
Abstract
Introduction
The prognostic value of cyclin-dependent kinase 5 (CDK5) was investigated in a cohort of patients with cetuximab-treated, chemotherapy-refractory, dual wild-type Rat Sarcoma and v-raf murine sarcoma viral oncogene homolog B1 (RAS/BRAF) metastatic colorectal adenocarcinoma.
Methods
Immunohistochemistry (IHC) was used to retrospectively analyze the expression of CDK5 in metastatic colorectal adenocarcinoma tissue samples of 129 patients. All statistical computations were performed in R 4.0.5. Dichotomous clinicopathological variables were then cross-tabulated across CDK5 strata and compared with Pearson’s χ2 test. Cumulative survival probabilities were estimated via the Kaplan–Meier estimator and contrasted with the log-rank test. Independent prognostic determinants were ascertained through Cox proportional-hazards.
Results
79 men and 50 women were enrolled in this study, with a median age 62.8 years. Among 129 specimens subjected to CDK5 IHC, 111 tumor cores yielded unequivocally evaluable results. 69 lesions were allocated to the low-to-intermediate expression tier (scores 0–2+), whereas 42 exhibited marked overexpression (score 3+). Elevated CDK5 immunoreactivity was shown to predict inferior progression-free survival (PFS) (7.0 versus 9.0 months; P=0.049) and a shortened cancer-specific survival (CSS) (27.8 vs 38.5 months; P=0.048). In addition, low-to-intermediate CDK5 expression remained independently associated with PFS (HR 0.544; 95 % CI 0.369–0.801; P=0.002) and CSS (HR 0.502; 95% CI: 0.329–0.766; P=0.001). CDK5 overexpression conferred a statistically significant detriment to PFS among patients harboring only extra-hepatic metastases (P=0.012), while within the hepatic-metastatic subset, no survival discrepancy was discernible between the high and low-to-intermediate expression cohorts (P=0.800).
Conclusions
Independent multivariable modelling identified elevated CDK5 as a robust predictor of both curtailed PFS and CSS. Intriguingly, this prognostic power appears to be contingent upon the site of disease: once the cancer metastasizes to the liver, the predictive signal of elevated CDK5 is abruptly extinguished.
Keywords
Introduction
Colorectal cancer (CRC) remains one of the most prevalent malignancies worldwide, with over 1.9 million new cases and 935,000 deaths reported globally in 2020.1,2 It is worth noting that the recent identification of favorable subsets within cancers of unknown primary (CUP), particularly a CRC-like subtype that has emerged as a distinct clinical entity sharing molecular and clinical features with CRC and frequently managed according to CRC treatment paradigms, may account for the observed trends. 3 In China, the incidence and mortality rates continue to rise, making CRC the second most common cancer and the fourth leading cause of cancer-related death, posing a significant threat to public health. 4 With the progression of population aging in China, elderly patients which are more susceptible to severe postoperative complications are accounting for an increasingly substantial proportion of the overall patient population. However, the extent to which age independently affects survival remains uncertain, largely because prognosis among elderly patients may be obscured by variations in presenting stage, tumor anatomy, concurrent comorbidities, and treatment selection. 5
In the era of precision oncology, epidermal growth factor receptor (EGFR) monoclonal antibodies, such as cetuximab, have become a cornerstone in the treatment of Rat Sarcoma (RAS) wild-type metastatic CRC (mCRC). 6 Objective response rates (ORR), progression-free survival (PFS), and overall survival (OS) in this molecularly selected population have been demonstrated to be significantly improved by cetuximab-based chemotherapy in clinical trials.
Despite these advances, primary and acquired resistance to Epidermal Growth Factor Receptor (EGFR)-targeted therapy remains a major clinical challenge. Therapeutic failure is contributed to by mechanisms such as KRAS mutations, EGFR extracellular domain alterations, and downstream Mitogen-Activated Protein Kinase (MAPK) pathway activation. Moreover, the absence of robust predictive biomarkers limits the ability to stratify patients who are most likely to benefit from EGFR inhibition, underscoring the need for novel prognostic indicators. Among patients with metastatic CRC receiving biologic agents, miR-126 upregulation correlates with bevacizumab resistance, whereas cetuximab resistance is tied to the overexpression of miR-31, miR-100, and miR-125b, alongside miR-7 underexpression. 7 However, a considerable gap remains between these findings and their clinical translation. The tumor-promoting role of cyclin-dependent kinase 5 (CDK5) in prostate and pancreatic cancers was first identified by Nelkin, and its association with the ral gene within the K-RAS signaling pathway was further demonstrated by him,8,9 with this pathway having been successfully targeted in colon cancer therapy. 10
In this study, we identified CDK5 as a potential predictive biomarker for cetuximab efficacy in RAS wild-type mCRC. High CDK5 expression was associated with poorer treatment outcomes, suggesting that CDK5 may serve as a novel molecular determinant to guide anti-EGFR therapy. These findings offer a promising avenue for refining patient selection and improving therapeutic precision in this subset of CRC patients.
Materials and Methods
Clinical Data
We performed a single-institution, retrospective cohort analysis encompassing 129 consecutive individuals with chemotherapy-refractory, dual wild-type RAS/BRAF (KRAS/NRAS/BRAF V600E) metastatic colorectal adenocarcinoma who commenced anti-epidermal growth factor receptor (EGFR) monoclonal antibody therapy (cetuximab) at the Affiliated Jinhua Hospital, Zhejiang University School of Medicine, between 12 August 2022 and 25 September 2024 (Figure 1A). And all patient details have been de-identified. Staging of the colorectal carcinoma was performed based on the 8th AJCC system, and histopathologic verification was carried out relying on endoscopic or operative specimens that were reviewed independently by 2 subspecialized gastrointestinal pathologists; discordant interpretations were resolved by a senior pathologist with advanced subspecialty certification. The curated institutional database was last updated on 9 February 2025. Systemic treatment algorithms and supportive interventions were implemented in strict accordance with contemporaneous National Comprehensive Cancer Network (NCCN) and Chinese Society of Clinical Oncology (CSCO) recommendations. No subject underwent metastasis-directed radiotherapy. Patients attaining at least partial radiologic response on systemic therapy were presented to a multidisciplinary tumor board (MDT) for evaluation of curative-intent resection of the primary tumor and all metastatic foci. Using a validated semi-quantitative H-score, lesions were assigned to either the low-to-intermediate CDK5-expression group (0–2+) or the high-expression group (3+)—a stratification that, in our previous study, proved to be significantly associated with colorectal cancer prognosis.
11
The HER2 status was divided into the positive group and the negative group, based on the HERACLES diagnostic criteria. Follow-up information was systematically acquired through scheduled outpatient encounters, augmented by telephone or domiciliary assessments executed by dedicated clinical research coordinators. Cancer-specific survival (CSS) was computed from the date of histologically documented metastatic disease to death attributable to colorectal cancer or last contact. Progression-free survival (PFS) was defined as the interval between the initial administration of anti-EGFR therapy and radiologic progression per RECIST 1.1, symptomatic progression, death from any cause, or censoring. All personal identifiers were irreversibly anonymized. Approval for the study protocol was received from the Institutional Review Board of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines are adhered to in this reporting.
12
The reporting of this study conforms to the STROBE guidelines.
13
Enrollment of study population and follow-up status. (A) Study cohort flow diagram. (B) Population pyramid delineating the demographic structure of the enrolled participants. (C) Distribution of follow-up durations within the study cohort
Methods
Immunohistochemistry Staining of CDK5
A colorectal cancer tissue microarray (80 cores/plate) was constructed from archival paraffin blocks aligned with surgical pathology numbers; 3 µm sections were baked at 60 °C for 1 h, then subjected to automated CDK5 IHC (Leica Bond-MAX) using an overnight 4 °C incubation with rabbit anti-CDK5 monoclonal antibody, followed by Bond polymer detection, DAB chromogen, hematoxylin counterstain and mounting. Staining intensity and percentage positivity were scored 0–3 by 2 independent gastrointestinal pathologists with a third senior referee for discrepancies: 0=none, 1=weak/yellow, 2=moderate/yellow-brown, 3=strong/brown (Supplementary Figure 1). All procedures were performed on an automated immunostainer following a strictly standardized protocol identical to that described in our prior study. 11
Statistical Analysis
All statistical computations were performed in R 4.0.5. Categorical variables were evaluated with the Pearson χ2 test, or, when expected cell frequencies fell below 5, Fisher’s exact test was applied. Continuous variables are presented as mean ± standard deviation (SD). Inter-group comparisons of parametric data were conducted using the 2-sample Student t-test, whereas non-parametric data were analyzed with the Mann–Whitney U test. The optimal age cut-off was determined by maximally selected rank statistics (MSRS), accounting for multiplicity. Survival functions were estimated via the Kaplan–Meier product-limit estimator; between-group differences in survival were interrogated with the Mantel–Cox log-rank test. Subsequently, forest plots were generated to visualize the
Ethical Approval
This project and manuscript were reviewed and approved by the Ethics Committee of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine on June 22, 2022 (Approval number: 2022-43). The Ethics Committee of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine has waived the requirement for obtaining informed consent.
The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024.
Results
Clinical Characteristics
Baseline Characteristics of the Study Population

dMMR:deficient mismatch repair; pMMR:proficient mismatch repair; HER2:Human Epidermal growth factor Receptor 2.
High Expression of CDK5 Was Correlated With a Poorer PFS for Metastatic Colorectal Cancer
In an earlier single-center cohort limited to 89 colorectal adenocarcinoma specimens, elevated CDK5 immunoreactivity was associated with advanced tumor–node–metastasis stage, which translated into markedly attenuated survival.
14
Yet, non-metastatic disease was found to be the only scope of those findings, whereas an inverse relationship between elevated CDK5 expression and oncologic outcomes in the non-metastatic setting was first disclosed by our subsequent limited-cohort investigation.
11
To definitively establish the prognostic import of CDK5 expression in metastatic colorectal adenocarcinoma harboring concomitant RAS/BRAF wild-type status and treated with cetuximab-based therapy, this study was conducted, and it was observed that elevated CDK5 immunoreactivity predicted inferior PFS (median PFS 7.0 versus 9.0 months; P=0.049, Figure 2A). A significant impact on PFS was likewise exerted by anatomical tumor location, with the shortest median PFS exhibited by right colon primaries (P=0.005, Figure 2B). A statistically significant prolongation of median PFS was conferred by HER2 expression (even minimal) relative to complete HER2 negativity (P=0.047, Figure 2C). Conversely, PFS was not materially influenced by peritoneal, hepatic, or pulmonary metastatic involvement (P>0.05, Figure 2D–F). Patients whose disease was stage IV at initial presentation experienced significantly extended median PFS compared with those initially diagnosed at stages I–III (P=0.00 Association of CDK5 expression and clinicopathologic variables with PFS. (A) Influence of CDK5 expression levels on PFS. (B) Prognostic significance of primary tumor anatomical site for PFS. (C) Association between HER2 status and PFS. (D) Effect of peritoneal metastatic burden on PFS. (E) Relevance of hepatic metastatic involvement to PFS. (F) Impact of pulmonary metastatic disease on PFS. (G) Relationship between baseline disease stage and PFS. (H) Contribution of curative-intent primary tumor resection to PFS. (Abbreviations) HER2: Human Epidermal Growth Factor Receptor2
High Expression of CDK5 Was Correlated With a Poorer CSS for Metastatic Colorectal Cancer
By stratifying the cohort according to CDK5 Immunohistochemistry scores into low-to-intermediate (0/1+/2+, n=69) and high (3+, n=42) expression tiers, we systematically interrogated the prognostic impact of CDK5 on Association of CDK5 expression and clinicopathologic variables with CSS. (A) Influence of CDK5 expression levels on CSS. (B) Prognostic significance of primary tumor anatomical site for CSS. (C) Association between baseline disease stage and CSS. (D) Contribution of curative-intent primary tumor resection to CSS. (E) Impact of cetuximab treatment line on CSS. (F) Relevance of hepatic metastatic involvement to CSS. (G) The optimal age threshold for CSS. (H) Contribution of age to CSS
Both univariate and multivariable survival models concordantly establish that heightened CDK5 expression serves as an adverse determinant of abbreviated PFS and CSS in the metastatic colorectal carcinoma setting PFS.
Uni-Variate and Multivariate Analysis of Progression-Free Survival (PFS) in the Study Population

aUni-variate and multivariate analyses were conducted using cox regression model. bStaging based on the 8th AJCC system of the colorectal carcinoma.

In-depth reassessment of progression-free survival and cancer-specific survival endpoints within the investigated cohort. (A) Progression-free survival prediction nomogram. (B) Cancer-specific survival prediction nomogram. (C) Multivariate Cox proportional-hazards regression model for PFS. (D) Multivariate Cox proportional-hazards regression model for CSS. (E) Subgroup-stratified Forest plot illustrating hazard ratios for PFS. (F) Subgroup-stratified Forest plot illustrating hazard ratios for CSS. (G) Prognostic significance of CDK5 expression for PFS among patients harboring only extra-hepatic metastases. (H) Prognostic significance of CDK5 expression for PFS among patients with hepatic metastases
Uni-Variate and Multivariate Analyses of Cancer Specific Survival (CSS) in the Study Population
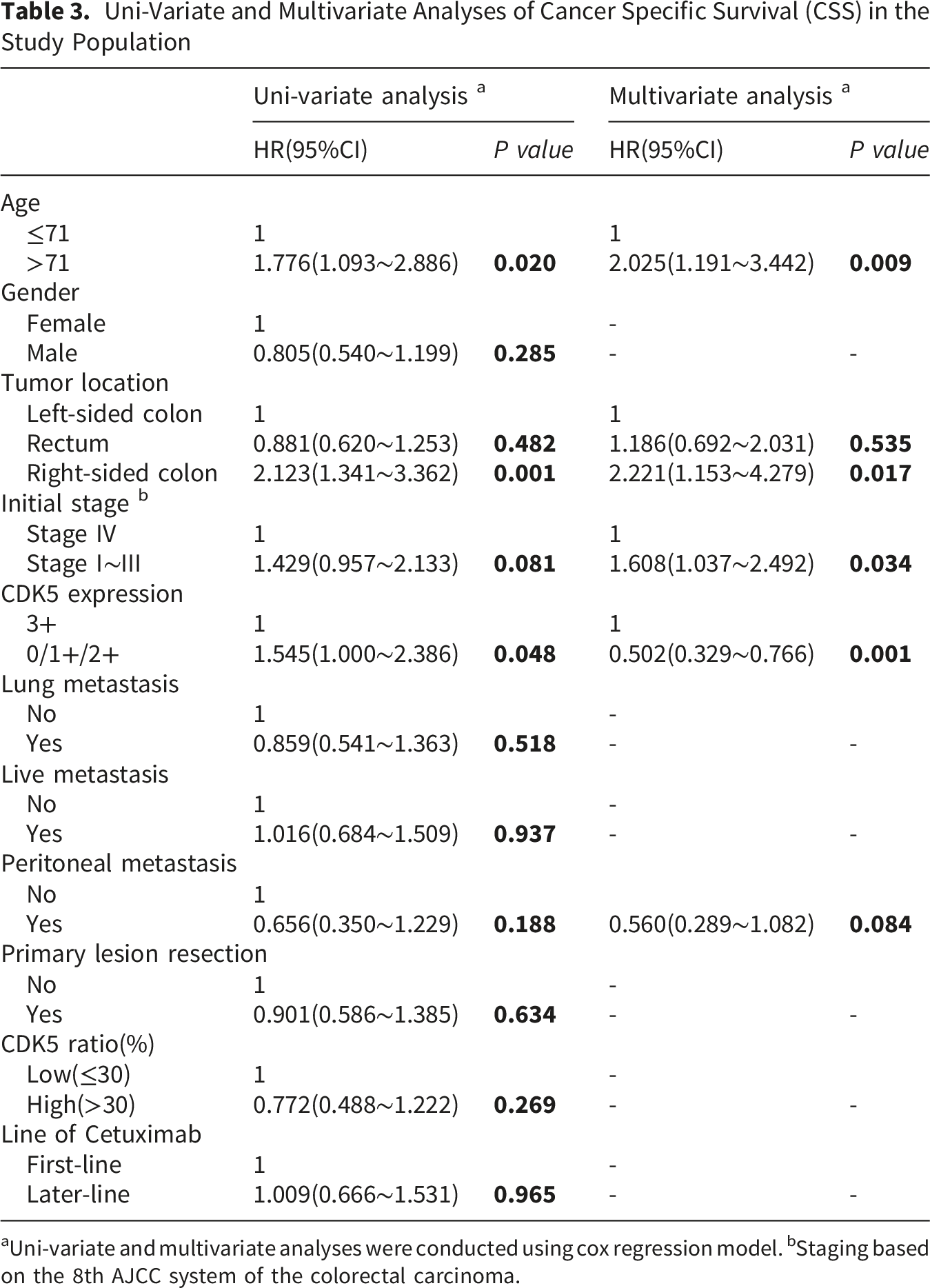
aUni-variate and multivariate analyses were conducted using cox regression model. bStaging based on the 8th AJCC system of the colorectal carcinoma.
Up-Regulated CDK5 Expression Demonstrated a Statistically Significant Association With Markedly Abbreviated PFS in the Non-hepatic Metastatic Subset
To delineate further the prognostic discriminatory capacity of CDK5 expression across clinicopathological stratified cohorts, a supplementary subgroup survival analysis was conducted to systematically appraise potential divergences in PFS between patients exhibiting high versus low-to-intermediate CDK5 expression levels. As delineated in Figure 4E, when sub-cohorts were partitioned by hepatic metastatic status, a statistically significant interaction effect was manifested by the predictive signal of CDK5 for PFS (p-interaction <0.05). In contradistinction, no significant disparity in
Discussion
Profiling CDK5 abundance in tissue microarrays derived from cetuximab-treated, chemotherapy-refractory, dual wild-type RAS/BRAF metastatic colorectal adenocarcinoma, it was observed that abbreviated PFS and
Although the present investigation was constituted as the first evidence demonstrating that outcomes in patients with RAS wild-type metastatic colorectal cancer treated with cetuximab were independently predicted by CDK5 expression, a novel molecular determinant for refined risk stratification in this clinical subset was thereby established. The abrupt evaporation of CDK5 prognostic value once metastatic cells colonize the liver is identified as the most unexpected finding of our study. Among patients whose disease remained confined to extra-hepatic sites, CDK5-high tumors exhibited a high increase in progression hazard, yet, this association was completely eliminated in patients with hepatic metastases. This spatially confined influence is not an artefact of sample size: the hepatic subset comprised 61 lesions with robust follow-up. Instead, the data mirror recent single-cell transcriptomic atlases that show liver-metastatic CRC cells down-regulate CDK5-dependent motility circuits while simultaneously up-regulating HGF-MET and LXR-APOE lipid-handling programs. 15 Mechanistically, the liver micro-environment appears to neutralize CDK5 through at least 2 validated pathways. First, hepatic stellate cell-secreted TGF-β triggers SMAD3-mediated nuclear translocation of CDK5, converting the kinase from a pro-migratory cytoplasmic signal into a transcriptional co-repressor of SLUG, 16 thereby attenuating epithelial-mesenchymal transition. 17 Second, CDK5 phosphorylates PDK1 at Thr346 within hepatocyte-conditioned matrices, 18 forcing tumor cells to abandon Warburg glycolysis in favor of oxidative phosphorylation and consequently reducing reactive oxygen species that otherwise fuel genomic instability. 15 Prior observations that CDK5 can behave as either an oncoprotein or a tumor suppressor depending on context were therefore extended by our results. In hepatocellular carcinoma, CDK5 amplification accelerates intra-sinusoidal dissemination via SLUG phosphorylation, 15 whereas in non-metastatic colorectal cancer cell lines, CDK5 knock-down paradoxically increases invasiveness through compensatory SRC-FAK activation. 16 It is now demonstrated that the liver itself acts as a privileged sanctuary where CDK5-driven aggressiveness is selectively disarmed. Consequently, future CDK5-centred biomarker panels must incorporate anatomic-metastatic stratification, and therapeutic strategies targeting CDK5 may only benefit patients with extra-hepatic disease. However, while tumor-agnostic biomarkers offer substantial promise for refining personalized therapeutic approaches in CRC, critical barriers persist regarding their clinical adoption. The absence of standardized molecular testing protocols, driven by heterogeneity in gene panel design, sequencing techniques, and bioinformatics analysis frameworks, introduces significant variability in biomarker detection and interpretive accuracy. Concurrently, tumor heterogeneity and adaptive resistance mechanisms—illustrated by alternative pathway activation in BRAF-mutant CRC—present major hurdles to achieving long-term treatment efficacy. These biological and technical constraints are further exacerbated by the financial demands of genomic profiling and disparities in testing accessibility, thereby restricting both the real-world utility and cross-population generalizability of agnostic biomarker strategies. 19
As a retrospective investigation, our study is subject to several inherent limitations: firstly, the retrospective construction of our tissue-microarray cohort precluded the synchronous acquisition of systemic immune parameters. Accumulating evidence indicates that intratumoral CD56+ natural killer (NK) cell density can modulate cetuximab efficacy irrespective of RAS/BRAF genotype. 20 Consequently, unmeasured heterogeneity in antibody-dependent cellular cytotoxicity (ADCC) capacity may have attenuated the true prognostic gradient conferred by CDK5, particularly in patients with liver-confined metastases where NK infiltration is intrinsically low. 20 Secondly, all specimens were procured from cetuximab-salvaged, chemotherapy-refractory cases—a context enriched for PIK3CA or PTEN aberrations that blunt anti-EGFR benefit. 21 Although dual wild-type RAS/BRAF status was mandated, definitive exclusion of latent PI3K/AKT signaling as a modifier of CDK5-survival associations is precluded by the absence of comprehensive phosphoproteomic data. Thirdly, single-institution reports attributing organotropic dissemination to distinct cytokine milieus are aligned with the restriction of CDK5 prognostic significance to extra-hepatic metastases 22 ; Validation within hepatic-metastasis-enriched registries is therefore imperative. Fourthly, subcellular localization (nuclear versus cytoplasmic) was not captured, yet emerging data ascribe opposing oncogenic properties to compartment-specific CDK5 pools. 23 However, to mitigate subjective bias, CDK5 immunostaining was independently evaluated by 2 gastrointestinal pathologists, with a senior consultant pathologist serving as an adjudicator for discrepant scores, and all assessments were blinded to clinical endpoints.
Capitalizing on the present findings, future work should adopt a rigorously integrated strategy to resolve the following unresolved mechanistic and translational questions: firstly, Prior study indicated that CDK5 loss can paradoxically enrich cancer-stem-cell pools under cetuximab pressure via compensatory RAS/ERK activation. 24 Functional validation is now required: patient-derived organoids (PDOs) from both hepatic and extra-hepatic sites should be subjected to inducible CDK5 knock-in/out followed by cetuximab ± oxaliplatin treatment to quantify stemness markers (ALDH1, LGR5) and apoptosis indices. Secondly, translation of CDK5 from prognostic descriptor to predictive determinant mandates prospective validation. A seamless adaptive phase II basket trial is envisioned, wherein cetuximab-refractory, RAS/BRAF-wild-type mCRC patients are randomized 1:1 to standard-of-care versus a first-in-class CDK5 inhibitor. Stratification factors will include metastatic topography (hepatic vs extra-hepatic) and tumoral CDK5 expression tertiles. Serial ultra-deep next-generation sequencing of circulating tumor DNA (ctDNA) will track KRAS/BRAF clonal evolution as an early pharmacodynamic surrogate for on-target efficacy and resistance.
It is indicated by the pronounced prognostic divergence between hepatic and extra-hepatic metastases that CDK5-mediated oncogenesis is not an intrinsic tumor cell property, but rather a phenotype sculpted by contextual cues within the metastatic microenvironment. 25 It is therefore hypothesized that canonical β-catenin signaling is amplified by CDK5 in cooperation with CXCL9/10-rich, T-cell-inflamed niches, whereas this interaction is attenuated by hypoxic, NK-cell-sparse hepatic microenvironments.
Conclusion
In summary, the study indicated that elevated CDK5 expression independently predicted abbreviated PFS and CSS (both P<0.05). It was revealed by stratified analyses that in patients with only extra-hepatic metastases, a statistically significant detriment to PFS was conferred by CDK5 overexpression; conversely, within the hepatic-metastatic subset, no survival discrepancy was discernible between high- and low-to-intermediate expression cohorts.
Supplemental Material
Supplemental Material - Topography-dependent Prognostic Value of CDK5 in Cetuximab-Treated, RAS/BRAF-wild-type Metastatic Colorectal Cancer: A Retrospective Tissue-Microarray Analysis
Supplemental Material for Topography-dependent Prognostic Value of CDK5 in Cetuximab-Treated, RAS/BRAF-wild-type Metastatic Colorectal Cancer: A Retrospective Tissue-Microarray Analysis by Qinghua Wang, Hongjuan Zheng, Zhijian Zheng, Bin Hu, Bingjing Jiang, Jianfei Fu and Ying Yuan in Cancer Control.
Footnotes
Acknowledgements
The authors have no additional acknowledgements to declare.
Ethical Considerations
This project and manuscript were reviewed and approved by the Ethics Committee of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine on June 22, 2022 (Approval number: 2022-43). The Ethics Committee of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine has waived the requirement for obtaining informed consent.
Author Contributions
Design and drafting the manuscript: Qinghua Wang, Hongjuan Zheng. Acquisition of data, collection and review of the literature: Zhijian Zheng. Pathological evaluation of tumour: Zhijian Zheng, Bin Hu, Bingjing Jiang. Critical revision of the manuscript for important content: Jianfei Fu, Ying Yuan.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jinhua Science and Technology Program (2022-4-086).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Original research data of the manuscript is available, if requested.
Supplemental Material
Supplemental Material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.