
Abstract
Introduction:
Direct comparison of the effects of antiarrhythmic agents on myocardial performance may be useful in choosing between medications in critically ill patients. Studies directly comparing multiple antiarrhythmic medications are lacking. The use of an experimental heart preparation permits examination of myocardial performance under constant loading conditions.
Methods:
Hearts of Sprague Dawley rats (n = 35, 402-507 g) were explanted and cannulated in working heart model with fixed preload and afterload. Each heart was then exposed to a 3-hour infusion of procainamide (20 µg/kg/min), esmolol (100 or 200 µg/kg/min), amiodarone (10 or 20 mg/kg/d), sotalol (80 mg/m2/d), or placebo infusions (n = 5 per dose). Cardiac output, contractility (dP/dTmax), diastolic performance (dP/dTmin), and heart rate were compared between groups over time by linear mixed modeling.
Results:
Compared with placebo, sotalol decreased contractility by an average of 24% (P < .001) over the infusion period, as did amiodarone (low dose by 13%, P = .029; high dose by 14%, P = .013). Compared with placebo, mean cardiac output was significantly lower in animals treated with sotalol (by 22%, P = .016) and esmolol 200 μg/kg/min (by 23%, P = .012). Over time, amiodarone decreased cardiac output (20 mg/kg/d, β = −89 [−144, −33] μL/min2 decrease, P = .002) and also worsened diastolic function, decreasing dP/dTmin by ∼18% and 22% (P = .032 and P = .011, low and high doses, respectively). Procainamide did not have a significant effect on any measures of systolic or diastolic performance.
Conclusions:
In isolated hearts, amiodarone and sotalol depressed myocardial contractility, cardiac output, and diastolic function. However, procainamide did not negatively affect myocardial performance and represents a favorable agent in settings of therapeutic equivalence.
Introduction
Antiarrhythmic agents are commonly used in the care of critically ill patients, including those with primary arrhythmias or following cardiac surgery. Many patients with arrhythmia also exhibit diminished cardiac function, making it important to quantify the direct effect of these agents on myocardial performance. Most arrhythmias may be variably treated by a number of different agents. The choice of agent may be guided not only by its rhythm-specific efficacy but also by its adverse effects, including their effects on the circulation. Few studies provide head-to-head comparisons of these effects in 1 or 2 drugs, either in animals or in humans. 1 However, such in vivo studies are unable to provide information about the direct myocardial depressant actions of each drug due to their mixed effects on cardiac function and vascular tone. Thus, the recommendations of consensus statements 2,3 and guidelines, 4 and the choice of agent at the bedside, are based on inferences of many studies with heterogeneous study designs, inclusion criteria, and measured end points. 5,6 The purpose of this study was to provide, for the first time, a direct head-to-head comparison of many commonly used antiarrhythmic agents on myocardial function absent their vascular effects (ie, under constant loading conditions).
The primary cellular target of most antiarrhythmic agents is one or more ion channels on the surface of cardiac myocytes. These agents control arrhythmia through multiple effects, including decreasing automaticity and triggering events, altering refractory periods, and slowing conduction. Antiarrhythmic agents are classified based on the channels they antagonize with the relatively simple Vaughn Williams classification: class I (which target the sodium channel), class II (which target the β receptor), class III agents (which target the potassium channels), and class IV agents (which target the calcium channel). In contrast to inotropic agents, which increase contractility by stimulating β receptors, antiarrhythmic agents may exert negative inotropic effects by blocking β activity, introducing the potential of worsening a tenuous hemodynamic state. 7 -9 The relative impact of bolus dosing some antiarrhythmic agents on myocardial performance measures has been previously quantified, with decreases in contractility and cardiac output a consistent finding during drug loading. 9
In order to better inform the choice of antiarrhythmic agent at the bedside, we compared the direct myocardial effects of continuous infusions (without loading) of commonly used intravenous antiarrhythmic agents, including procainamide (IA), esmolol (II), and amiodarone (III), on contractility, diastolic performance, and cardiac output in an experimental construct. Because agents may have distinct effects on each myocardial and vascular function, we used an experimental construct that maintained a constant preload and afterload. We hypothesized that amiodarone would have the most profound effect on measures of contractility and cardiac output given the multiplicity of its actions on myocytes.
Materials and Methods
Animal Preparation
The following protocol was approved by the Institutional Animal Care and Use Committee at Boston Children’s Hospital. Sprague Dawley rats (n = 35, 402-507 g) were housed in the Animal Resources at Children’s Hospital with a 12-hour:12-hour day–night cycle and with free access to food and water until the date of experimentation. Animals were anesthetized with inhalational isoflurane (1.5%-2.5%) and anticoagulated (heparin 100 U/100 g intraperitoneally). The heart and lungs were explanted en bloc and immediately placed in ice cold modified Krebs Henseleit buffer (KHB) as previously described. 10,11 The aorta was then cannulated and retrograde-perfused using a perfusion pressure of 90 mm Hg (Harvard Apparatus, Holliston, Massachusetts IH51-B). The pulmonary veins were isolated and ligated bilaterally, and the left atrium was cannulated for the provision of preload KHB, as was the pulmonary artery for the collection of coronary effluent. A pressure–volume conductance catheter (SPR-944; Millar Instruments, Houston, Texas) was inserted into the left ventricle retrograde through the aortic valve. The heart was then transitioned into working heart model with a fixed left atrial pressure of 10 mm Hg and fixed mean aortic pressure of 90 mm Hg. All perfusates passed through a 0.22-μm filter prior to entering the heart.
Treatment Groups
Following a 30-minute period of baseline observation, hearts were exposed in random order (by randomization table) to a continuous infusion of one of the following drug–dose combinations for a 3-hour period: procainamide (20 μg/kg/min), esmolol (100 or 200 μg/kg/min), amiodarone (10 or 20 mg/kg/d), sotalol (80 mg/m2/d), or placebo (KHB infused at a similar infusion rate; n = 5 per drug/dose). Dosing of all drugs was chosen to represent early maintenance dosing according to our institution’s current practice (not accounting for the effects of protein binding, which was absent in our model), including the per day dosing of amiodarone and sotalol. All dosages were based on measured whole body weight or body surface area. No animals were excluded from analysis.
Measurements
We calculated maximum rate of pressure rise (dP/dtmax, mm Hg/s) and cardiac output (μL/min, determined from conductance data) from the pressure–volume curve as measures of systolic function. Diastolic performance was assessed based on the maximum rate of pressure fall (dP/dTmin, mm Hg/s) and the isovolumic relaxation constant (τ, milliseconds, determined by the curve fit of the isovolemic pressure–volume curve). Heart rate (bpm) was assessed from the ventricular pressure tracing. Coronary vascular resistance was calculated as follows: (diastolic aortic root pressure − mean right atrial pressure)/coronary flow rate. Coronary flow rate was quantified each 5 minutes using timed collections in a graduated cylinder.
Signals were sampled by a conductance system (MPVS Ultra; Millar Instruments) and recorded and analyzed in LabChart 8 Pro software (PowerLab 16/35; AD Instruments, Houston, Texas). Raw data were recorded at a frequency of 1 kHz. The median value for each minute of data collected was calculated using the DataPad function within the software.
As we have previously described, 11 we chose to infuse set doses (ie, 100 μg/kg/min) of medication from a syringe into the KHB perfusing the left atrial block (whose flow rate was equivalent to the cardiac output); in many other models, the left atrial block is perfused with KHB containing a set concentration of a given agent. We chose to deliver the infusions in this manner to make the analyses more applicable to clinical practice. To permit comparisons to serum concentrations, we calculated an estimated drug concentration within coronary perfusate for each minute of perfusion as follows: administered dose (eg, 100 μg/kg/min) × animal body weight × 1 minute divided by measured cardiac output over the same period.
Statistical Methods
For each condition (ie, drug–dose combination), the value of each end point (1-minute medians) was compared to the control group over time using linear mixed modeling (LMM; IBM SPSS Statistics for Windows, version 22.0, Armonk, New York), adjusting for any differences in the baseline period. To account for multiple comparisons within the LMM, we adopted the Bonferroni correction, using an α value of .05. Further, slope coefficients (represented as β value) were calculated from the LMM for each drug dose and variable tested to quantify the effect of the drug on the outcome of interest, with calculation of standard error of the mean and 95% of confidence interval and using an α value of .05.
Results
Agent Concentrations
The calculated concentrations of each dose of drug are listed in Table 1. The concentration of drugs tested at more than one concentration increased with increasing doses. However, medications that caused more significant decreases in cardiac output (eg, amiodarone) were present in relatively higher concentrations as the higher drug infusion rate was diluted in a relatively lower volume.
Calculated Drug Concentrations in Coronary Perfusate.a
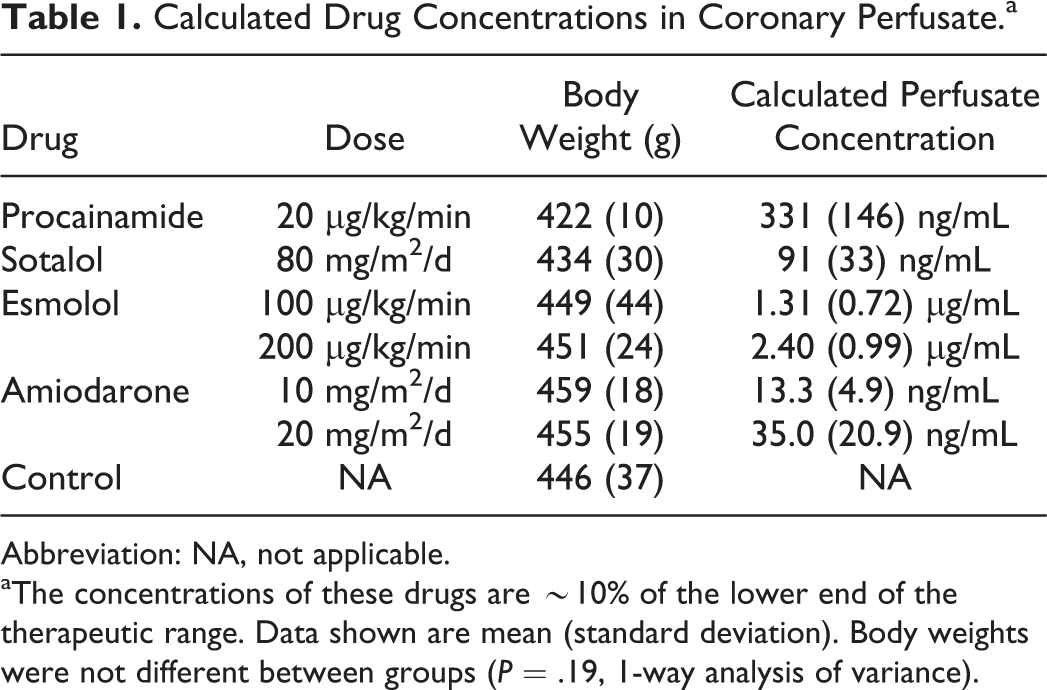
Abbreviation: NA, not applicable.
aThe concentrations of these drugs are ∼10% of the lower end of the therapeutic range. Data shown are mean (standard deviation). Body weights were not different between groups (P = .19, 1-way analysis of variance).
Systolic Function
As depicted on a pressure–volume loop (Figure 1), exposure to amiodarone (and other agents) had a significant effect on contractility. Compared with placebo controls, dP/dTmax decreased more rapidly over time in animals exposed to sotalol (β = −5.3 [−9.4, −1.1], P = .014) and amiodarone 10 mg/kg/d (β = −4.7 [−4.7, 2.1], P = .032) or 20 mg/kg/d (β = −12.2 [−16.2, −8.1], P < .001; Figure 2A). Compared with placebo, sotalol decreased contractility by an average of 24% (P < .001) over the infusion period, as did amiodarone (low dose by 13%, P = .029; high dose by 14%, P = .013). Additionally, exposure to esmolol 200 μg/kg/min resulted in a lower average dP/dTmax during the infusion period (P = .043; Figure 2B). Neither esmolol 100 μg/kg/min nor procainamide had a significant impact on contractility under these conditions.
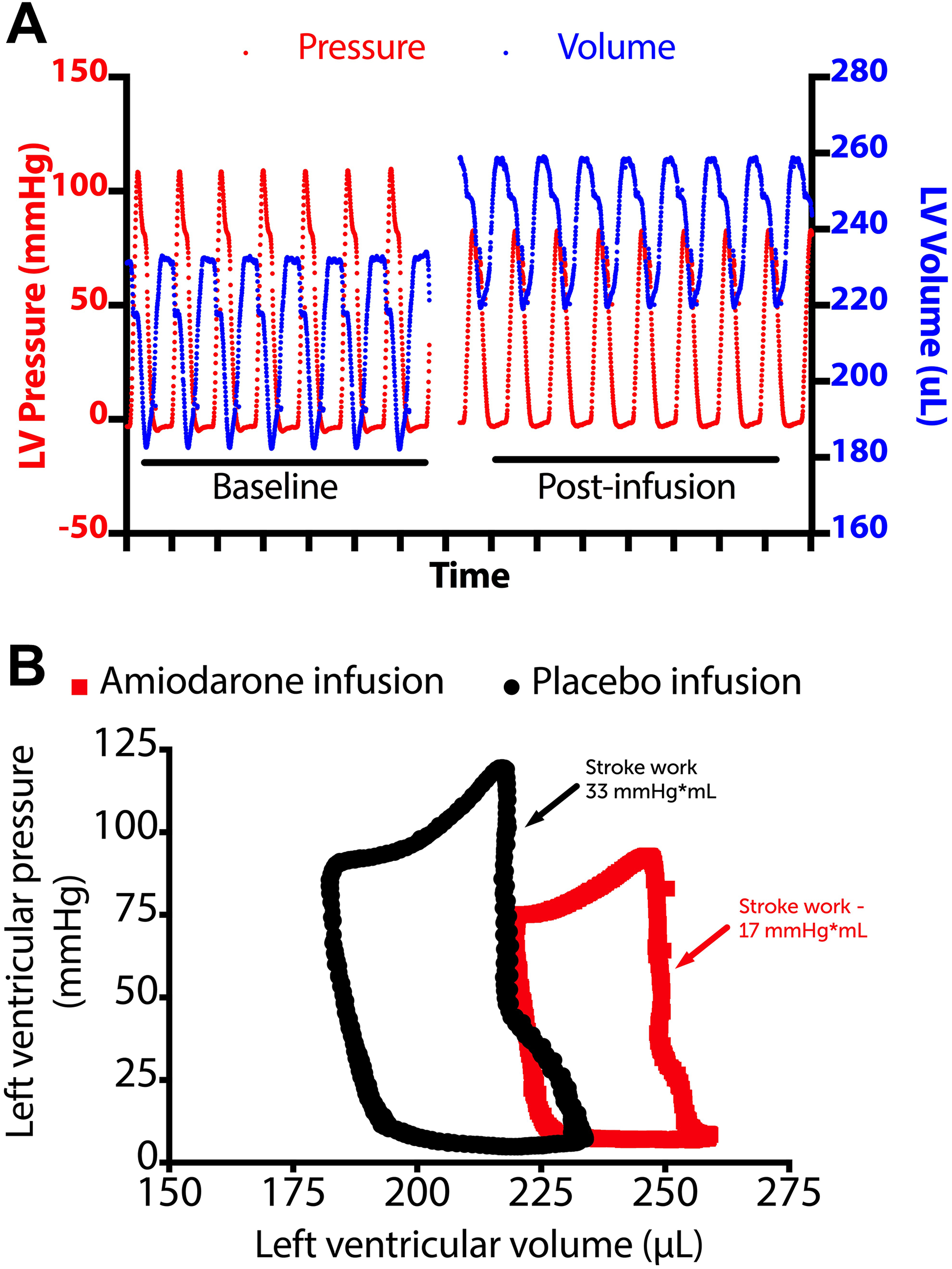
A, Representative left ventricular (LV) pressure and volume tracings of a rodent heart prior to (left) and following (right) a 3-hour infusion of amiodarone. Note the increase in end-diastolic volume and pressure following the infusion. B, The LV pressure volume relationship of 2 rodent hearts following a 3-hour infusion of amiodarone (20 mg/kg/d, red) or placebo (Krebs buffer, black) into the left atrial block under constant loading conditions. Stroke volume and stroke work (quantified as area within the curve) were lower following infusion of amiodarone than placebo.

Effects of antiarrhythmic agents on contractility. A, Compared with the placebo group, the maximum rate of pressure rise (dP/dTmax, a measure of contractility) decreased more rapidly over time (depicted by the slope of the line) in animals treated with sotalol (P = .014) and amiodarone 10 mg/kg/d (P = .032) or 20 mg/kg/d (P < .001). Black line represents the mean change from baseline in dP/dTmax over time for the placebo control group, shading represents standard error of the mean (SEM). Data points represent 1-minute mean for each time point, dark line is LOWESS curve of the mean. B, Examined another way, the mean change in contractility during the infusion period was significantly lower in animals exposed to sotalol, esmolol 200 μg/kg/min, and both doses of amiodarone. P Values as shown based on linear mixed modeling with adjustment for baseline differences and compared with the placebo control group.
Compared with placebo control hearts, the mean cardiac output during the infusion period was significantly lower in animals treated with sotalol (mean of 22% lower than the control group, P = .016) and esmolol 200 μg/kg/min (mean 23% lower than the control group, P = .012), but not with procainamide (Figure 3A). Further, the rate of decline in cardiac output was significantly higher in hearts exposed to amiodarone (20 mg/kg/d, β = −89 [−144, −33] μL/min2 decrease, P = .002) and sotalol (β = −73 [−129, −18] μL/min2 decrease, P = .011). The magnitude of heart rate change was <5% for all drug–dose combinations tested, none of which reached statistical significance (Figure 3B).

Effects of antiarrhythmics on cardiac output and heart rate. A, Mean change in cardiac output during the infusion period was significantly lower in animals exposed to sotalol and high-dose esmolol compared to the placebo control group. Difference in mean cardiac output during the infusion period was not significantly different in hearts exposed to amiodarone and the control group. P Values as shown based on linear mixed modeling with adjustment for baseline differences and compared with the placebo control group.
Diastolic Function
Both doses of amiodarone worsened diastolic function, decreasing dP/dTmin (ie, less negative) compared to time-matched controls (10 mg/kg/d, by ∼19% compared to controls, P = .032 and at 20 mg/kg/d by 23% compared to controls, P = .011; Figure 4A). Additionally, the rate of decline in dP/dTmin (ie, becoming less negative) was significantly higher (ie, worse) in hearts exposed to sotalol (β = 9.8 [3.9, 15.9] mm Hg/s/min exposure, P = .002 relative to control) and either dose of amiodarone (10 mg/kg/d, β = 8.5 [2.7, 14.3] mm Hg/s/min exposure, P = .005 relative to control; 20 mg/kg/d, β = 21.8 [15.9, 27.7] mm Hg/s/min exposure, P < .001 relative to control). The left ventricular time constant, τ, exhibited significant variance between groups but was not significantly different for any of the dose–drug combinations tested (Figure 4B).

Effects of antiarrhythmics on diastolic function and coronary vascular resistance. A, The decrease diastolic function (as measured by dP/dTmin, the maximum rate of diastolic pressure fall) was more significant in hearts exposed to amiodarone than in the control group. B, τ, the isovolemic relaxation constant, was similar between all groups. C, Hearts exposed to high-dose amiodarone exhibited a significant decrease in coronary vascular resistance, expressed here as a percentage change from baseline. P Values as shown based on linear mixed modeling with adjustment for baseline differences and compared with the placebo control group.
Coronary Vascular Resistance
Exposure to high-dose amiodarone decreased coronary vascular resistance compared to controls (P = .038; Figure 4C). No other drug–dose combinations exhibited a measureable effect on coronary vascular resistance.
Discussion
In the management of arrhythmia, several agents may be equivalently effective. The choice between them is often based on the competing efficacy and risk profiles of each. To our knowledge, no prior study has compared multiple antiarrhythmic drugs head-to-head using a consistent preparation and stringently measured end points. We believe that our work may help to explain differences noted in past and future studies by providing a comparison of drug effects on the myocardium itself by holding loading conditions constant. We found that among the intravenous antiarrhythmic agents tested, sotalol and amiodarone significantly decreased contractility compared to controls and sotalol and high-dose amiodarone also significantly decreased cardiac output. In general, antiarrhythmic medications impaired diastolic function, except for procainamide and high-dose esmolol. Procainamide had no significant effect on any measures of myocardial performance.
Hemodynamic Effects of Amiodarone
In our series, high-dose amiodarone had a consistently negative inotropic and negative lusitropic effect compared to commonly used doses of alternative antiarrhythmic agents. Prior reports have been consistent in describing a reduction in dP/dTmax, cardiac output, and dP/dTmin during acute loading (5 mg/kg) of amiodarone in intact animals. 12,13 These same findings—an approximately 15% to 20% reduction in contractility and cardiac output—have also been reported during acute loading doses of amiodarone in patients, with or without underlying ventricular dysfunction. 14 Our data add to this by describing that an infusion of the drug may result in a similar degree of dose-related myocardial depression. Because the biodistribution of amiodarone is widely variable (apparent volume of distribution between 1 and 148 L/kg 15 ), the behavior of an amiodarone infusion in vivo would also be expected to be widely variable. Our model simplifies this problem by establishing a known volume of distribution (ie, the myocardium and KHB perfusate), creating a consistent, non-protein-bound “plasma” level of the drug, which in this case can be calculated to be ∼40 ng/mL, ∼5% of the maximum concentration expected following an intravenous loading dose of 5 mg/kg. 16
In a clinical situation, the vasodilatory properties of the drug are likely to also be an important factor with variable effects. In some patients, such as those with afterload-sensitive systolic dysfunction, a reduction in systemic vascular resistance may somewhat offset the direct negative inotropic effect of the drug, a phenomenon which has been described in animals with and without ventricular dysfunction. 13,14 Alternatively, in patients with preload-sensitive diastolic dysfunction, venodilation may reduce preload and further reduce cardiac output. This phenomenon may be exacerbated by amiodarone’s effect on diastolic excursion; the negative impact of amiodarone on the maximum rate of diastolic pressure fall shown here is consistent with that described in other experimental preparations. 12 This combination of negative inotropy, impaired diastolic function, and vasodilation may explain the relatively common occurrence of hypotension 17 and rare instances of cardiovascular collapse upon administration of amiodarone in clinical use. 18 Our work shows that even when cardiac factors are isolated from vascular effects, an infusion of amiodarone exhibits a negative inotropic and lusitropic effect. Understanding whether a clinical finding of hypotension, for example, results from intrinsic cardiac effects versus vascular effects of an antiarrhythmic is critical to the appropriate management of such a side effect. Further, amiodarone was the only drug that demonstrated coronary vasodilatory properties, affecting a decrease in coronary vascular resistance at high-dose exposure. The systemic vasodilatory properties of amiodarone are well known, with acute loading doses of amiodarone decreasing systemic vascular resistance and improving coronary blood flow by ∼15%. 7,14 This property is commonly thought to be related to the solvent in which amiodarone is commonly prepared (polysorbate or “Tween” 80). 19 Of note, there is a newly marketed formulation of amiodarone that uses a cyclodextrin carrier, which was not evaluated in this study. 20
Hemodynamic Effects of Sotalol
There are 2 forms of sotalol described in the literature: racemic sotalol, used here, which has an enantiomeric ratio of 1:1
When compared head-to-head, racemic sotalol has shown a similar negative inotropic effect to amiodarone, presumably related to its β-blocking activity. 13 Since that time, the use of oral racemic sotalol has been described safe for use in infants 24 and children. 25,26 This drug is theoretically attractive due to the absence of long-term toxicities (such as the thyroid and pulmonary toxicities present with amiodarone) and its availability in both oral and intravenous form. In our model, racemic sotalol decreased contractility and cardiac output to an extent comparable to intravenous amiodarone. However, it has recently been described that intravenous racemic sotalol (though sourced from a different manufacturer than ours) can be safely used in children with tachyarrhythmias without the propagation of hypotension. 27 Although we found the negative inotropic effects to be comparable to those of amiodarone, the clinical safety profile of sotalol may be enhanced over that of amiodarone because of the lack of vasodilation, a seemingly prominent feature of intravenous amiodarone. A multicenter registry investigating the use of the new formulation of intravenous racemic sotalol in the pediatric population is currently underway in the United States.
Hemodynamic Effects of Esmolol
Esmolol is an ultra-short-acting β receptor antagonist with a terminal elimination half-life of ∼7 minutes. 28 It is commonly used to reverse hypertension or induce hypotension in the operative and perioperative settings. 29 -32 In these settings, esmolol has accrued a favorable safety profile, largely owing to its rapid titratability. As prior studies have shown, 33 we found that esmolol significantly decreased contractility and cardiac output in our model, with a relative sparing of diastolic function. This combination—a decreased inotropic effect with a sparing of diastolic function—may favorably affect patients with heart failure, particularly those with ischemic heart disease, in whom β-blocker therapy improves echocardiographic measures of diastolic function, including mitral valve E-wave velocity and E/A ratio. 34 The short-acting kinetics of this agent have led to its increased use in neonates over the past several decades. 35
Hemodynamic Effects of Procainamide
Among the agents tested, procainamide exhibited the most benign effects, with all measures of myocardial performance being similar to the control group, including contractility, cardiac output, diastolic function, and coronary vascular resistance. Our findings are consistent with similar studies in isolated feline papillary muscle preparations 36,37 and rodent hearts, 38 which have suggested a weak positive inotropic effect. Several clinical studies have also suggested that administration of procainamide in patients with ischemic heart disease has either a positive 39 or negligible effect on fractional shortening. 40 Infusion of N-acetylprocainamide, an active metabolite of procainamide, results in a weak vasodilatory effect, mild increase in ejection fraction, and mild reduction in cardiac index even at plasma levels above what is currently considered the therapeutic range. 41 In addition to its favorable safety profile, procainamide has been shown to be superior to amiodarone in achieving control of supraventricular tachycardia 42 and ∼80% effective when used in combination with hypothermia for control of postoperative junctional tachycardia. 43 Given its favorable clinical profile, as well as its comparatively mild effects on inotropic state, procainamide remains a favored first-line agent for the treatment of many tachycardias at our institution.
Limitations
There are several important limitations to this work. First, though this model allows for the examination of direct myocardial effects of antiarrhythmic medications under controlled preload and afterload, in practice the vasoactive effects of these drugs are quite important. However, the intent of this work was to describe the direct myocardial effects of each drug under constant loading conditions. Second, this model tested explanted hearts devoid of parasympathetic innervation, although the Langendorff method has been widely used to study the hemodynamic effects of drugs. 10,33,36 Thus, drug effects may differ somewhat in vivo. Third, our model tested a defined mass of drug infused per unit time, a mass that was diluted in a variable cardiac output. Because cardiac output varied within a narrow range, drug concentrations were relatively constant and did not accumulate over time since perfusate was not recirculated. We chose this construct to emulate the clinical use of these medications, permitting comparisons between commonly used doses and drugs. In this construct, the calculated concentration of medications was ∼10% than the expected serum concentrations for the drugs described. Because inotropic effects may vary in either direction with increasing concentrations of some drugs, it is possible that the inotropic effects of these drugs may differ in vivo from those identified in this construct. Similarly, we were unable to assess the additive effects of drug metabolites in this ex vivo construct. Fourth, these medications were tested in adult rodent hearts for the purpose of relative comparison. It is possible that the magnitude of these effects on a healthy human heart may differ from those found here. Also, the Langendorff preparation is thought to be somewhat hypoxic (despite the use of hyperoxic buffer) and prone to develop edema over time (due to the low oncotic pressure of the perfusate). The negative inotropic effects of these drugs may differ in patients with already diminished cardiac output, focal ischemia, or in critical illness. Fifth, because we intended to examine only the direct drug effect on the myocardium, we studied hearts only in sinus rhythm rather than an arrhythmia. The physiologic benefits of more effectively treating an arrhythmia may offset the negative inotropic of a superior agent in some situations. However, because of the benign nature of certain agents, such as procainamide, in this series, this work may support their use as a first-line agent in situations where therapeutic efficacy is considered equivalent or when the risk of negative inotropy exceeds the benefit of improved efficacy of another agent.
Conclusions
In isolated hearts with constant loading conditions, amiodarone and sotalol depressed myocardial contractility, cardiac output, and diastolic function. Procainamide did not negatively affect myocardial performance and represents a favorable agent in settings of therapeutic equivalence. We believe that these comparative results may be useful to inform future guidelines regarding the choice of antiarrhythmic agents.
Footnotes
Acknowledgments
The authors are grateful to AltaThera Pharmaceuticals for the provision of the sotalol formulation and to Lynn Sleeper for advice regarding the statistical analysis.
Author Contributions
C. Mackin and E. S. DeWitt contributed equally as first authors. C. Mackin, K. J. Black, B. D. Polizzotti contributed to design and contributed to acquisition, analysis, and interpretation. E. S. DeWitt and Kheir contributed to conception and design and contributed to acquisition, analysis, and interpretation. X. Tang contributed to design and contributed to analysis and interpretation. S. J. van den Bosch and M. E. Alexander contributed to conception and design and contributed to analysis and interpretation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the American Heart Association Innovative Research Grant, as well as philanthropic donations from the Hess Family and the Haseotes Family. Dr DeWitt’s salary was supported by NHLBI T-32 Training Grant.