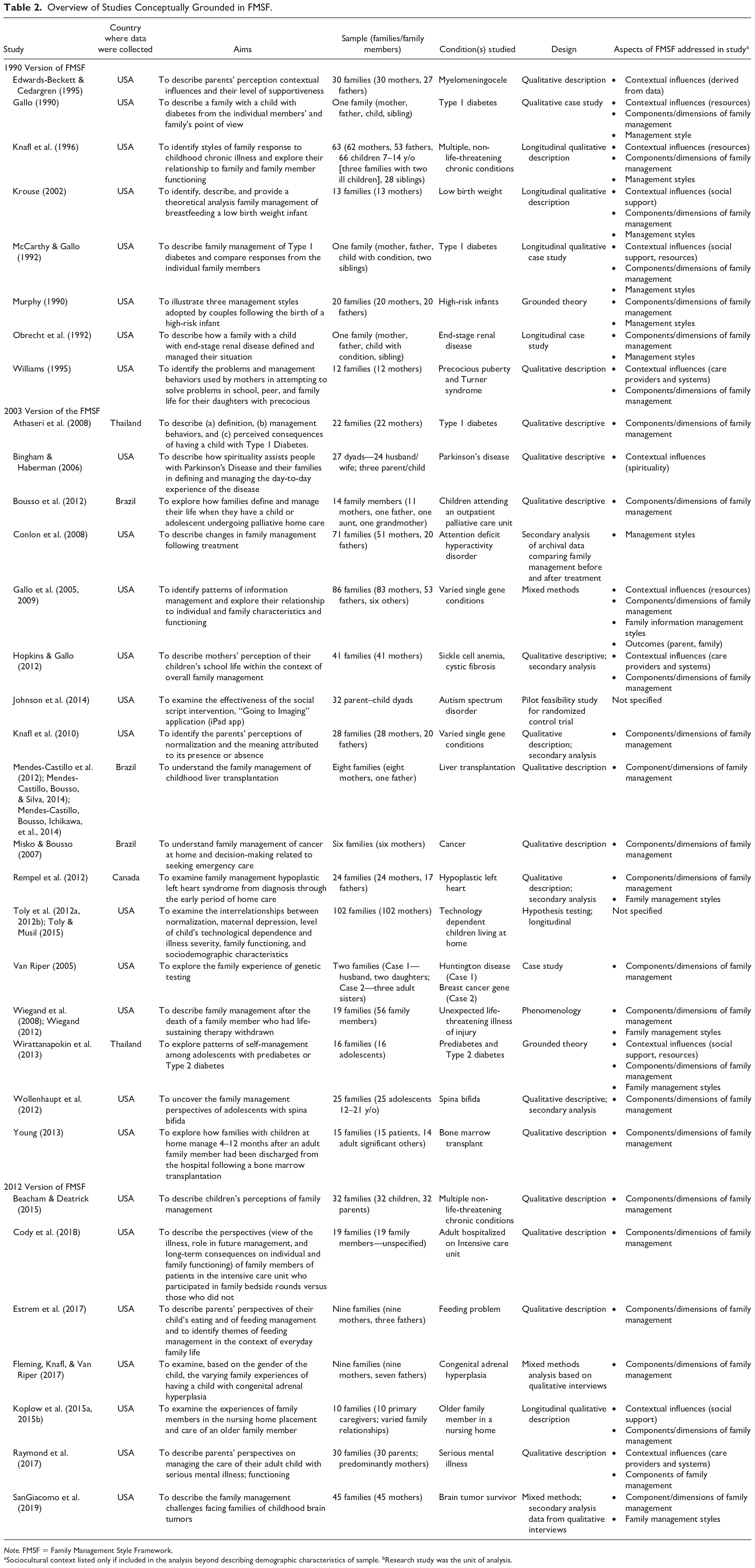
Note. FMSF = Family Management Style Framework.
Sociocultural context listed only if included in the analysis beyond describing demographic characteristics of sample. bResearch study was the unit of analysis.
Beginning with the 1990 version of the FMSF, investigators were extending the framework to the study of health challenges not included in its original development. For example, Krouse (2002) applied it in a study of family management of feeding low birthweight infants; Van Riper (2005) explored the family experience of genetic testing; and Raymond and colleagues (2017) described parents’ perspectives on managing the care of their adult child with serious mental illness.
Consistent with their descriptive or exploratory intent, most investigators described their study design as qualitative, with six being longitudinal. In most studies (n = 25/78%), investigators addressed a single condition (e.g., Type 2 diabetes, end-stage renal disease) or group of related conditions (e.g., cancer, serious mental illness). In eight studies, researchers focused on a health-related challenge not linked to a specific condition (e.g., technology dependence, feeding problem). The number of families included in the samples ranged from case studies of one or two families to (Gallo, 1990; McCarthy & Gallo, 1992; Obrecht et al., 1992; Van Riper, 2005) to Toly and colleagues’ (Toly et al., 2012a, 2012b; Toly & Musil, 2015) study of more than 100 families of children with technology dependence. About one half (51%) of studies enrolled 20 families or less and only four studies enrolled participants from 50 or more families.
Family members included in the sample varied across studies. In nine studies, sample inclusion criteria required participation by multiple family members, with five focusing on dyads within the family. For example, both Beacham and Deatrick (2015) and Johnson and colleagues (2014) recruited child–parent dyads; Murphy (1990) included mother–father dyads; and Young (2013) recruited adult patients who had received a transplant and an adult family member. Investigators reporting family case studies included data from an even broader range of family members. McCarthy and Gallo (1992) purposely selected a family for their case study of family management that included interview data from the mother, father, child with the chronic condition, and one sibling. Investigators in nine studies offered family members the option of participation by multiple family members, but this was not a requirement for inclusion in the sample. In other studies, a family member fulfilling a specified family role (e.g., primary caregiver) was recruited and the family designated who would represent them in the sample. When families were given the option of participation by multiple family members or asked to designate a family participant, the final sample predominantly comprised mothers. In seven studies, inclusion criteria specified mothers.
We also examined the extent to which investigators studied all or selected aspects of the framework. Across the 32 studies based on the FMSF, Gallo and colleagues’ (2005, 2009) study of family information management was the only one that addressed all four aspects of the framework (Contextual Influences, Major Components, Management Styles, and Outcomes). More often researchers studied selected aspects of the framework. Investigators addressed a single aspect of the FMSF in 14 studies and two or three aspects in 15 studies. Of the 14 studies focusing on a single aspect of the framework, most (n = 11) focused on describing how the six dimensions of family management were reflected in their sample. For example, Estrem and colleagues (2017) used the dimensions of the framework to describe parents’ efforts to manage a child’s feeding problems and Misko and Bousso (2007) used them to describe family management of a child’s cancer at home. In 12 of the 32 studies, investigators went beyond describing how the FMSF dimensions were reflected in their sample to identify styles of family management based on the FMSF dimensions, with the styles varying across samples. For example, Rempel and colleagues (2012) described changing patterns of family management in parents of children who were surgically treated for a life-threatening cardiac condition. Investigators in nine studies examined parents’ perceptions of the link between the contextual influences included in the framework and family management.
FaMM
In Table 3, the characteristics of studies using the FaMM are summarized, and in Tables 4 and 5, reports of the internal consistency reliability (ICR) for FaMM scales are presented. Researchers from 11 countries have reported using the FaMM. In contrast to the FMSF where U.S.-based samples predominated, the majority (n = 25/61%) of studies using the FaMM were conducted outside the United States.
Overview of Studies Using the FaMM.
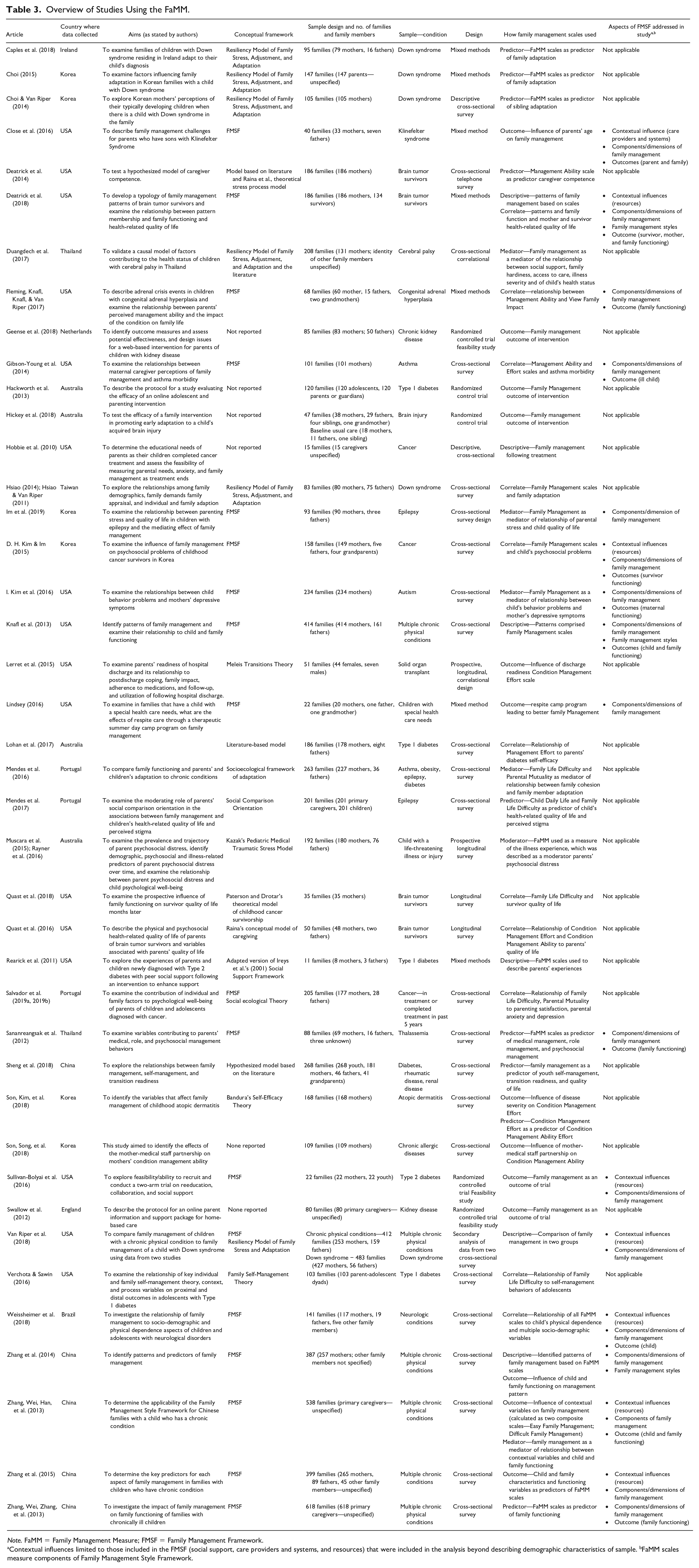
Note. FaMM = Family Management Measure; FMSF = Family Management Framework.
Contextual influences limited to those included in the FMSF (social support, care providers and systems, and resources) that were included in the analysis beyond describing demographic characteristics of sample. bFaMM scales measure components of Family Management Style Framework.
Internal Consistency Reliability of Family Management Measure in Studies Reporting a Range of Scores Across Scales.
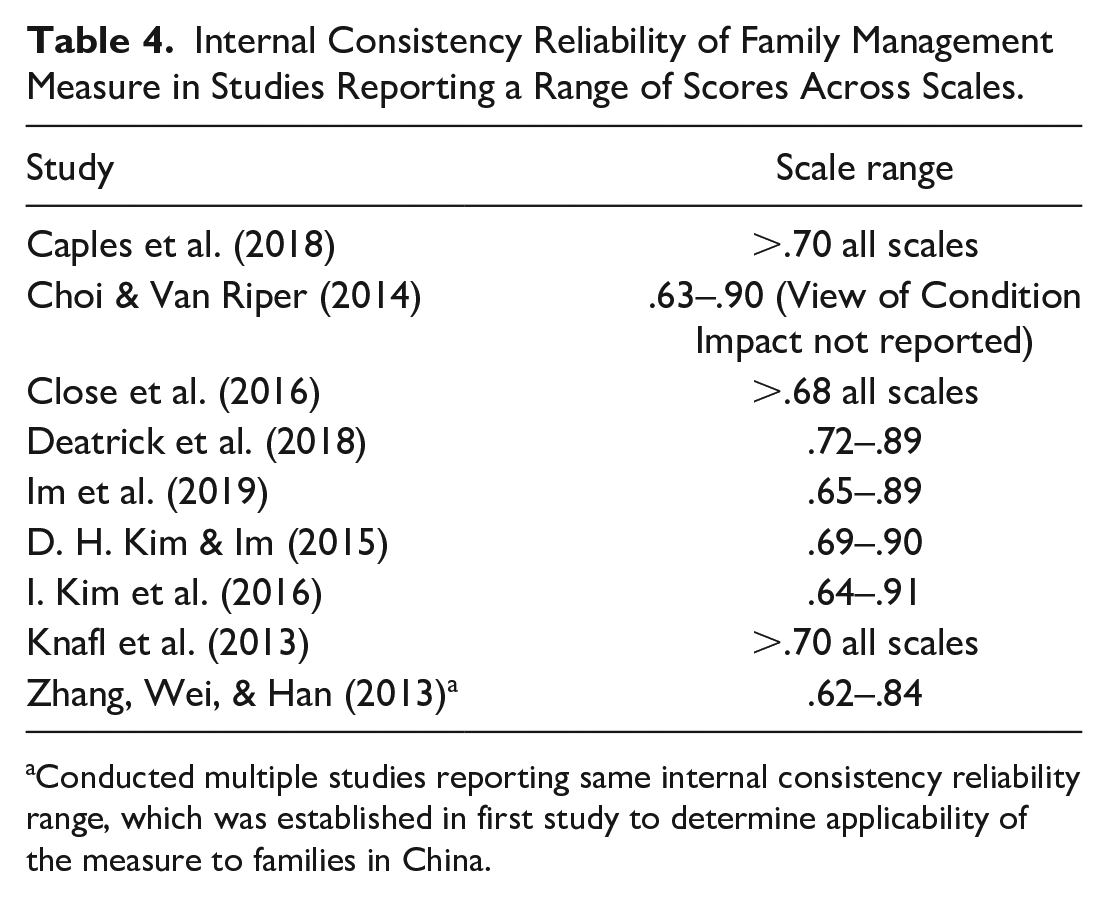
Conducted multiple studies reporting same internal consistency reliability range, which was established in first study to determine applicability of the measure to families in China.
Internal Consistency Reliability of Individual Family Management Scales.
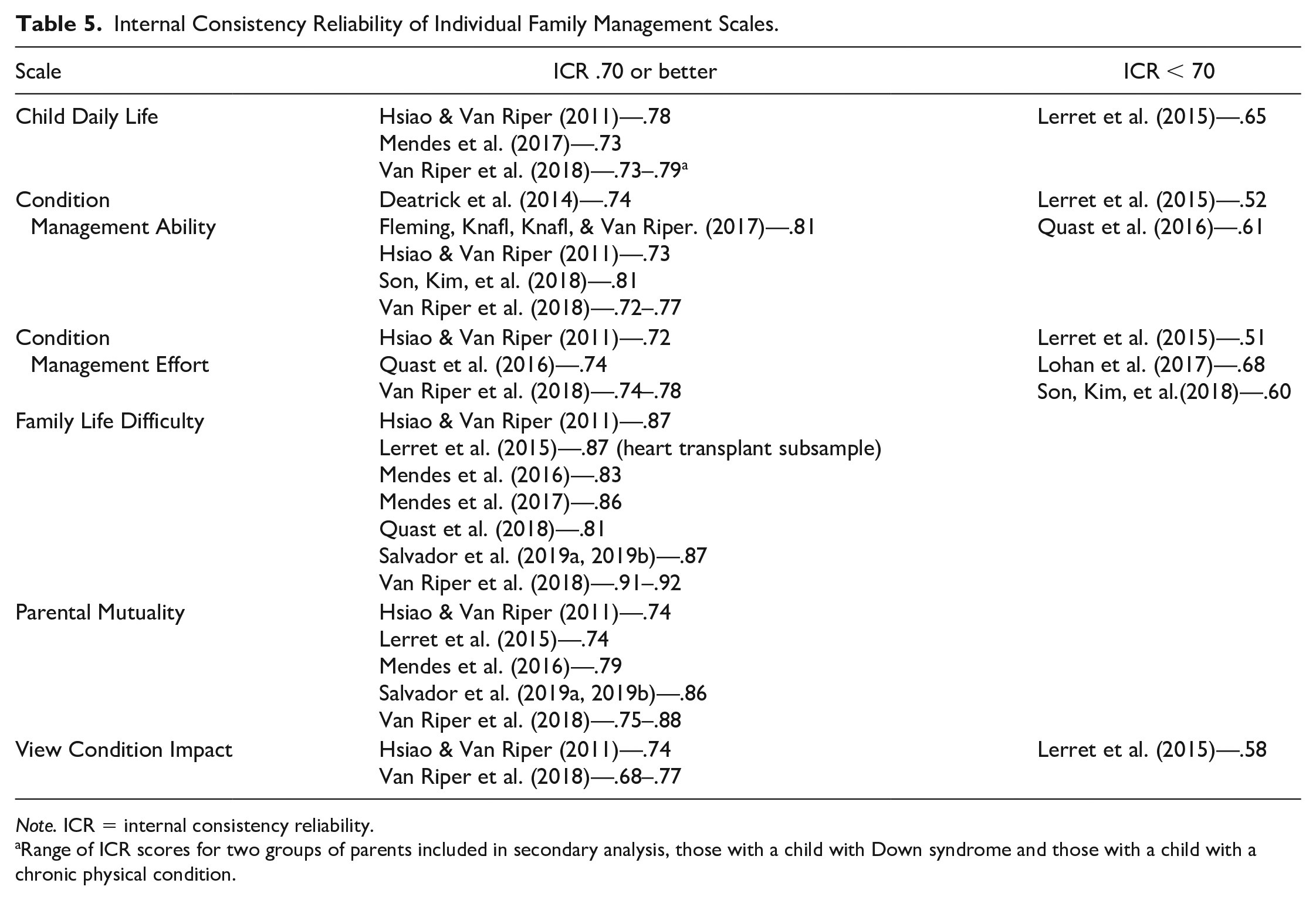
Note. ICR = internal consistency reliability.
Range of ICR scores for two groups of parents included in secondary analysis, those with a child with Down syndrome and those with a child with a chronic physical condition.
Seventeen of the 41 studies using the FaMM were based on the FMSF, eight of which were conducted outside the United States. Eighteen studies were based on other frameworks, providing evidence that the FaMM is suitable for use in studies with diverse theoretical underpinnings. Authors of six studies did not report using a framework. Five studies of families of children with Down syndrome undertaken in Ireland (Caples et al., 2018), Korea (Choi, 2015; Choi & Van Riper, 2014), Taiwan (Hsiao, 2014; Hsiao & Van Riper, 2011), and the United States (Van Riper et al., 2018) were based on the Resiliency Model of Family Stress, Adjustment, and Adaptation (McCubbin & McCubbin, 1993). Other examples of using the FaMM in studies not based in the FMSF include Muscara and colleagues’ (2015; Rayner et al., 2016) use of Kazak’s Pediatric Medical Traumatic Stress Model (Kazak et al., 2006) in their study of parents of children with a life-threatening condition and Son, Kim, and colleagues' (2018) use of Bandera’s Self-Efficacy Theory (Bandura, 1997) to examine factors influencing family management in the context of having a child with atopic dermatitis. In two studies, investigators reported using two frameworks, one of which was the FMSF (Salvador et al., 2019a, 2019b; Van Riper et al., 2018). In 30 studies, investigators used all FaMM scales. In the remaining 11 studies, investigators used selected scales.
For the 17 studies based on the FMSF and using the FaMM, we also examined what aspects of the framework investigators studied. Because the FaMM scales were grounded in the FMSF dimensions, all studies addressed this aspect of the framework. Except for Lindsey’s (2016) study of family management following parents’ participation in a respite program and Im and colleagues’ (2019) study of the mediating effect of family management on the relationship between parental stress and child quality of life, all other studies addressed multiple aspects of the framework. Researchers in 11 studies measured outcomes of family management for the person with the condition, parents, and/or the family system and investigators in eight studies examined contextual influences on family management, with most addressing resources.
Across studies, investigators incorporated the FaMM in varying ways. Using correlation or regression analyses, 28 studies focused on examining the relationship between family management as measured by one of more FaMM scales and other family or family member variables. For example, Gibson-Young and colleagues (2014) examined the relationship between maternal perceptions of Condition Management Ability and Condition Management Effort and asthma morbidity in 101 children in the United States. Lohan and colleagues (2017) studied the relationship between parents’ Condition Management Effort and their perceptions of their diabetes self-efficacy. In other studies, investigators examined variables such as parental age (Close et al., 2016) or family functioning (Zhang et al., 2015) as predictors of family management. In seven studies, investigators examined the mediating or moderating effect of FaMM scales. For example, in a study of Korean families in which a child had epilepsy, Im and colleagues (2019) examined the mediating effect of family management on the relationship between parenting stress and the child’s quality of life. The FaMM scales also were used to compare family management of different types of conditions as in Van Riper and colleagues’ (2018) comparison of families of children with Down syndrome to those of children with a chronic physical condition. In three studies (Deatrick et al., 2018; Knafl et al., 2013; Zhang et al., 2014), investigators used cluster analysis of the six FaMM scales to identify patterns of family management.
Across studies, samples varied as to condition, size, and family member participants. The 18 different conditions studied included chronic physical conditions such as Type 1 diabetes and asthma, cancer and other life-threatening conditions, genetically based conditions, and conditions associated with intellectual or developmental disabilities. Most investigators studied a single condition or related conditions (e.g., cancer, neurologic disease), with only seven studies recruiting sample families in which children were diagnosed with different conditions. The number of families included in these samples ranged from 11 to 895, with more than half (n = 25; 61%) including more than 100 families. In 29 studies (71%), only one family member participated in the study, with 13 studies explicitly recruiting mothers, six specifying parent or primary caregiver, and the remaining recruiting family members in varied roles. In the latter case, mothers always made up most of the sample. Investigators in four studies recruited parent–child dyads (Hackworth et al., 2013; Sheng et al., 2018; Sullivan-Bolyai et al., 2016; Verchota & Sawin, 2016). In eight studies, participation by multiple family members was optional.
Investigators varied in the extent to which they reported the ICR of the FaMM scales in their study, with 15 reporting no results or citing the ICR data from the instrument development study (Knafl et al., 2011). In nine studies investigators reported a range of scores across scales (Table 4), with the ICR reaching .70, often considered the cut-off for acceptable reliability (DeVellis, 2003) in three studies and .62 or higher for all scales in the remaining studies. Investigators for 10 studies reported the ICR for each scale used in the study. Regarding individual FaMM scales, Table 5 provides evidence of the reliability of FaMM scales across multiple conditions and sociocultural contexts. The strongest evidence for ICR was for the Family Life Difficulty scale. In seven studies, investigators from different countries (Korea, Portugal, United States) studying different conditions (brain tumor survivorship, cancer, Down syndrome, epilepsy, solid organ transplant, multiple conditions) reported ICR scores ranging from .81 to .92 and no investigator reported an ICR value less than .70. Support for the ICR of Parental Mutuality also was strong with investigators from five studies based on samples representing different countries (Korea, Portugal, United States) and conditions (cancer, Down syndrome, solid organ transplant, multiple conditions) reporting ICR scores greater than .70. For the remaining four scales (Child Daily Life, Condition Management Ability, Condition Management Effort, View of Condition Impact), there were reports of ICR scores both exceeding and falling below .70, though those exceeding predominated and reflected samples representing different countries and conditions. The weakest evidence for support of ICR was for the View of Condition Impact scale. Investigators in two studies (Duangdech et al., 2017; Sananreangsak et al., 2012) incorrectly scored the FaMM by calculating a total single score rather than individual scales scores.
Discussion
Through this scoping review, we traced the use of FMSF and FaMM and described the frequency and range of research applications across conditions, age groups, and countries. Our review provides evidence of the broad applicability of both the framework and measure and highlights areas of concentrated activity and areas of limited application. The review also provides evidence to guide future research.
Although the framework and measure were developed based on studies of families in the United States with children with non-life-threatening chronic physical conditions not associated with developmental delays, the review provides strong evidence of broader applicability, especially about the types of conditions studied and cultural context. The FMSF and the FaMM have been used in studies of families in which children have a condition that is life-threatening or includes intellectual disability or developmental delay. Both also have been used in studies of survivorship and the aftermath of serious injury, and the FMSF has been used in studies addressing family response to a health challenge facing an adult family member. The FaMM items reference “our child with the condition,” limiting the applicability of the measure for studies in which an adult is the family member facing a health challenge. Although most researchers using the FaMM focused on family management of childhood chronic conditions, we identified several that used the FaMM to study family life in the context of an adult family member who was living with their parents due to cognitive or physical deficits (see, for example, Deatrick et al., 2018; Van Riper et al., 2018).
The review also provides evidence of the cross-cultural applicability of the FMSF and FaMM with the first study based on a sample from outside the United States conducted in Thailand (Athaseri et al., 2008). Cross-cultural applications increased substantially after the publication of the FaMM and reports of its ICR support its applicability in multiple cultural contexts. Not all authors reported the ICR data for their sample. Doing so would help future investigators make informed decisions about the appropriateness of the measure for their intended sample. In addition to the ICR data summarized in Table 4, Van Riper and colleagues’ (2020) analysis of the use of the FaMM with samples of parents of individuals with Down syndrome from 11 countries spanning North and South America, Europe, and Asia provides additional support for the measure’s broad applicability.
The items comprising the FaMM were grounded in the FMSF, and the scales were identified using well-established techniques for instrument development (DeVellis, 2003; Knafl et al., 2011). The scales measure different aspects of family management, with each scale addressing a different underlying latent construct. Despite the FaMM being described as comprising six separate scales with no total score and scoring instructions available on the FaMM website (https://nursing.unc.edu/research/office-of-research-support-and-consultation/family-management-measure/), we found instances of investigators calculating a total score that was then used in their analyses. Such analyses are questionable, and we encourage anyone using the FaMM to adhere to scoring instructions.
Across conditions and cultural contexts, most investigators have focused on examining the FMSF components (Definition of the Situation, Management Behaviors, Perceived Consequences) and their underlying dimensions or the FaMM scales, with less attention directed to identifying patterns of family management, contextual influences, and outcomes. This focus is understandable given the design complexity and resources needed to incorporate multiple aspects of the framework into a single study. However, from the outset the developers maintained that a strength of the framework was the emphasis on identifying patterns of family management based on the configuration of the dimensions of family management across family members. Beginning with the first publication (Knafl & Deatrick, 1990), the framework included influences on family management, and in the first revision (Knafl & Deatrick, 2003), family member and family system outcomes of family management were added.
Although recognizing it may not be feasible to include multiple aspects of the framework in a single study, we encourage investigators focusing on selected aspects of the framework to consider addressing those that have been less studied. For example, contextual influences such as health insurance, access to specialty care, and family income could be included in the demographic and family information respondents often are asked to provide and examined in the analysis as contextual influences on family management. Another possibility would be to add measures addressing social support or health care relationships to examine how these influence family management. The FMSF was based on syntheses of predominantly qualitative research addressing family response to childhood chronic conditions. The contextual influences included in the framework were based on study results reporting what family members identified as factors contributing to the ease or difficulty of family management. Although the contextual influences included in the FMSF reflect issues recognized as social determinants of health that are widely acknowledged as important to understanding structural impediments to families in managing health conditions, there are other factors that are recognized and could be included. Further attention to the social determinants of health also calls for recognition and study of issues such as racism that are now widely acknowledged as important to explaining health disparities (Deatrick, 2017). Although recommending that researchers consider extending their study aims beyond the current focus on the components and dimensions of family management, the body of research addressing these provides an opportunity for undertaking research syntheses of results reporting how the dimensions of family management are reflected across conditions and cultures.
Qualitative data related to the dimensions of family management and scores on the FaMM scales are the building blocks for identifying family management styles, and when investigators have these data, they can take the next step and extend their analysis to identifying different styles. By using analytic approaches such as matrix display of qualitative data reflecting family management dimensions across families and quantitative cluster analyses based on the FaMM scales, investigators can identify styles of family management that can be compared with those previously identified (Deatrick et al., 2018). Although full delineation of management styles, requires a large enough sample to identify subgroups within the sample with similar patterns of family management, even with relatively small samples, investigators can undertake exploratory analyses to detect provisional management styles. By identifying management styles and examining their relationship to family and family member outcomes, investigators will have a better understanding of the management approaches that put families and family members at risk for poor outcomes. Understanding the implications of different management styles also will contribute to the development of tailored interventions aimed at buttressing family management strengths and mitigating problematic aspects.
Sample design presents another opportunity for taking full advantage of the FMSF by including multiple family members in the sample. Beginning with our initial conceptualization (Knafl & Deatrick, 1990), we have emphasized the value of including the perspectives of multiple family members in studies addressing family management. Nonetheless, most investigators applying the framework or using the measure have limited their sample to one family member, most often the mother. The inclusion of multiple family members in the sample provides researchers with the opportunity to undertake conceptually grounded, dyadic, or family system analyses examining the implications of family members having shared versus discrepant or conflicting views of family management (Deatrick et al., 2020).
The focus of both the FMSF and FaMM is family management within a single household and that focus is reflected in the research applications to date. The contribution to condition management of individuals outside the household is incorporated under the Social Network Contextual Influence. Yet to be addressed are those situations where members from multiple households are actively involved in condition management as might be the case when divorced parents have shared custody of a child or when extended family members assume major caregiving responsibilities. Additional studies are needed to examine the unique challenges of multi-household family management and factors supporting and hindering effective, well-coordinated management across households.
Like all scoping reviews, there were limitations to this one. We included only those studies published in English language journals. It is possible that our search missed relevant publications, but we believe we minimized that possibility by working closely with a research librarian to identify relevant citations. The review was limited to research applications because our initial screen of the reports revealed few clinical applications to date. Research reports often make recommendations related to practice applications and these provide a beginning point for clinicians to consider how the FMSF could guide practice or how the FaMM could be incorporated into clinical assessments.
Conclusion
When we began developing the FMSF in the late 1980s, our objective was to provide researchers with a framework that would guide efforts to advance knowledge of family response to childhood chronic conditions. Building on existing research, we aimed to devise a framework that was applicable to multiple conditions and family structures. We believe this review of research studies supports the conclusion that we achieved that goal. Over the years, others have applied the framework to a much broader spectrum of conditions, populations, and cultural contexts than we originally anticipated. We are grateful for their creative and innovative applications, which have contributed in important ways to extending the scope of the FMSF.
In urging investigators to incorporate multiple aspects of the FMSF into their studies and focus on the less developed aspects of sociocultural context, management styles, and outcomes, we recognize this often requires design trade-offs, especially regarding sampling. Trade-offs typically entail balancing the ideal family research design with the reality of limited resources. For example, a decision to study dyads leads to a decision to study fewer families or a statistical technique requiring a large sample size leads to a decision to recruit only one family member. Considering all aspects of the FMSF when planning a study can help investigators evaluate various options related to their study aims and design and contribute to making well-reasoned decisions about their priorities for advancing knowledge of family management of health-related challenges.
Footnotes
Acknowledgements
The authors wish to thank University of North Carolina at Chapel Hill librarian Jamie Conklin for her expert input and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
![]() , with M. Van Riper et al.).
, with M. Van Riper et al.).