
Abstract
Statin nonadherence is a major challenge to optimal management. Patients nonadherent to statin therapy do not receive the expected benefit relative to the degree of low-density lipoprotein cholesterol (LDL-C) lowering obtained. This is important because new evidence guidelines recommend statins as the first-line therapy for those in high-risk groups (secondary prevention, patients with diabetes 40-75 years of age, and LDL-C ≥ 190 mg/dL) and in selected primary prevention patients. Statin assignment in the latter group occurs only in those with an estimated ≥7.5% 10-year atherosclerotic cardiovascular disease risk after shared decision making in a clinician–patient risk discussion. However, in numerous studies, statin nonadherence shows little or no benefit in reducing cardiovascular events or mortality compared to placebo, effectively negating the risk reduction expected from statin use and concomitantly increasing the total cost of health care. The causes and solutions for nonadherence are multifactorial and include patient, clinician, and health system factors. We believe that a clinician–patient partnership that facilitates patients’ understanding of the potential for optimal benefit with the least adverse effects is an important first step toward improving adherence. A transtheoretical model of stages of behavior change helps clinicians address many of the common factors limiting adherence to statins. We conclude with a teaching tool emphasizing a structured approach to statin therapy with patient-centered risk discussions.
Keywords
Case History
A 62-year-old African American woman was seen in the outpatient clinic. She had hypertension and hypercholesterolemia for several years prior to an acute myocardial infarction (MI) 1 year ago. After an angioplasty with drug-eluting stent in the left anterior descending artery, she was discharged on secondary prevention medications including atorvastatin 80 mg/d. A lipid panel obtained 6 weeks after discharge showed a low-density lipoprotein cholesterol (LDL-C) of 75 mg/dL. By contrast, laboratories drawn 1 day prior to the office visit showed an LDL-C of 99 mg/dL. She was asked by the medical student whether she took her medications regularly, and she stated she did. However, when asked specifically how many doses she missed in the 30 days prior to the visit, she stated she missed 8 doses for a variety of reasons. Importantly, she did not have a system for taking her medications. This case illustrates how a systematic approach to adherence is needed to get optimal LDL-C lowering with therapies proven to provide net benefit in randomized controlled trials (RCTs). Two simple questions—asking about a system for medication use and inquiring about pills missed in the past 30 days—were crucial to uncover an important patient issue. This review explores barriers and offers an approach utilizing a teaching tool for all members of the health care team to address this important clinical problem.
Introduction
Statins reduce LDL-C, have anti-inflammatory effects, and reduce total mortality in both secondary and high-risk primary prevention when compared to placebo. 1 The 2013 American College of Cardiology/American Heart Association guidelines on the treatment of cholesterol to reduce atherosclerotic cardiovascular disease (ASCVD) emphasized the notion of adherence to both lifestyle changes and statins as important features of management. 2 Evidence for statin efficacy in reducing ASCVD is demonstrated with various large-scale RCTs, all showing that treatment with a moderate- or high-intensity statin affected a predictable reduction in relative risk. 3 –9 For every 38.7 mg/dL reduction in LDL-C, event rates were lowered, on average, by 20% to 22%, thereby supporting the recommendation to treat with appropriate intensity of statin therapy. 1,10,11 This results in a larger absolute risk reduction in those at higher risk. Notably, the guidelines did not recommend for or against treating to an arbitrary “goal” LDL-C or non-HDL-C as the best means to reduce ASCVD risk because RCTs were not designed to answer this question. 2 Instead, the goal for therapy is to drive LDL-C lower with adherence to both lifestyle and an optimal intensity of statin shown in RCTs to provide benefit in high-risk patient groups. Results of the IMProved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) 12 trial indicate that, in very high-risk patients with acute coronary syndrome and 1 high-risk feature, addition of ezetimibe to a moderate-intensity statin results in lower LDL-C and improves outcomes as contrasted with moderate-intensity statin alone. If further LDL-C lowering with RCT-proven therapy results in improved cardiovascular outcomes, then addressing adherence to such therapy as an additional means to get LDL-C lower creates an opportunity that should not be overlooked.
The challenge of adherence is not a new problem, and it is not limited to statins. Multiple studies have investigated the impact of nonadherence with antihypertensives, oral hypoglycemics, chemotherapy, highly active antiretroviral therapy, and other medications for chronic medical conditions. 13 –15 Evidence continues to support the importance of adherence to medication regimens and the immense challenge of overcoming the barriers involved. This review focuses on nonadherence as it applies to statin therapy, with the aim of providing clinicians with an approach to optimize use of this ASCVD risk reduction therapy.
General Principles of Adherence
Adherence is defined as the “extent to which patient behaviour corresponds with recommendations from a health care provider (page 136)” 16 and it is synonymous with terms such as compliance or concordance. Nonadherence, therefore, is the inverse of this statement, and it can be subdivided further at various points in the therapy regimen. 17 Primary nonadherence refers to the failure to initiate therapy, while secondary nonadherence relates to not taking the medication at the prescribed dosage and schedule or prematurely discontinuing the treatment. 18
Measuring adherence is challenging, and both direct and indirect methods have their benefits and drawbacks. 19 Direct observed therapy is impractical for routine use and can be skewed by patients hiding or “cheeking” pills in their mouths. Similarly, objective measurements of the drug or its metabolites have varying utility and are typically expensive, and they do not account for “white-coat adherence” or improved adherence in the window before and after a health care encounter. Indirect methods are more common and include questionnaires, self-reporting, and pill counts, which are simple to execute but susceptible to manipulation. Rates of prescription refills also act as a surrogate for adherence as such data are readily available from pharmacies, but it is not equivalent to ingestion of medication. Most statin adherence trials use an arbitrary cutoff of 80% defining adherence, though clinicians should note that those who have greater than 80% adherence may derive even further benefits owing to reduced LDL-C levels. 18
Prevalence of Statin Nonadherence
Prevalence rates of statin nonadherence vary significantly among studies with a range of 7% to 67% nonadherence at 1-year follow-up, including patients requiring both primary and secondary prevention.20–30 Moreover, nonadherence rates appear to increase in general with time as seen in studies with longer follow-up duration. Studies that assessed adherence rates among statin users were included if the total number of patients followed was greater than 1000 and there was a follow-up time of at least 1 year. A summary of these data are provided in Table 1.
Prevalence of Statin Nonadherence.
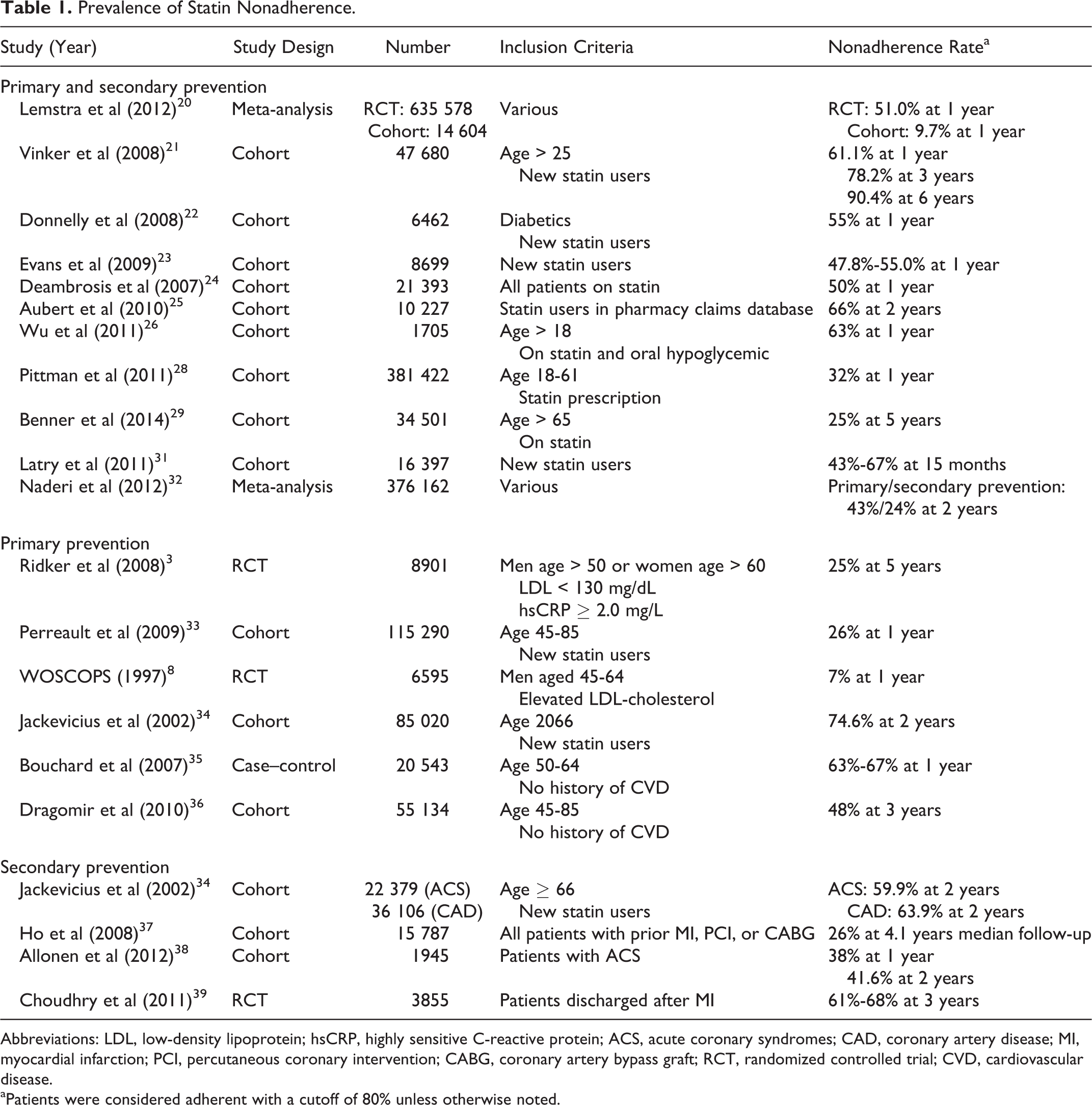
Abbreviations: LDL, low-density lipoprotein; hsCRP, highly sensitive C-reactive protein; ACS, acute coronary syndromes; CAD, coronary artery disease; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; RCT, randomized controlled trial; CVD, cardiovascular disease.
aPatients were considered adherent with a cutoff of 80% unless otherwise noted.
Effect on Outcomes
Statin nonadherence, not surprisingly, negates the risk reduction that statins provide when taken as directed. Numerous studies have demonstrated that patients with low adherence to statins had either no reduction or an increase in cardiovascular disease mortality compared to placebo, while those with adherence showed a marked decrease. 8,33,35 Statin discontinuation was also independently associated with higher all-cause mortality, hospitalizations, and revascularizations. 40,41 Nonadherence is associated in particular with significantly increased mortality in patients discharged after acute coronary syndrome. 38 Indeed, in IMPROVE-IT, 12 the high rates of nonadherence may have substantially reduced the observed benefit. Finally, nonadherence to statins was also observed to increase the rate of cerebrovascular events. 42
Nonadherence itself may be associated with unhealthy behaviors that may contribute to poor outcomes. For instance, investigators in the Coronary Drug Research Project 43 found that survivors of MI with good adherence to the intervention drug, clofibrate, had improved outcomes compared to noncompliers, even though overall outcome by intention-to-treat analysis showed no difference between clofibrate and placebo. Moreover, patients with good adherence to placebo had improved outcomes compared to those nonadherent to placebo, suggesting that behavioral factors extrinsic to the medication itself impact outcomes as well.
Economic Costs
Statin nonadherence has a significant economic role in increasing overall health care costs. Two large studies of primary and secondary prevention evaluating statin adherence and overall health care cost found that low adherence was associated with an increase in hospitalization and an increase in total health care costs of US$1060 and US$868, respectively. 36,25 Another investigation of 1705 diabetic patients found that statin nonadherence increased all-cause medical costs by 15%. 26 A large retrospective cohort study of 381 422 patients investigating statin adherence and health care costs over 18 months found that though patients with high adherence spent approximately US$350 more on their statin prescription, 28 the total cost of health care was US$904 higher in the nonadherent group. Finally, Peterson and McGhan 44 performed a systematic review of multiple pharmacoeconomic analyses of statin noncompliance and determined that cost-effectiveness of statins between full adherence and nonadherence is in the range of US$4500 to US$250 000 per life-year saved, depending on factors such as age, risk, and primary versus secondary prevention.
Causes and Predictors of Poor Statin Adherence
Numerous factors come into play that affect how likely and effectively patients will adhere to their statin therapy. These multifactorial causes can be broadly grouped into 3 categories, that is, health system factors, patient-specific factors, and clinician-specific factors. 45
Health systems and the reality of patients and clinicians as part of this system have significant effects on medication adherence that are not easily overcome. Part of the system’s involvement is related to patient access to health care, allowing them to receive appropriate medical management. 46 This includes significant time constraints on clinicians as a result of heavy patient volumes and inadequate resources that ultimately overtax the entire health system. Time spent with patients may be insufficient to address all of the important health concerns, not to mention time spent discussing statins and adherence. Another issue is coordination of health care. In the early 2000s, the average Medicare beneficiary saw 7 physicians per year (including specialists), which requires communication and coordination between physicians not only to ensure that the patient is aware of his or her plan of care but also to delegate and acknowledge which aspects of the patient’s care each physician is managing. 47 Finally, several studies have, not unexpectedly, shown a negative association between drug adherence and increasing copayment for the medication, and cost of medication and low socioeconomic status are often cited as reasons for noncompliance. 48,49 One RCT comparing patients post-MI with “usual” prescription coverage to those with full coverage found that elimination of copayments significantly improved rates of adherence. 39
Multiple factors related to statin adherence relate to factors specific to individual patients. Factors including mental illness, dementia, age (both young and elder), and lower socioeconomic status are very commonly cited as being associated with or as predictors of statin nonadherence. 8,29,40,50 Mental illness is particularly notable as anxiety and depression are also highly associated with cardiovascular disease and stroke. 51,52 Interestingly, severity of illness plays a role in nonadherence as well; numerous studies demonstrate that patients with recent MI or symptomatic heart disease tend to have higher rates of statin adherence than those with chronic CAD and minimal symptoms or those in primary prevention. 29,31,53 –55 In a retrospective study of 4886 veteran patients, an increased number of medications at baseline was directly and significantly associated with increased statin adherence; unlike the expected negative effect of polypharmacy, this suggests that patients on more medications may truly believe they are ill and are therefore more likely to adhere to their medication. 56
This association between illness perception and statin adherence relates to patients’ understanding of their illness. Lack of understanding of the disease, lack of involvement in treatment or decision making, and poor literacy are all cited as causes of medication nonadherence. 50,57,58 Poor literacy is particularly notable, given the significant rate of suboptimal health literacy in approximately 90 million people in the United States. 59 Furthermore, in the Understanding Statin use in America and Gaps in Education (USAGE) study of 10 138 individuals responding to an Internet survey on statin use, the highest likelihood ratios for adherence were associated with satisfaction with medication and with the doctor’s explanation of high cholesterol, while factors associated with poor adherence were dissatisfaction with the physician’s explanation of high cholesterol and using the Internet to learn about statin treatment. 50 All of these factors point toward a significant deficit in patient education affecting nonadherence.
Additionally, adverse effects are a common reason for medication nonadherence. The 2 most common adverse effects associated with statin use are musculoskeletal symptoms and new onset of diabetes. The USAGE study was not a randomized trial but found muscular side effects to be a significant factor associated with poor adherence. 50 Although myalgias are commonly seen in patients, their incidence is around 5% to 18%. 60,61 Varying rates of myalgias probably reflect lack of a standard definition of statin myalgia and the confounding by a background of musculoskeletal symptoms in patients given statins. Statin myopathy and rhabdomyolysis are much less common and in about 1 in 1000 and 1 in 10 000 patients, respectively. 60,62 –65 With regard to diabetes, 3 factors affect the incidence of diabetes diagnoses with statins. First is the intensity of the statin: moderate-intensity statins have a risk of 1 in 1000, while high-intensity statins have a risk of 3 in 1000. 2 Second are metabolic risk factors such as blood glucose control, obesity, and the metabolic syndrome. In the Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) 3 study, lack of these risk factors made appearance of diabetes unlikely. Indeed, in those who progressed to diabetes on a statin, statin initiation appeared to hasten the diagnosis by only 5.4 weeks on average. 66 Third, age of the patient plays a role as well. Pravastatin was not associated with new-onset diabetes in the West of Scotland Coronary Prevention Study (WOSCOPS) 8 trial where participants were significantly younger (45-64 years old) than in the PROspective study of pravastatin in the elderly at risk (PROSPER) 9 trial (70-83 years at entry). Finally, a recent review discussed the paucity of evidence linking statins to memory, liver, or kidney damage. 67
As far as the impact of adverse effects on adherence, however, 1 study of adherence of multiple medications found no differences among classes of medication, suggesting that side effects (which were variable) were not the main cause. 32 In fact, it is argued that discontinuation of medications due to adverse effects, termed “rational nonadherence,” is a result of patient-specific concerns that are not addressed by the physician. 68 This is especially true as there are multiple statins available and several extrinsic factors to consider that may address the undesired effects. 69 Indeed, Zhang et al 70 showed that of 57 292 people who had statins discontinued at least once during the study, 35 871 (62.6%) were taking a statin 1 year later, with the majority taking a different statin than initially prescribed.
Finally, but still contingent on communication, hospital discharges and subsequent follow-up pose a significant barrier to adherence largely due to poor communication between clinicians. Medication discrepancies following discharge occur approximately 15% of the time; direct communication between hospitalists and primary care physicians occurs less than 20% of the time, and discharge summaries are available at less than 34% of the time at the first follow-up visit. 71,72 Makaryus and Friedman 73 noted that, in a small study of 47 patients at discharge, less than 50% of patients were able to list all of their medications and even fewer could explain their purpose.
Improving Statin Adherence
The multifactorial complexities that makeup the barriers to statin adherence earn themselves a multifaceted, multidimensional approach as supported by a recent Cochrane database review. 74 We will address potential strategies to the obstacles that were presented previously, and we will focus predominantly on providing individual clinicians with effective strategies that can begin to effect change.
Statin adherence is affected by the patient–clinician relationship with communication as a cornerstone of that interaction. Statin adherence increases with a strong patient–clinician dialogue that focuses on what statins are and why they are important to reduce events of ASCVD. 75,76 The USAGE survey demonstrated that patients nonadherent to their statin were more likely to be dissatisfied with their physicians’ explanation of the treatment. 50 The “From the Heart” survey 77 showed that although 77% of patients claim to be satisfied with information about cholesterol, only 26% were aware that heart attacks were a potential consequence of elevated lipid levels. Moreover, adherence increases with satisfaction with statins, stemming from having clear discussions about and screening for adverse effects, as well as adjusting therapy (eg, switching to a different statin) when medication becomes intolerable. This puts patients in a governing role as decision makers regarding their own health care and empowered patients are more motivated to manage their disease. At the very least, in the absence of formal counseling, clinicians can point patients to veritable resources including pharmacists, health programs, and reputable Web-based materials. 45
Additionally, it is essential for clinicians to make the best use of their time to discuss statins and adherence with patients. A cross-sectional survey of approximately 18 000 Medicare seniors found that there are significant gaps in the clinician–patient discussion to address medications. 78 Only 32% of patients discussed their medications with their clinician in the past year; meanwhile, of the patients who were nonadherent due to cost and noncost reasons, only 39% and 27%, respectively, breached the subject with their physicians. Moreover, communication ratings are independently associated with medication adherence beyond statin therapy, extending into oral hypoglycemics, 79 antihypertensives, 80 and adjuvant therapy. 81 There is a significant linear relationship between a strong working patient–clinician alliance and medication adherence. 82
Health systems can help facilitate clinician–patient communication by improving efficiency in order to allow clinicians more time with their patients to discuss adherence and issues surrounding their medications, particularly given current time constraints and the heavy volume of issues to discuss with patients. 83 A potential suggestion to improve efficiency is to focus on a team-based approach in which nonphysician staff assists with some of the duties of the patient encounter to give the physician more time to discuss medications. Additionally, further assessment of adherence can be done at multiple stages in the visit, including entry questionnaires, discussions with pharmacists in the office or in the community, phone calls, and providing educational material. 45 Similarly, electronic medical records and use of electronic prescriptions aid in efficiency of the visit as well as in identifying patients at risk of nonadherence. One study of 19 038 patients showed that delays in filling statin prescriptions of greater than 30 days was associated with a higher rate of nonadherence. 84
Furthermore, with over 4.5 billion mobile phone users worldwide, including 2 billion smart phone users, 85 there is great promise for this technology to address medication nonadherence. From text-messaging interventions to vibrating pill bottles, there are a myriad of new innovations available. 86 Two Cochrane reviews and several small studies have suggested the potential positive impact of mobile technology on medication adherence. 87 –89 These are promising tools.
Facilitating Behavioral Change
The stages and processes of self-change as they relate to behavior were originally described in 1983 as an integrative model to facilitate smoking cessation.
90
This transtheoretical model (TTM) of behavior was reapplied more recently by Johnson et al,
91
specifically in the realm of adherence toward lipid-lowering therapy as a behavior modification. The TTM defines the stages as follows: Precontemplation: intent to take an action at some point in the future. Contemplation: intent to take action in the near future (within 6 months) but without clear plan or commitment. Preparation: intent to make change within 1 month in addition to small behavioral changes already underway. Action: successful behavior change for less than 6 months. Maintenance: successful behavior change for more than 6 months.
Although presented linearly, the model is in fact cyclical, and patients often go back and forth through various stages and for different behavior changes at different rates and times. Each stage has a set of pros and cons that determine progression to the next stage (ie, when the pros outweigh the cons). This highlights two key factors: first, it is important to be aware of the stages and with which stage an individual patient may associate himself or herself at given moment, and second, it is important to have a risk–benefit discussion addressing the issues of that current stage in order to help the patient progress further. This is consistent with the philosophy of the clinician–patient risk discussion mentioned in the 2013 cholesterol guidelines. 2
Patients in the precontemplation and contemplation stages are uncertain about starting statin therapy. Patient education materials can supplement the discussion of the role of risk factors and atherosclerosis. This leads naturally into how proven risk reduction therapies such as lifestyle and if appropriate, statin therapy, can reduce that risk. If statins are considered, the discussion should include the potential for benefits and adverse effects of statins, including possible drug–drug interactions based on the patient’s clinical characteristics. It may be especially helpful for a patient’s spouse or family member to be present as patients may recall as little as 50% of information during an office visit. 92
Getting patients from the preparation stage to the action stage requires addressing and acknowledging patient-specific barriers to adherence. This is a crucial step that requires directly asking patients their concerns about statin therapy and what barriers to statin therapy need to be addressed. For instance, if cost is a barrier, it may be reasonable to start with a generic statin. Similarly, if there are concerns regarding side effects, efficacy, or the purpose of statins, the evidence can be reviewed with the patient. Again supplementary materials about statin side effects such as musculoskeletal complaints, new onset of diabetes, drug–drug interactions, liver or kidney concerns, and anecdotal reports about memory problems can be useful here. Patients may have many different reasons for nonadherence, whether practical, emotional, or perceptual, and we cannot address them without first knowing what they are for each individual patient. 93
Finally and perhaps the most challenging is progression to the maintenance stage and continuing treatment. First, much like asking about barriers to treatment, it is important to ask about adherence. Careful questioning may identify issues of adherence that the patient does not voluntarily disclose. Nieuwkerk et al 75 published a study looking at 2 questions to address adherence: “How many days during the past week did you take your lipid-lowering medication?” and “What percentage of your prescribed lipid-lowering medications did you take in the past month?” We would also add the question “Do you have a system for taking your medications?” Additional questions are summarized in Table 2. The goal is to confirm that the patient is tolerating statin therapy and is taking their statin regularly. Those who miss doses should be instructed in an organized system. However, in order to maintain adherence, it is important to revisit briefly their understanding of the need for statin therapy as well as readdressing old barriers and asking about new challenges. Adherence is a dynamic process, and its evaluation should not be less so.
Questions a Clinician Can Ask to Assess a Patient’s Medication Adherence.a
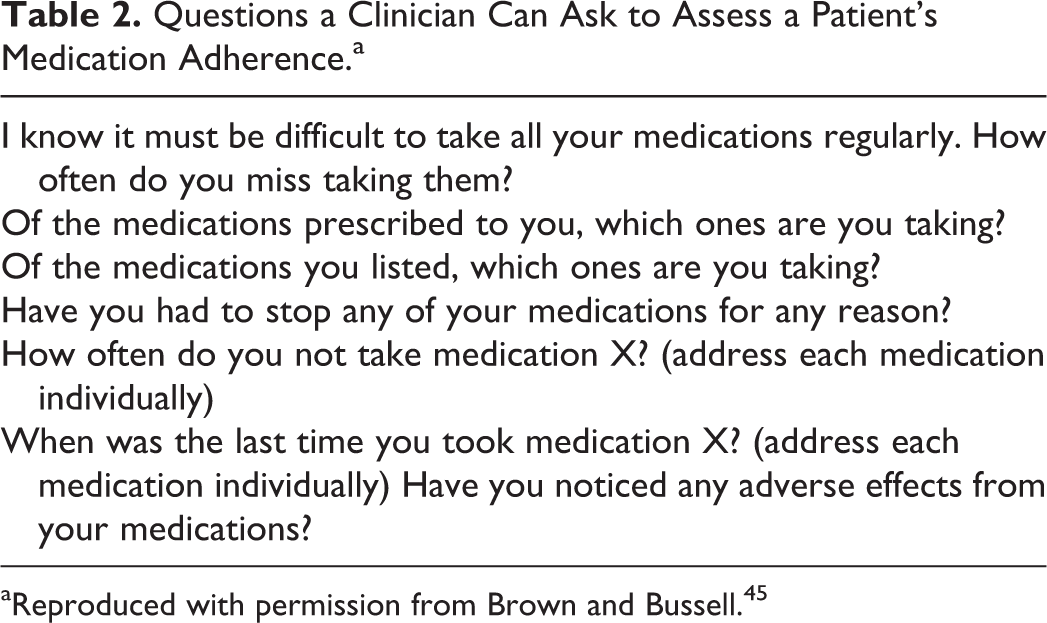
aReproduced with permission from Brown and Bussell. 45
We have created the RELATE mnemonic in conjunction with the TTM as a tool to teaching and understanding statin adherence in patients who may require or are already taking a statin (Figure 1). This may be particularly useful in instructing staff members who will work with these patients. The first 3 steps refer to patients in the precontemplation and contemplation stages who require discussions about Risk for ASCVD and the Effects of statins as well as a discussion of their Level of understanding. Subsequently, as patients prepare to take a statin, clinicians must Acknowledge the barriers to therapy. And finally, in order to maintain adherence to their statin, clinicians and patients should continue to have discussions about Tolerance and adherence as well as continuously Evaluating the importance of their medication and any question or issues the patient would like to clarify. By reviewing the RELATE mnemonic (Table 3), health care providers at all levels may be able to address more effectively the challenges surrounding statin nonadherence.

RELATE approach to addressing statin adherence as applied to the transtheoretical model (TTM).
RELATE Checklist for Clinicians.

Abbreviation: ASCVD, atherosclerotic cardiovascular disease.
Our patient was ready to change. We reviewed with her the most important barrier—lack of an organized system. We also addressed her concerns about muscular side effects, highlighting that nonpersistent, mild myalgias are unlikely to be related to her statin. She decided to put her statin in a 7-day pillbox on Sundays. When seen in 3 months, she reported had missed no medications in the past 30 days and achieved the expected further reduction in her LDL-C levels to the 70 to 75 mg/dL range.
Conclusion
Statin nonadherence is a multifaceted, multifactorial problem that is abundant and has no simple solution. In those patients proven to benefit by RCTs, adherence to statins allows the full ASCVD risk reduction to be realized. Moreover, there is a large body of evidence to demonstrate that benefit dwindles with nonadherence. We have reviewed the factors that contribute to nonadherence. Some of them relate to global health care functioning and costs that may take many years to change. Others can be addressed now, by patients and clinicians working together. Nonadherence should not be viewed as the fault of the patient but an important warning sign that must be addressed promptly for optimal management. We suggest that taking the time to RELATE to patients using concepts emphasized by our teaching tool will improve efforts to ensure optimal statin adherence.
Footnotes
Author Contributions
Alexander Turin, Jay Pandit, and Neil J. Stone contributed to conception and design; acquisition, analysis, and interpretation; drafted the article; critically revised the article, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.