
Abstract
The effects of angiotensin receptor blocker, diuretic, a calcium antagonist, and their combination were evaluated on the progression of cardiovascular and renal damage in spontaneously hypertensive rats (SHRs) given excess salt. To this end, 8-week male SHRs were divided into 7 groups. The control group (C) received normal NaCl (0.6%) diet. All other groups were given 8% NaCl rat chow. In addition, group 2 was given placebo (tap water alone), group 3 the angiotensin receptor antagonist telmisartan (10 mg/kg per d), group 4 received the diuretic chlorothiazide (80 mg/kg per d), group 5 was given telmisartan plus the diuretic, group 6 was given the calcium antagonist amlodipine (10 mg/kg per d), and group 7 was given telmisartan plus amlodipine. All treatments lasted for 8 weeks. Compared with controls, mean arterial pressure (MAP), renal blood flow, coronary flow reserve, minimal coronary vascular resistance, diastolic time constant, and maximal rate of ventricular pressure fall were all adversely affected by salt loading. Increased left ventricular mass with marked cardiac fibrosis was also found in the salt-overloaded SHR group. Telmisartan normalized all indices except MAP, whereas diuretic and amlodipine only partially restored cardiac functional and mass indexes. Combination therapy with telmisartan and either diuretic or amlodipine also normalized all indices including arterial pressure. These data suggest that (1) cardiovascular damage induced by excess salt in the SHRs was not pressure dependent; (2) compared with the calcium antagonist and diuretic, blockade of angiotensin receptors was extremely effective in this model.
Keywords
Numerous experimental and clinical studies indicate that excess salt, in addition to arterial pressure increase, induces severe cardiovascular and renal injury. 1 -5 In our studies, this was evidenced by marked ventricular fibrosis and structural myocardial damage associated with impaired coronary hemodynamics and left ventricular function, as well as marked proteinuria, decreased effective renal blood flow, and glomerular filtration rate in salt-loaded spontaneously hypertensive rats (SHRs). 6 -9 Moreover, our renal micropuncture studies demonstrated impaired glomerular dynamics manifested by increased glomerular hydrostatic pressure, massive proteinuria, and glomerular and arteriolar damage. 8 We have suggested that these salt-induced cardiovascular and renal injuries were mediated through local tissue renin–angiotensin systems (RAS). 9,10 This was further supported by the finding that AT1 receptor blockade with candesartan attenuated adverse cardiovascular and renal effects of excess salt in SHRs without affecting arterial pressure. 9
Classically, formation of angiotensin II in circulating blood is a crucial event in the mechanism of RAS actions. However, renin has long been suggested to also exert some actions independent of the classical RAS. It is now well established that angiotensin II is also formed locally, in various tissues, thereby exerting its actions independent of the circulating RAS. 11,12 Therefore, since circulating RAS is inhibited in salt-loaded rats, this model permits the examination of the role of local tissue RAS in mediating cardiovascular and renal injury.
Thus, the purpose of this study was to examine the effects of blockade of RAS components on the development of myocardial hypertrophy, left ventricular dysfunction, cardiac fibrosis, and renal injury in a rat model with hypertensive cardiovascular damage that was exacerbated by dietary salt excess. To this end, this study was designed to determine the efficacy of the angiotensin II type 1 receptor blocker telmisartan in the prevention of pressure increase and development of target organ damage from high dietary salt intake. As already stated, we have demonstrated previously that another angiotensin II receptor blocker, candesartan, exerted beneficial effects in this model. 9 Therefore, the purpose of this study was to examine whether structurally different angiotensin II receptor blockers exerted similar effects and in this way, demonstrate that the effect depended on receptor blockade and not on their other possible effects. Furthermore, our study also reexamined and demonstrated earlier finding that angiotensin II receptor blockade prevented salt-induced cardiovascular injury independently of arterial pressure changes.
We therefore proposed to examine the efficacy of telmisartan in combination with a diuretic and a calcium antagonist in preventing salt-induced cardiovascular and renal damage, since they are one of the most often used combinations in clinical practice.
Materials and Methods
Animals
Male, 7-week-old, SHRs were purchased from Harlan Laboratories (Indianapolis, Indiana) and were maintained in a temperature- and humidity-controlled room with a 12-hour light–dark cycle. All rats were handled in accordance with National Institute of Health guidelines; and our Institutional Animal Care and Use Committee approved the study protocol in advance.
Experimental Protocol
At 8 weeks of age, rats weighing 180 to 200 g, were divided randomly into 7 groups, with 12 rats in each. The first (control) group received no treatment and was given standard diet, containing 0.6% NaCl, with tap water ad libitum. All other groups were given rat chow containing 8% NaCl and tap water. All diets were obtained from Harlan-Teklad (Madison, Wisconsin). The second group was given inert vehicle (water). The third group was given the angiotensin II, type 1, receptor blocker telmisartan in drinking water. Concentration of telmisartan in water was adjusted for each rat so that they ingested approximately 10 mg/kg of telmisartan daily. The fourth group was given the diuretic chlorothiazide (80 mg/kg per d) by gastric gavage. Rats in the fifth group were given telmisartan and the diuretic. The sixth group was given the calcium antagonist amlodipine (10 mg/kg per d) by gavage, and the seventh group was given telmisartan and amlodipine.
All rat groups received their respective treatments for 8 weeks. Body weight was measured weekly in all rats. Arterial pressure, left ventricular (LV) function, cardiovascular mass indices, and the extent of cardiac fibrosis were examined at the end of the 8-week study.
Two rats in the second group died during the treatment with signs of heart failure. Technical failure was encountered in a few rats during determination of hemodynamics and heart function so that the final number of rats per group ranged from 8 to 12.
Systemic and Regional Hemodynamics and Left Ventricular Function
At the end of the study, all rats were anesthetized with pentobarbital (40 mg/kg, intraperitoneally [ip]) and the right carotid artery was cannulated with a transducer-tip catheter (Micro-Tip 3F, Millar Instrumentsm, Houston, Texas) that was advanced into the left ventricle (LV). A second catheter (PE-50) was placed into the femoral artery. Both catheters were connected to a multichannel recorder (Grass Instrument, West Warwick, Rhode Island) interfaced to an IBM computer with digital data acquisition system (EMKA Technologies Inc, Falls Church, Virginia). 9 Arterial pressure was measured via femoral artery catheter and indexes of left ventricular function, including LV end-diastolic pressure, the diastolic time constant (tau), and maximal rates of pressure rise and fall (dP/dT max and dP/dT min) were determined from the LV pressure tracing. 9 Both indexes of LV diastolic function, maximal rate of pressure decline and diastolic time constant, actually quantify LV isovolumic relaxation and are, therefore, better estimates of active ventricular relaxation than ventricular stiffness. 13
After these measurements were obtained, the Millar catheter was withdrawn and a jugular vein and LV were cannulated with polyethylene catheters (PE-50) for determination of systemic, coronary, and renal hemodynamics as described previously.14–16 Baseline measurements of systemic and regional hemodynamics were obtained by injecting radioactive-labeled microspheres (57Co) into the LV. Cardiac output was measured by the reference sample microsphere method,14–16 and cardiac index was calculated from cardiac output and body weight and expressed as mL/min per kg. Total peripheral resistance index (U/kg) was calculated by dividing the mean arterial pressure (MAP) by the cardiac index. After basal measurements were obtained, maximal coronary vasodilatation was achieved with dipyridamole infusion (4 mg/kg per min, intravenously for 10 minutes). 17 These hemodynamic studies were repeated using a second microsphere radionuclide (113Sn). At the end of each study, the rat was killed by pentobarbital overdose; and, immediately thereafter, the heart, lungs, liver, brain, kidneys, and samples of skeletal muscle were removed. After cardiac removal, the atria were dissected free from the ventricles and discarded, and the free wall of the right ventricle was separated carefully from the LV (the septum remaining with LV). Tissue samples, as well as blood reference samples, were placed in plastic vials and radioactivity counted in a gamma counter (2470 Wizard, PerkinElmer, Waltham, Massachusetts) with a multichannel analyzer. Organ blood flows were calculated by multiplying the fractional distribution of radioactivity to each organ by cardiac output and were normalized for wet weight (mL/min per g). Coronary flow reserve was calculated as the difference between flows during the baseline and dipyridamole infusion periods. Organ vascular resistances were calculated by dividing MAP by the respective organ flow and were normalized for organ weight and expressed as U/g. Minimal coronary vascular resistance is defined as that vascular resistance achieved by dipyridamole. The data obtained in any particular rat were discarded completely if either the fractional distribution of radioactivity to the lungs was greater than 5%, suggesting arteriovenous shunting 18 or if the difference in radioactivity between the 2 kidneys was greater than 15%, suggesting uneven distribution of the 2 microsphere injections. 14,15
Left Ventricular Collagen Concentration
As an estimate of ventricular collagen content, hydroxyproline concentration was determined for the left and right ventricular samples, as previously described 16 and was expressed as mg/g of dry weight.
Statistical Analysis
Analysis of variance (ANOVA) and Student-Newman-Keuls post hoc tests were employed to test for significant differences between groups. 19 All values are expressed as the mean ± 1 standard error of the mean (SEM). A 5% confidence level was considered to be of statistical significance.
Results
Body and Ventricular Weights and Myocardial Hydroxyproline Concentration
Body weight was found to be significantly (P < .05) reduced in SHRs given excess salt, and the various therapies completely or partially restored body weight (Figure 1). Left ventricular mass was significantly (P < .05) greater in salt-loaded SHRs; and the various therapies only partially restored LV weight index, whereas combination therapy with telmisartan and amplodipine reduced LV mass to control level (Figure 1). Right ventricular mass was increased (P < .05) in SHRs given high salt diet (HS) and all therapeutic regimens restored it to control level (Figure 1). Collagen, as estimated by LV hydroxyproline concentration, increased (P < .05) in salt-loaded SHRs, and this was not affected with either diuretic or amlodipine when given alone but was prevented by telmisartan, either alone or in combination with the diuretic and amlodipine (Figure 1).

Body and ventricular weights and LV hydroxyproline concentration. LV indicates left ventricle; RV, right ventricle; SEM, standard error of the mean; SHRs, spontaneously hypertensive rats; group C, control SHRs given regular salt diet; group P, SHRs given high salt diet (HS; 8%); group T, SHRs given HS and telmisartan (10 mg/kg per d); group D, SHRs given HS and diuretic (chlorothiazide 80 mg/kg per d) by gastric gavage; groups T + D, SHRs given HS, telmisartan, and diuretic; group A, SHRs given HS and amlodipine (10 mg/kg per d) by gastric gavage; T + D, SHRs given HS, telmisartan, and amlodipine. Values are mean ± 1 SEM. At least 8 rats per group. # P < .05 when compared to C; *P < .05 when compared to HS.
Systemic Hemodynamics
Mean arterial pressure increased significantly (P < .05) in SHRs given HS; it was reduced to the control level by either amlodipine or telmisartan in combination with diuretic or amlodipine but was not affected by telmisartan or the diuretic given alone. No difference in cardiac index and heart rate was noted between the groups (Figure 2). Similar to the arterial pressure, total peripheral resistance was increased (P < .05) in salt-loaded rats and this was not affected by telmisartan or diuretic given alone but was reduced to control level by either amlodipine alone or telmisartan given in combination with diuretic or amlodipine.
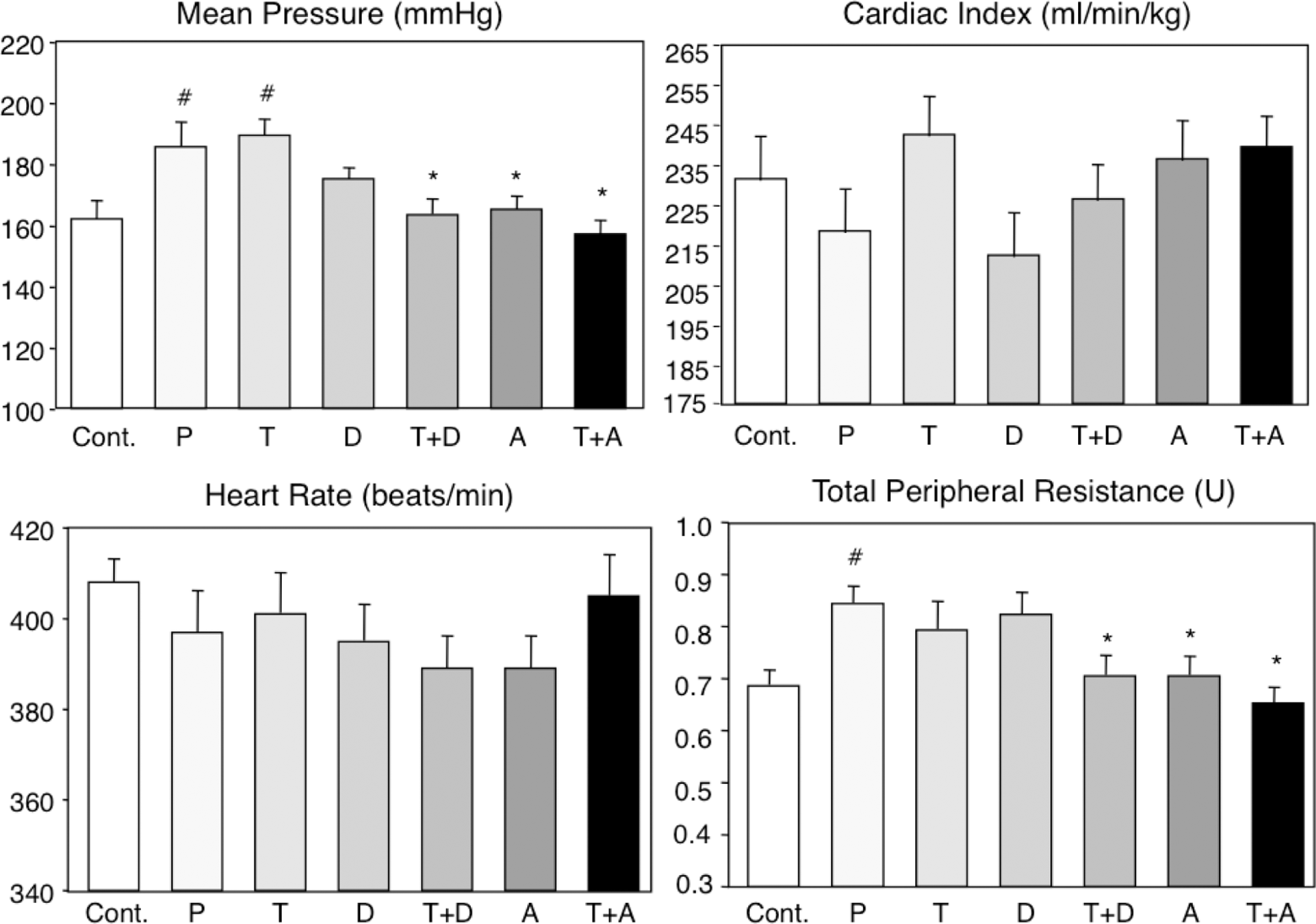
Systemic hemodynamics. SEM indicates standard error of the mean; SHRs, spontaneously hypertensive rats; group C, control SHRs given regular salt diet; group P, SHRs given high salt diet (HS; 8%); group T, SHRs given HS and telmisartan (10 mg/kg per d); group D, SHRs given HS and diuretic (chlorothiazide 80 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and diuretic; group A, SHRs given HS and amlodipine (10 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and amlodipine. Values are mean ± 1 SEM. At least 8 rats per group. # P < .05 when compared to C; *P < .05 when compared to HS.
Coronary Hemodynamics
Basal coronary blood flows as well as coronary vascular resistances were not different between the groups (Figure 3). On the other hand, when compared with rats on regular diet, coronary flow reserve was greatly (P < .05) reduced in SHRs given excess salt. Therapy with telmisartan or combination of telmisartan with diuretic or amlodipine restored coronary flow reserve to control values. Diuretic or amlodipine given alone only partially improved flow reserve. Minimal coronary vascular resistance was significantly (P < .05) increased in SHRs given excess salt; all treatments restored minimal vascular resistance to control values.

Coronary hemodynamics. SEM indicates standard error of the mean; SHRs, spontaneously hypertensive rats; group C, control SHRs given regular salt diet; group P, SHRs given high salt diet (HS; 8%); group T, SHRs given HS and telmisartan (10 mg/kg per d); group D, SHRs given HS and diuretic (chlorothiazide 80 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and diuretic; group A, SHRs given HS and amlodipine (10 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and amlodipine. Values are mean ± 1 SEM. At least 8 rats per group. # P < .05 when compared to C; *P < .05 when compared to HS.
Renal Hemodynamics
When compared with rats on regular diet, basal renal blood flow was greatly (P < .05) reduced and the renal vascular resistance significantly (P < .05) increased in rats given excess salt; all therapies greatly improved these 2 variables (Figure 4). Renal flow reserve was significantly (P < .01) reduced in SHRs on HS and all therapies restored it. Similarly, minimal renal vascular resistance was greatly increased in rats given excess salt and this was prevented by all therapies.

Renal hemodynamics. SEM indicates standard error of the mean; SHRs, spontaneously hypertensive rats; group C, control SHRs given regular salt diet; group P, SHRs given high salt diet (HS; 8%); group T, SHRs given HS and telmisartan (10 mg/kg per d); group D, SHRs given HS and diuretic (chlorothiazide 80 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and diuretic; group A, SHRs given HS and amlodipine (10 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and amlodipine. Values are mean ± 1 SEM. At least 8 rats per group. # P < .05 when compared to C; *P < .05 when compared to HS.
Indexes of Heart Function
No differences in left ventricular end-diastolic pressure (LVEDP) and maximal rate of pressure rise were observed among groups (Figure 5). Maximal rate of pressure decline was greatly (P < .01) decreased in SHRs given excess dietary salt; this was completely restored by telmisartan either alone or in combination with diuretic and amlodipine. Similarly, the diastolic time constant was increased (P < .01) by excess salt; completely restored by telmisartan or combination therapy; and partially restored by diuretic or amlodipine alone.
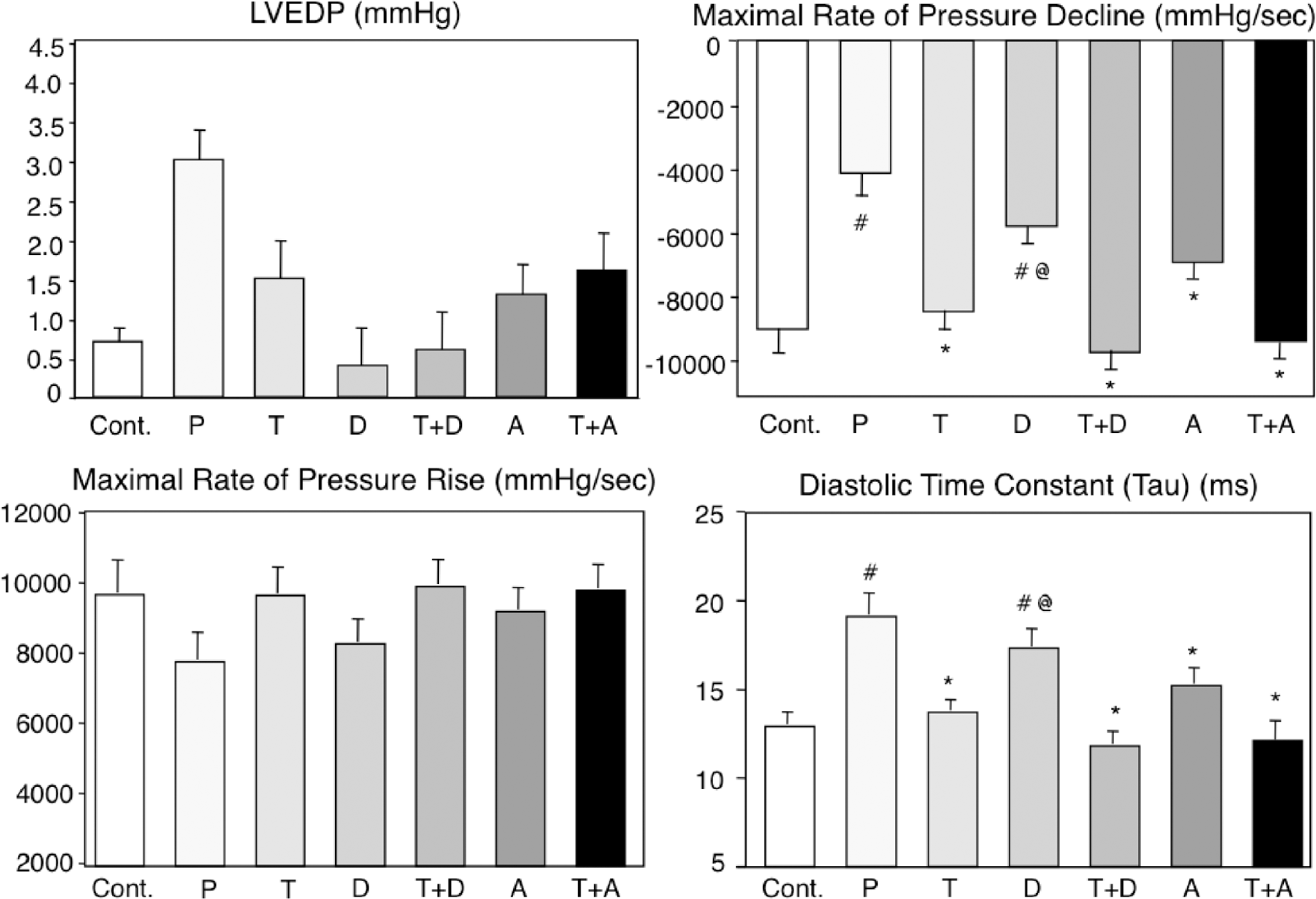
Indexes of heart function. LVEDP indicates left ventricular end-diastolic pressure; SEM, standard error of the mean; SHRs, spontaneously hypertensive rats; group C, control SHRs given regular salt diet; group P, SHRs given high salt diet (HS; 8%); group T, SHRs given HS and telmisartan (10 mg/kg per d); group D, SHRs given HS and diuretic (chlorothiazide 80 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and diuretic; group A, SHRs given HS and amlodipine (10 mg/kg per d) by gastric gavage; group T + D, SHRs given HS, telmisartan, and amlodipine. Values are mean ± 1 SEM. At least 8 rats per group. # P < .05 when compared to C; *P < .05 when compared to HS.
Discussion
The presented data conclusively demonstrated that dietary salt excess adversely affected cardiovascular and renal function. Thus, compared with rats on regular salt diet, SHRs exposed to salt overload exhibited increased LV mass and fibrosis, elevated arterial pressure, compromised coronary hemodynamics, and LV diastolic dysfunction.
These findings are well in agreement with the previously published data. 1,2,5 -7 It should be noted that, compared with human beings, especially those taking the highest dietary salt, the salt load in this study is excessive. We choose this high salt load as it produces very consistent cardiovascular injury within a relatively short time span. Lower salt loads also induce cardiovascular and renal injury but to a lesser extent and after longer periods of time. 7
The presented results also clearly revealed that an angiotensin II, type 1 receptor blocker telmisartan, was very effective in preventing the cardiovascular injury and changes in renal hemodynamics in SHRs exposed to dietary excess salt, although it did not lower the arterial pressure. Our previous studies also demonstrated that dietary salt overload induced significant renal damage that could be prevented by a treatment with angiotensin receptor antagonists. 8 -10 The 2 other examined agents, diuretic and calcium antagonist, were far less effective in preventing adverse effects of excess salt when given alone. The combinations of telmisartan and diuretic or calcium antagonist were also very effective in protecting the cardiovascular and renal systems from the adverse effects of salt overload. We have previously demonstrated that another angiotensin II, type 1, receptor antagonists, candesartan and losartan, are also very effective in preventing the foregoing adverse structural and functional effects of excess salt. 9,10,20 Therefore, the findings that 3 structurally different angiotensin receptor blockers exert the same protective effect without affecting arterial pressure demonstrated that these effects were mediated via receptor blockade and not through other possible mechanisms. This was further supported by our recent findings that salt-induced renal injury was mediated by angiotensin receptor activation. 10 There are several angiotensin II receptor blockers that have been approved for treating hypertension. They differ with respect to structure, dosing, metabolism, and elimination. 21 However, their clinical efficacy, at least in treating elevated arterial pressure, appears to be very similar. 21,22 A few exceptions have been reported so far. Thus, candesartan has been demonstrated to be more effective than telmisartan, valsartan, and olmesartan in patients with morning hypertension. 23 Similarly, telmisartan was found to be more effective in reducing proteinuria than losartan in patients with diabetic nephropathy. 24
Another interesting observation of this study was the lack of effect of telmisartan on arterial pressure in salt-loaded SHRs with concomitant prevention of adverse structural and functional cardiovascular effects of excess salt. Similar effects were also observed in salt-loaded, candesartan-treated SHRs. 9,20 On the other hand, the calcium antagonist amlodipine decreased arterial pressure to control level in this study but was far less effective than telmisartan in preventing cardiovascular and renal damage with salt overload. This discrepancy between the effects of various agents on arterial pressure as well as structural and functional damage clearly indicated that pressure was not the sole, or even major, mediator of the adverse effects of excess salt. Moreover, this finding was also noted in SHRs on regular salt diet treated with mineralocorticoid receptor blocker in which minimal reduction in arterial pressure was accompanied with great reduction in LV fibrosis and improvement in LV function. 25 Similarly, left ventricular mass was found to be increased in normotensive Sprague-Dawley rats given high salt diet. 26 Of particular interest are discrepant effects of telmisartan and amlodipine on arterial pressure, LV mass, and LV fibrosis. Thus, telmisartan did not affect arterial pressure, decreased LV mass but not to the control level, and completely prevented LV fibrosis. On the other hand, amlodipine reduced arterial pressure to control value, reduced LV mass but not to the control level, and did not have any effects on LV fibrosis. Thus, it appears that in salt-loaded SHRs the increase in LV mass is mediated by both increased pressure and increased RAS activity, whereas the LV fibrosis resulted from local, cardiac, RAS activation.
In conclusion, these results demonstrated that an angiotensin II, type 1, receptor antagonist telmisartan when, given alone as well as in combination with either a diuretic or a calcium antagonist was extremely effective in preventing adverse cardiovascular effects of dietary excess salt. Furthermore, the presented data indicated that beneficial effects of telmisartan were independent of arterial pressure and that excess salt exerted adverse cardiovascular effects directly, possibly by the activation of local, tissue RAS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported in part by a grant from Boehringer Ingelheim.