
Abstract
Introduction
Diabetes mellitus (DM) is a chronic disease that leads to various potential complications. Patients with type 2 diabetes (T2DM) have an increased risk of death from cardiovascular causes compared with those without diabetes. 1 In Hong Kong, the prevalence rate of T2DM is 9.8% and cardiovascular disease (CVD) is a major health issue. 2 Appropriate management of hypertension, dyslipidemia, and other cardiovascular risk factors are necessary to prevent cardiovascular morbidity and mortality. However, neither hyperglycemia nor other cardiovascular risk factors are adequately controlled in patients with T2DM. 3 There is an apparent need for a multidisciplinary approach in the management of patients with T2DM. Previous pharmacist-led disease management programs have been shown to improve glycemic control and reduce cardiovascular risk factors in T2DM patients.4,5 The relative risks of coronary heart disease (CHD) and cerebrovascular accidents (CVAs) were also significantly reduced.5,6
There is no definitive disease management program outlining approaches to reduce cardiovascular risks in patients with T2DM, in Hong Kong. Therefore, we hypothesized that a structured pharmacist care program would have a positive impact in reducing cardiovascular risks in the clinical setting. The aim of this study was to investigate the impact of a structured pharmacist care program on cardiovascular risks in T2DM patients in a local public hospital.
Methods
The study was a 9-month, prospective, randomized, controlled trial conducted at the diabetes clinic of Tung Wah Eastern Hospital (TWEH) in Hong Kong, during May 2008 to March 2009. It is a 250-bed public convalescent hospital, serving the community of the eastern district in Hong Kong. The study protocol was approved by the Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee and the Hong Kong East Cluster Ethics Committee.
Inclusion Criteria
Trained diabetic nurses referred eligible patients to pharmacists if they were 18 years or older, had a clinical diagnosis of T2DM and current therapy with at least 5 drugs (in which 1 was a hypoglycemic agent), and had a hemoglobin A1c (HbA1c) level equal to or greater than 8%. We included patients with this HbA1c levels because they have been previously shown to greatly benefit the most from the program due to their higher risk of developing CVD. 7
Exclusion Criteria
The study excluded patients with the following: gestational diabetes; pregnancy; a secondary cause of hypertension (renal artery stenosis, renoparenchymal disease, aortic coarctation, preeclampsia, Conn syndrome, and pheochromocytoma); history of myocardial infarction, unstable angina, and heart failure; an uncorrected endocrine abnormality (Cushing disease, acromegaly); and end-stage renal failure (glomerular filtration rate <10 mL/min or undergone peritoneal dialysis or hemodialysis). Patients were also excluded from the study if they had marked dementia or unstable psychiatric illnesses, malignancy, or life-threatening conditions including cardiac arrest, sepsis, respiratory distress, and patients under care in the intensive care unit.
Randomization
During the enrollment visit, written consent was obtained. The pharmacist was blinded to the randomization codes—intervention group (1) or control group (0)—which were computer generated and sealed in envelopes labeled with consecutive numbers. The envelopes were opened in the clinic in an ascending manner by the pharmacist, and patients were randomized into either intervention group or control group. Baseline information such as demographic data, laboratory data, and compliance score were obtained. The number of patient clinic visits to the physicians were the same for both groups.
Intervention group
Patients allocated to the intervention group received 15 to 30 minutes of face-to-face interview with a pharmacist before each physician visit. At each visit, 5 main areas were addressed, namely, medication adherence, knowledge and beliefs, skills, perceived health as well as cognitive functions. The pharmacist recorded a complete medication history, including prescription drugs as well as over-the-counter drugs, vitamins, and herbal supplements. The pharmacist also evaluated the patients’ medication adherence. The importance of drug adherence was reinforced and patient-specific, protocol-driven education about CVDs, and lifestyle modifications were provided (Protocol shown in Appendix A). 8 A doctor’s note from pharmacist was attached in the medical record for any identified drug-related problem. In order to reinforce the patient’s drug knowledge, a color-coding system was adopted. Color stickers were placed on their pillboxes or drug bags to recall from their memories the class of medication and to identify what drugs they were taking.
Control group
Patients in the control group received the same medical care without pharmacist interventions. The patient’s drug and disease knowledge were assessed at baseline and at the end of the study by the same pharmacist.
Endpoints
The primary endpoint was the change in CHD risk after 9 months follow-up. A validated cardiac risk score specifically for the Hong Kong population was used to calculate the CHD risk of the patient. 9
The equation of CHD risk score is shown as follows:
The 5-year probability of CHD can be calculated by:

The equation of stroke risk score is shown below:
The formula of a 5-year stroke probability is as follows:

Compliance and Cost-Effectiveness
Patient’s medication knowledge and compliance were assessed by the same pharmacist for both intervention and control groups. The number of patients correctly describing the purpose of all their medicines before and after counseling was compared. A compliance score for each medication was calculated by dividing the number of tablets taken by the correct number and expressed as a percentage. 12 A mean compliance score was calculated for each patient. The change in compliance score between the intervention and control groups was compared. Patients were considered compliant to medication regimen if their compliance score was greater than 80%. 13 Pharmacist used a standard questionnaire to assess the drug and disease knowledge of the patients, and questions were asked in the same manner to all patients. Five main areas were the focus each time, namely: low medication adherence, knowledge and beliefs, skills, perceived health, and cognitive function. The number of patients correctly describing the purpose of all their medications before and after counseling were compared. All interventions and time spent by the pharmacist were documented. The cost-effectiveness of this care program was estimated using risk predictors and the direct cost of pharmacist time in counseling and associated administration time. Patients’ out-of-pocket expenses and indirect costs were not included. 6 Cost-effectiveness was expressed as prevention of CHD. The reciprocal of risk reduction and additional cost per person were used to calculate the cost per CHD event avoided. The cost-effectiveness was then determined by the potential cost saving per person compared with standard practice. Since the most significant manifestation of CHD was acute myocardial infarction (AMI), the potential cost saving per person was calculated by subtracting the cost of managing each AMI patient from the cost per CHD event avoided.
Statistical Analysis
A Statistical Package for the Social Sciences (Windows version 17.0, SPSS Inc, Chicago, Illinois) and Microsoft Excel XP (Microsoft Corp, Redmond, Washington) were used for statistical analyses. All data were expressed as the mean and standard derivations (SDs), median and interquartile range (IQR), or percentages (%), unless otherwise specified. Categorical data were analyzed using the chi-square test. The 2-sample Student t test was used to compare the change in CHD and stroke risks, BP, HbA1c, HDL-C, LDL-C, TG, ACR, and the compliance score between the study groups. A P value less than .05 was considered statistically significant.
Based on a previous 9-month study, 40 patients would be required for each group to achieve 80% power, at a 5% 2-sided α level using Altman nomogram for sample size calculation to detect a 10% difference in favor of the intervention group at follow-up.6,14 Allowing for patients lost to follow-up, 50 patients were recruited into each group.
Results
A total of 120 were referred by DM nurses during the recruitment period, of which, 2 declined interviews, 6 were ineligible, and 7 were not willing to enter the study. Hence, 105 eligible participants were recruited and randomly assigned to either control group or intervention group. After randomization, 54 participants were assigned to the control group, whereas the remaining 51 participants were in the intervention group. All patients completed the study. Baseline characteristics as well as CHD and stroke risk scores were similar between the 2 groups (Table 1). The total numbers of physician visits were the same for both intervention and control group patients. Medications used during the study period are summarized in Table 2. A statistically significant difference was observed for metformin in the intervention group at the end of study and for fibrates in the control group at the end of study. The reason for the differences was unknown. However, no statistical significant differences were observed for the other drugs used before and at the end of study period for both the intervention and control groups.
Baseline Values and Changes Over 9 Months Between Control Group and Intervention Group a
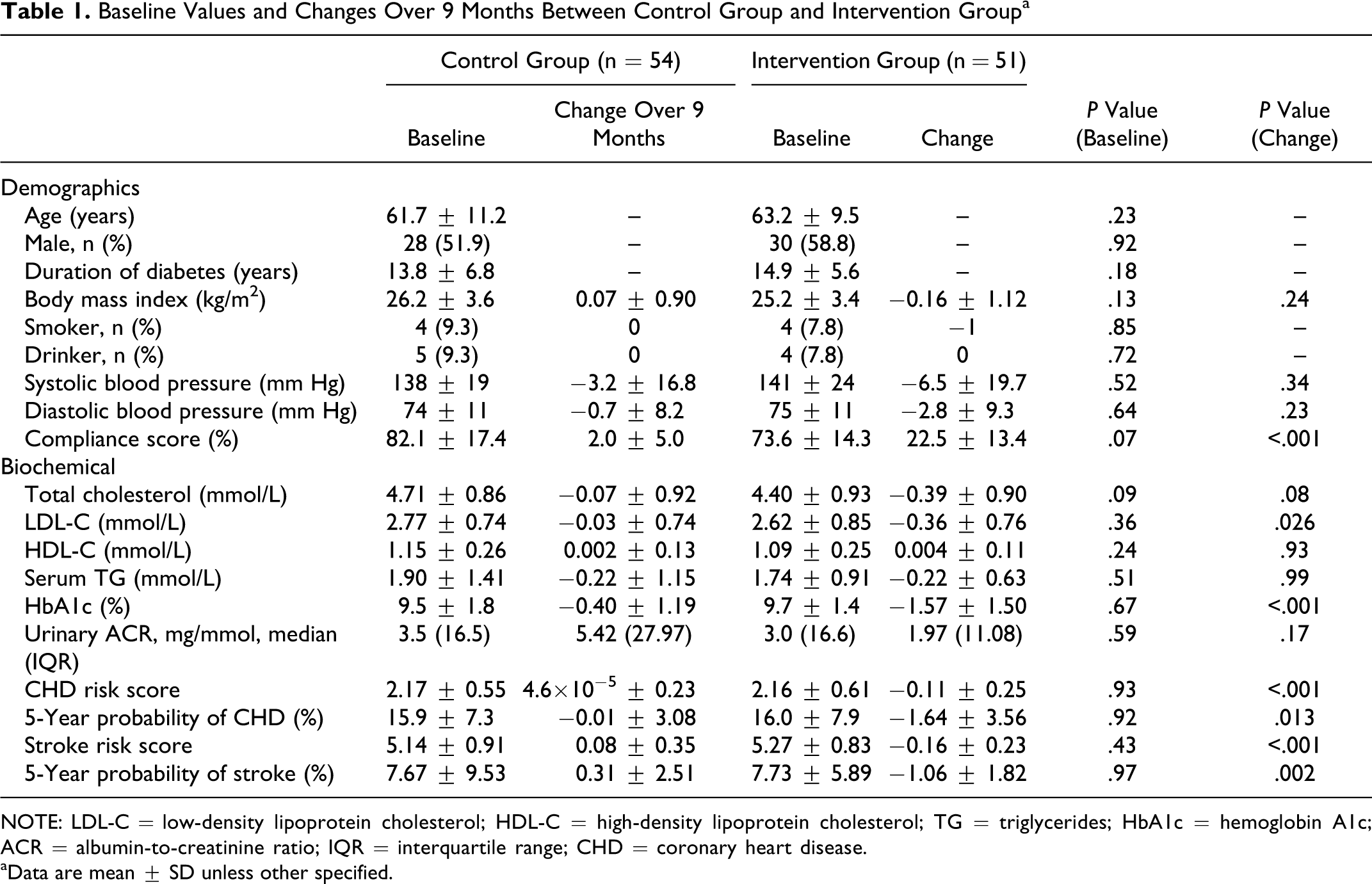
NOTE: LDL-C = low-density lipoprotein cholesterol; HDL-C = high-density lipoprotein cholesterol; TG = triglycerides; HbA1c = hemoglobin A1c; ACR = albumin-to-creatinine ratio; IQR = interquartile range; CHD = coronary heart disease.
aData are mean ± SD unless other specified.
Medication Use and Changes Over 9 Months in Intervention and Control Groups
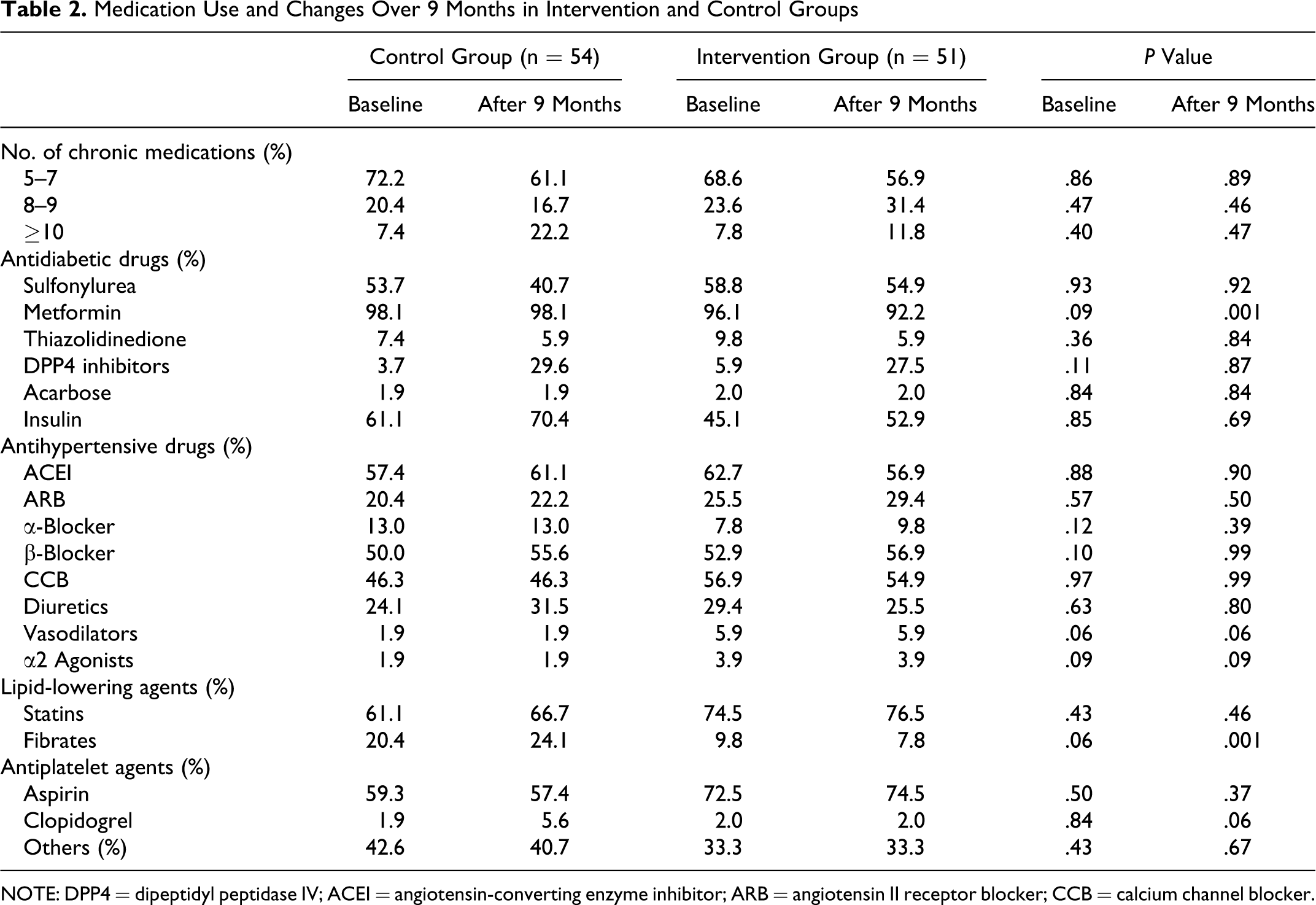
NOTE: DPP4 = dipeptidyl peptidase IV; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin II receptor blocker; CCB = calcium channel blocker.
Clinical Outcome Measures
Patients in the intervention group had a statistically significant reduction in CHD risk scores compared with the control group (−0.11 ± 0.25 vs 4.6 × 10−5 ± 0.23, P < .001). The 5-year probability of developing CHD risk was significantly decreased in patients under the pharmaceutical care program compared with the control group (−1.64% ± 3.56% vs −0.01% ± 3.08%, P = .013). The stroke risk was also significantly reduced in patients under the pharmacist’s care (−1.06 ± 1.82 vs 0.31 ± 2.51, P = .002). Both HbA1c and LDL-C were also greatly reduced in the intervention group compared with the control group (−1.57% ± 1.50% vs −0.40% ± 1.19%, P < .001 and −0.36 ± 0.76 vs −0.03 ± 0.74, P = .026, respectively; Table 1).
There were nonsignificant improvements in serum HDL-C, TG, total cholesterol, systolic blood pressure (SBP), and diastolic blood pressure (DBP), as well as improvements in the body mass index in the intervention group. Both groups showed an increase in urinary ACR, but there was no significant difference between the 2 groups. No cardiovascular events or surgical events were experienced by the patients during the study.
At the end of study, 9.8% of patients in the intervention group did not meet any treatment goals as suggested by the ADA, 11 whereas 16.7% did not reach any goals in the control group. The present study significantly reduced the number of people who had HbA1c greater than 9% compared to those in the control group (−45.1% vs −3.7%, P = .02; Table 3 ).
Comparison of Patients Who Reached Treatment Goals

NOTE: HbA1c = hemoglobin A1c; LDL-C = low-density lipoprotein cholesterol; HDL-C = high-density lipoprotein cholesterol; M = male; F = female; SBP = systolic blood pressure; DBP = diastolic blood pressure.
A total of 271 pharmacist interventions were conducted. Each patient received an average of 5 pharmacist interventions during the study period. Over 33% of interventions were made with respect to medication adherence, that is, advising patients the correct administration time, and reminding them about the correct dose and frequency of the most updated regime. Another 30% of the interventions were related to lifestyle modifications, such as encouragement to increase exercise activity, smoking cessation, and importance of adherence to dietary programs. A total of 29 notes were sent out to physicians to communicate all drug-related problems, such as poor drug compliance and side effects experienced by the patients. All the doctor notes were accepted and documented in the medical records.
The average compliance score of the intervention group was 96.0% ± 6.8%, while the control group was 84.1% ± 18.1%. Patients in the intervention group had a greater improvement in compliance compared to those in control group (22.5% ± 13.4% vs 2.0% ± 5.0%, P < .001). Reasons for noncompliance were forgetfulness (30%; 18 participants in intervention group vs 13 participants in control group), lack of understanding (83%; 47 participants in intervention group vs 40 participants in control group), fear of or experiencing side effects (16%; 10 participants in intervention group vs 6 participants in control group), and deliberate noncompliance (10%; 4 participants in intervention group vs 6 participants in control group).
Patients’ knowledge regarding the purpose of their medications increased from 71% (baseline) to 96% in the cohort of patients who received pharmacy intervention but decreased from 83% (baseline) to 65% in the control group. This difference was statistically significant (P < .001). The total time spent by pharmacist during the entire study was 2414 minutes. On average, each patient interacted with the pharmacists for approximately 50 minutes throughout the entire study. The additional cost of pharmacist time per patient was US$64 (US$1 = HK$7.8). The present study showed that the CHD risk of patients under a pharmacist care program could be reduced by 1.64%. Hence, the cost per CHD event avoided was US$3902.4. Based on a local study, 15 the cost of treating an acute myocardial infraction was US$8988.7. The potential saving from this program was US$5086.3 per patient.
Discussion
The present study showed that a 9-month pharmaceutical care program significantly reduced cardiac risk scores and the 5-year probability risk of developing CHD in T2DM patients. There were also noteworthy decreases in modifiable vascular risk factors, that is, glycemic control and lipid level.
The current study was the first to use the validated CHD risk score equation for Hong Kong Chinese diabetic population to calculate the estimated risk of developing CHD over 5 years. Most of the overseas studies used the Framingham risk score and the United Kingdom Prospective Diabetes Study (UKPDS) CHD risk engine to calculate the CHD risk score for diabetic patients. However, overestimation of the absolute risk of CHD in Chinese population has been reported. 16 The current equation used for CHD risk score was tailored for Hong Kong DM population; therefore, findings of the current study may not apply to other ethnic groups.
The Fremantle Diabetes Study demonstrated a decrease in the 10-year estimated risk of a first CHD event in pharmaceutical care participants (from 25.1% to 20.3%) but not in control participants. 5 Another study 6 conducted in the United Kingdom showed that the cardiac risk in patients with T2DM after intensive pharmacist care was reduced by 11.9%. It is worth pointing out that all these studies showed a promising reduction in estimated CHD risk in patients under a pharmaceutical care program compared to those in respective control groups receiving standard medical care.4–6
Patients under our pharmacist care program lowered their HbA1c by a mean of 1.6%, whereas only a 0.4% drop was observed in the patients receiving usual standard care. This finding was consistent with most previous diabetes management programs that showed reductions in HbA1c level by as much as 1% to 2%.17,18 We considered our program a success as every 0.5% reduction in HbA1c would likely lead to a 7% decrease in myocardial infarction and a 12% decrease in risk of stroke. 7 The intervention group also showed a favorable lipid profile compared to the control group. A greater than 13% reduction in LDL-C level was seen in patients after pharmacist intervention, whereas only a 1% drop was observed in the control group. Although the magnitude of changes in HDL-C and total cholesterol levels was small, the improvement was greater in the intervention group. Our study was consistent with overseas data, in which behavioral counseling did not produce substantial changes in cholesterol level. 19
Both SBP and DBP were reduced in 2 groups over 9 months but to a greater extent in the intervention group. The mean reduction of SBP in the intervention group was 7 mm Hg, double that seen in the control group; however, the reduction was not statistically significant. The mean decrease in DBP was 4 times greater in the intervention group compared to the control group. Our findings matched those obtained from a pharmacy care program in the United States, which also demonstrated significant reductions in SBP and DBP by 6.9 and 2.5 mm Hg, respectively. 20 Patients were also counseled on dietary sodium intake. A local epidemiologic study found that 78% of the participants had an estimated sodium intake of more than 2300 mg/d, a sodium intake value that has been shown to be significantly related to the slope of BP rise associated with increasing age. 21 In view of this study, the present pharmacist’s program stressed the importance of low-salt diet in addition to enhancing medication adherence. After taking a dietary history, a specific dietary recommendation was given to each patient.
Numerous studies showed that long-term decreases in BP are associated with as much as a 50% reduction in stroke or myocardial infarction. 1 Our study demonstrated a reduction in stroke risk in the intervention group, but an increase in the control group. These data further highlight the value of the pharmacist care program that targeted all conventional risk factors as both cardiac and stroke risks were significantly reduced in the intervention group. Despite the greater drop in BP in the intervention group, the present study did not reveal any beneficial changes in urinary ACR. These findings were comparable to an overseas study in which no significant difference in ACR was shown. 5 Nevertheless, the deterioration was slower in the intervention group, and this trend may be significant if the duration of intervention was longer.
In a previous clinical trial, the erratic timing of doses (unbeknownst to the primary care provider) was found to be the culprit of poor control rather than inadequate drug doses. 22 Poor adherence to medication could be improved when patients and clinicians were both aware of the frequency of missed doses. In the present study, pharmacists specified all drug-related problems including poor drug compliance and side effects experienced by patients; these problems were communicated to the physicians via doctor notes. Written and verbal communications with physicians and nurses are crucial to building professional working relationships necessary to ensure optimal patient care.
The current pharmacist care program is not meant to replace the formal DM education, however, the program provides a useful supplement or enhancement to the care of diabetic patients. Our study participants received formal DM education before recruitment, but additional benefits were seen following our pharmacist care program. Similar results were also observed in another study of diabetic patients. 23
Several limitations in our study should be addressed. The present study only evaluated the short-term outcomes of patients and was unable to determine whether these benefits would persist during a longer study period. Therefore, further research to assess the long-term benefits of such a pharmacist care program is warranted. Moreover, the compliance rate was calculated based on patient self-reporting, which likely overestimated the adherence. Though there are no perfect methods for assessing medication compliance, a recent literature review concluded that standardized self-report adherence measures corresponded adequately with objective measures. 24 We tried to limit these potential biases by focusing on objective measures for study endpoints. Blinding of participants and investigators was not possible in our study. Furthermore, it was not possible to blind the remainder of the medical team that may have impacted the level of education provided to their patients under standard care. The extra attention received by the patients may have produced potential positive outcomes in both groups. However, it is noted that the changes in intervention group were significantly greater than the control group. Finally, the present study was conducted in 1 public hospital in Hong Kong; the equations used are tailored for Hong Kong people, which limits generalizability. The cost-effectiveness analysis may not be easily extrapolated to the other health care systems with different costs.
Conclusion
Our study demonstrated the value of a pharmacist care program in significantly reducing cardiovascular risk in T2DM patients. Furthermore, pharmacist interventions contributed toward significant improvement in patients’ knowledge and understanding of drug therapy and enhanced medication adherence. Therefore, the pharmacist can be a valuable addition to standard care for patients with T2DM.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: the School of Pharmacy, The Chinese University of Hong Kong and the Diabetes Research Fund, Diabetes Hong Kong.
Appendix
Pharmacist’s Intervention Protocol 8
| Problem Category | Problem | Solutions |
|---|---|---|
| Medication adherence |
Suspect patient not taking medications as prescribed |
Show the patient you care Discuss low adherence with the patient, determine reason and solve problem with patient Determine whether patient experiences side effects of the drugs or complicating regimen with over-the-counter and herbal drugs Contact physician to describe the side effects experienced by the patient Reinforce the importance of medication adherence |
|
Suspect patient misses doses or has erratic timing of doses |
Examine whether drug was taken, timing of dosing appropriate or missed doses Provide ways to resolve the problems (eg, instruction handout) |
|
|
Patient misses refills |
Identify the reason If the patient cannot afford to pay for the medication, refer patient to medical social workers |
|
| Knowledge and belief |
Lack of understanding of cardiac diseases |
Explain fundamentals of cardiac diseases and its management to patient in terms he or she can understand Provide educational materials to clarify concept |
|
Lack of understanding of the relationship of hypertension or diabetes control to cardiac diseases management |
Explain how poor management of hypertension and diabetes contribute to increased risks of developing cardiac diseases Provide educational handout if necessary |
|
|
Lack of understanding of drug information |
Explain in terms patients can understand the rationale for using each medication and its relationship to the disease management |
|
|
Needs diet-specific instruction |
Ask patient about diet habits. Stress importance of low-salt and low-sugar diet Provide educational handout |
|
|
Needs lifestyle modification |
Encourage patient to have regular exercise for at least 30 minutes daily Limit alcohol consumption Encourage to quit smoking |
|
|
Patient does not believe he or she needs medication |
Build the confidence in medication management routines Provide verbal and written educational materials Discuss patient’s expectations with him or her |
|
| Skills Prescription—taking skills Communication skills |
Inability to read and comprehend instructions on prescription label |
Explain medication administration (interval between doses) Literacy problem: use color coding/figure to explain the drugs |
|
Patient expresses difficulty discussing problems with physicians |
Determine gaps in patient’s knowledge and treatment plan Provide patient with a list of questions to ask the physician during clinic visit |
|
|
Patient forgets what physician says |
Ask patient to have doctors or nurses write down the instructions |
|
|
Patient does not agree with physician’s treatment |
Medication not effective: Encourage patient to discuss alternative treatment with physicians Side effects: Encourage patient to discuss the problem with physician Pharmacist contact physician to describe side effect experienced by the patient |
|
| Perceived health |
Patient does not realize the severity of illness Patient with mild disease is frightened about the fate |
Establish the severity of the disease Educate patient about the importance of treating hypertension, diabetes and associated comorbid conditions to prevent or slow down the progression of cardiac diseases Be optimistic with patient |
| Cognitive function |
Patient does not remember to take medication Patient without supervision |
Identify a daily routine activity (patient dose at a regular time) that a patient may use as a cue to take his or her medication on schedule Use alarm clock to remember next dose Provide motivation for patient to take medications and use aids (pillboxes) to improve adherence |
