
Abstract
Cannabidiol (CBD) is a nonpsychoactive phytocannabinoid with anti-inflammatory activity mediated by enhancing adenosine signaling. As the adenosine A1 receptor activation confers protection against ischemia/reperfusion (I/R)-induced ventricular arrhythmias, we hypothesized that CBD may have antiarrhythmic effect through the activation of adenosine A1 receptor. Cannabidiol has recently been shown to suppress ischemia-induced ventricular arrhythmias. We aimed to research the effect of CBD on the incidence and the duration of I/R-induced ventricular arrhythmias and to investigate the role of adenosine A1 receptor activation in the possible antiarrhythmic effect of CBD. Myocardial ischemia and reperfusion was induced in anesthetized male rats by ligating the left anterior descending coronary artery for 6 minutes and by loosening the bond at the coronary artery, respectively. Cannabidiol alone was given in a dose of 50 µg/kg, 10 minutes prior to coronary artery occlusion and coadministrated with adenosine A1 receptor antagonist 8-cyclopentyl-1,3-dipropylxanthine (DPCPX) in a dose of 100 µg/kg, 15 minutes prior to coronary artery occlusion to investigate whether the antiarrhythmic effect of CBD is modified by the activation of adenosine A1 receptors. The experimental groups were as follows: (1) vehicle control (n = 10), (2) CBD (n = 9), (3) DPCPX (n = 7), and (4) CBD + DPCPX group (n = 7). Cannabidiol treatment significantly decreased the incidence and the duration of ventricular tachycardia, total length of arrhythmias, and the arrhythmia scores compared to control during the reperfusion period. The DPCPX treatment alone did not affect the incidence and the duration of any type of arrhythmias. However, DPCPX aborted the antiarrhythmic effect of CBD when it was combined with it. The present results demonstrated that CBD has an antiarrhythmic effect against I/R-induced arrhythmias, and the antiarrhythmic effect of CBD may be mediated through the activation of adenosine A1 receptor.
Introduction
In patients with coronary artery disease, sudden death is the most common result of ischemia-induced lethal ventricular arrhythmias during the acute phase of the myocardial infarction (heart attack). Reperfusion of the previously ischemic myocardium seems to be a unique medical treatment option, which restores blood flow through blocked arteries to save myocardium from eventual necrosis in an hospitalized patient; however, reperfusion itself ironically leads to the life-threatening ventricular arrhythmias. 1,2
Cannabidiol (CBD), obtained from Cannabis sativa plant (marijuana), is a nonpsychoactive phytocannabinoids. 3 The chronic use of CBD is well tolerated without side effects in humans, 4 and it has been used in clinical practice for the treatment of the spasticity in multiple sclerosis, Huntington disease, pain, and inflammation. 5 –8 Cannabidiol has multiple pharmacologic actions, including antioxidant, anti-inflammatory, and antinecrotic effects. 9 All these pharmacological actions suggest that it could potentially be used as a tissue protective and antiarrhythmic agent. Likewise, it has also been revealed that CBD has a cardioprotective effect against myocardial ischemia–reperfusion (I/R) injury. 10,11 Durst et al demonstrated that chronic administration of CBD reduced myocardial I/R injury through the prevention of systemic inflammatory response. 10 Walsh et al subsequently demonstrated that a single acute dose of CBD (50 µg/kg intravenously) reduced myocardial I/R injury. 11 This study also demonstrated for the first time that CBD has an antiarrhythmic effect against ischemia-induced ventricular arrhythmias. However, the mechanism underlying the antiarrhythmic effect of CBD is obscure. Cannabidiol has a very low affinity for the cannabinoid receptor 1 (CB1) and cannabinoid receptor 2 (CB2). 12 The antiarrhythmic effect of CBD may be mediated through the modulation of CB1 and CB2 or non-CB1 and CB2, G protein-coupled receptor 55, and vanilloid receptor type 1. 13,14
Carrier et al revealed that CBD is a competitive inhibitor of adenosine uptake at the equilibrative nucleoside transporter (ENT). 15 Cannabidiol possesses the ability to enhance the extracellular adenosine concentration through the inhibition of adenosine uptake and thereby CBD increases the endogenous activity at adenosine receptors and the adenosine signaling. Cannabidiol has an anti-inflammatory effect produced by the adenosine A2A receptor activation, which is provided by the enhanced adenosine signaling. 15,16
Ischemic preconditioning (IP) causes extracellular adenosine accumulation that activates adenosine receptors. Therefore, IP provides a cardioprotective effect via the activation of adenosine A1 receptor. 17 –19 It has also been shown that a decrease in ischemia and I/R-induced arrhythmias occurs through adenosine A1 receptor activation, induced by selective adenosine A1 agonists, 2-chloro-N6-cylclopentyl-adenosine, and N6-(2-phenylisopropyl)-adenosine R-(−)isomer. 20 –22 As the researchers have indicated that CBD may enhance adenosine signaling and therefore may lead to the adenosine A1 receptor activation, we hypothesized that CBD may decrease reperfusion-induced arrhythmias via the activation of adenosine A1 receptor.
The aim of this study was to determine the effect of a single acute dose of CBD on reperfusion-induced ventricular arrhythmias and to explore the potential role of the adenosine A1 receptors in this effect.
Methods and Materials
Animals
This study used 42 male Wistar albino rats, weighing 280 to 380 g each. They were bred in the Experimental Animal Production and Research Centre, Bülent Ecevit University, Turkey. The animals were kept in a room with a temperature of 21°C ± 2°C, 40% to 65% humidity, and a 12-hour light–dark cycle and permitted to consume as much tap water and standard rat pellet food as they wish. The animals were treated in experimental procedures according to the guidelines and recommendations of the World Medical Association. All the experimental procedures in this study were discussed and approved by the Animal Research Local Ethical Committee of Bülent Ecevit University, Zonguldak (protocol no: 2013-17-17/07).
Surgical Procedures
The surgical protocols performed in this study were previously defined by Bozdoğan et al. 23 The anesthetized rats with an intraperitoneal injection of thiopental sodium (85 mg/kg) were placed on an animal rectal temperature controller (9404-A; Commat Ltd, Ankara, Turkey) to maintain the body temperature in the range of 37°C ± 1°C during ischemia and reperfusion periods. The trachea and the left carotid artery were cannulated for artificial respiration and the measurement of arterial blood pressure, respectively (blood pressure transducer, SS 13 L; Biopac Systems, Goleta, California). A standard limb lead II electrocardiogram (ECG) and arterial blood pressure were recorded and monitored throughout the experimental period (data acquisition system MP35; Biopac System; Figure 1). Thoracotomy was performed by cutting the fourth and fifth ribs on the left side of the chest. The animal respirator was started using room air to provide artificial ventilation (60 strokes/min at a tidal volume of 1.5 mL/100 g; SAR 830; Life Science, California). The pericardium was incised, and then the hearts were gently exteriorized. A 5/0 silk suture was passed around the left anterior descending (LAD) coronary artery approximately 2 to 3 mm from its origin. The heart was then replaced and allowed to stabilize for 10 minutes. During this period, rats with a sustained decrease in mean arterial blood pressure (MABP) values below 70 mm Hg or ventricular arrhythmias prior to the ligation were excluded. After heart rate (HR) and blood pressure stabilization, a slip loop was made using the loose ends of the previously placed silk suture. The coronary artery occlusion was induced by ligation of LAD with the slip loop for 6 minutes. The slip loop was then loosened by pulling a loose end of the loop to permit reperfusion.

Original electrocardiogram (ECG) recordings and arterial blood pressure tracings (recorded with speed 80 mm/s) from a control anesthetized rat (A), a CBD-treated rat (B), a DPCPX-treated rat (C), and a CBD- and DPCPX-treated rat (D). Ventricular fibrillation (VF) can be seen in sample (A), ventricular premature contraction (VPC) can be seen in both samples (B) and (D), and ventricular tachycardia (VT) can be seen in sample (C). CBD indicates cannabidiol; DPCPX, 8-cyclopentyl-1,3-dipropylxanthine.
The heart was removed and cannulated through the aorta following the termination of the 6 minutes of reperfusion period. In order to wash out the coronary vessels, the heart was subjected to retrograde perfusion with 10 mL of saline solution at 37°C. Following this, the heart was perfused with 2 mL of 96% ethanol to specify the zone at risk, followed by reocclusion of the left coronary artery. The nonischemic zone of the heart was thoroughly perfused with ethanol and appeared white in color. The zone that was not perfused with ethanol was defined as the area at risk and remained red in color (the original tissue color). The zone at risk was separated from the rest of the heart by cutting along the border between these 2 zones. Finally, the total ventricle and zone at risk were weighed; the zone at risk was measured as the percentage of total ventricle weight. 24
Various results were seen in all rats for which a successful coronary artery occlusion had been performed. This included ST-segment elevation and increased QRS amplitude on ECG, a 20% to 40% reduction in arterial blood pressure compared to the preischemic values, and zone at risk values greater than 40%. The reversal of ischemia-induced ST-segment changes and the recovery of MABP were observed in all rats, which had undergone successful reperfusion. A total of 9 animals were omitted on the basis of these criteria.
Experimental Groups and Drug Treatment
Four separate experimental groups were designed in the following way: (1) vehicle control, (2) CBD (50 µg/kg), (3) 8-cyclopentyl-1,3-dipropylxanthine (DPCPX), a selective adenosine A1 receptor antagonist (100 µg/kg), and (4) CBD followed by DPCPX.
Cannabidiol was purchased from Enzo-Life Sciences (No: ALX-430-152, Farmingdale, New York). The DPCPX was purchased from Sigma Chemical Co (No: C101, St Louis, Missouri). Drugs containing solutions were prepared daily by dissolving the drugs with dimethyl sulfoxide (DMSO). Cannabidiol in a dose of 50 µg/100 µL/kg and DPCPX in a dose of 100 µg/100 µL/kg were given iv through the femoral vein; this was carried out 10 and 15 minutes before the coronary artery occlusion, respectively. An amount of DMSO 100 µL/kg was given to rats in the control group, both 10 and 15 minutes before the coronary artery occlusion. The doses of CBD and DPCPX were based on the previous studies. 11,25
Data Analyses
By using a data acquisition system, ECG and blood pressure recordings were analyzed to determine the MABP and HR parameters at regular intervals throughout the ischemia and reperfusion periods (MP35; Biopac System). In accordance with the Lambeth Conventions, arrhythmias were identified during the ischemia and reperfusion periods as ventricular fibrillation (VF), ventricular tachycardia (VT), and other types of arrhythmias (ventricular premature contraction [VPC]) including bigeminy, salvos, and single extrasystoles 26 (Figure 1). A grade was given to each animal as an index of the severity of arrhythmias (arrhythmia score) according to a scale as follows 27 : 0—no arrhythmia; 1—in the absence of VF, the duration of VT and/or VPC is shorter than 10 seconds or equal to 10 seconds; 2—in the absence of VF, the duration of VT and/or VPC is between 11 and 30 seconds; 3—in the absence of VF, the duration of VT and/or VPC is between 31 and 90 seconds; 4—the duration of reversible VF is shorter than 10 seconds or equal to 10 seconds and/or the duration of VT and/or VPC is between 91 and 180 seconds; 5—the duration of VF is longer than 10 seconds and/or the duration of VT and/or VPC is longer than 180 seconds and 6—irreversible VF. For all groups, measurements were taken for the durations and the incidence of arrhythmic attacks and the mortality. The ECG traces were further analyzed, and QT and QRS intervals of an average of 5 consecutive beats were measured prior to and during the ischemic period at 1, 3, and 5 minutes of ligation (Figure 2A).
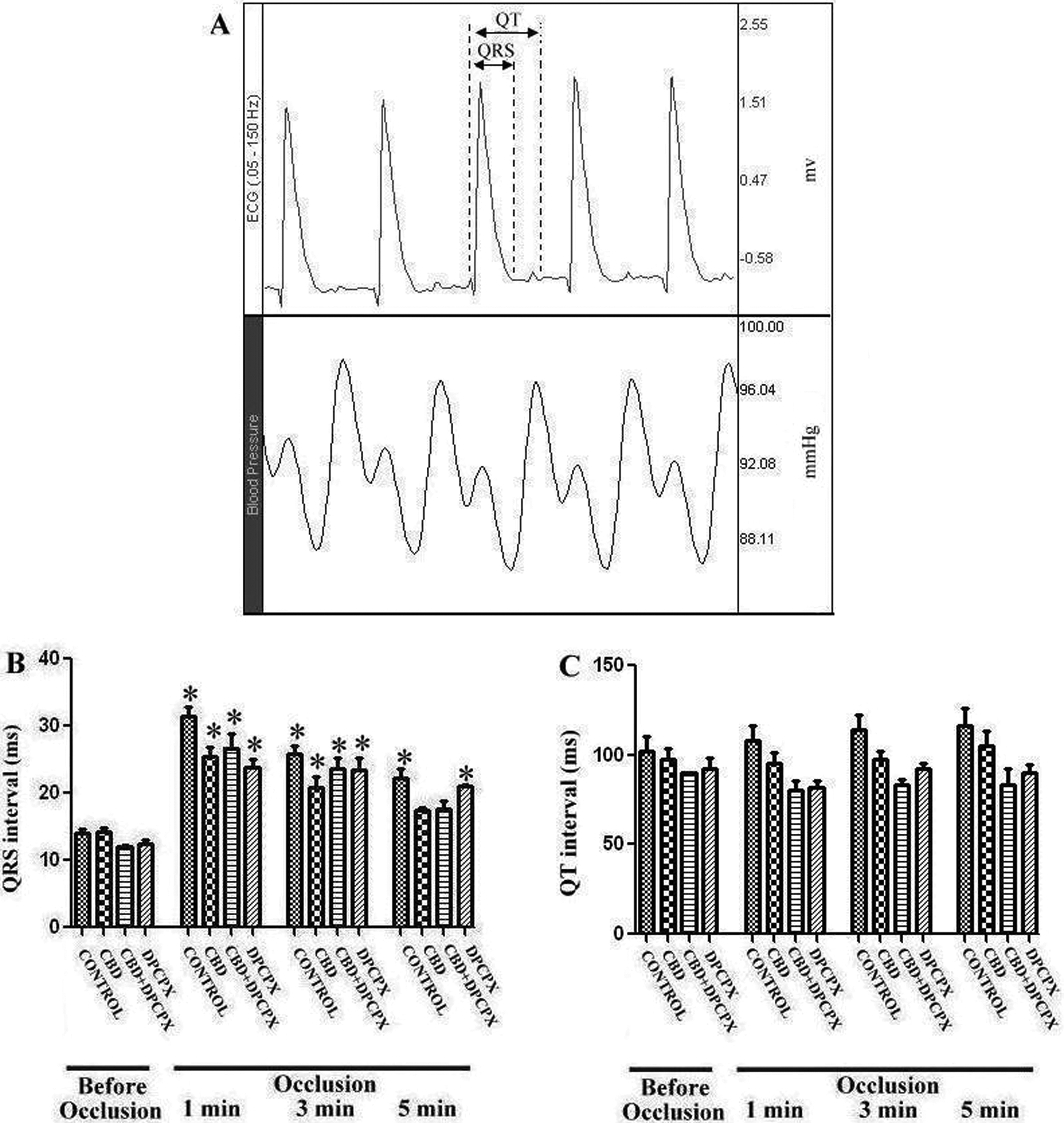
An original electrocardiogram (ECG) recording from a control anesthetized rat (A). Effect of CBD, DPCPX, and CBD and DPCPX treatments on QRS (B) and QT (C) intervals (average of 5 beats) before and during coronary artery occlusion in anesthetized rats. *P < .05: compared with preischemic values. Values represent mean ± standard error (SE) of n = 7 to 10 animals/group. CBD indicates cannabidiol; DPCPX, 8-cyclopentyl-1,3-dipropylxanthine.
Statistical Analyses
Data were analyzed using GraphPad Prism version 5 (GraphPad Software, La Jolla, California). Fischer exact test was performed for statistical analyses of mortality and the incidence of arrhythmias. All other data were expressed as mean ± standard error. As the numbers of animals were different in the groups, the nonparametric Kruskal-Wallis test with Dunn post hoc test was used to compare drug-treated groups with control for all parameters excluding the mortality and the incidence of arrhythmias. The QRS and QT interval values in various time point of the ligation were also compared with preocclusion values using the Kruskal-Wallis test with Dunn post hoc test. Changes in P values of less than .05 were considered to be significant.
Results
Hemodynamic Parameters
Table 1 summarizes the effect of drug treatments prior to and during the ischemia and reperfusion periods. Characteristically, MABP fell immediately following the ligation in all groups by approximately 20% to 30% compared to preischemic values. It also recovered and approached the preischemic values at 5 minutes of the reperfusion period (Table 1). Drug treatments did not affect MABP and HR values when compared with the control group at any time point prior to ischemia and during the ischemia and reperfusion periods (Table 1).
The Mean Arterial Blood Pressure (MABP) and Heart Rate (HR) During 6 Minutes of Ischemia and Reperfusion.a

Abbreviations: lig, ligation; rep, reperfusion; basal, before the ligation; CBD, cannabidiol; DPCPX, 8-cyclopentyl-1,3-dipropylxanthine; SE, standard error.
a Values represent mean ± SE, n = 7-9.
Arrhythmias During Ischemia and Reperfusion
The weights of the animal (not shown) and the zone at risk were not significantly different between the groups (Table 2). The ligation of the LAD resulted in the generation of ventricular arrhythmias, the majority occurred as VPC. Drug treatments did not affect the duration of any type of arrhythmias when compared with the control in this period (data not shown).
The Effects of Drug Treatments on the Incidence and the Duration of Arrhythmias During 6 Minutes of Reperfusion.a

Abbreviations: VF, ventricular fibrillation; VT, ventricular tachycardia; VPC, ventricular premature contraction; CBD, cannabidiol; DPCPX, 8-cyclopentyl-1,3-dipropylxanthine; SE, standard error; N, the number of animals just before the reperfusion; N, the number of dead animals after 6 minutes of reperfusion; n, the number of animals experienced arrhythmias.
a Values represent mean ± SE.
b P < .05: compared with control group.
The reperfusion of the myocardium resulted in more severe arrhythmias in the control group than those developing during the ischemia, as expected. Arrhythmias appeared in between 1 and 15 seconds of the reperfusion period in all groups; this varied from VPC, VT to VF. The DPCPX treatment did not significantly affect the arrhythmia score, the incidence, and the duration of any type of arrhythmias when compared with the control group. Cannabidiol administration alone decreased the arrhythmia score, the incidence, and duration of VT and the total length of arrhythmias in comparison to vehicle-treated control animals (arrhythmia scores: CBD, 2.2 ± 0.4; vs control, 4.0 ± 0.4; P < .05; Table 2, Figure 3; total length of arrhythmias: CBD, 21 ± 5 s vs control, 80 ± 22 s; P < .05; Table 2, Figure 4). However, the coadministrated CBD with DPCPX did not decrease the arrhythmia score, the incidence and duration of any type of arrhythmias during 6 minutes of reperfusion (Figure 3 and Figure 4).
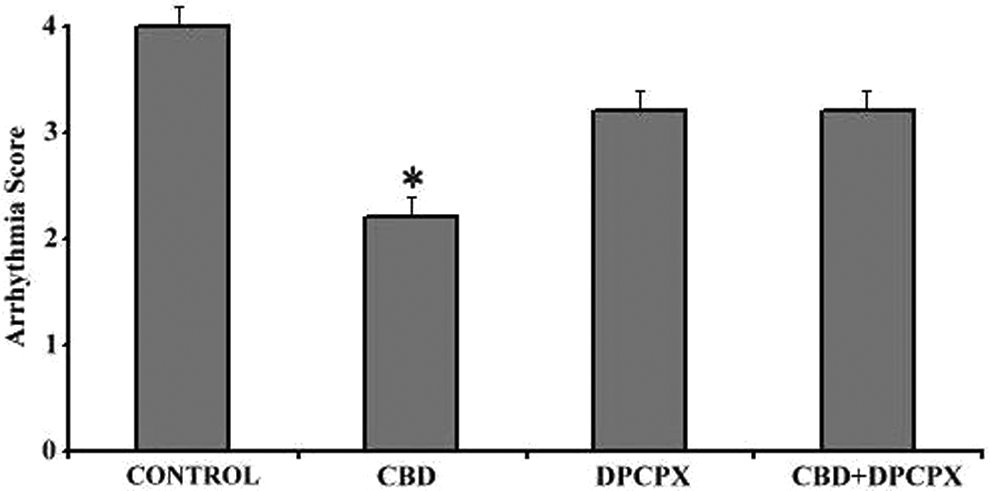
The effect of drug treatments on the arrhythmia score during 6 minutes of reperfusion. Values represent mean ± standard error (SE). *P < .05: compared to control.

The effect of drug treatments on the total length of arrhythmias during 6 minutes of reperfusion. Values represent mean ± standard error (SE). *P < .05: compared to control.
The Effect of Drug Treatments on QT and QRS Intervals
The QRS interval widened immediately after the ligation. These values in all groups were significantly longer in comparison to preischemic values at 1 and 3 minutes of the occlusion period. However, the increment in QRS interval gradually decreased in all groups, and the lengths of QRS interval approached the preischemic values at 5 minutes of the occlusion period (Figure 2B). The QT interval did not significantly increase, compared with the preischemic value during the ischemic period (Figure 2C). Any drug treatments affect neither QT nor QRS intervals prior to and during the ischemic period (Figure 2B and C).
Discussion
The novel finding from the present study is that the treatment of CBD in a bolus 50 µg/kg dose suppresses reperfusion-induced ventricular arrhythmias. The present study demonstrates for the first time that CBD has an antiarrhythmic effect on the reperfusion-induced arrhythmias. There is only 1 study that reveals the effect CBD on ventricular arrhythmias to this date. 11 In this comparable study, the same dose of CBD was used to suppress ischemia-induced ventricular arrhythmias in anesthetized rats. However, it was not found to be effective in decreasing the number of ventricular arrhythmias during the reperfusion period. The discrepancy between the present and the comparable results seems to depend on the different duration of ischemic periods prior to the reperfusion period in these studies. The 30 minutes of ischemia in the comparable study did not produce a significant number of ventricular arrhythmias in control animals to test the effect of CBD on reperfusion-induced arrhythmias. In the research using the ischemia–reperfusion arrhythmia model in rat, the ischemic period has been generally taken 5, 6, or 7 minutes prior to the reperfusion period to evaluate the effect of drugs on reperfusion-induced arrhythmias. 24,28,29 The present study was also specifically designed to research the effect of CBD on reperfusion-induced arrhythmias. Therefore, the duration of ischemic period was chosen as 6 minutes that produced significant amount of reperfusion arrhythmias in our previous studies. 30,31
In the present study, CBD administration did not affect both the HR and the MABP prior to and during the ischemia and reperfusion periods in thiopental-anesthetized rats (85 mg/kg). This result is not consistent with the previous comparable study in which CBD was administrated at a dose of 50 µg/kg as given in the present study. 11 In this study, the bolus administration of CBD prior to and during the ischemic period significantly decreased the MABP values in pentobarbital-anesthetized rats (60 mg/kg). The different types of anesthesia used in these studies provide a possible explanation for the discrepancy in these results.
Extracellular adenosine concentration increases due to the adenosine triphosphate (ATP) metabolism following the myocardial ischemia. 32 In an isolated rat heart study, it was suggested that the endogenous adenosine accumulation during the ischemia has an antiarrhythmic effect through the activation of adenosine A2A receptors. 33 However, in this study, adenosine A1 receptor blockage with DPCPX did not affect the occurrence of arrhythmias in acute ischemic myocardium. In the present study, DPCPX at a dose of 100 µg/kg did not significantly affect the incidence and duration of I/R-induced arrhythmias. These results are consistent with a recent report by Bozdoğan et al who revealed that DPCPX at a dose of 10 µg/kg did not affect the occurrence of arrhythmias in the same model. 34 In contrast to these findings, Lee et al found that a blockade of adenosine A1 receptors with DPCPX at a dose of 500 µg/kg increased the occurrence of arrhythmias during 30 minutes of ischemia in anesthetized rats. 35 The discrepancy in these results may depend upon the different doses of DPCPX (100 vs 500 µg/kg) or the difference in the periods during which the effect of DPCPX on arrhythmias was observed (ischemic period vs reperfusion period). The present results support the notion that endogenously released adenosine does not significantly affect the occurrence of ventricular arrhythmias via the activation of adenosine A1 receptor.
The underlying mechanism of the antiarrhythmic effect of CBD may depend on its direct electrophysiological effect. Cannabidiol has been reported to inhibit the slow component of delayed rectifying potassium channels (IKs) in guinea pig isolated ventricular myocytes. 36 The IKs blockers prolong the cardiac action potential duration and QT interval and suppress electrically induced ventricular tachyarrhythmias in animals during acute coronary occlusion. 37 However, it was reported that in the rat ventricular myocytes, the transient outward (Ito) and the inwardly rectifying (IK1) potassium current are responsible for repolarization process, and the delayed rectifying outward potassium current (IK) has only a negligible effect on repolarization process. 38 We cannot find any data in the literature about the effect of CBD on Ito and IK1. We nevertheless measured the QT and QRS intervals to address the possible involvement of the electrophysiological effects of CBD in its antiarrhythmic effect. However, ECG analyses reveal that CBD administration did not increase the QT and QRS intervals, which is consistent with the previous report by Walsh et al. 11 The QRS intervals increased in the ischemic period compared with the preischemic value that we would expect; the slow conduction in the ischemic myocardium could be the reason for this prolongation. Walsh et al proposed that the antiarrhythmic effect of CBD in the ischemic period may be mediated through an inhibitory effect on platelet activation. 11 In their following studies, the same researchers reveal that the antiarrhythmic effect of CBD may not be mediated through the CBD1 receptor activation during the ischemia. 39
In the present study, although CBD alone suppressed I/R-induced ventricular arrhythmias, it was not found to be effective against I/R-induced arrhythmias in the presence of adenosine A1 receptor blockage with DPCPX. These results reveal that the antiarrhythmic effect of CBD may be mediated through the adenosine A1 receptor activation. Cannabidiol inhibits the cellular uptake of adenosine by acting as a competitive inhibitor of ENT. 15 Therefore, in the present study, CBD may have increased the interstitial concentration of adenosine and the enhanced adenosine signaling through the inhibition of adenosine uptake as in the previous study. 15 Cannabidiol may have revealed its antiarrhythmic effect through the adenosine A1 receptors activation, which is provided by the enhanced adenosine signaling. It has been proposed that the antiarrhythmic mechanism of the adenosine A1 receptor activation depends upon the myocardial ATP-dependent potassium (KATP) channels activation. 40,41 This might provide homogeneity between ischemic and nonischemic myocardial regions and/or the preservation of mitochondrial energy production. 42 In previous studies, the nucleoside transport inhibitor drugs, which may increase extracellular adenosine concentration and adenosine signaling, have been shown to possess antiarrhythmic effects. 43,44 These findings support and fall in line with our proposal for the underlying mechanism of the antiarrhythmic effect of CBD.
Conclusion
To our knowledge, the present results reveal for the first time that CBD has an antiarrhythmic effect against I/R-induced arrhythmias. The antiarrhythmic effect of CBD seems to be mediated through the adenosine A1 receptor activation.
As CBD is well tolerated in humans, 4 it may be a potential candidate for the treatment of I/R-induced ventricular arrhythmias. However, further studies are needed to predict its potential therapeutic use. As drug treatment in the ischemic period before reperfusion is more applicable to the clinical situation of I/R-induced ventricular arrhythmias than that of preischemic treatment, the effect of the CBD treatment during the course of ischemic state on I/R-induced arrhythmias should be researched. The chronic use of CBD in patients with coronary artery disease may cause adenosine receptor desensitization, which may abort its potential antiarrhythmic effect. Therefore, the long-term effect of CBD on adenosine receptors should also be determined.
Footnotes
Authors’ Note
This study was performed in the Biology Department of the Faculty of Arts and Sciences, Bülent Ecevit University, Zonguldak, Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research fund grant from Bülent Ecevit University (BAP No:2013-84906727-10).