
Abstract
The provision of care work by families plays an integral role in the quality of life of older adults living in a nursing home setting. This critical interpretive synthesis examines family members’ perceptions of their roles and responsibilities in nursing home settings and interrogates the structural and relational barriers and enablers to family involvement as they relate to fostering an inclusive environment. Electronic databases and published literature were searched for empirical studies that were conducted in a nursing home setting and described involvement from the perspective of family members. Thirty-two articles published between 2006 and 2016 were included in the review. Although involvement comprised a variety of roles and responsibilities, it was grounded in family–resident relationships, influenced by family–staff relationships, and deeply affected by broader sociopolitical factors. We conclude that involvement should be understood as a democratic process with supporting policies and programs to encourage family inclusion in facility life.
Keywords
Immediate and extended family, friends, and neighbors (hereafter referred to as family members) have an integral role in the quality of life of older adults living in nursing homes (NHs). Research has consistently demonstrated that family members continue to provide instrumental, emotional, and personal care support after their relative moves into an NH (Davies & Nolan, 2006; Gaugler, 2005; Ryan & McKenna, 2015), contradicting the myth that family members relinquish their roles as caregivers after this transition. Yet, they often occupy ambiguous positions in these settings: Even though family members adopt roles that contribute to their relative’s overall physical and psychosocial well-being (Cohen et al., 2013; Port, 2006), they experience increased levels of burden and strain (Gaugler, 2005) related to challenges of negotiating their relatives’ care with care staff and NH administration (Baumbusch & Phinney, 2014).
Although research on family involvement has proliferated over the past several decades, it has typically focused on the frequency and duration of visits and the different kinds of roles family members adopt to support their relative. In an earlier synthesis of family involvement in NHs and assisted living facilities, Gaugler (2005) theorized that the preplacement family–relative caregiving situation and the postplacement interrelationships between resident, family, staff, and the NH organization influence family involvement. What this previous review emphasized was the importance of carefully attending to the relational dimensions of family involvement. However, as the family and staff perspectives were combined, this review concealed the family members’ own perspective about their experiences of being involved. In a sociopolitical climate where family care work is often viewed as a commodity (Banerjee & Armstrong, 2015), it is essential to unpack the ways in which family care work is “something more than different caring roles in relation to staff” (Whittaker, 2009, p. 165). This means that the perspective of the family needs to be foregrounded and more fully understood. Moreover, considering that family members are integral to person-centered or relation-centered care, it is imperative to also further interrogate how structural conditions might affect the relational context in which family inclusion in facility life operates.
Theoretical Perspective
This review is conceptually rooted in social inclusion (Bach, 2005; Yanicki, Kushner, & Reutter, 2014). An inclusive environment fosters mutual recognition and respect, and a sense of belonging and acceptance; it gives opportunity for full participation in community life; and it creates the conditions to enable equal citizenship with freedom from oppression. Thus, inclusion brings to the fore the practice of creating democratic engagement within NHs. This means that inclusive spaces “envisions forms of social identity, reciprocity and solidarity that provide a foundation for rights to be realized in relation to others for a life well-lived in community” (Bach, 2005, p. 130). Moreover, this means that family members have access to opportunities and resources that empower them to participate in their relatives’ life including participation in decision making, planning, and policy development in the NH environment (Yanicki et al., 2014). Therefore, thinking in terms of inclusion can prompt alternative ways of understanding involvement. Specifically, it locates involvement and family care work in the collective responsibility and cooperation of family, staff, NH organizations, and political/governing bodies rather than solely as an individual responsibility located in the family system. As such, inclusion of family in NH life operates from shared goals of nurturing inclusive spaces that enrich the lives of all who live, work, and visit the NH setting.
Our understanding of inclusion is, thus, informed by a feminist political economy approach (Armstrong & Braedley, 2013) that brings attention to wider sociopolitical forces (e.g., neoliberalism and market models of care work) and sociocultural factors (e.g., race, gender) that may create tension in how care work is valued and supported at the local NH level and enacted in the relationships between family, care staff, and residents.
Given this theoretical framing of social inclusion informed by a feminist political economy approach, we seek to contribute to the dialogue and debate about family involvement in NH settings; and we extend the literature by giving primacy to the perspectives of family members themselves. The research questions guiding this review were as follows:
Method
Critical interpretive synthesis (CIS) was the method of inquiry for this review. CIS was developed to generate new findings and/or theory from a large number of complex and diverse multidisciplinary sources. Embracing heterogeneity in the literature, CIS posits that variance and difference observed in research findings pose the opportunity to move beyond the aggregation of findings to generate practice-based theory (Dixon-Woods et al., 2006; Tricco et al., 2016). Indeed, the term critical in CIS references the expectation that researchers will interrogate underlying assumptions represented in the research literature for the purpose of developing a more comprehensive understanding of the phenomenon (Dixon-Woods et al., 2006). Although CIS is considered fluid and flexible without “fixed procedures to be accomplished in a pre-defined sequence” (Dixon-Woods et al., 2006, Discussion section para. 6), Kastner, Antony, Soobiah, Straus, and Tricco (2016) argued that this flexibility limits the method. Therefore, researchers are tasked to be transparent about the research process and to detail their methodological approach to enable others to critically engage with their synthesis (Kastner et al., 2016; Tricco et al., 2016).
Selection Criteria
Inclusion criteria for this review were as follows: (a) The setting provided 24-hr nursing services, commonly referred to as an NH or long-term care facility; (b) the population of interest was family members of residents—consistent with the caregiving literature, a family member was defined as any relative, partner, friend, or neighbor; (c) the article described a primary study and not a review or opinion piece; (d) the study was published in an English-language journal; and (e) the publication date was between 2006 and 2016.
As we were interested in how involvement manifested in the everyday functioning of NHs, we excluded intervention studies and studies that focused on the transition into the NH and involvement related specifically to end-of-life care.
Search Strategy
Purposive sampling was initially used to select papers from several databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Ageline, Sociological Abstracts, Medline, Social Work Abstracts, and Academic Search Complete. We identified three broad subject areas as relevant to this review: family (broadly defined), involvement, and NHs. Keywords and database-specific subject headings were selected in relation to these subject areas. Table 1 provides an example of the search strategy that was used.
Sample of Search Terms.
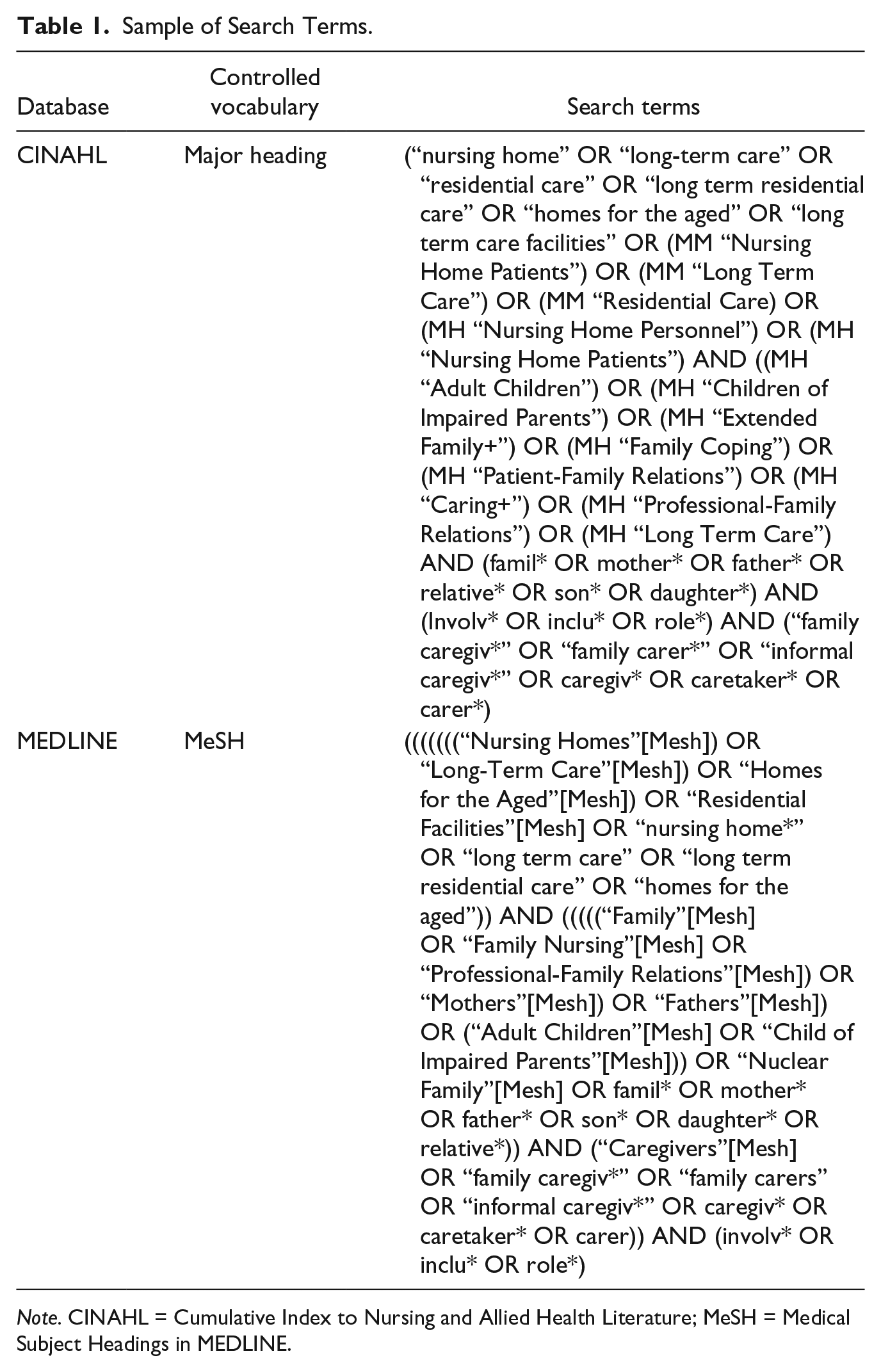
Note. CINAHL = Cumulative Index to Nursing and Allied Health Literature; MeSH = Medical Subject Headings in MEDLINE.
The initial search yielded 1,546 search results (see Figure 1: Study selection flowchart). Two reviewers (J.B. and P.G.) screened titles and abstracts. Relevant articles were imported into EndNote software for duplicate screening and removal, resulting in 216 articles retained. After a second review of abstracts (J.B. and G.P.), 34 articles were retained, and following a review of full texts (G.P.), 16 articles were retained. In both cases, excluded articles did not meet the inclusion criteria (e.g., reporting on involvement in a setting other than an NH) or met the exclusion criteria (e.g., reporting on findings from an intervention). In addition, hand searches of reference lists and expert knowledge yielded an additional nine articles. Decisions about relevance were documented via analytical memos. As the analysis progressed, it was evident that involvement in NH settings has diffuse boundaries with other theoretical areas (e.g., family–staff relationships). Therefore, to extend the investigation, we employed theoretical sampling (Dixon-Woods et al., 2006), which yielded an additional seven studies. The total number of studies included in the review was 32.
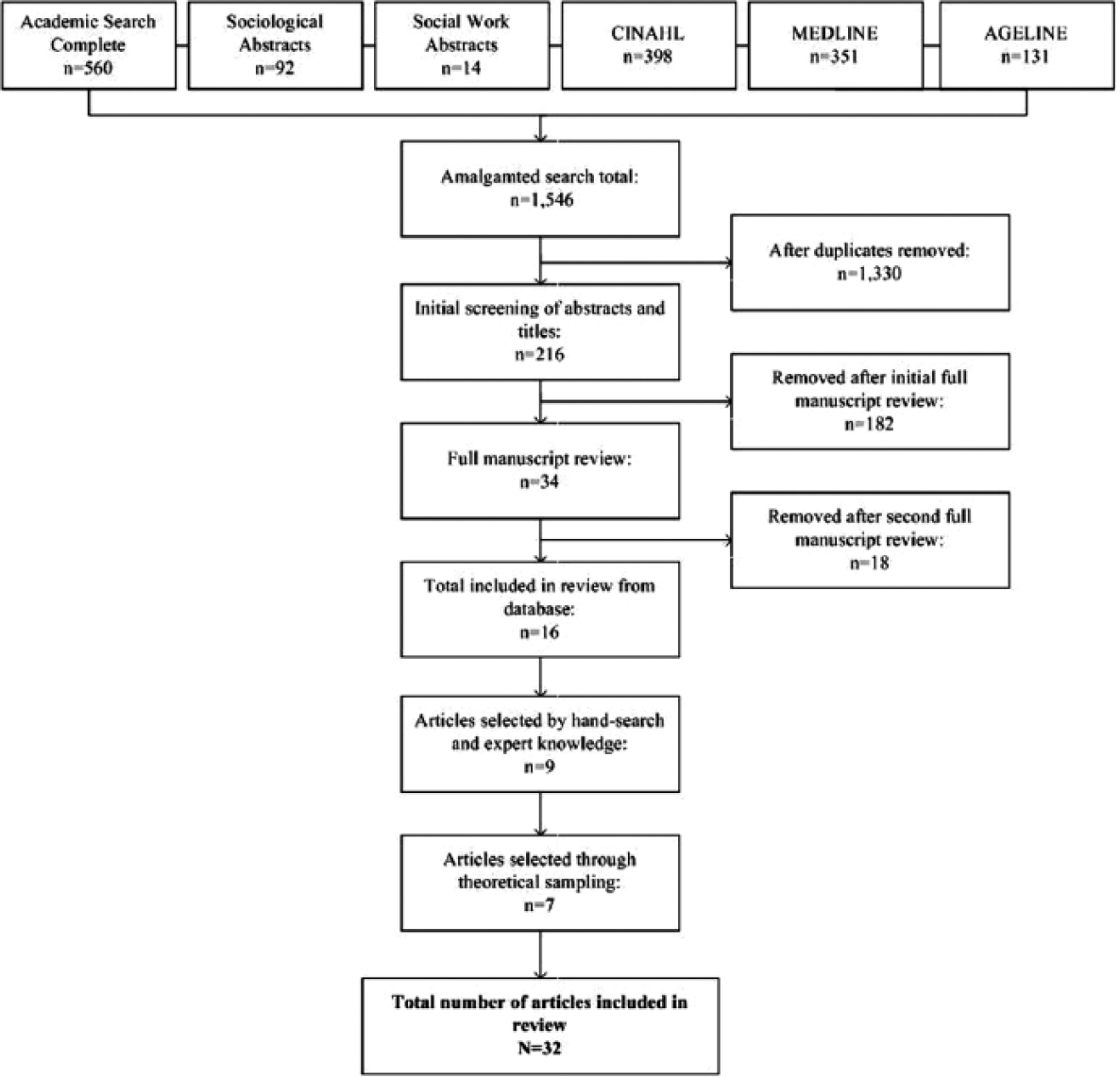
Study selection flowchart.
We did not conduct a formal quality appraisal of the included studies; in CIS, even a methodologically flawed study may have high relevance and, therefore, add to the understanding of phenomenon of interest (Dixon-Woods et al., 2006). The studies reported in this review represent a wide range in rigor and there was a lack of consistency in reporting, which limited the capacity to compare and contrast the literature. For example, several studies, including quantitative studies, did not report on their sampling strategy; and whereas some studies described the sample in great detail, others gave little information. This made it difficult to examine, across studies, how gender, class, or race might influence family involvement. Similarly, although some studies offered significant detail regarding contextual information, in many studies, this information was absent; again, making it difficult to explain how structural factors (e.g., policy) might shape involvement.
Data Analysis and Theory Development
The analysis proceeded in the following manner: First, each retained paper was read several times to gain an appreciation for emerging key concepts. Next, for each individual study, a priori categories including data on study design, setting, sample characteristics, and findings (both direct quotes from study participants and the researchers’ interpretation) related to family members’ role/involvement were extracted onto a spreadsheet. The next steps involved the iterative process of coding the data informed by grounded theory procedures (initial, focused, and axial coding; Saldana, 2013) and checking the coding of the extracted data with the original sources to ensure that these codes accurately reflected the study’s content. Constant comparison methods (Charmaz, 2015) were then used to systematically compare these data to identify and categorize themes and patterns to construct a deeper understanding of inclusion of family in the NH environment. Theoretical sampling was employed to build a more robust critique related to two subthemes: (a) power relations and (b) collaborative and reciprocal relations. Analysis was primarily conducted by the first author and all authors contributed to theory development.
Findings and Synthesis
Twenty-five studies met the inclusion criteria and seven were included through theoretical sampling for a total of 32 studies. Studies from 12 countries were included with the majority having been conducted in Canada and the United States. Twenty-four studies were qualitative employing interpretivist/constructivist qualitative design (n = 9), grounded theory (n = 5), ethnography (n = 6), phenomenology (n = 3), and participatory action research (n = 1). Of the eight quantitative studies, all were descriptive cross-sectional studies.
As illustrated in Table 2, three main themes illustrate the complexities of family involvement in NHs. The review begins with the theme “being involved,” which provides an overview of family involvement. This is followed by the theme “beyond task,” which outlines the symbolic nature of family involvement as it relates to the interpersonal (family–relative) context. The theme “negotiating care” examines involvement in relation to family–staff relationships and broader organizational and sociopolitical factors that may enhance or impede the inclusion of family members in the everyday life of the NH.
Overview of Themes.
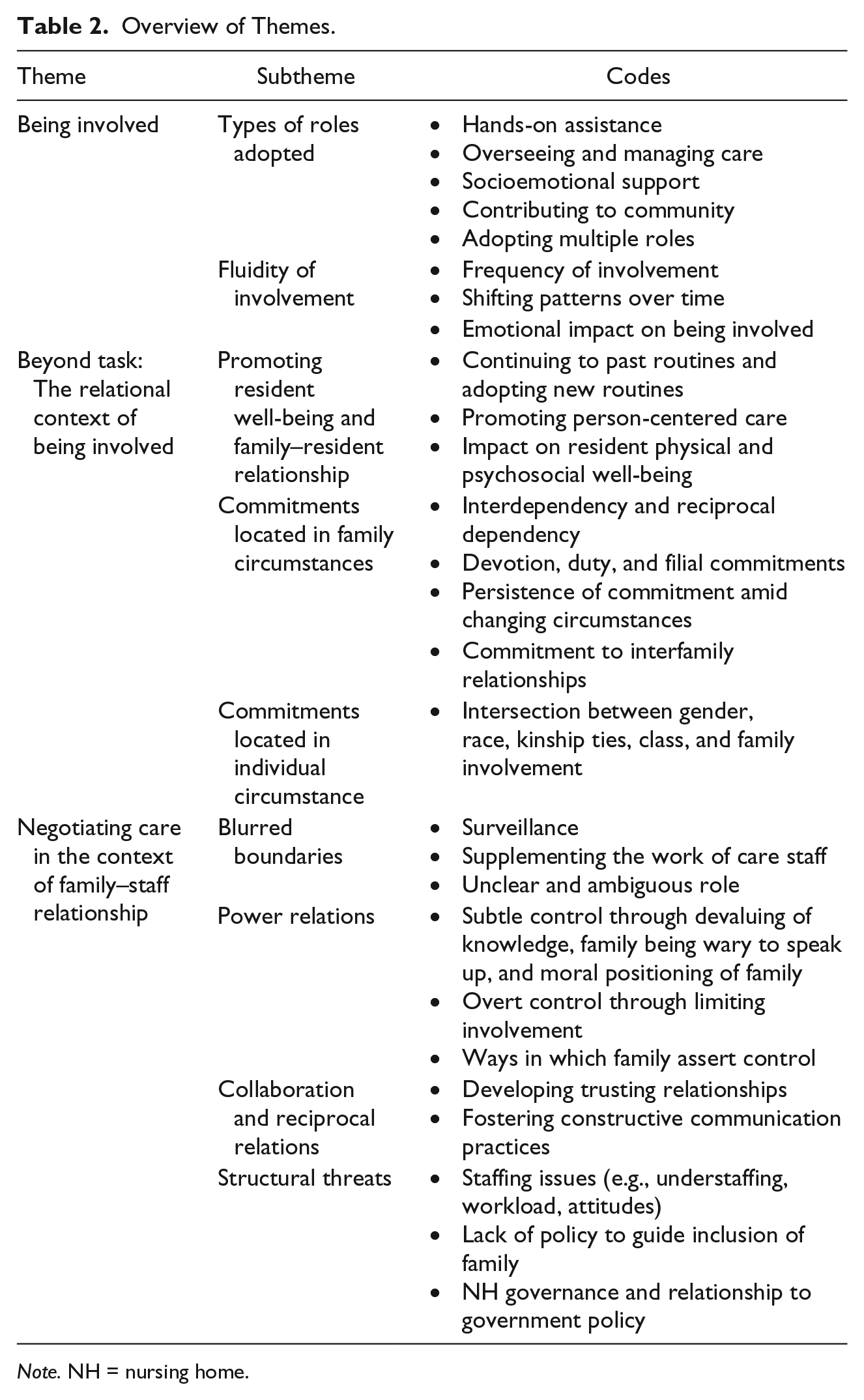
Note. NH = nursing home.
Being Involved: An Overview of Family Involvement in NHs
To contextualize the subsequent themes and to situate the discussion, this theme provides an overview of family members’ patterns of involvement in NH settings. We first describe the types of roles adopted. We then describe the fluid nature of involvement as it relates to the frequency and duration of family involvement, paying particular attention to how involvement may shift over time.
Types of roles adopted
Although family members adopted multiple roles, broadly speaking, their visits were characterized in four ways. First, family provides hands-on assistance including mealtime assistance and help with personal care. These tasks were relegated not only to the “little things,” such as grooming or clipping nails, but also to tasks typically assigned to staff, such as bathing, showering, toileting, and assisting their relative to bed (Baumbusch & Phinney, 2014; Davies & Nolan, 2006; Petersen, Wilson, Wright, Ward, & Capra, 2016; Ryan & McKenna, 2015; Whittaker, 2009; Zhan, Feng, Chen, & Feng, 2011).
Second, family members took on the role of overseeing and/or managing care. This role was characterized by taking their relative to appointments outside the NH (Davies & Nolan, 2006), doing laundry (Zhan et al., 2011), providing supplies (Habjanič & Pajnkihar, 2013), and managing their relative’s affairs (Bern-Klug & Forbes-Thompson, 2008). This role was also marked by being vigilant and being an advocate in relation to monitoring their relative’s quality of life and the quality of care they received from staff (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008; Holmgren, Emami, Eriksson, & Eriksson, 2014; Kellett, 2007; Legault & Ducharme, 2009).
Third, family members provided their relative with socioemotional support. Involvement, in this sense, was expressed in terms of replicating routines (Davies & Nolan, 2006; Førsund, Kiik, Skovdahl, & Ytrehus, 2016), organizing leisure activities (Habjanič & Pajnkihar, 2013), being a “link to the outside world” (Helgesen, Athlin, & Larsson, 2013; Helgesen, Athlin, & Larsson, 2015) by providing their relative with updates on family or neighbors (Zhan et al., 2011) or engaging their relative in activities outside the NH (Førsund et al., 2016; Helgesen et al., 2013; O’Shea, Weathers, & McCarthy, 2014), and providing items of personal value (Habjanič & Pajnkihar, 2013; Helgesen et al., 2013). This role was also characterized by family members conveying to staff their relatives’ preferences, values, and life story so as to help staff understand their relative in the context of his or her life course (Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006).
Finally, family members described their role in terms of contributing to the community by enhancing the well-being of other residents through leisure activities, social visits, distributing refreshments and/or assisting at meals (Davies & Nolan, 2006; Habjanič & Pajnkihar, 2013; Petersen et al., 2016), and providing hands-on assistance when needed (Baumbusch & Phinney, 2014; Brown Wilson, Davies, & Nolan, 2009; Petersen et al., 2016). For some family members, their involvement was tied to their own skills and interests (Habjanič & Pajnkihar, 2013). Others voiced that they simply liked to help out and enjoyed conversing with other residents (Davies & Nolan, 2006). Researchers observed that family members’ contributions to the NH community also augmented roles typically enacted by staff (e.g., assisting other residents at mealtimes; Baumbusch & Phinney, 2014; Petersen et al., 2016).
The fluidity of involvement
Of the studies that reported visiting patterns, it was clear that visits, although variable, occurred on a consistent basis, with family members visiting their relative at least once or twice a week (Baumbusch & Phinney, 2014; Cohen et al., 2013; Førsund et al., 2016; Gladstone, Dupuis, & Wexler, 2006; Habjanič & Pajnkihar, 2013; Petersen et al., 2016; Ryan & McKenna, 2015; Tsai & Tsai, 2012; Whittaker, 2009). Yet, it was clear that family members did not view involvement in fixed or static terms, but saw it as something more fluid and shifting over time (Førsund et al., 2016; Gladstone et al., 2006).
Gladstone and colleagues’ (2006) qualitative longitudinal research of 35 family members lends important insight into the shifting nature of involvement—not just in terms of types of roles adopted in response to their relatives’ care needs but also in terms of the overall frequency of visits. The researchers observed that whereas overall visiting patterns did not change from baseline to follow-up 1 year later, individual family members’ visiting patterns did, with 37% of the sample having less contact, 40% having the same amount, and 23% visiting more frequently. Family members shared a variety of reasons for changes in contact, which point to both relational and structural influences related to their involvement. If the standard of care was questioned (i.e., decreased satisfaction), visits increased to monitor care, to be more visible so that staff knew that they were being observed, or to provide more hands-on support. Visits also increased if a relative’s health condition deteriorated. Involvement decreased if families were more satisfied with care; if their relative was unaware or unresponsive, had difficulties carrying on a conversation; if family members perceived their relative to have adapted to facility life; or if other family members became more involved. Involvement also decreased if a family member’s own personal condition changed including having to balance competing demands, emotional difficulty of visiting (e.g., feeling sadness watching relative deteriorate), and feelings of guilt about facility placement.
As evidenced in Gladstone et al.’s (2006) study, involvement can have a significant negative impact on the physical and emotional health of family members. Reflecting the wider literature on family care work, family members expressed grief and loss in relation to witnessing their relative’s deteriorating health (Bern-Klug, 2008; Irving, 2015; Mullin, Simpson, & Froggatt, 2011; Whittaker, 2009) and NH placement (Zhan et al., 2011). They expressed guilt related to the admission of their relative (Ryan & McKenna, 2015; Tsai & Tsai, 2012) and stress related to observations of insufficient staffing and conflict in decision making (Bern-Klug, 2008; Perry, Dalton, & Edwards, 2010). They expressed worry about their own future health as reflected in their relatives’ illness trajectory (Whittaker, 2009) and over the need to be always “on duty” even when they were off-site (Kellett, 2007).
Beyond Task: The Relational Context of Being Involved
Given that family involvement shifts over time and affects family members’ well-being, it is important to illuminate the dimensions of the family–relative relational context—including that of the family system and the family members’ individual circumstance. In so doing, we illuminate how involvement is more than a resource or commodity, and is deeply rooted within complex relational dynamics.
Promoting resident well-being and family–resident relationship
Researchers were clear that an underlying motivation for family members to be involved was located in their self-expectation to promote the physical, social, and psychological well-being of their relative, and this was achieved in a variety of ways. First, family members structured their visits around activities that promoted connection to past routines (Baumbusch & Phinney, 2014; Petersen et al., 2016; Whittaker, 2009). Yet, at the same time, they adopted new routines to adapt to the NH (Kellett, 2007) and their relative’s changing needs (Førsund et al., 2016; Gladstone et al., 2006). Second, family members nurtured their relatives’ relationships beyond the NH—by taking their relative on outings or sharing stories about family and friends (O’Shea et al., 2014; Zhan et al., 2011). Third, to promote person-centered care, families shared their knowledge about relatives’ life story, preferences, and values with staff (Bern-Klug & Forbes-Thompson, 2008; Brown Wilson et al., 2009; Davies & Nolan, 2006). Finally, some family members voiced the importance of being involved in decision making about everyday care (Davies & Nolan, 2006; Irving, 2015; Reid & Chappell, 2017); however, the degree to which family members actually participated was variable within and across studies. For example, in a cross-sectional survey of 233 family members from 23 special care units, Helgesen et al. (2015) reported that the majority of family members did not participate in decision making and did not express desire to be. Yet, in other studies, they reported a desire to be involved in decision making (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008). Although staff appeared to welcome family input, many family members noted that the opportunity to participate in decision making was controlled by staff (Baumbusch & Phinney, 2014) or they were rarely asked to share their relative’s story and had to initiate these discussions themselves (Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006; Ryan & McKenna, 2015).
Researchers have also noted that involvement can also be understood as a representation of enduring relationships; and by taking up these roles, family members actively sustained these relationships. This reflects particular relational commitments motivated by reciprocal dependence or interdependency. Echoed across several studies, family members expressed involvement in terms of their ongoing commitment to their relative in care. This was embedded in emotional bonds related to a sense of loyalty, devotion, or duty (Bern-Klug & Forbes-Thompson, 2008; Førsund et al., 2016; Fukahori et al., 2007; Gladstone et al., 2006; Kellett, 2007; Mullin et al., 2011; Whittaker, 2009); a sense of filial piety or generational responsibility (Fukahori et al., 2007; Gladstone et al., 2006; Holmgren et al., 2014; Tsai & Tsai, 2012, 2013; Zhan et al., 2011); as well as a sense of maintaining family relationship and “togetherness” (Førsund et al., 2016; Tsai & Tsai, 2012).
Family members’ commitment to the relationship persisted despite physical deterioration (Whittaker, 2009) and cognitive losses their relative incurred (Perry et al., 2010) as well as the accompanying despair of this loss (Mullin et al., 2011), which, for some family members, affected the ebb and flow of their involvement (Førsund et al., 2016; Gladstone et al., 2006). Simultaneously, family members acknowledged the reciprocal benefits of their involvement in terms of maintaining their own identity and sense of self (Davies & Nolan, 2006; Kellett, 2007; Whittaker, 2009); as a study participant voiced, “I’m not visiting my mother just because she needs me; I’m visiting her because I need her” (Whittaker, 2009, pp. 162-163).
Commitment located in family circumstances
For some family members, their ongoing commitment appeared to be shaped by the larger interrelational dynamics of the family system as well as their own contextual circumstances. For example, filial commitments often motivated family members to engage in the daily life of their relatives in care. This was influenced by the degree of “emotional closeness” (Helgesen et al., 2013), sociocultural norms of family caregiving (Fukahori et al., 2007; Lau, Shyu, Lin, & Yang, 2008; Zhan et al., 2011), and by the family member’s commitment to the interrelationships of the family itself. Tsai and Tsai (2012) studied the meaning of family visits and demonstrated that involvement was linked to “a family education model” (p. 306), wherein participants felt it was their responsibility to set an example and teach others about filial commitments. Spousal participants explained that their involvement was motivated, in part, to enable their children to concentrate on their jobs. Zhan and colleagues (2011) described a situation wherein conflict in the family system was related to placement decisions, either by the family, without consultation with each other, or the relative herself or himself who voiced that the placement decision was his or her choice.
Commitment located in individual circumstances
Only a handful of studies acknowledged the influence of a family member’s social locations (e.g., age, gender, class, race) or circumstances on involvement. Given the gendered nature of care work, it is not surprising that the majority of study participants in the research reviewed were women (1,418 women vs. 582 men). Fukahori et al. (2007) argued that gendered roles and social expectations placed on women explained the tendency for women to visit their relatives in NHs for longer durations. Similarly, in Holmgren and colleagues’ (2014) critical ethnography of three NHs, women expressed that involvement was part of their specific gender and relational role. As such, women (primarily daughters) expressed that they felt “squeezed between their gendered generational responsibilities” (p. 230) and their care work. As one participant stated, “It’s very much in woman’s nature, whether you have an aptitude or interest in such things [laughs]. We are born to be caregivers, one can say” (p. 230). Of the studies that reported kinship relations, participants included considerably more children (daughters, daughters-in-law, sons, sons-in law) than spouses (1,289 vs. 334, respectively). Although many studies did not further delineate between daughters and sons, Legault and Ducharme (2009), who examined advocacy roles of daughters, estimated that more than 60% of family carers of people with dementia in NHs are daughters.
Although several studies did not report participants’ age, of those that did, the average age was 58.01 years (range = 20-93 years). Seven studies also reported employment status, demonstrating that many family members were employed either part- or full time (Baumbusch & Phinney, 2014; Fukahori et al., 2007; Gladstone et al., 2006; Gladstone, Dupuis, & Wexler, 2007; Holmgren et al., 2014; Petrovic-Poljak & Konnert, 2013; Tsai & Tsai, 2012; Zhan et al., 2011), and one study reported that family members organized their involvement around paid employment (Baumbusch & Phinney, 2014).
In terms of race and class, very little research addressed this issue forthright and many researchers identified that this was an important area for future research (Bern-Klug, 2008; Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006). That said, Holmgren et al. (2014), in the aforementioned critical ethnography, observed racialized dynamics within the NH setting that resulted in the othering of an immigrant family member and the affordance of power to those family members of the same race category of staff and those of higher economic status. Taken together, these multiple intersections have significant import on how families are included in facility life, which will be more fully explored in the “Discussion” section.
Negotiating Care in the Context of Family–Staff Relationships
Although researchers demonstrated that involvement was located in family members’ kinship relationships and their own personal context, it was abundantly clear that family members were also motivated to be involved because they perceived gaps in the quality of care their relative received and/or they wanted to be helpful in a system that was overtaxed. This theme, thus, elucidates the family–staff relational context in which care work is enacted. First, it examines the blurred boundaries between family and staff care work. Next, it examines collaborative and reciprocal relationships and power relations. Finally, it addresses structural threats to family involvement.
Blurred boundaries: Surveillance and supplementing staff roles
As noted earlier, a role that many family members adopted was an overseer of care. In many cases, this role was grounded in the perception that they must monitor care as they held idiosyncratic knowledge about their relative (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008) and their presence provided a reminder to the staff that they were being observed (Austin et al., 2009; Davies & Nolan, 2006; Legault & Ducharme, 2009). Being involved was sometimes an act of surveillance (Baumbusch & Phinney, 2014; Mullin et al., 2011), wherein family members perceived their involvement as necessary to ensure that their relatives (and other residents) were being treated with dignity and respect (Baumbusch & Phinney, 2014; Legault & Ducharme, 2009).
For many family members, being vigilant was linked to their confidence and trust in the ability of the staff to recognize acute medical conditions and provide quality of care (Baumbusch & Phinney, 2014). This often translated into the provision of more hands-on care. Whereas some family members provided more hands-on care because they wanted to be useful and helpful to staff (Austin et al., 2009; Brown Wilson et al., 2009; Davies & Nolan, 2006; Habjanič & Pajnkihar, 2013), for other family members, identified gaps in the quality of care translated into taking more active roles. Family members were observed to take a more active role to help out staff when workload was particularly problematic (Baumbusch & Phinney, 2014; Davies & Nolan, 2006), when they observed a resident in need (Brown Wilson et al., 2009), or when they (or their relative) felt that they could provide better care than staff (Zhan et al., 2011).
It was clear that there was not a stark bifurcation between the roles and tasks of staff and that of families. Indeed, some family members readily acknowledged that they were doing the tasks normally assigned to staff, as one family member in Baumbusch and Phinney’s (2014) study expressed, “I’m the second care aide, I should get paid” (p. 81; see also, Gladstone et al., 2006; Habjanič & Pajnkihar, 2013). Helgesen et al. (2015) observed that 54.1% of family members surveyed (n = 233) reported that they shared the responsibility with staff for the resident’s well-being and 50.2% of family members surveyed reported that their participation was crucial for the resident’s well-being (spouses reporting this as more crucial than children). Similarly, the daughters in Legault and Ducharme’s (2009) study tended to view their involvement as one of shared responsibility with staff.
The blurring of boundaries was a source of stress and conflict between family and staff and/or the organization (Bauer, Fetherstonhaugh, Tarzia, & Chenco, 2014; Baumbusch & Phinney, 2014; Holmgren et al., 2014). A family member in Ryan and McKenna’s (2015) study stated, “I sometimes find it difficult to know where the lines of responsibility stop and start when it comes to the home and to the family” (p. 42). The ambiguous position of family members was reflected in a survey of 68 family members and 85 nursing staff. The researcher found that staff believed that family members should be limited to socioemotional roles. Conversely, family members believed that they should be more involved in personal care. This lack of clarity about family members’ roles contributed to contested and power relationships as they relate to the negotiation of care for their relative.
Collaborative and reciprocal relationships
Family members adopted different styles of engagement (Brown Wilson et al., 2009; Gladstone et al., 2007), which, for some, was influenced by their expectations of the staff roles (Gladstone et al., 2007; Legault & Ducharme, 2009) and the degree to which they were provided information (Gladstone et al., 2007). Helgesen et al. (2015) reported that the majority of family members felt well supported and listened to, although there were relational and intergenerational differences with spouses feeling better supported than children, and older family members feeling better supported than younger. Similarly, family members in Petersen and colleagues’ (2016) study felt supported by management and were clearly acknowledged by staff who “greet, discuss care, make joint decisions, and thank families” (p. 89).
What was central to collaborative relationships was the notion of trust and communication (Bauer et al., 2014; Brown Wilson et al., 2009; Lau et al., 2008; Legault & Ducharme, 2009; O’Shea et al., 2014). In Bauer and colleagues’ (2014) study, family members identified that being listened to, responded to, and valued as central to trusting relationships. Similarly, Legault and Ducharme (2009) observed that although trust varied (and fluctuated over time), it was fundamental to daughters’ advocacy role. Key to the development of trust were the notions of reciprocity and information sharing, as well as shared responsibility and communication that did not raise conflict with staff. Lau and colleagues (2008) reported that collaborative relationships included the dynamic factors of self-disclosure, evaluation of care, and strategies used to contribute to care, to facilitate family ties, and to see situations from staff’s perspective. Brown Wilson et al. (2009) also identified reciprocal relationships and mutual understanding as central to collaborative relationships. This kind of relationship was grounded in trust and mutual understanding. For example, some family members who recognized and understood the pressures that staff faced (e.g., meeting the needs of all residents) tended to trust the staff.
Power relations
Family involvement, however, was not always supported by staff. Research has found that staffs’ perceptions of family members were shaped by their experiences of family involvement and, therefore, they adopted different ways of interacting with families (Bauer, 2007). These stances are reflected in the wider body of literature that describes staff–family relationships (see Bauer, 2007; Bramble, Moyle, & McAllister, 2009) and illustrate the subtle and overt ways in which staff and administrators managed and controlled family involvement.
In terms of subtle control, the devaluing of family members’ knowledge was one way power relations manifested. Family members expressed feeling ignored (Baumbusch & Phinney, 2014; Holmgren et al., 2014) and their concerns not being taken seriously or followed-up upon (Legault & Ducharme, 2009). They also spoke about their knowledge of their relative not being desired or respected (Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006) and their contributions to the NH community rarely encouraged or recognized by staff (Davies & Nolan, 2006). In addition, subtle control was made evident by family members’ experiences of being wary to speak up for fear that their relative may be the target of reprisals by staff (Bern-Klug & Forbes-Thompson, 2008; Holmgren et al., 2014; Legault & Ducharme, 2009) or concern that staff may feel “attacked” or their credibility questioned (Legault & Ducharme, 2009). Finally, subtle control was observed in the ways staff positioned family members as care recipients rather than as equal members of the care team Bauer et al., 2014; Baumbusch & Phinney, 2014).
Reflecting more overt ways of control, several studies illustrated how staff set limits to family involvement. For example, involvement was confined to particular routines or limited to discussions about care in formal meetings (Holmgren et al., 2014). Two studies identified that administrators, rather than working with family members to address concerns, invited family members to move their relative if they were dissatisfied with the quality of care (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008).
Yet, family also adopted particular ways of engaging to assert or control the staff. Some researchers have portrayed surveillance as a subtle form of control. Whittaker (2009) noted that involvement contributed to an “impossible” role for families, whereby they searched for traces of poor care and neglect as shown on their relative’s body, representing a form of control. Similarly, family members expressed that they judged care (Helgesen et al., 2013; Legault & Ducharme, 2009), which, when assessed to be substandard, increased their involvement so that staff knew they were being observed (Gladstone et al., 2006). From an intersectional perspective, Holmgren and colleagues (2014) observed two family members controlling their relationship with staff based on their own cultural and economic capital. These social locations allowed the family members to foster allegiances with the staff not available to other families.
The work environment and structural threats to involvement
Although involvement in care was motivated by a myriad of family–relative and family–staff relational factors, for some family members, involvement was directly linked to their assessment of the work environment. The work environment imposed significant barriers on staff’s capacity to provide quality care or care that went beyond “basic care” (Bern-Klug & Forbes-Thompson, 2008). In turn, these structural threats prompted family members to both supplement staff work and oversee the care they provided, as described below.
First, family members identified a number of staffing issues that contributed to compromised quality of care, which, in turn, prompted their motivation to be involved. Without exception, all studies reported that family members identified the challenges associated with understaffing and excessive workload. Families also expressed the need for knowledgeable and dependable staff who consistently provided quality care (Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006; Helgesen et al., 2013; Lau et al., 2008). The use of agency or on-call staff, which affected the continuity of care (Baumbusch & Phinney, 2014; O’Shea et al., 2014), was also identified as problematic. Staff’s and administrators’ attitudes also affected family member’s involvement (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008). Along with staff’s lack of buy-in to relational philosophies of care (Bauer et al., 2014; Baumbusch & Phinney, 2014), discordance between family members’ own perceptions of involvement (i.e., being more than a visitor; Baumbusch & Phinney, 2014), staff’s perceptions of what family involvement entailed (psychosocial support; Natan, 2009), and the added workload that came with some family members (Bauer et al., 2014; Baumbusch & Phinney, 2014) contributed to the degree of family inclusion in the facility. Some family members identified that the cultural composition of staff hampered collaborative relationships and dialogue (Bauer et al., 2014; Baumbusch & Phinney, 2014; Holmgren et al., 2014; Petrovic-Poljak & Konnert, 2013), and for some, this was a source of conflict and experience of “othering” (Holmgren et al., 2014).
Second, at the local NH policy level, several studies identified the lack of formalized opportunities for families to participate in decision making, instead relying on informal conversations, ultimately resulting in miscommunication between staff and family (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008). Furthermore, staff’s transparency in the event of incidents, the quality of contact or of the information received about the admission to the NH (Legault & Ducharme, 2009), and family members’ beliefs and previous experiences with NHs (Lau et al., 2008) were identified as influencing family members’ trust in the NH, which, in turn, influenced their involvement.
At the broader regulatory level, researchers identified that family involvement was informed by the relationship between government policies and NH governance. For example, all the family members in Austin and colleagues’ (2009) study talked about health care restructuring, which influenced staff assignments and workload that, in turn, influenced how they were involved. Similarly, Baumbusch and Phinney (2014) demonstrated how the impact of restructuring (e.g., increase in resident complexity, changes in staffing) influenced family members to adopt roles typically assigned to care staff. The researchers also linked their findings to specific government policies of NH bed allocation that influenced the degree to which the NH could support a particular resident’s cultural/language needs, which prompted family members to be more involved.
Discussion
The themes in this review illuminate the complexities involved in family members’ engagement in the lives of their relatives residing in NHs. The first theme, “being involved” described the kinds of roles family members adopted. It described how family adopted multiple roles, demonstrating that involvement extends well beyond being a “visitor”; and, with longitudinal evidence (Gladstone et al., 2006), showed how involvement shifted over time in relation to the family members’ personal circumstance and the relationship with their relative and staff. This brought us to the second theme, “beyond task,” which showed how family involvement was located in the complexities embedded in the relationship with their relative (Tsai & Tsai, 2012; Zhan et al., 2011) as well as how involvement was linked to the family members’ own social locations (e.g., gender and race; Holmgren et al., 2014). The final theme, “negotiating care” highlighted how involvement was shaped by the family members’ appraisals of quality of care and the busyness of the work environment, which affected their relationships with the staff. It also highlighted that family members were well-aware of the structural challenges that shaped how care work was enacted. In this section, we discuss the findings in relation to the notion of inclusion in terms of (a) the family–staff relationships; (b) the need for policies, at the local NH and government level, to support family care work in NH settings; and (c) the importance of valuing care work at the wider societal level.
First, at the relational level, family roles are complex and, at times, contested: Although there seems to be overall agreement regarding the value of family involvement, there is less agreement about the kinds of roles families should enact, and researchers have demonstrated that staff and administrators held conflicted views about the role of the family (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008; Natan, 2009; Reid & Chappell, 2017). Yet, as Austin et al. (2009) contended, “ethical action involves the attempt to understand the other’s situation, perspective, and vulnerability, and requires a true engagement with the other” (p. 364). Thus, at the relational level, an important step in building inclusive spaces requires mutual respect and recognition. This has important implications for the moral positioning of family members (e.g., to be free from oppression and othering; Holmgren et al., 2014) and the provision of different and equal opportunity for family members to take part in decisions and activities that affect their relative (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008; Davies & Nolan, 2006). Poor communication practices and unclear expectations related to family’s role do very little to nurture a space of recognition and respect. Moreover, the process related to “othering” such as labeling families as “difficult,” silencing/devaluing their knowledge and contributions (Bauer et al., 2014; Baumbusch & Phinney, 2014; Holmgren et al., 2014), and giving poorer quality of care based on race, gender, or socioeconomic status (Holmgren et al., 2014) do very little to foster a sense of solidarity and recognition. Rather, it perpetuates social exclusion creating us–them relationships and reifying hierarchical boundaries. As McNay (2004) argued,
To be misrecognised is not to be thought ill of or devalued in other’s attitudes but to be denied the status of a full partner in social interaction as a consequence of institutionalized patterns of value that deem certain individuals less worthy of respect and esteem than others. (p. 189)
It also has implications related to the recognition that families’ role in care work will likely continue once their relative moves into an NH, as will their relationship that has developed over a life course. In addition, families may be in transition, or even in crisis, as they adapt to new roles and the profound changes in their relative’s well-being (Rolland, 2017). As Bern-Klug (2008) and Whittaker (2009) demonstrated, it is important to contextualize family care work in the reality of dying and death that characterizes NH settings. In so doing, it illuminates the existential conditions in which family involvement operates, leaving family often on their own to deal with complex emotions (Rolland, 2017). In this sense, the creation of inclusive spaces translates into the recognition that, for many families, care work can be shaped by an array of emotions (e.g., grief); yet, it simultaneously is integral to their well-being (Bern-Klug & Forbes-Thompson, 2008; Whittaker, 2009). In addition to staff recognition and respect for family care work, the notion of mutual respect and recognition also extends to families themselves who need to understand the limits of what an NH can offer.
In fostering inclusive spaces, family nurses have an important leadership role in demonstrating mutual recognition and respect through the creation of welcoming environments that give opportunity for family to participate in community life, through the provision of adequate and honest information at admission and throughout the NH stay, and through role modeling collaborative relationships. This could take the form of inviting families to participate in decisions in the NH and the care of their relative in meaningful ways; or helping families understand philosophies of care such as person- or relation-centered care and how this might be reconciled when conflicting positions between staff, family, and residents; or requesting feedback from family members on ways in which they envision an inclusive space.
Second, if family nurses are to be integral to fostering inclusive spaces, there must be support at the local NH and broader policy level. At the local level, of the research that linked involvement and NH policy (Baumbusch & Phinney, 2014; Bern-Klug & Forbes-Thompson, 2008), it was clear that there appeared to be little policy in this area to support or formalize family’s rights to be involved. If family inclusion is by happenstance, the potential for marginalization of individuals and groups, as observed in Holmgren and colleagues’ (2014) study, will persist. The need for inclusive policies at the local level is, therefore, imperative—including policies that address the multiple intersections of staff and family (e.g., cultural competencies).
Family members recognized that policy developments at the government level (e.g., health care restructuring) contributed to challenging work environments for the staff (e.g., increased workload), which, in turn, prompted them to oversee care or take on tasks normally assigned to care staff (Austin et al., 2009; Baumbusch & Phinney, 2014). As Baumbusch and Phinney (2014) posited, “an unintended consequence of restructuring may be a transfer of historically paid care work activities to unpaid care workers (i.e., family members) contributing to confusion and tension among those engaged in these activities” (p. 90). In jurisdictions shaped by neoliberal welfare regimes, family care work is seen as a policy solution rather than a policy challenge (Armstrong & Braedley, 2013). Therefore, there is greater reliance on family care work without adequate supports for family and without addressing the root cause of structural threats in the NH itself. Family involvement, in this sense, is an individual responsibility that diverts attention from the threats posed by suboptimal working conditions for staff. This places NH settings in precarious situations, whereby family involvement becomes increasingly relied upon without the motivation to seek sustainable solutions for understaffing and increased workload. The commitment to foster inclusive environments goes beyond the coordinated actions and capacities of individuals; regulatory bodies have the responsibility to develop policies that promote such environments.
Finally, there is an urgent need to address societal attitudes and beliefs that continue to devalue care work across the life course. Sevenhuijsen (2000) argued that caregiving and care receiving must be recognized in our everyday social and political lives; and “care” should be understood as a democratic process that leads to inclusive democracy. Failing to address care work as more than a commodity (Banerjee & Armstrong, 2015), “more than different caring roles in relation to staff” (Whittaker, 2009, p. 165) will perpetuate a system that locates family involvement in individual responsibility, divesting the citizenry from its collective responsibility of an ethos of care.
Limitations and Areas for Future Research
It is worth reflecting that family members represented in the reviewed studies visited their relatives frequently and many were heavily involved in care. Whereas Gladstone and colleagues (2007) have taken a longitudinal perspective on family involvement, most studies gathered data from one point in time making it difficult to conclude whether heavy involvement persisted. Furthermore, as much of the research focused on those who were highly involved, the motivations and circumstances of those who were less involved were not clearly understood. Therefore, further research focusing on the ebb and flow of involvement is warranted. Similarly, although the area of staff–family relationship is an expanding area of research (see Bauer et al., 2014), more research is needed to examine how these relationships unfold over time.
Because the health system will continue to exert different pressures on family to adopt roles in NHs, understanding family members’ capacities and limitations remains critically important. Consideration must be given to family contextual factors (e.g., geographic proximity, employment status, and family members’ own health status) and facility-level factors (e.g., inclusive opportunities). There is also an urgent need to scrutinize the ways in which age, gender, class, and race intersect to shape involvement and family experiences in NHs. Such information is beneficial to enhance our understanding of the patterns of involvement at the individual level and enable linkages among relational and macrostructural factors. This also includes the need for a critical understanding of the socio-organizational processes that enhance or impede meaningful inclusion of families in NHs. Taken together, given the diversity in the ways family are involved, the various ways in which NHs facilitate inclusivity, and the shifting sociopolitical and organizational contexts, research should continue to investigate this complex topic.
Footnotes
Acknowledgements
The authors thank the anonymous reviewers of the Journal of Family Nursing for their helpful feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Canadian Institute for Health Research (CIHR).
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.