
Abstract
Aim:
Recently, digoxin use has been found to associate with higher mortality. Yet, potential mechanisms by which digoxin use increases mortality remain unclear. Increased arrhythmogenicity from digoxin use is one possibility. Thus, we aimed to evaluate the relation between digoxin and shock events in patients with implantable cardioverter defibrillators (ICDs).
Methods:
We performed a retrospective chart review of all patients with ICDs and at least 1 device interrogation at our institution between January 1, 2012, and January 1, 2015. We aimed to cover 1 year of interrogation period. Patients with heart failure, atrial fibrillation, or both were included in the analysis. Patients were divided into 2 groups based on digoxin use, defined as use of digoxin for any period of time during ICD interrogation period. Incidence of ICD shock events and electrical storms and hospitalizations were compared between the 2 groups.
Results:
The study included 202 patients. Of those, 55 patients were on digoxin and 147 were not on digoxin. Patients on digoxin were more likely to receive ICD shocks (odds ratio [OR] = 2.5, 95% confidence interval [95% CI] = 1.01-6.18, P = .04) and have increased risk of electrical storms (P = .02). Moreover, total hospitalizations were higher in digoxin users (P = .02). Multivariate logistic regression analysis also showed that digoxin use was an independent predictor of shock events (OR = 4.07, 95% CI = 1.43-11.58, P = .009).
Conclusion:
Digoxin is associated with increased shock events and electrical storms in patients with ICDs; however, large randomized controlled studies are needed to confirm our findings.
Introduction
Since the introduction of cardiac glycosides in the 18th century, digoxin has been used as a positive inotropic agent in patients with systolic heart failure (HF) as well as a rate-controlling agent for patients with atrial flutter and/or atrial fibrillation (AF). 1 The Digitalis Investigation Group (DIG) trial, the largest randomized controlled trial (RCT) to date, evaluated the effect of digoxin in patients with HF. The study showed that digoxin provides symptomatic relief and decreases the frequency of hospitalizations in patients with HF without any mortality benefit. 2 The use of digoxin in AF on the other hand is not supported by data from large RCTs. However, current practice guidelines do endorse its use in patients with AF in the setting of HF. 3,4
Recently, the safety of digoxin has been found controversial after several observational studies showed increased mortality when digoxin was used in patients with AF and HF. 5 To date, the etiology of increased mortality with digoxin use is not well-understood. A possible mechanism is that digoxin is associated with increased arrhythmogenicity. In a post hoc analysis of the Multicenter Automatic Defibrillator Implantation Trial–Cardiac Resynchronization Therapy (MADIT-CRT) trial, 6 digoxin use was associated with an increased incidence of ventricular arrhythmias in patients with HF. In addition, digoxin use was previously reported to be a predictor of appropriate implantable cardioverter defibrillator (ICD) shocks in patients with HF. 7 In the present study, we aimed to evaluate whether digoxin is associated with increased rates of ICD shocks in patients with HF and/or AF.
Methods
Patient Selection
We performed a retrospective chart review of all patients with ICDs who had at least 1 visit for device interrogation at the University Health in Shreveport, Louisiana between January 1, 2012, and January 1, 2015. The study was approved by the institutional review board of Louisiana State University Health Science Center in Shreveport, Louisiana.
Patients included in the study had to be 18 years of age or older and had AF and/or HF. Patients were excluded if they had end-stage renal disease during the period of interrogation or if ventricular arrhythmia/ICD shock was in the setting of ST-segment elevation myocardial infarction.
Atrial fibrillation could be paroxysmal, persistent, or permanent for inclusion in the study. For the purpose of this study, HF was defined as an average ejection fraction (EF) of <45% based on all echocardiograms done during the period of interrogation. If no echo was available during that duration, EF was obtained from either multigated aquisition scan or a nuclear stress test. If EF information was not available from any of the aforementioned sources during the period of interrogation, information was obtained from the most recent study in the medical record.
Data Collection and Patient Grouping
An electronic medical record was used to collect demographic and clinical data on all patients included in the study. Device interrogation data were obtained from the 3 most recent interrogations during the study time line to cover at least 1 year. If those 3 interrogations covered less than 1 year, more interrogations were included, when available, until a 1-year coverage was reached. The most recent interrogation was obtained from an outpatient visit in all patients and then the preceding interrogations were either outpatient or inpatient.
Patients were divided into 2 groups based on digoxin use. The study group included patients who were on digoxin at any point during the period of interrogation. The control group included patients who were not on digoxin during the period of device interrogation.
Outcomes
The main outcome in the present study was ICD shock events. Implantable cardioverter defibrillator shocks included total shocks, appropriate and inappropriate shocks, and electrical storms. An appropriate shock was defined as any shock event delivered in the context of ventricular tachycardia (VT) or ventricular fibrillation (VF). Shock events considered inappropriate were observed in the context of either a supraventricular arrhythmia or a sinus tachycardia. For the purpose of this study, an electrical storm was defined as 3 or more ventricular arrhythmias requiring ICD shocks within 24 hours. The number of hospitalizations during the 1-year period of interrogation was also compared between digoxin users and nonusers.
Statistical Analysis
Descriptive statistics for baseline characteristics of the participants are presented as frequency, percentage, mean, and standard deviation (SD) for the 2 groups—digoxin users and nonusers. Chi-square test of association was used to compare dichotomous groups. When sample size was small, dichotomous groups were compared using Fisher exact test. Continuous variables were compared using independent samples t tests when skewness, kurtosis, and Kolmogorov-Smirnov values were in acceptable ranges and data were expressed as mean with SD. If the data did not meet the criteria for the independent samples t test, then the nonparametric Mann-Whitney U test was applied to assess the difference in median values between groups. Multivariable logistic regression analysis was also performed to adjust for potential confounders. All statistical tests were 2 tailed and results were considered significant at P < .05. The likelihood of outcomes was assessed by estimating the odds ratios (ORs) and 95% confidence intervals (CIs). All analyses were conducted using IBM SPSS Statistics (version 21.0; IBM Corporation, Armonk, New York).
Results
Between January 1, 2012, and January 1, 2015, 476 patients were presented to our institution for device interrogation visits. After applying inclusion and exclusion criteria, 202 patients were included in the study. The study group (digoxin users) included 55 patients and the control group (patients not on digoxin) included 147 patients. Selection process is demonstrated in Figure 1.
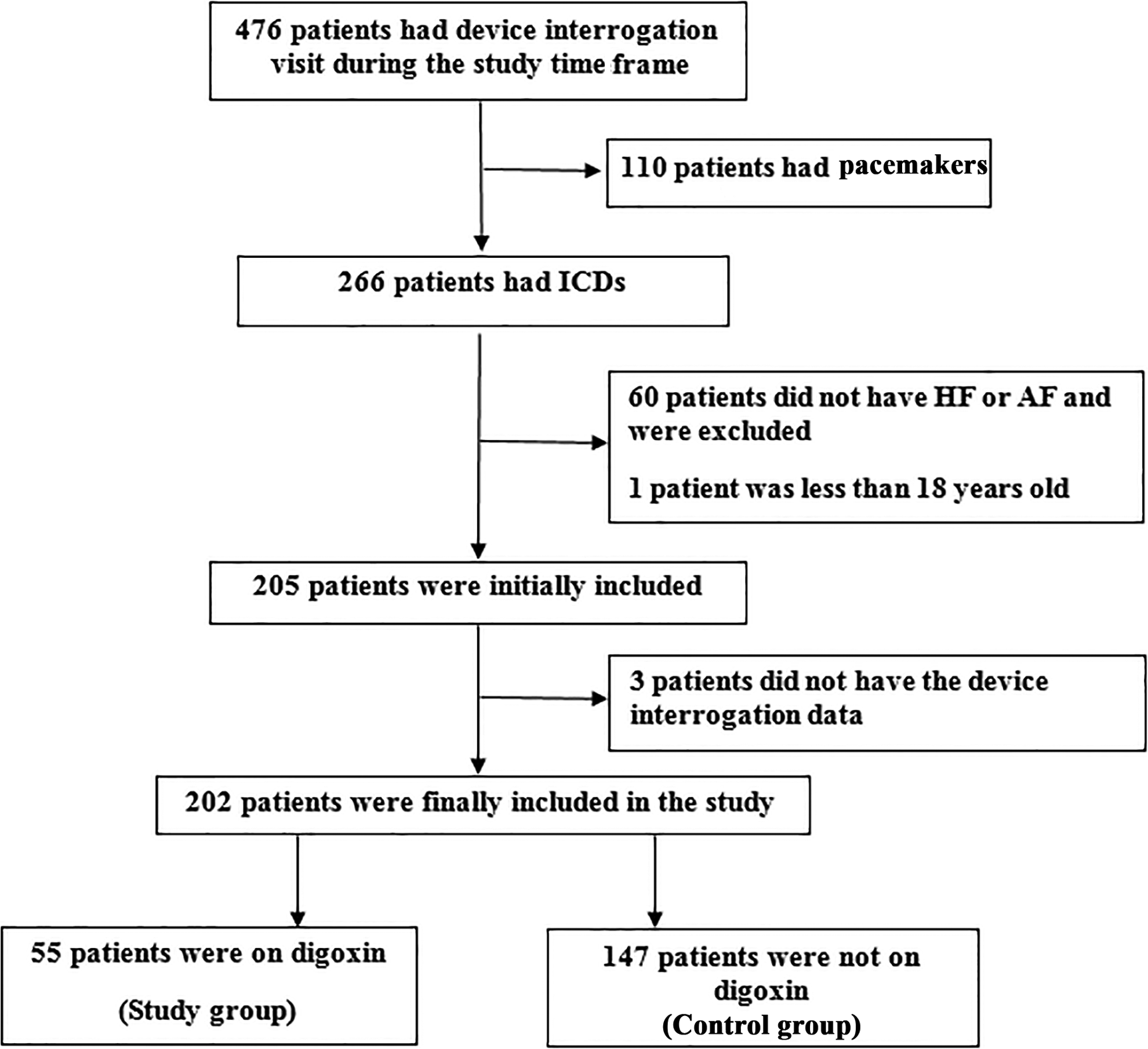
Flowchart for patient selection.
Baseline Characteristics
Baseline characteristics are shown in Table 1. There were no significant demographic differences between the 2 groups. When compared to patients not on digoxin, patients on digoxin were more likely to have AF and HF (38.2% vs 21.8%, P = .02) and less likely to have HF without AF (50.9% vs 72.1%, P = .01). Between the 2 groups, there were no differences in AF without HF (10.9% vs 6.1%, P = .99). Mean EF was similar between the 2 groups (27.86 [13.03] vs 27.38 [11.18], P = .8). All other medical comorbidities were evenly distributed between the 2 groups. The mean corrected QT (QTc) interval was shorter in digoxin users (452.85 [34.5] vs 466.44 [35.41], P = .04). Patients on digoxin were more likely to have Biventricular ICDs (BiV-ICDs) (38.2% vs 18.4%, P = .003) and patients not on digoxin were more likely to have single- or dual-chamber ICDs. There was no difference between the 2 groups regarding the indication of ICD as either primary or secondary prevention. The number of interrogations ranged between 1 and 6 interrogations, with an average of 3 interrogations per patient.
Baseline Characteristics of Patients with ICD.

Abbreviations: ACEI, angiotensin converting enzyme inhibitor; AF, atrial fibrillation and/or flutter; ARB, angiotensin receptor blocker; BB, β blocker; BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; EF, ejection fraction; HF, heart failure; HTN, hypertension; ICD, implantable cardioverter defibrillator; IQR, interquartile range; SD, standard deviation; QTc, corrected; QT interval; BiV, biventricular; VF, ventricular fibrillation; VT, ventricular tachycardia. Significant p values are typed in bold.
aTotal patients with HF.
bPatients who were not paced.
Outcomes
Outcome results are shown in Table 2 and Figure 2. Patients on digoxin were more likely to have ICD shocks when compared to controls (18.2% vs 8.2%, OR: 2.5, CI: 1.01-6.18, P = 0.042). Both appropriate and inappropriate shocks were numerically higher in the digoxin group (12.7% vs 7.5% and 7.3% vs 2%, respectively) but did not reach statistical significance. Furthermore, patients on digoxin were more likely to have electrical storms than patients not on digoxin (9.1% vs 1.4%, P = .02). Patients on digoxin also had more hospitalizations (69.1% vs 53.1%, P = .04). However, hospitalizations due to HF exacerbation (25.5% vs 23.8%, P = .81) or hospitalizations secondary to shock events (9.1% vs 5.4%, P = .35) did not differ between the 2 groups. Multivariable logistic regression analysis also showed a significantly higher likelihood of experiencing total shocks for those who were on digoxin compared to those who were not on digoxin (Table 2).
Outcomes Among the Study Population.a

Abbreviations: CI, confidence interval; HF, heart failure; OR, odds ratio.
aOutcomes presented with odds ratio were analyzed using Chi-square test. Outcomes presented as P value only were analyzed using Fisher exact test due to small sample sizes that did not permit odds ratio calculation.
bAnalyses were adjusted for age, sex, body mass index, hypertension, diabetes mellitus, coronary artery disease, ejection fraction, and type of implantable cardioverter defibrillator.

Diagram showing higher incidence of shock events and electrical storms in digoxin users as compared to patients not on digoxin.
Outcomes were evaluated in a subgroup of patients with HF without AF and patients with HF and AF (Table 3). Similar to the results of all patients, patients with only HF and who were on digoxin had significantly higher total shock events compared to patients with only HF who were not on digoxin (P = .03). Both appropriate and inappropriate shocks were numerically higher in the digoxin group but were not statistically significant. Moreover, electrical storms were also higher in patients on digoxin (P = .008). Conversely, in patients with both HF and AF, there were no statistically significant differences in the incidence of shocks or electrical storms between patients on digoxin and patients not on digoxin.
Outcomes in Specified Subgroups.

Abbreviations: AF, atrial fibrillation and/or flutter; HF, heart failure.
Discussion
In this retrospective study, digoxin use was independently associated with an increased incidence of ICD shock. In addition, our study is the first to show an increased incidence of electrical storms in patients with ICD on digoxin when compared to patients who were not on digoxin.
Digoxin has been widely used as a positive inotropic agent in patients with systolic HF and as a negative chronotropic agent in patients with AF. The main mechanism of the positive inotropic effect of digoxin is inhibition of Na+/K+-ATPase in cardiac myocytes, which reduces efflux of cytosolic Na; therefore, Ca++ efflux through the Na+/Ca2+ exchanger is reduced, leading to increased intracellular Ca++ and increased contractility. 8
After the DIG trial showed absence of a mortality benefit with digoxin use in patients with HF, 2 there was a significant decline in its use in routine clinical practice. 9,10 However, digoxin continues to be used for symptomatic relief and to decrease frequency of patient hospitalization. More recently, large observational studies and meta-analysis showed increased mortality in patients on digoxin, which has led to major concerns about its safety. 1,5,11 However, the exact mechanism of increased mortality with digoxin use is yet to be determined.
Given the proarrhythmic potential of digoxin and its narrow therapeutic window, a possible mechanism of increased mortality with digoxin use is increased rates of cardiac arrhythmias. 12 It has been proposed that the mechanism of digoxin-induced arrhythmia may be related to excessive intracellular Ca++ leading to transient increase in inward depolarizing currents, thus leading to generation of delayed afterdepolarizations. 13,14
In the current study, patients on digoxin had significantly higher incidence of ICD shock events when compared to patients who were not on digoxin (P = .042). Both appropriate and inappropriate shocks were numerically higher in the digoxin group but did not reach statistical significance likely due to the small number of events. Our findings are in agreement with Desai et al, 7 who found that digoxin use was one of the predictors of appropriate ICD shocks in patients with HF, and with Erath et al, who found a trend toward increased total ICD shock events in patients on digitalis that was mainly driven by increased appropriate shocks. 15 In addition, in a retrospective substudy of the MADIT-CRT trial, 6 digoxin use was associated with increased appropriate shock events. Moreover, Adelstein et al also found increased incidence of appropriate shocks in patients with HF. 16 However, their findings were limited to patients with EF of <22% and patients with coronary artery disease who have BiV-ICDs. Likewise, Soliman et al found that digoxin is associated with a significant increase in appropriate ICD therapy. However, their findings were also limited to patients with HF with BiV-ICDs who have New York Heart Failure Association class III symptoms. 17
Previous studies show ICD shocks, whether appropriate or inappropriate, are associated with higher risk of mortality in patients with HF. 18 -22 Appropriate ICD shocks are indicators of increasing ventricular arrhythmias and deteriorating HF status, thus explaining the increased mortality. Alternatively, the association of inappropriate shocks with increased mortality has been shown in subgroup analysis of the MADIT II 18 and the Sudden Cardiac Death in Heart Failure Trial. 21 A proposed explanation is possible mechanical injury to the myocardium secondary to the shock itself. 23
In a subgroup analysis, shock events were significantly higher in patients with HF alone and not in patients with both HF and AF. This is in agreement with Chamaria et al who found that there was no increased mortality in a subgroup of patients with HF and AF who were on digoxin. 24 In addition, the results of our study is in agreement with the results of the main analysis of Vamos et al, who observed increased mortality with digoxin use in patients with HF. 5 Vamos et al did not analyze data specifically for patients with both HF and AF, while our study divided patients into those with HF plus AF and those with HF without AF, making it difficult to compare our results to the results of Vamos et al.
Our study is the first to prove digoxin use is also associated with increased incidence of electrical storms when compared to patients not on digoxin. Electrical storms have also been shown in previous studies to be independent predictor of increased morbidity and mortality from HF. 25,26 Increased electrical storms were also evident in subgroup of patients with only HF but not in patients with HF and AF.
Limitations
The current study is retrospective in nature, and therefore, there may be residual confounding factors that were unaccounted. In addition, the sample size was small, which can affect the results obtained by the multivariable analysis. Device parameters for detection and therapy of arrhythmias were not standardized and were determined by the physician who placed the device. Review of the device parameters in the included patients however show that the VT and VF zones in the digoxin and nondigoxin groups were comparable (Table 1). Another limitation is that data on serum digoxin level during the period of interrogation were not available. Therefore, future large randomized prospective studies are needed to confirm our findings and to stratify the association between digoxin use and increased shock events based on serum digoxin level.
Conclusion
Digoxin use is associated with increased ICD shock events and electrical storms in patients with HF and/or AF. Therefore, risks versus benefits of digoxin therapy have to be evaluated before its use in those patients.
Footnotes
Authors’ Note
This was a retrospective chart review of human patients which was approved by the institutional review board of Louisiana State University Health Sciences Center in Shreveport, Louisiana.
Acknowledgments
We would like to thank Alexandria Brackett for her assistance in preparing this manuscript.
Author Contributions
George S Mina contributed to design, contributed to acquisition and interpretation, drafted the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Madan Acharya contributed to acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Taylor Shepherd contributed to acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. George Gobrial contributed to acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Michael Tekeste contributed to acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Hussam Watti contributed to acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Ruchi Bhandari contributed to analysis, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Aditya Saini contributed to conception and design, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Pratap Reddy contributed to interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Paari Dominic contributed to conception and design, contributed to interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.