
Abstract
Objective:
Although prevention of radial artery thrombosis and cardiac complications after interventions using radial access is well investigated, there is yet no clinical study that completely evaluated access-related complications. However, there is still no consensus on what exact treatment should be used in these patients. In clinical practice, analgesic, anticoagulant, and antiplatelet treatments usually improve symptoms in patients with pain; however, in some patients, complaints may persist and may not respond to these treatments. In these patients, low-risk embolectomy with a small skin incision may be beneficial.
Methods:
A total of 102 patients with radial artery thrombosis after cardiac catheterization were included in the study between 2016 March and 2018 December. After the patients’ initial evaluation, anticoagulation with enoxaparin or tinzaparin and antiplatelet therapy with acetylsalicylic acid and oral/local analgesic/anti-inflammatory and local anesthetic therapy were administered for 1 month. Patients whose symptoms resolved after medical treatment were followed up as outpatients. Embolectomy was performed in consenting patients who did not respond to the medical treatment.
Results:
Of 102 patients included in the study, 33 underwent embolectomy, whereas 69 received only medical treatment. None of the patients experienced any complications, morbidity, or mortality in the peroperative period and during the medical treatment. The pretreatment symptom scores of patients who actively use their hands in daily life and profession were significantly higher than the scores of patients who are relatively less active (P = .013). Pretreatment symptom scores were negatively correlated with age (r = −0.584); symptom scores increased significantly with the decrease of patient age. No benefit from medical treatment and need for surgery was significantly greater in patients who are younger and use their hands actively in daily life and profession (P = .028). The decrease in symptom scores after treatment was significantly greater in the surgical group than in the medical group (P = .003).
Conclusion:
Radial access should be exercised with care in patients who may develop significant thrombosis-related complaints and it is necessary to decide whether radial access is essential. If patients have ongoing symptoms despite medical treatment, embolectomy can be considered as a treatment option.
Introduction
In recent years, an increase in cardiovascular interventions has been associated with an increase in iatrogenic injuries. Pseudoaneurysms of the femoral artery are the most frequent type of injuries 1 ; however, radial artery thrombosis (RAT) can also occur in patients with radial artery access. 2 Many studies have described precautions intended to prevent thrombosis after radial access 3 -13 ; however, there is still no clinical study that completely evaluated access-related complications and no consensus on what exact treatment should be in these patients.
If the patient does not show signs of ischemia in the hand and arm or any related symptoms of pain, burning, and numbness then RAT is not clinically significant. In these patients, the symptoms can resolve with analgesic, anticoagulant, and antiplatelet therapies 14,15 ; however, in some patients, the complaints may continue, with no response to medical treatment.
The aims of this study are to investigate the factors that cause prominent subjective symptoms in patients who developed RAT after radial access, to assess effectiveness of medical treatment, and to show the feasibility and results of low-risk embolectomy with a minimal skin incision in patients who did not respond to medical treatment.
Methods
Study Population
This study was approved by the Institutional Review Board of Yüksek İhtisas Education and Research Hospital, Ankara/Türkiye (2015/58 decision number). Patients who were followed up with only medical treatment were provided detailed verbal information, and signed informed consent was obtained from patients who underwent embolectomy. This study included 53 patients from Yüksek İhtisas Education and Research Hospital, 36 patients from Aksaray University Education and Research Hospital, 13 patients from Dışkapı Yıldırım Beyazıt Education and Research Hospital. While including all the patients in the study, all the same inclusion criteria were used.
This multicenter prospective clinical study included a total 102 patients with RAT after cardiac catheterization who were referred by a cardiologist or presented for vascular surgery with complaints involving the hand and forearm by development of RAT between March 2016 and December 2018. After patients’ initial evaluation, anticoagulation with enoxaparin 200 IU/kg/d, 2 × 1, or tinzaparin 200 IU/kg/d, 1 × 1; antiplatelet therapy with acetylsalicylic acid (ASA) 300 mg/d orally 1 × 1, if not currently used, and oral/local analgesic/anti-inflammatory and local anesthetic therapy were administered for 1 month. Patients who improved after medical treatment were followed up as outpatients and given no further treatment. Embolectomy was offered to patients who did not improve with medical treatment. Patients with partial or total RAT but without any complaints related to transradial access (TRA) and not given any medication were not included in the study.
The baseline characteristics of patients in both groups and the details of prior coronary interventions were compiled and analyzed. The symptom scores (added as supplementary file) used to evaluate the severity of subjective complaints, such as pain, numbness, burning, and the degree of motor force in the forearm and hand. Pretreatment symptom scores were obtained before the initial medical treatment. Posttreatment scores confirmed the absence of prominent symptoms, and there was no need of further medication. The follow-up period was not predetermined regardless of whether surgical or medical treatment was administered. Patients whose complaints had completely resolved following treatment were excluded from follow-up and advised to visit the hospital if their complaints reappeared. Patients with RAT after cardiac catheterization but no complaints on discharge or follow-up were excluded from the study.
The patients’ recovery was completely evaluated based on the symptoms. If the patient was asymptomatic or had mild symptoms that would not limit his daily life, following medical or surgical treatment, then we considered this patient to be cured and stopped the treatment. If symptoms persist to affect the daily life of patients after treatment, and if the patient was noticeably disturbed by this situation, we considered this patient not yet recovered and continued medical treatment. As a result, if the symptoms (more or less) did not affect the daily life in activity, no treatment was necessary in this situation. On the contrary, if it affected patient’s daily life significantly, we considered that this patient required treatment.
People who actively use their hands and arms in their daily life and profession were accepted as “active in daily life.” In our study, those included in this group consist of patients with professions such as musicianship, computer operating, writing, tailoring, nursing, angiography technician, medicine, teaching, etc. The patients in this group had high sociocultural levels in general.
Surgical Procedure
Embolectomy was performed in an operating room with 2% prilocaine as local anesthesia and intravenous midazolam for sedation, as needed. A 2-cm skin incision was made at the wrist level, and a small arteriotomy was made on the distal portion of the radial artery. Distal and proximal embolectomy was performed with a 2F Fogarty catheter (Edwards Lifesciences), and full flow was achieved in the radial artery. Next, the arteriotomy and skin were closed to complete the procedure. Patients were followed up for 1 day and discharged after pulse control and checking for any problems at the operation site.
Radial Access and Cardiac Intervention
This study includes patients for both diagnostic and interventional patients’ procedures. Cardiac catheterizations with TRA were performed by senior operators with at least 10 years of experience and having performed a minimum of 100 diagnostic angiographies and 50 interventions each year. Patients with a normal Allen test were given local anesthesia with 2 to 3 mL of 2% prilocaine, and cannulation of the radial artery was performed with 5F or 6F hydrophilic 7-cm sheaths (RADIFOCUS Introducer II, Terumo, Europe NV). After sheath insertion and administration, 200 mg nitroglycerin and 5000 IU heparin were administered and 6F diagnostic coronary catheters (Boston Scientific) were used for radial coronary angiography. Routine presedation with agents, such as midazolam or diazepam, was not used. To exclude radial artery spasm or other complications, radial angiography was performed in the same line after the procedure. A TR Band (Terumo, Europe NV) was used to control bleeding after the procedure. It was inflated with 30 mL of air that was slowly evacuated over an average of 2 hours. The nondominant arm was generally used for access. In case of arterial spasm, the opposite arm or femoral artery was accessed in the same session.
Statistical Analysis
Between-group differences in continuous variables were compared using the Kolmogorov-Smirnov, median, Mann-Whitney U, or independent sample t tests. The χ2 or Fisher exact tests were used to compare categorical variables. The significance of associations of patient characteristics and symptom scores was determined by Pearson correlation coefficient. Statistical analysis was performed with SPSS version 25.0 (IBM Corp). The significance level was set at α = .05; P < .05 was considered statistically significant.
Results
During the study, a total of 3652 patients underwent radial access in 3 centers and 102 patients who developed RAT were included in this study. Of the 102 patients, 92 were followed up for the appearance of RAT. Ten were initially asymptomatic but were readmitted to hospital because of clinically significant complaints.
We suggested and applied immediately surgical treatment in the first evaluation, since they would not benefit from medical treatment in 2 patients who developed pseudoaneurysm at the radial intervention site and in a patient with hand-critical ischemia (3 of 102 patients). Thirty of the 102 patients did not show any improvement with medical treatment and were treated with embolectomy. None of the embolectomy patients had procedure-associated complications, perioperative morbidity, or mortality. Fifty-one of 69 patients showed improvement with 1 month medical treatment so they excluded from the follow-up. We continued additional medical treatment for an average of 1 month for patients (18 of 69) who did not accept surgery, but were still symptomatic despite 1 month of medical treatment. In the control evaluation after the second medical treatment, we found that almost all patients receiving additional medical treatment had significant symptomatic improvement (only 5 of 18 patients had minimal symptoms). Patients whose complaints had completely resolved following treatment were excluded from follow-up and advised to visit the hospital if their complaints reappeared. When we question patients with minimal symptoms after additional medical therapy (5 patients), we found that their current complaints did not significantly limit their daily lives, so that these patients were considered to be cured and anticoagulant treatment was terminated and only analgesic treatment was recommended (Figure 1).

Flow diagram showing the design of the study according to the response to the treatment of the patients included in the study.
Baseline Characteristics
The baseline characteristics of both groups are summarized in Table 1. The surgical patients were significantly younger than the medical patients (55.5 ± 7.5 years vs 63.3 ± 5.7 years, P = .023). Differences in sex, smoking, obesity, hyperlipidemia, diabetes mellitus, hypertension, chronic obstructive pulmonary disease, additional coronary interventions, and body mass index between the 2 groups were not significant. There was no difference in the arm used for access (P = .803), but the surgical patients actively used their hands in their daily activities (P = .028).
Baseline Characteristics of Patients With Radial Artery Thrombosis After Coronary Angiography.

Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention; SD, standard deviation.
Operative Findings
The characteristics of the surgical patients are shown in Table 2. The mean duration of the embolectomy procedure was 26.5 ± 3.3 minutes. None of the patients experienced any complications, postoperative morbidity, or mortality. Embolectomy was terminated in 2 patients because full flow could not be achieved; postoperative medical treatment was done. Embolectomy was performed 3 days after discharge in one patient because of signs of acute ischemia in the hand. The symptoms completely resolved after surgery with no permanent sequelae. Radial artery rethrombosis occurred in one patient 7 months after embolectomy without any signs of ischemia in the hand or significant symptoms. This patient was medically treated and followed. Two patients had pseudoaneurysms at the sheath insertion site and were surgically treated (Figure 2).
Surgery Details of the Surgical Group.
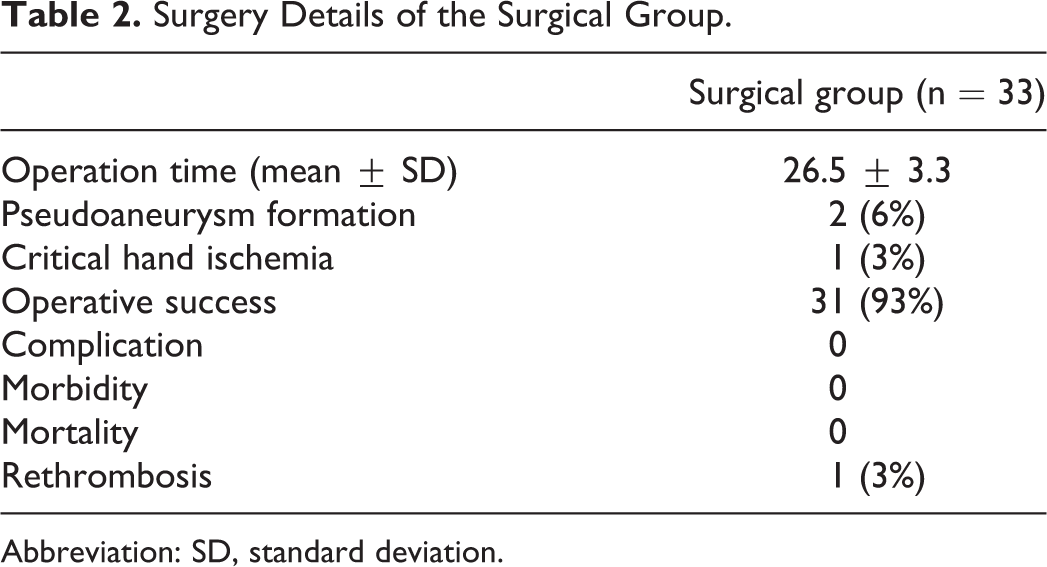
Abbreviation: SD, standard deviation.

A, Intraoperative view of a 44-year-old woman with a thrombosed pseudoaneurysm of the radial artery at the sheath entrance site (arrow). Thrombosed pseudoaneurysm was diagnosed by color Doppler ultrasound. B, The same patient after removal of the thrombus and repair of the pseudoaneurysm. The extracted acute thrombus is shown (arrow). C, Subacute organized thrombus from 56-year-old man. Embolectomy was performed because the patient did not improve with medical treatment. D, An image of the same patient 6 months after embolectomy. A very small skin incision scar (approximately 2 cm long) is visible (arrow).
Other Findings
The duration of treatment and symptom scores in the 2 groups are shown in Table 3. Pretreatment symptom scores were significantly higher in the surgical group than in the medical group (P = .11), but there were no significant differences in their posttreatment symptom scores (P = .829). The decrease in symptom scores after treatment was significantly greater in the surgical group than in the medical group (P = .003). The pretreatment symptom scores of patients who actively used their hands in daily life and profession were significantly higher than those of patients who were relatively less active (P = .013). Pretreatment symptom scores were negatively correlated with age (r = −0.584); symptom scores increased significantly with decrease in patient age. Follow-up and medication use were significantly longer in the medical group than in the surgical group (P < .0001).
Data of Symptom Scores and Treatments in Both Groups.a
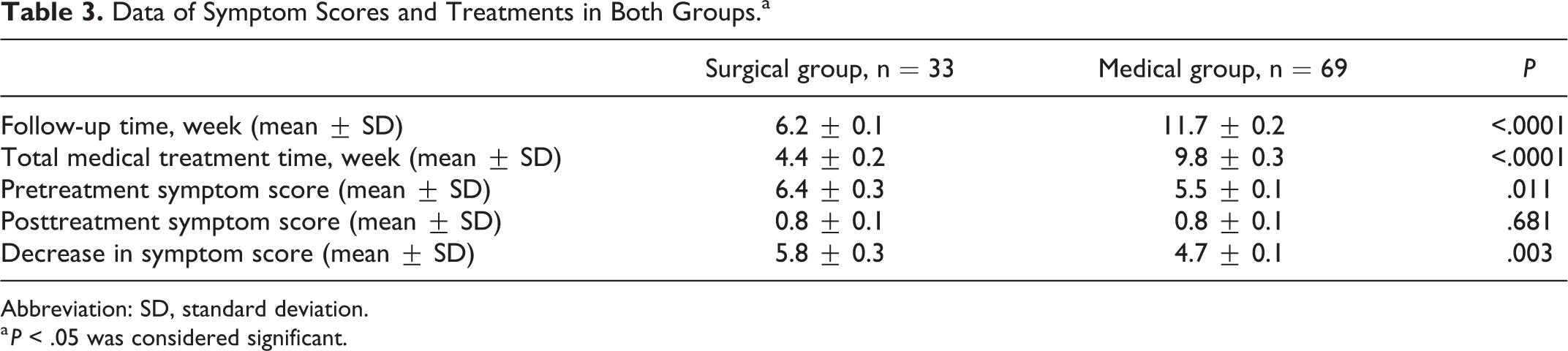
Abbreviation: SD, standard deviation.
a P < .05 was considered significant.
Discussion
Recently, radial artery access is being routinely performed in many centers for cardiac catheterization. Compared with transfemoral access, TRA is associated with lower adverse cardiac events and has lower mortality even in high-risk patients. Transradial access is associated with less bleeding, reduced access-site vascular complications, less patient discomfort, earlier mobilization, and reduced procedure-related costs than femoral access. However, TRA is technically more difficult with a longer learning curve and is associated with radial artery spasm and RAT. 16
Radial artery thrombosis may be associated with age, sex, diabetes, obesity, and radial artery diameter. The diameter and length of introducer sheaths and catheters used during the intervention, presence and duration of additional coronary interventions, heparin use, and the duration of hemostasis to control postoperative bleeding may also influence RAT development. Radial artery thrombosis is always possible in patients with unfavorable risk factors regardless of optimal interventional conditions. All patients with TRA should be evaluated for thrombosis before discharge. Patients without a pulse or with significant symptoms at the sheath insertion site should be evaluated for RAT with color Doppler ultrasound. There have been many studies on RAT after cardiac catheterization, but we have seen only a few case reports and 2 clinical trials that evaluated patient care after thrombus formation. 14,15
Zankl et al 14 administered low-molecular-weight heparin (LMWH) for 4 weeks to symptomatic patients who developed RAT after cardiac catheterization. They reported partial or complete recanalization in 86.7% of their patients and 4 asymptomatic patients with recanalization without treatment. They did not report the proportion of patients with symptomatic improvement or the subsequent treatment of patients who failed medical treatment. A similar study by Uhlemann et al 15 compared formation of RAT with use of 5F or 6F introducer sheaths. The 6F introducer sheath was found to be associated with the development of thrombosis; 2 weeks of LMWH was effective for recanalization compared with no medical treatment.
In this study, 1 month of LMWH was successful in 69% of RAT patients and embolectomy was performed in patients with failed medical treatment. Anticoagulation and antiplatelet medications are successful in many patients; however, they do not produce the desired results in some. Low-risk embolectomy to the radial artery under local anesthesia may be a simple and effective alternative to long-duration medical treatment in those patients. This is the first, multicenter prospective clinical study to show that embolectomy can be performed in RAT patients who did not respond to medical treatment. Patients’ complaints improved significantly in the embolectomy group, and their baseline symptom scores before the initial medical treatment decreased significantly following embolectomy. The decrease in symptom scores was better in embolectomy patients than in medical patients (P = .003, Table 3).
The clinical importance of prompt diagnosis of RAT in initially asymptomatic patients remains unclear, but some patients develop symptoms after hospital discharge and resumption of their daily activities. The development of complaints was not affected by the use of the dominant arm for radial access (P = 0.803). Active use of hands in daily life or in a profession may be the main reason for the development of complaints. One of our patients was a musician who was asymptomatic at discharge with no clinical signs of RAT. The patient was readmitted with pain, burning, and numbness in his hand and arm. Significant tenderness at the sheath insertion site and no radial artery pulse were found on physical examination. When the coronary intervention was reviewed, it was learned that only transient radial artery spasm had developed. Color Doppler ultrasound revealed complete thrombus of the radial artery. After 4 weeks of medical treatment, the patient was readmitted within 2 weeks because of a daily increase in symptoms. The patient improved significantly on the first day after embolectomy.
Medical treatment was not given to patients with partial or total RAT but without any complaints related to TRA, so these patients were excluded from the study. Prophylactic medical treatment might be given to patients who use their hands actively in their usual daily activities even in the absence of clinical signs of RAT. Prophylactic anticoagulants or only ASA for 1 month may be recommended for patients who develop transient radial artery spasms during the cardiac intervention to prevent the development of thrombosis.
Our aim was not to determine the rate of thrombosis after radial intervention or to show the best technique to reduce thrombosis. The primary study objective was to completely evaluate patients who developed access-related complication after cardiac intervention and to create a guide for the treatment of these patients as well. Other objectives were to determine the effectiveness of medical treatment in patients with RAT and recommend embolectomy as an alternative treatment who did not respond to 1 month of medical treatment. The implications of the results and recommendations are given below: Care should be exercised when using radial access in young patients and patients who use their hands actively in daily life and in their profession. Radial artery thrombosis can be treated medically or surgically if medical treatment fails in patients with obvious complaints. As shown in this and previous studies, RAT may develop without symptoms in some patients. Radial access should be used with caution in patients who may develop significant thrombosis-related complaints. Patients with multivessel coronary disease may eventually require coronary artery bypass surgery. As radial artery grafts may be desired in those patients, it is necessary to decide whether radial access is essential. As in previous studies
14,15
and our study, it was observed that LMWHs (enoxaparin and tinzaparin) had a significant success in the treatment of arterial embolism and thrombosis.
Radial artery thrombosis is a quiet complication of TRA that rarely leads to critical hand ischemia requiring intervention because of the dual vascular supply of the hand from the palmar arch. 17 -19 Rhyne and Mann reported successful elimination of critical hand ischemia in a patient with RAT by percutaneous intervention. Rademakers and Laarman 18 attempted percutaneous intervention in a patient who developed critical hand ischemia, but when that failed, a vascular surgeon was consulted. Ayan et al 19 reported a patient who required a fourth-finger amputation after developing critical hand ischemia related to TRA.
The ethics of repeat percutaneous intervention for treatment of critical hand ischemia after TRA are questionable. Repeat percutaneous intervention may result in delays and permanent severe sequelae. If a surgery is ultimately needed, then there may be an increased risk of bleeding and the results may be limited. To avoid serious permanent complications in such patients, support from vascular surgery should be requested on readmission.
There are a few limitations to the present study. In this study, there were fewer patients in the surgical group than in the medical group, which may be a limitation because medical treatment was successful and many patients would not agree to surgery as the initial treatment. We performed surgery following the failure of medical treatment after patient’s approval. Most patients had a significant improvement in their symptoms soon after surgery and expressed a wish that they had surgery sooner.
Conclusion
Radial access should be performed with caution in patients who may develop significant thrombosis-related complaints, and it is necessary to decide whether radial access is essential. In patients with prominent subjective symptoms due to RAT after cardiac catheterization, medical treatment can significantly improve symptoms and provide recanalization of the radial artery, but sometimes it does not. Despite severe complications that require surgery, such as critical hand ischemia or pseudoaneurysm formation, embolectomy is beneficial. The efficacy and safety analysis shows that low-risk embolectomy is a safe and simple method, which can be recommended as an effective and alternative method for the medical treatment of RAT after cardiac catheterization.
Supplemental Material
supplementary_file_1 - Use of Embolectomy With Local Anesthesia for Anticoagulation Failure in Radial Artery Thrombosis
supplementary_file_1 for Use of Embolectomy With Local Anesthesia for Anticoagulation Failure in Radial Artery Thrombosis by Metin Yılmaz, Serkan Sönmez, Oğuz Uğur, Murat Gül, Oğuz Yıldırım, Deniz Özkan, Bahadır Aytekin and İlker İnce in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Contributions
Serkan Sönmez, Oğuz Uğur, İlker İnce: carrying out the operations, interventons and collecting data; Murat Gül: statistical analysis; Oğuz Yıldırım: literature reviewing and interpretation of data; Deniz Özkan: drafting the manuscript and designing the figures; Bahadır Aytekin: writing of the manuscript; Metin Yılmaz: study design, final review and correspondence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.