
Abstract
Introduction:
Patients with sepsis have high rates of major adverse cardiovascular events (MACE) in the literature, but the stratification of those at risk has been limited. Statin indicated groups provides clear criteria for therapy, but the risk of MACE after sepsis based on these groups has never been assessed.
Materials and Methods:
This was a retrospective cohort analysis conducted on adult patients admitted from January 1, 2013, to December 31, 2013, with suspected or confirmed sepsis and data available on statin use. Patients’ past medical history; statin use prior, during, or at time of discharge; and occurrence of MACE were recorded from electronic health records.
Result:
A total of 321 patients were screened and 265 were found to have data available on statin use. The mean age of the patients was 59 ± 15 years and 47% were female. Overall, 9% were observed to have a MACE at 1 year, with significantly higher rates in those in a statin indicated group (12.2%). On admission, 174 patients were not taking a statin out of whom 52% were in a statin indicated group. Among those in a statin indicated group who survived to hospital discharge, only 10% not on a statin on admission received a statin on discharge, whereas 89% on a statin on admission received a statin on discharge.
Conclusion:
There is a high risk of MACE after sepsis especially among those in statin indicated groups with significant clinical inertia in prescribing practices.
Introduction
Sepsis is a frequently encountered clinical condition and the sixth most common reason for hospitalization in the United States according to data from 2009. 1 Unfortunately, mortality rates in sepsis remain elevated at 15% to 30% with no demonstrable improvements over the last decade. 2 In recent years, long-term cardiovascular complications of sepsis are becoming increasingly recognized with incidence rates up to 30%. Cardiovascular events may provide some of the explanation for the increased long-term mortality in sepsis survivors. 3
Several trials have demonstrated the efficacy of statins in the primary and secondary prevention of cardiovascular events. 4,5 The use of statins is largely focused on primary or secondary prevention of vascular disease in stable, nonhospitalized patients. 6,7 Despite their widespread benefit, statins continue to be under prescribed. Given the presumed mechanism of plaque destabilization in acute illnesses leading to more clinical events, statins seem especially appealing in sepsis. However, large randomized clinical trials have failed to show a benefit in preventing progression of sepsis or on all-cause mortality, but have not specifically looked at cardiovascular events. 8 Retrospective studies looking at statins in sepsis have not consistently assessed cardiovascular end points, and more data are needed on the incidence of cardiovascular events and the role of statins in reducing these events. 9
Given the high cardiovascular event rate after sepsis, understanding whether these traditional statin indicated groups are associated with an increase in major adverse cardiovascular events (MACE) after sepsis would be helpful, as there is a therapeutic intervention that may be helpful. Furthermore, understanding the current practice pattern of statins in these patients is essential to improve compliance. Anecdotally, there is suboptimal assessment of appropriate background risk and medications in patients admitted to the hospital, although this has not been systematically explored in this specific cohort.
Materials and Methods
This was a retrospective cohort analysis performed at a single, university tertiary care center. The study was preapproved by the Institutional Review Board. Three hundred twenty-one patients who were admitted to the University of Kentucky HealthCare from January 1, 2013, to December 31, 2013, were screened for all inclusion and exclusion criteria. Portions of this cohort have been analyzed for other aspects of cardiovascular risk assessment after sepsis, but not specifically looking at statin indications or practice patterns. 10
Patients
All patients had to be 18 years or older and have either suspected or confirmed sepsis with biochemical evidence of myocardial injury defined as detectable troponin levels (>0.015 ng/dL). The 2012 Surviving Sepsis guidelines were used for defining patients with sepsis as this was used clinically at this time. Patients were screened if they had at least 2 systemic inflammatory response syndrome (SIRS) criteria with a confirmed or presumed source of infection. 11 Given the lack of specificity of the SIRS criteria, patients who met this initial criteria also had to have a confirmed pathogen or a presumed organ system involved if no pathogen was identified. This cohort was identified from the institutions’ electronic data repository and by reviewing the electronic health record of individual patients when confirmatory data was needed. Variables for the Acute Physiology and Chronic Health Evaluation II (APACHE II) score were used as a part of previous reporting and were used as an additional inclusion criteria if the majority of variables were present.
All patients with an acute coronary syndrome, percutaneous coronary intervention (PCI), structural heart intervention or electrophysiologic procedure within 7 days, and cardiac surgery within 30 days were excluded. Patients with no data available on statin use were also excluded. Patient inclusion and exclusion are summarized in Figure 1.

STROBE patient flow diagram.
Statin Indicated Groups
During the study period, the Adult Treatment Panel III (ATP III) guidelines were the primary clinical guidelines for lipid management in at-risk patients. 6 By the end of the study period and at the time of manuscript preparation, the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guidelines were used most frequently for treatment of blood cholesterol. 7 Thus, statin indicated groups were defined based on common indications between the ATP III and the 2013 ACC/AHA guidelines. Specifically, patients with established cardiovascular disease including cerebrovascular accidents and peripheral arterial disease, patients with diabetes mellitus, and those with established diagnosis of hyperlipidemia were included in the statin benefit group. If they failed to meet any of these criteria they were deemed to not be in a statin indicated group. Those in multiple statin indicated groups were counted only once for this analysis. This decidedly conservative approach was taken to ensure that the primary and secondary end points were accurately assessed and not contaminated by patients who may not benefit from statin therapy.
Outcomes
The primary outcome was MACE rates stratified by statin indication. Major adverse cardiovascular event was defined as a composite of cardiovascular death, acute myocardial infarction (MI), or PCI at 1 year. Cardiovascular death was defined as cardiogenic shock as a primary or major secondary contributor to mortality or a fatal ventricular arrhythmia. Acute MIs were identified using the Third Universal Definition of Acute Myocardial Infarction. 12 Percutaneous coronary interventions were identified through a review of the catheterization laboratory database at our institution. All outcomes were identified by reviewing the electronic medical record. All end points were preliminarily reviewed by multiple team members, and finally adjudicated by a board-certified cardiologist (V.A.G.).
The secondary outcome was identification of the number of patients who were in at least one statin indicated group but were not prescribed a statin at discharge. The discharge prescribing practice was further stratified based on whether they were prescribed a statin medication on admission. This was determined through the review of the electronic medical record looking at admission paperwork, specific medication reconciliation done by the pharmacists often after calling a patient’s primary pharmacy, as well as discharge documentation (discharge instructions, medication reconciliation, and discharge instructions).
Statistical Analysis
Given no previous data on the association of different statin indications and MACE, a true sample size calculation could not be performed. However, assuming a confidence level of 95%, a power of 80%, and a MACE rate of 5% in the group with no statin indication (overall MACE rate in our previous study on patients with sepsis), 10 a sample size of 300 patients should be able to detect an absolute difference in MACE rates of >5% between groups. All continuous variables are reported as mean and standard deviations for normally distributed variables and median with interquartile ranges for non-normal distributions. Categorical variables are reported as percentages. Pearson χ2 analysis was used to assess an association between statin benefit groups with MACE was assessed using χ2. Finally, a McNemar test was performed to assess the association of discharge statin prescription with admission statin medication. All statistical analysis was done using SPSS version 26 (IBM). A P value of <.05 was used for significance.
Results
Three hundred twenty-one patients were screened, of whom 296 patients met the initial inclusion and exclusion criteria for the study; 32 additional patients were excluded due to missing data on statin use prior to hospitalization or upon discharge. The remaining 264 patients were included in the analysis. Full patient flow can be seen in Figure 1.
Baseline Demographics
Baseline demographic data of our cohort is illustrated in Tables 1 and 2. Of the 264 patients included in the analysis, 141 (53%) were male and 243 (91%) were Caucasian. The mean age of our cohort group was 59 ± 15 years. This was a critically ill population with a mean APACHE II score of 16.8 ± 6.0. In the validation studies, this APACHE II score was associated with an ∼25% inhospital mortality. 13 Consistent with this severity of illness, 172 of the 264 patients (65%) required vasopressors at some point during their hospitalization and necessitated intensive care unit (ICU) admission.
Differences Between the ATP III and 2013 ACC/AHA Guideline Recommendations for Statin Prescribing.

Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; ATP III, Adult Treatment Panel III; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MI, myocardial infarction; PAD, peripheral arterial disease.
a CHD equivalent: diabetes, symptomatic coronary artery disease, peripheral arterial disease.
b Risk factors include: HDL < 40 mg/dL, hypertension or on antihypertensive medication, smoking, family history of premature coronary heart disease, male ≥ 45 years, female ≥ 55 years.
Baseline Demographics.

Abbreviations: ACE, angiotensin converting enzyme; APACHE II, Acute Physiology and Chronic Health Evaluation II; ARB, angiotensin receptor blocker.
Of note, there were 75 patients with known coronary artery disease (CAD, 28%), 100 patients with diabetes mellitus (37%), 95 patients with hyperlipidemia (36%), and 11 patients with a prior cerebrovascular accident (4%).
Outcomes
Primary outcome
In the overall cohort of 264 patients, 24 (9%) patients experienced a MACE. However, the MACE rate was substantially higher among patients in a statin indicated group versus patients who were not in a statin indicated group (12.2% vs 3.2%, χ2 value of 5.8, P = .016). The patients in a statin indicated group were older, but otherwise did not have significant differences in severity of illness (by APACHE II score), gender, peak troponin values, or rates of acute kidney injury. The majority of MACE in both groups happened during their index hospitalization and many of these patients did not survive this admission (11 patients in the statin indicated group and 2 patients in the nostatin indicated group). Of those who were discharged alive, 10 patients in a statin indicated group experienced a MACE in the subsequent 1 year. Those with a history of clinical atherosclerotic cardiovascular disease had the highest incidence of MACE (25%) followed by those with multiple indications (14%). By contrast, only 1 additional patient in the nostatin indicated group experienced a MACE in the subsequent 1 year. The overall summary of the primary outcome is seen in Figure 2.
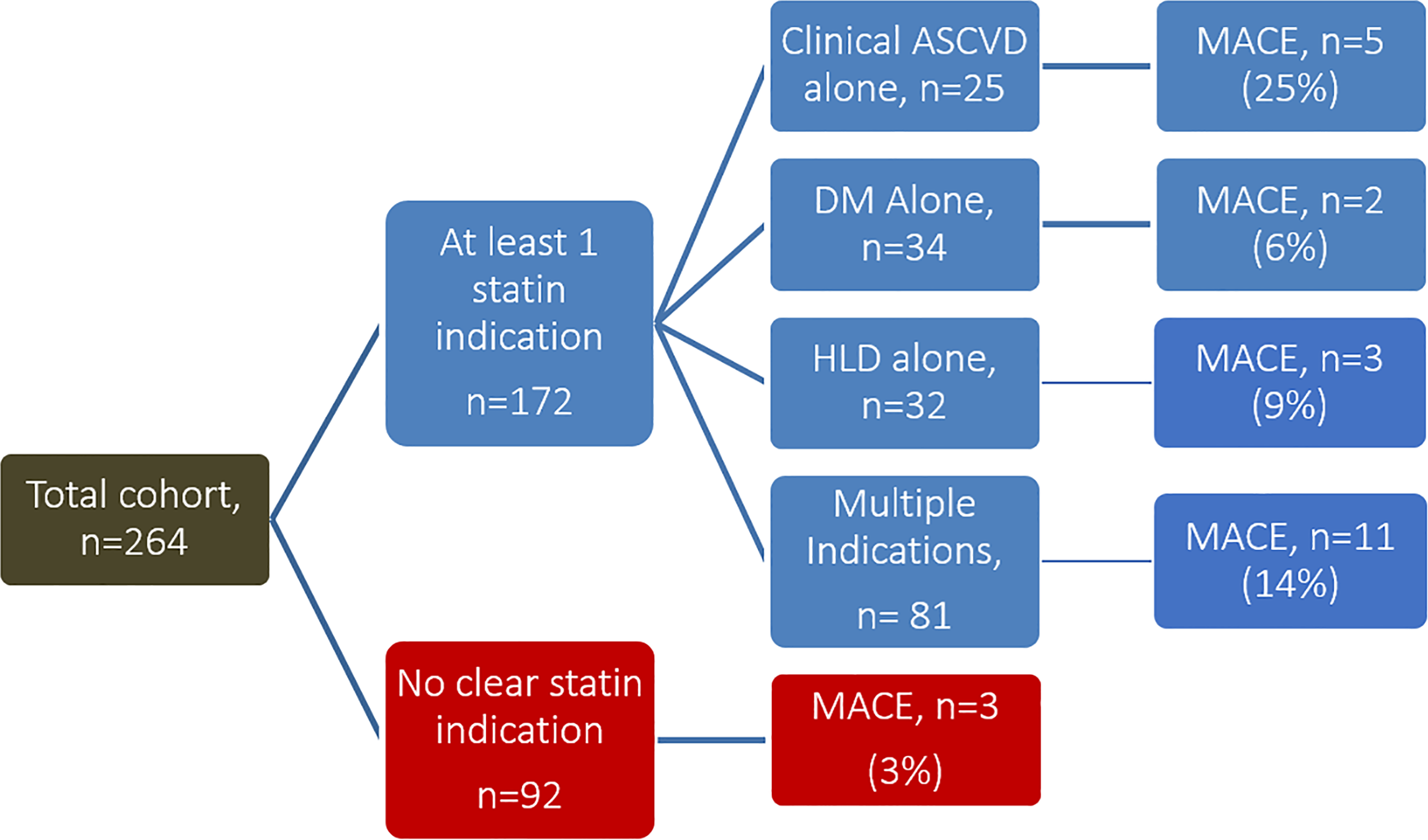
Distribution of patients with major adverse cardiovascular event (MACE) rates according to statin indication.
Statins were frequently prescribed during patients’ hospitalization. Of this cohort, 105 patients were prescribed a statin during their hospitalization. The majority of these patients (n = 82) were on a statin prior to admission. Of the 33 patients only started on a statin during the hospitalization, only 6 were discharged alive on a statin, while 12 were discharged alive not on a statin and 15 patients died during their hospitalization.
Secondary outcome
On admission, 172 patients were in at least 1 statin indicated group with 123 of these patients surviving to hospital discharge. Sixty (49%) of these 123 patients were discharged on a statin while 63 (51%) such patients were not discharged on a statin. There was a significant difference in discharge statin prescription based on whether they were on a statin prior to admission. Only 10% of the patients (6 of 62) not on a statin on admission received a statin on discharge, whereas 89% of the patients (54 of 61) on a statin on admission received a statin on discharge (Figure 3). Admission statin prescription status was significantly associated with discharge statin prescription.

Distribution of statin prescribing on discharge in the statin indicated group based on admission statin prescription.
Discussion
There are several notable findings from this analysis: the risk of adverse outcomes is disproportionate in those who have guideline indications for statin therapy, there is potential for significant improvement in identification of at risk patients, and there is significant clinical inertia seen in medication prescribing patterns.
There is increasing data that suggests that cardiovascular risk increases with sepsis, and cardiovascular prevention strategies should be considered in the spectrum of sepsis management. Major adverse cardiovascular event rates in this cohort was 9% (n = 265) in the first-year postdischarge. This overall rate is similar to the annualized risk of MACE in obstructive CAD, or high-risk stress tests. 14 More importantly, the risk of MACE is 3 to 4 fold higher in those with a guideline indication for statin therapy as opposed to those who do not. With the proven efficacy of statin therapy in reducing MACE in these cohorts beyond sepsis, the addition of guideline-directed medical therapy has the theoretic potential to reduce the risk of MACE substantially, affecting millions of patients worldwide.
Despite the overall increase in MACE rates after sepsis in statin indicated groups, the event rates are all less than or equal to 25% among the different subgroups, and 12.2% in the statin indicated groups overall. While initiating guideline-directed therapy should be considered for all of these cohorts, additional guidance is likely needed to better identify septic patients at risk. To better understand a more personalized strategy, more data are needed in terms of the major driver of events and the prognostic performance of other clinical, laboratory, and imaging findings.
The other significant finding in this study was the significant clinical inertia in this patient population. Only 10% of patients not on a statin on admission and falling into a statin indicated group were discharged on a statin, while 89% of those admitted on a statin were discharged on a statin. This suggests that one of the biggest predictors of discharge medication reconciliation is admission medication reconciliation regardless of baseline risk or medication indication. This analysis is more a reflection of statin prescribing practices broadly, and not specifically a reflection of a specific guideline document. The ATP III guidelines defined the same at risk subgroups as those identified within the 2013 ACC/AHA guideline documented with some additional focus on low-density lipoprotein levels. Given the overlap, the lack of routine lipid assessment in this cohort of hospitalized patients, and the lack of data on statin prescribing practices for acutely hospitalized patients, this preliminary assessment raises the question about barriers to reassessing guideline-directed baseline medical therapy in hospitalized patients.
This concept of clinical inertia in medication prescribing practices has been proposed previously in different clinical scenarios, but not in statin prescribing specifically. 15,16 Clinical inertia is defined as lack of initiation, intensification, or de-escalation of treatment in patients not currently at evidence-based goals of care. Previous data has shown similar suboptimal prescribing of statins in patients with established CAD or other risk factors. Registry data show that while over 80% of patients are prescribed a statin following an MI or coronary revascularization, only about a third of these patients filled a high-intensity statin prescription. 17 -19 In a study from Medicare beneficiaries, high-intensity statin therapy was being used in 35% of patients within 1 year of cardiovascular event. 20 This data however reflected practice prior to the publication of the 2013 AHA/ACC cholesterol guidelines and prior to atorvastatin becoming generic. In fact, data from 2011 to 2014 of a commercial insurance database demonstrated increased prescription of high-intensity statins following MI’s. Despite this favorable trend, a significant proportion of post MI patients were still being discharged on low and medium intensity statins. 21 More recently, data from the Patient and Provider Assessment of Lipid Management (PALM) registry revealed underutilization and underdosing of patients meeting statin indications based on the 2013 ACC/AHA guidelines. 22 While there is some literature on overcoming clinical inertia in other areas (specifically in diabetes) largely utilizing, there is limited data in statin utilization. 23
There are many potential explanations for the observed underutilization of statin therapy at discharge. Some hospital providers are reluctant to initiate primary prevention medication as they are often not responsible for following up with the patient after discharge. Adverse medication side effects are common post discharge but are largely preventable and ameliorable with appropriate patient education and appropriate follow-up. 24 This concern about side effects was associated with actual prescribing practices in the PALM registry and was highest among those primarily responsible for primary prevention indications for statins. 25 This concerns is likely augmented in critically ill patients with sepsis, where ICU myopathy and steroid myopathy are potential concerns. Interestingly, the lack of continuity of care can deter certain clinicians from prescribing primary prevention statin therapy prior to discharge. Another reason could be the focus on the acute presenting illness and secondary prevention of disease while deferring primary prevention therapy to the primary care provider after discharge. This study suggests that clinical inertia in prescribing practices is an important consideration as well. Strategies that create individualized treatment plans that continuously reassess indications for therapy, leverage electronic health record and clinical decision support capabilities, and/or pharmacists driven process have been shown to be effective in improving statin adherence. 26,27
This study has several limitations. Due to the nature of the study design, it is subject to the inherent limitations of a single-center retrospective analysis including accuracy of documented information within the electronic medical record, the tracking of follow-up data, and applicability to other patient populations. There was a high mortality and the many of the MACE events happened in the index hospitalization, and limits the interpretation of outpatient risk. There was no information about liver function tests at discharge or reasons why statins were not prescribed to eligible patients. Additionally, we do not have access to pharmacy prescription data to assess how many of statin eligible patients were prescribed these medications after discharge by their primary physicians. Finally, the data were analyzed when a major shift in statin prescribing was occurring with the publication of the 2013 ACC/AHA statin guidelines.
Conclusion
Major adverse cardiovascular event rates are high after sepsis, especially among cohorts that traditionally fall in statin-indicated groups. While the overall risk is increased in these specific cohorts, statin prescribing is highly variable and clinical inertia seems to play a significant role in prescribing patterns. Every hospital encounter with an at-risk population group is a distinct opportunity for improving and optimizing guideline-directed medical therapy. A systematic approach to identify and follow-up on high risk patients is essential to optimize medical therapy for primary and secondary prevention of cardiovascular events.
Footnotes
Authors’ Note
Research was conducted at the University of Kentucky, Lexington, Kentucky.
Author Contributions
VG was responsible for conceptualization, investigation, data curation, validation, formal analysis, writing (original draft, review and editing). TA and SS were responsible for investigation, writing (original draft, review and editing). SL was responsible for conceptualization, data curation, writing (review and editing), and supervision. VS was responsible for conceptualization, writing (review and editing) and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [5T32HL091812-07, 2015-2016].