
Abstract
Background:
African Americans have greater risk of cardiovascular events than comparator populations of white European origin. A potential reason for this is reduced nitric oxide bioavailability in African Americans, resulting in increased prevalence of factors that contribute to ventricular dysfunction. We investigated the effects of nebivolol with the diuretic hydrochlorothiazide (HCTZ) in hypertensive African Americans with echocardiographic evidence of diastolic dysfunction.
Methods:
A total of 42 African American patients were assigned to nebivolol and HCTZ in an open-label fashion for a 24-week period. Changes in blood pressure (BP), echocardiographic parameters, and success in attaining target BP were determined. As an indirect determinant of endothelial function, serum total nitric oxide (NOx) levels and asymmetric dimethyl arginine (ADMA) levels were performed at baseline and after the treatment period.
Results:
The systolic BP decreased from 150 ± 13 to 136 ± 16 mm Hg (P < .005). Diastolic BP decreased from 94 ± 13 to 84 ± 9 mm Hg (P = .008). Of the patients that completed the study, 77% achieved a combined target BP of systolic BP <140 mm Hg and a diastolic BP <90 mm Hg. Serum NOx increased by 41% and 39% in patients that were treated with 10 mg and 20 mg daily nebivolol, respectively. The ADMA levels decreased by 44% following treatment. The change in systolic BP was strongly correlated to the change in ADMA (r = .54; P = .024). Furthermore, in comparison to a group of age-matched patients controlled with diuretic therapy only, the ADMA levels were significantly lower in the nebivolol posttreatment group (controlled BP with diuretic: 0.32 ± 0.07μmol/L; nebivolol posttreatment: 0.24 ± 0.06 μmol/L; P < .05).
Conclusion:
Reduced BP with nebivolol in hypertensive African Americans and echocardiographic evidence of diastolic dysfunction correlates with improved endothelial function. Furthermore, improvement in endothelial function and increased nitric oxide bioavailability suggests a potential mechanism of efficacy of nebivolol in these patients.
Introduction
Long-term hypertension is often accompanied by an impaired relaxation of the ventricles due to diastolic dysfunction. 1 ,2 The evidence of diastolic dysfunction is associated with a greater risk of the development of heart failure and increased morbidity for cardiovascular diseases. 3,4 Diastolic dysfunction is often present in combination with hypertension and left ventricular hypertrophy. There are multiple antihypertensive agents that have varying degrees of reduction of left ventricular hypertrophy. 5 Over 50% of all patients with hypertension have evidence of diastolic dysfunction, and many of these patients will ultimately develop heart failure, but there is still no targeted therapy. A few studies demonstrated the beneficial effects of angiotensin receptor blockers on diastolic function. 6 –8 However, the recent Valsartan in diastolic dysfunction (VALIDD) study with valsartan versus control detected that despite a decrease in blood pressure (BP), there was no change in overall diastolic function in patients with hypertension and diastolic dysfunction. 9
African Americans have the highest prevalence of hypertension in the world, significantly higher than people of African origin living outside the United States. 10 According to the 2003-2004 National Health and Nutrition Examination Survey (NHANES), hypertension prevalence is 39.1% in African Americans and 28.5% in white Americans. 11 The increased prevalence of hypertension in African Americans has been attributed to both genetic and environmental factors. 12 Persons of black African descent in the Western world have a greater risk of heart failure than comparator populations of white European origin. 13
Low levels of nitric oxide have been observed in people with high BP, particularly among African Americans and may be an important factor in essential hypertension. 14,15 Nebivolol is a highly cardioselective vasodilatory beta1-receptor blocker that lowers BP by reducing peripheral vascular resistance and significantly increases stroke volume with preservation of cardiac output when compared to atenolol, another beta1-receptor blocker. 16 –18
The clinical role of asymmetric dimethyl arginine (ADMA) as a marker of cardiovascular risk can be deduced from an increasing number of clinical studies. These findings demonstrate the presence of a statistically significant and independent relationship between ADMA, endothelial function, and the incidence of major adverse cardiovascular events or death. 19 In patients with essential hypertension, ADMA levels have been shown to be 2-fold higher than those in normotensive controls. 20 Experimental studies have also demonstrated that intra-arterial infusion of ADMA causes local vasoconstriction in the corresponding circulation. 21 Moreover, intravenous infusion of ADMA has been shown to increase total peripheral resistance significantly. 22 These studies confirm previous data from animal experiments and suggest a physiological role for ADMA in the regulation of normal BP and a pathophysiological role for this molecule in hypertension. Other observations have demonstrated a correlation between ADMA levels, endothelial dysfunction, and the presence of LVH. 20
We conducted a prospective study to evaluate the effects of nebivolol plus diuretic therapy in self-described African American participants with stages I to II hypertension. We also made comparisons in a group of patients whose BP was controlled with diuretic therapy to determine whether these effects may be secondary to BP control.
Methods
Study Population
The study was reported to Clinical Trials.gov (NCT00999752), and the protocol was submitted and approved by the local Institutional Review Board. Written informed consent was obtained from all patients. A total of 42 self-described African American patients with stage I or II hypertension were screened and then treated with nebivolol (starting with 5 mg/d and force titrated to a maximum dose of 20 mg/d) for a 24-week period in an open-label manner. Patients were also simultaneously initiated on hydrochlorothiazide (HCTZ) at 25 mg/d and maintained on this dose for the 24-week period.
Inclusion criteria included self-described African American males or females between the age of 18 and 75 years with a diagnosis of hypertension. In addition, to qualify for the study, patients had to exhibit evidence of early diastolic dysfunction. These patients underwent an echocardiogram, and criteria included an E/A ratio (the ratio between early [E] and late atrial [A] ventricular filling velocity) of less than 1.0 plus either a deceleration time (DT) >220 ms or an isovolumic relaxation time (IVRT) >105 ms. Exclusion criteria consisted of patients with poorly controlled diabetes mellitus (glycosylated hemoglobin >8.0%), known coronary heart disease, and/or cerebrovascular disease. In addition, patients with advanced renal dysfunction (defined by a serum creatinine >3.5 mg/dL or creatinine clearance <20 mL/min) were excluded from the study.
Changes in systolic and diastolic BP and success in attaining target BP (systolic BP <140 mm Hg and diastolic BP <90 mm Hg) were the primary end points. Plasma levels of ADMA and tissue Doppler imaging (TDI) by echocardiography were performed at baseline and at week 24. Pill counts were obtained at each visit to determine compliance. The study protocol complies with the Declaration of Helsinki and was approved by the institutional review board before implementation of the study.
Measurement of BP
An Omron sphygmomanometer (Schaumburg, Illinois) was used to measure systolic and diastolic BP. The determinations for BP were made in the morning (no later than 0900 hours) in a fasting state and in a supine position. Patients were asked to refrain from smoking prior to the BP determination. These BP measurements were performed in a consistent manner. Measurements were taken at 5-minute intervals and a total of 3 readings were obtained at each visit. The average of the 3 measurements was calculated for each visit.
Assessment of Diastolic Function by TDI
We determined diastolic function with 2-dimensional ultrasound images using a Philips SONOS 5500 3.5 mHz linear array transducer and a Philips Image Point ultrasound system (Philips, Atlanta, Georgia). Ejection fraction (EF) was calculated and the left ventricular mass index was measured. The LV internal dimension and interventricular septal and posterior wall thickness were measured in end diastole and end systole according to the recommendations of the American Society of Echocardiography. 23 Pulsed wave (PW) recordings of the early diastolic (E) and atrial (A) wave, the E/A ratio, E-wave DT, and IVRT were measured. Measurements at up to 3 cycles were taken and averaged. Imaging data were recorded digitally in the apical 4-chamber view. Volumes were placed at the junction of the LV wall with the mitral annulus of the septal and lateral myocardial segments and 2 mid-ventricular sites in the same walls. The apical four chamber view was used to assess the longitudinal systolic and diastolic function. The tissue imaging analyses were measured both at the lateral and medial parts of the mitral annulus.
Measurement of ADMA Levels
The ADMA is released from proteins that have been posttranstlationally methylated and subsequently hydrolysed and is metabolized by the enzyme dimethylarginine dimethylaminohydrolase (DDAH), which hydrolyses ADMA to dimethylarginine and
The concentration of ADMA was measured in serum samples by using a commercial enzyme-linked immunosorbent assay (ELISA) kit (DLD Diagnostica, Hamburg, Germany). The kit uses an immunoaffinity, highly specific and sensitive rabbit anti-ADMA antibody. The ADMA concentrations obtained and the performance of the ELISA have been found to be consistent with other widely applied methods used to quantify ADMA, such as gas chromatography–mass spectrometry and liquid chromatography–mass spectrometry. 25 In order to verify the production of nitric oxide, the Griess Reaction assay technique was performed to quantify the nitrite concentration in serum. 26 Using a commercial available total nitric oxide (NOx) assay kit (R&D Systems), serum samples were assayed, and NOx levels were measured spectrophotometrically at an absorbance of 548 nm.
Statistical Analysis
All values are presented as the mean ± standard deviation (SD) or standard error of the mean (SEM) for continuous variables and as the percentage of total patients for categorical variables. A 2-sided Student t test was used for comparison of continuous and categorical variables. A P value of <.05 was considered statistically significant, and all P values were 2 sided. Calculations were performed with SPSS software (version 10.0, Statistical Package for the Social Sciences, Chicago, Illinois).
Results
Study Demographics
Forty-two participants were enrolled of which 35 participants (15 males and 20 females) completed the study. The treatment was well tolerated and unwillingness to continue and comply with the protocol was the main reason for participants dropping out of the study. The follow-up of all patients was 100% complete. None of the patients dropped out of the study due to side effects from the treatment. Table 1 shows patient characteristics and baseline demographics for those who completed the study. There was no change in glucose, renal function, or lipid profile during the study.
Study Demographics and Effects of Nebivolol on Metabolic Parameters a
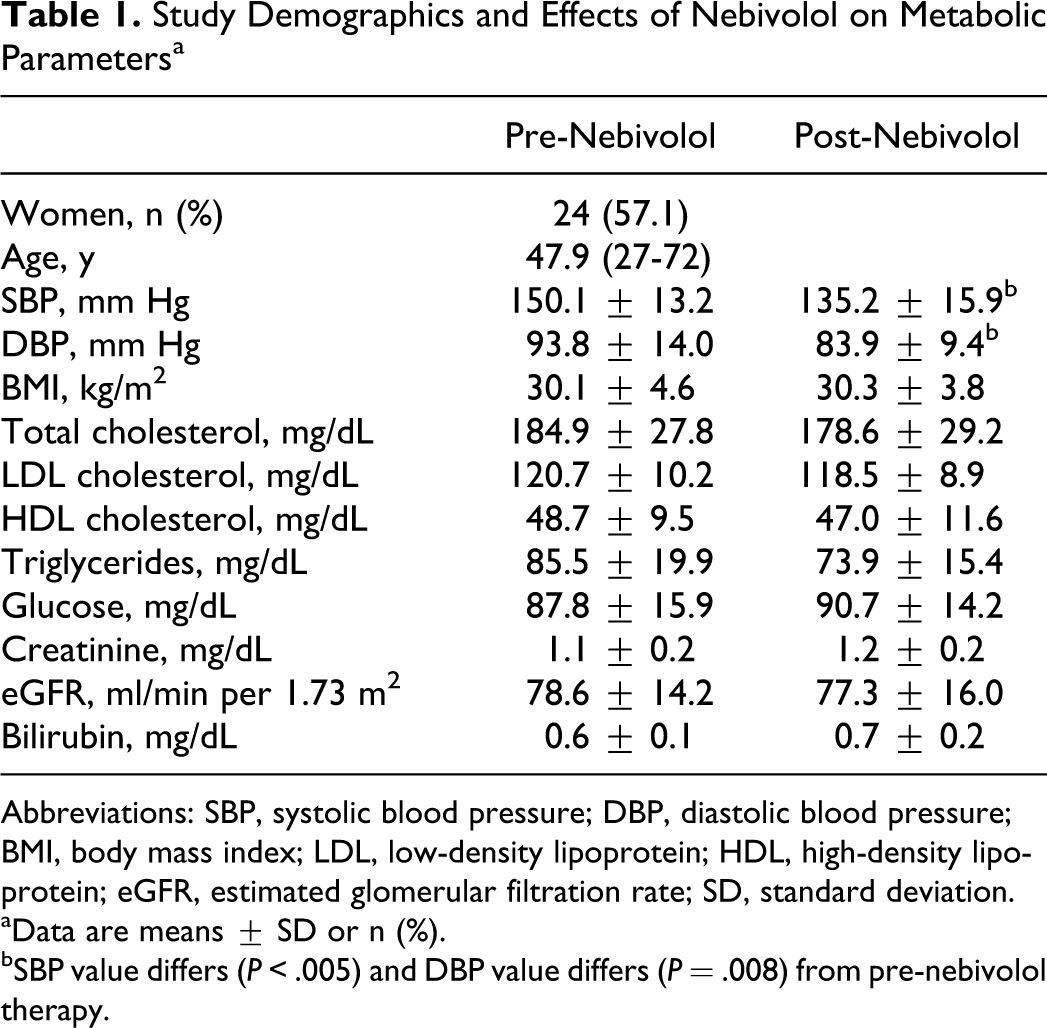
Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; eGFR, estimated glomerular filtration rate; SD, standard deviation.
aData are means ± SD or n (%).
bSBP value differs (P < .005) and DBP value differs (P = .008) from pre-nebivolol therapy.
Analysis of BP With Nebivolol Treatment
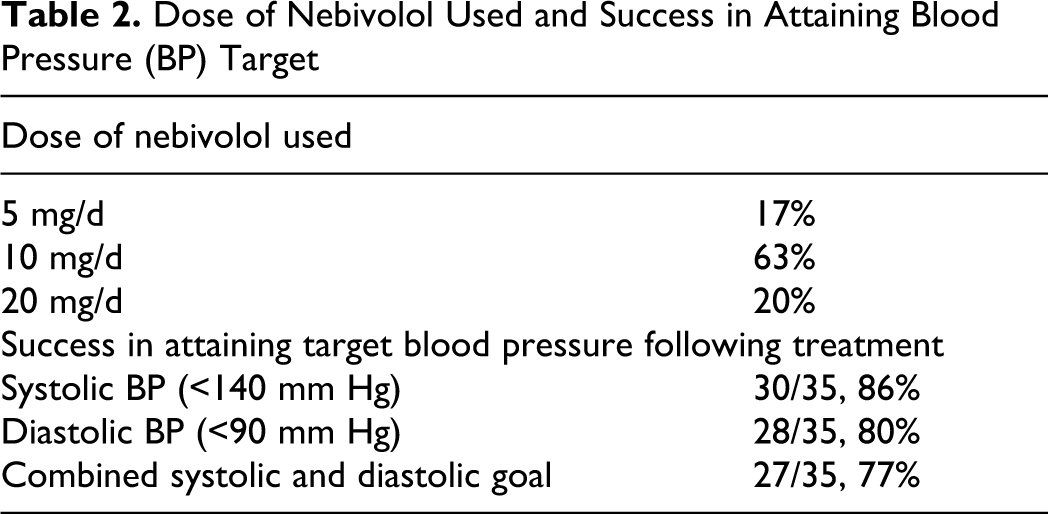
Table 1 displays the SBP and DBP in patients with nebivolol treatment. Mean SBP decreased by 15.1 ± 7.6 mm Hg (P < .005) and DBP decreased by 10.0 ± 6.4 mm Hg (P = .008) following 24 weeks of treatment with nebivolol. All of the patients that completed the study had a reduction in SBP and DBP, and 77% of the patients reached the target goal of SBP
Dose of Nebivolol Used and Success in Attaining Blood Pressure (BP) Target
Effects of Nebivolol on Echocardiographic Findings
Table 3 shows the effects of nebivolol therapy on echocardiographic parameters at baseline and after the 24-week treatment period. There was no significant change in diastolic function even though there was a statistically significant decrease in systolic and diastolic BP following treatment. The mean E/E' did not change following nebivolol treatment (pretreatment: 9.0
Changes in Echocardiographic Parameters With Nebivolol Plus HCTZ Therapy
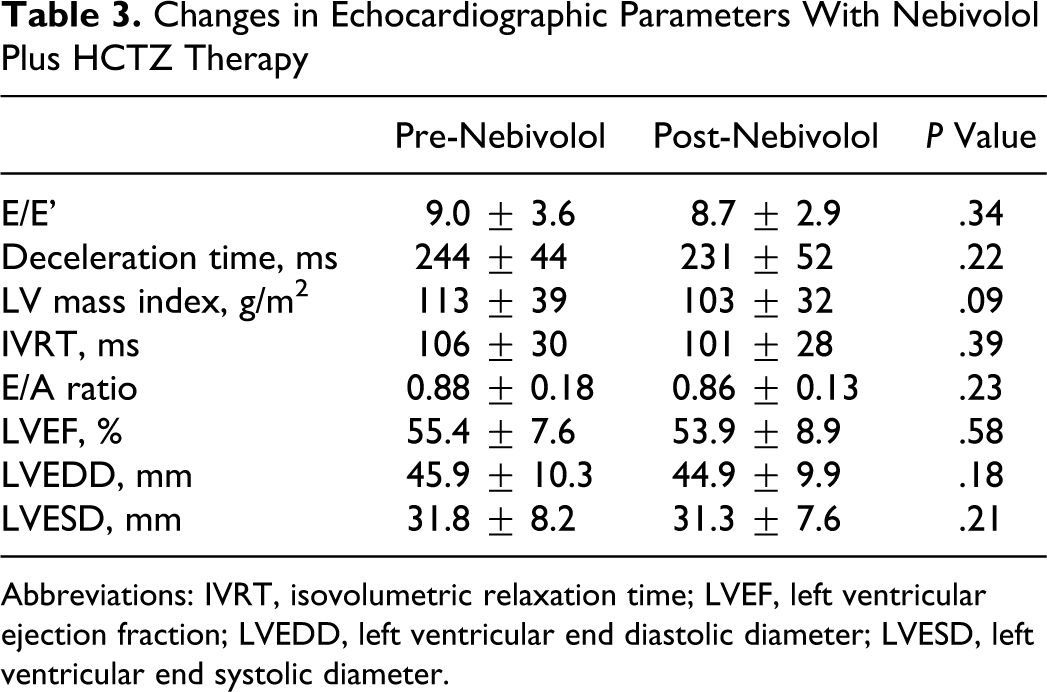
Abbreviations: IVRT, isovolumetric relaxation time; LVEF, left ventricular ejection fraction; LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end systolic diameter.
Determination of Serum Nitrite/Nitrate Formation to Measure Nitric Oxide Activity
We utilized the Griess diazotization reaction to spectrophotometrically detect nitrite formed by the spontaneous oxidation of NO under physiological conditions. 26 The Griess reaction can be used to analyze nitrate via its catalytic reduction to nitrite. Using a commercially available kit, we determined in the nitrate reduction assay that nebivolol treatment significantly increased serum nitrite/nitrate (NOx) levels in patients that were placed on 10 and 20 mg/d daily (Table 4). There was a trend (though not statistically significant) in patients who were placed and remained on 5 mg/d. In addition, there was a statistical increase in NOx concentration in patients who successfully met the target BP goals. In contrast, no change in serum NOx levels was observed in the group that did not have success in attaining the target BP goal.
Changes in Serum Total Nitric Oxide (NOx) Levels With Nebivolol Plus HCTZ Therapy a

Abbreviations: BP, blood pressure; SD, standard deviation.
aUsing the Griess reaction assay, we determined nitric oxide concentrations based on the enzymatic conversion of nitrate to nitrite by nitrate reductase. Assays are performed in triplicate. Values reported are the serum total NOx levels (μmol/l) ± standard deviation (SD).
bValue differs (P < .05) from pre-nebivolol therapy. The P values are shown.
Treatment With Nebivolol Reduces ADMA Levels in African Americans With Hypertension
Serum levels of ADMA were measured before and after the 24-week study period. We also made a comparison to a group of age-matched African American hypertensives controlled with diuretic therapy only (SBP: 134 ± 11 and DBP: 81 ± 10 mm Hg).
At the pretreatment period, the nebivolol group had a significantly higher level of ADMA than the controlled diuretic group. After 24 weeks of nebivolol treatment, the activity of ADMA decreased significantly by 44% over pretreatment levels (Figure 1; P = .008). This reduction in ADMA levels was positively correlated with the reduction in systolic BP (Figure 2; r = .54, P = .024). Furthermore, in comparison to the group of age-matched hypertensives treated with diuretic therapy only, the nebivolol group had significantly lower levels of ADMA (Figure 1). This was observed even though there was no difference in systolic or diastolic BP between the nebivolol posttreatment and the diuretic treatment groups.
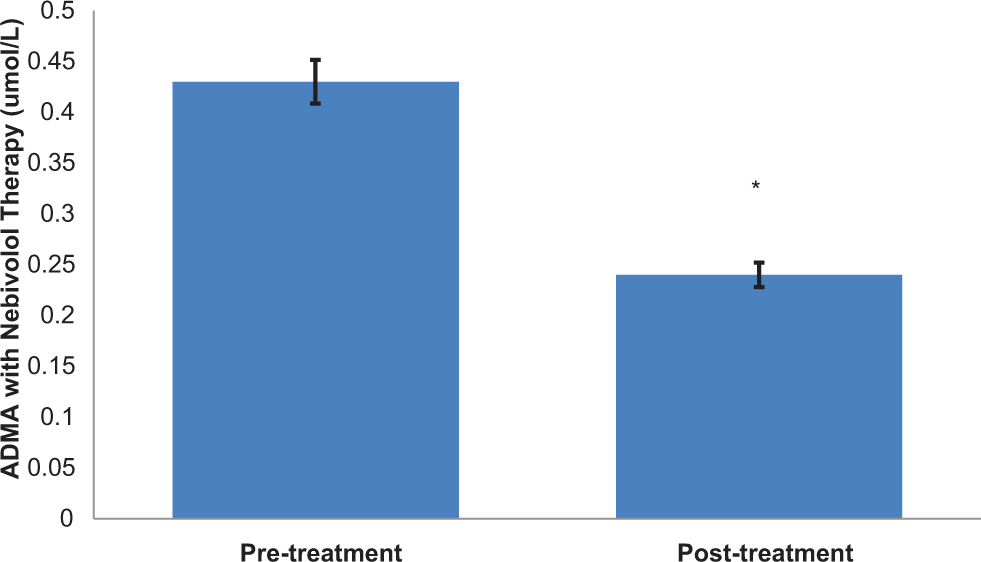
Effects of nebivolol therapy of plasma levels of ADMA. Plasma was collected, and ADMA levels were measured, as described in the Methods section. Values are the means
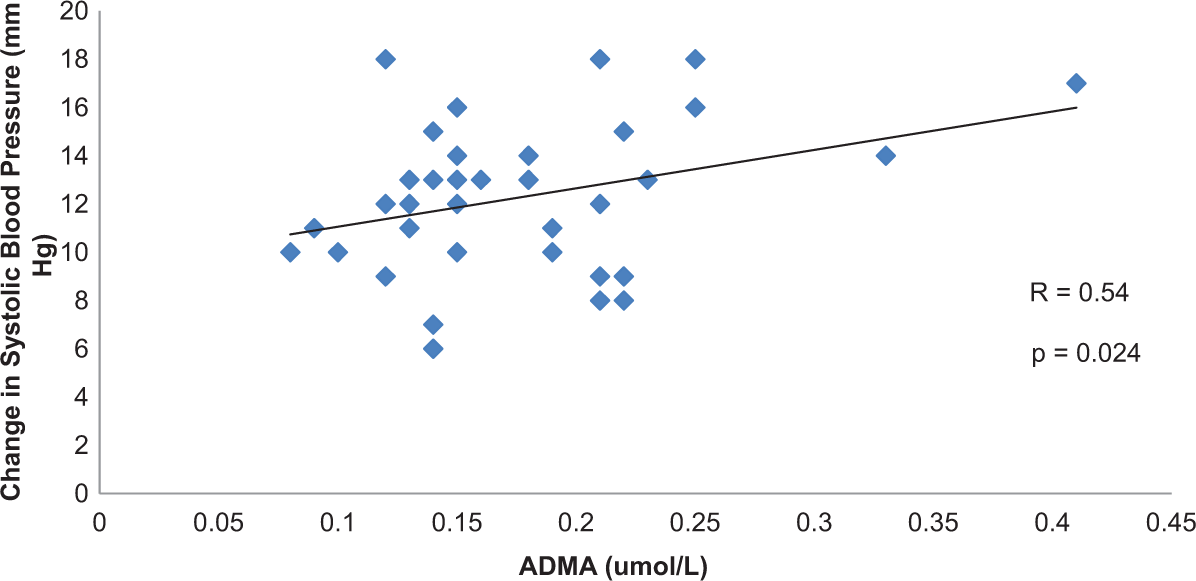
Correlation between changes in systolic blood pressure and plasma ADMA levels: effects of nebivolol in African Americans with hypertension. The points detailed in the graph indicate the individual change in systolic BP and plasma ADMA levels. R = coefficient of correlation. Significance level of the correlation is calculated.
Discussion
Although medical treatment has been effective in the treatment of hypertension, the incidence of this disorder continues to be high, particularly in African American patients. Our study indicates that in addition to diuretic therapy, there is a substantial benefit with nebivolol therapy in BP reduction in hypertensive African American patients. Systolic and diastolic BP reductions were significant in all patients, and the success rate in attaining normotensive BP levels with nebivolol was substantial. The net hemodynamic effect of nebivolol is the result of a balance between the depressant effects of beta-blockade and an action that maintains cardiac output. It is thought that the antioxidative and nitric oxide-mediated mechanisms of action observed in nebivolol may be beneficial in reducing the progression of insulin resistance, diabetes mellitus, and cardiovascular diseases. 27,28 Proinflammatory mechanisms are thought to be a hallmark of the cardiovascular disease process, notably in disease states such as hypertension. Taken together, the abnormal proinflammatory state leads to a worsening of metabolic control, abnormal vascular function, and eventually cardiovascular and renal diseases. 29 ,30
Using echocardiographic criteria, our study indicates that BP reduction with nebivolol did not have any significant impact on diastolic function in our patient population. These findings are of interest in that antihypertensive therapies have demonstrated varying results of BP reduction with diastolic function. 31,32 Specifically, the VALIDD study demonstrated improvement in TDI parameters but no significant change in E/E’. 9 However, Voors et al recently reported that eprosartan therapy in hypertension did not have any effect on any parameter of diastolic function despite a significant reduction in BP. The present study suggests that 24 weeks of treatment may be an insufficient time to detect any changes in diastolic function. 33 Also, the echocardiographic parameters of our study participants indicated comparable function to the general population, 34 whereas patients in other studies had worsened parameters.
For individual African Americans, overall perceived and real barriers to engage in exercise and healthy diets may outweigh perceived positive outcomes of total lifestyle changes, underscoring the importance of individual effective problem solving to reduce barriers and information to influence outcome expectancies. 35,36 These important culturally relevant factors were incorporated into the nutrition and physical activity educational materials which were provided to patients at each study visit.
Our findings demonstrate that nebivolol therapy increases serum total nitric oxide (NOx) concentration in a dose-dependent fashion. These results are consistent with the understanding that the mechanism of action of nebivolol operates via vasodilation through a nitric oxide-dependent mechanism. 16,17 Furthermore, it appears that the association of a low serum NOx level in hypertensive patients may be benefited with nebivolol treatment. As previously reported, 14 African Americans with hypertension demonstrate this finding, and the efficacy and tolerability of nebivolol therapy may be quite beneficial to this population.
The increase in serum NOx levels with nebivolol therapy correlates with a decrease in serum ADMA levels in African America patients with hypertension. In patients with elevated ADMA levels, nitric oxide synthase will not exert its expected function because its activity is blocked.
37,38
Indeed, a randomized clinical study has demonstrated for the first time that in patients with elevated ADMA concentration, statins only enhance endothelium-dependent vasodilation when they are administered concomitantly with dietary
Limitations of the Study
Our investigation is a short-term study (ie, 24 weeks of therapy) of a relatively small number of patients to determine potential mechanisms by which nebivolol added to diuretic therapy may be effective in a high-risk African American population with hypertension. We did determine that nearly 80% of our study participants did achieve the combined target goal systolic BP of <140 mm Hg and diastolic BP of <90 mm Hg. Our findings that nebivolol reduced ADMA levels may be a reflection of its success in BP reduction. The effective changes in blood pressure reduction, trend to a decrease in LV mass levels, and an improvement in serum NOx levels are likely due to a contribution of both nebivolol and HCTZ therapy. We did make a comparison of the posttreatment group with a group of hypertensives whose BP is controlled with diuretic therapy only. Even though ADMA levels were lower in the nebivolol group, further follow-up of these patients could demonstrate that these levels could be similar in both treatment groups. It is possible that the significant reduction of ADMA in the nebivolol group may be a reflection of a time element. Finally, the participants in our study are at significant risk of development of cardiovascular and renal diseases and its related complications. Therefore, these results may not be applicable to lower-risk populations.
Conclusions
The long-standing problem with hypertension in African Americans is likely a combination of environmental and genetic factors. Proinflammatory mechanisms are important in the pathogenesis of cardiovascular disease. The findings in the present study suggest in part the mechanisms by which the utilization of nebivolol may be beneficial in the prevention of cardiovascular and concomitant renovascular diseases. Even though BP reduction with nebivolol did not have significant effect on echocardiographic parameters of diastolic dysfunction, the marked reduction in ADMA levels indicates alternative or additive mechanisms by which the compound may reduce factors that are involved in the pathogenesis of cardiovascular diseases. Via an increase in nitric oxide bioavailability and improved endothelial function, the pharmacological addition of nebivolol has powerful effects within the vasculature of African American patients with hypertension. Long-term outcome studies should be considered to determine the utility of these agents and lifestyle modification in the primary prevention of cardiovascular diseases in this high-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by an unrestricted grant from Forest Laboratories (New York, NY), who also provided the drugs for the study.