
Abstract
Introduction
The purpose of this study was to use a Virtual Community Engagement Studio (V-CES) model to develop and refine short message service (SMS) content in English and Spanish related to dietary quality, physical activity, and sleep hygiene intended for individuals with cancer and their caregivers.
Methods
Community expert stakeholders participated in an English or Spanish V-CES and provide actionable feedback on the content and delivery of 180 previously developed SMS messages.
Results
Participants were nine stakeholders representative of the Southern Arizona cancer care community (eg, survivors, caregivers, healthcare providers, community health workers). SMS as a health promotion intervention strategy in context of cancer survivorship was viewed as accessible and appropriate. Actionable feedback from the V-CES included using positive affirmations, incorporating motivational strategies, using relatable language, and emphasizing evidence. Spanish language SMS should consider regional context during translation. Stakeholders recommended that two SMS be sent daily to dyads between 8:00 am and 7:00 pm, at relevant times for each behavior.
Conclusion
Future research will test the SMS for feasibility and acceptability among survivor-caregiver dyads. The V-CES model is an innovative approach for developing and refining dyadic health behavior interventions and may be beneficial for future research to engage communities.
Keywords
Introduction
As of 2024, an estimated 18 million individuals with cancer and 3 million caregivers are living in the United States (US), 1 with numbers expected to increase as screening and available treatments continue to advance. Diet, physical activity, and sleep concordant with current recommendations for diet and physical activity from the American Cancer Society (ACS) 2 and sleep from the American Association of Sleep Medicine (AASM)/Sleep Research Society (SRS) 3 are associated with lower all-cause mortality in the general population. 4 Yet, few individuals with cancer and cancer caregivers currently meet these recommendations. 5
Diet, physical activity, and sleep behaviors are interconnected, mutually time exclusive, and modifiable. The health and related behaviors of individuals with cancer and their caregivers (dyad) are often interdependent while the cancer diagnosis and treatment are ‘teachable moments’ for key health behavior change.6,7 Thus, promoting behavior change for diet, physical activity, and sleep for the dyad simultaneously may result in more sustained behavior change, improving the long term health for both. 8 A dyadic approach to intervention also aligns with current national standards for cancer survivorship care that include assessing survivors’ health behaviors and providing appropriate strategies for needed behavior change, and to also assess the caregivers’ wellbeing and health behaviors regularly. 9
Digital health interventions, such as short message service (SMS) or text messages, are one promising approach for delivering such intervention. SMS are easy to implement, scalable, and accessible for many populations, including rural adults, as 98% of adults in the US own an SMS-enabled cellphone. 10 Among individuals with cancer, SMS is widely accepted for health behavior promotion. 11 While interventions may promote physical activity together with diet or sleep, many existing do not consider the co-occurrence of the three behaviors and intervene simultaneously. Behavioral interventions in the context of cancer control also should consider cultural aspects, 12 for example regional food practices and language spoken. 13 With Spanish being the second-most common language spoken in the US after English, 14 it is important to develop bilingual behavioral interventions for greater reach. Engaging stakeholders early in evidence-based health intervention development can result in effective and relevant interventions for to the community that can more rapidly translate into practice. 15 The Obesity-Related Behavioral Intervention Trials (ORBIT) model provides a framework for developing behavioral interventions in the context of chronic disease, wherein Phase 1 focuses on designing and refining the core intervention components. 16 Phase 1 of the ORBIT model is an ideal time to design the behavioral change content and engage stakeholders.16,17 Consistent with ORBIT Phase 1, this paper details the process of engaging community expert stakeholders to provide actionable feedback and recommendations on the refinement of a new dyadic SMS health behavior intervention designed according to the capability (C), opportunity (O), and motivation (M) model of behavior change (COM-B)18,19 to promote diet, physical activity, and sleep among English and Spanish speaking individuals with cancer and their caregivers.
Methods
SMS Content Development
We began by generating an English-language library of 180 SMS on dietary quality, physical activity, and sleep hygiene (60 per behavior) in accordance with ACS and AASM/SRS guidelines.2,3 All SMS content corresponded to the COM-B model for behavioral change. COM-B is a theoretical framework that purports three components that are necessary for behavior change to occur.18,19 COM-B was applied within ORBIT Phase 1 to classify the intervention components or behavior change techniques present in each SMS. 17 SMS were developed following best practices for broad reach across sociocultural factors including income and education which included (1) ≤ 160 characters per SMS and ≤3 SMS blocks per message; (2) ≤8th grade reading level; (3) theoretically informed behavior change approaches; and (4) cultural relevance. 20 SMS were initially drafted using generative artificial intelligence (ChatGPT 3.5, Open AI, San Francisco, USA) prompting, refined by the study team, and verified for accuracy by subject content experts (Principal Investigators). Initial SMS libraries were then translated into Spanish by a bilingual and bicultural member of the study team. Comprehensive details on the SMS development have been published elsewhere. 21
Virtual Community Engagement Studio
After drafting the initial SMS libraries, we next engaged community stakeholders to refine the messages prior to testing them in an intervention. We implemented procedures outlined in the Virtual Community Engagement Studio Toolkit 22 that our team previously used to adapt survivorship health behavior interventions. 23 The Community Engagement Studio (CES) model was originally developed by the Meharry-Vanderbilt Community Engaged Research Core (CERC) and provides a standardized, structured approach for collecting feedback on research materials and plans from key stakeholders with diverse perspectives on the question at hand. This model outlines a four-step process that includes (1) orienting attendees to the CES process; (2) presenting research materials for discussion; (3) facilitated discussion; and (4) structured evaluation. We conducted two separate virtual CES (V-CES) sessions, one in Spanish (12/02/2023) and one in English (12/04/2023) so each SMS library could be discussed in the intended recipient language.
Community stakeholders were identified from local outreach events and existing networks and included individuals with cancer, cancer caregivers, healthcare providers, public health professionals, and community health workers. All stakeholders voluntarily agreed to participate in the V-CES and all procedures were conducted in accordance with ethical guidelines. After completion of all V-CES activities, stakeholders were compensated $25 for their time.
Prior to the scheduled V-CES, all stakeholders were provided an orientation guide and access to the SMS libraries in the appropriate language. The V-CES sessions were held on Zoom for Healthcare (Zoom Video Communications, Inc. San Jose, CA), a HIPAA-compliant version of Zoom, and were led by a bicultural and bilingual facilitator. To begin the V-CES, a standardized recording was played that provided an overview of the intervention and goals for the SMS. Five questions guided the discussion: (1) “What are your thoughts on text messages as a way to promote multiple health behaviors?”; (2) “What are your thoughts about the themes within each health behavior?”; (3) “Imaging you were a participant in this study, how many messages would you want to receive each day and when?”; (4) “Why would you choose to participate in/refer a patient to a study using text messages to promote multiple health behaviors?”; (5) “What health outcomes are important to you?”. Each V-CES lasted approximately 90 min and was audio recorded. The facilitator also took notes to augment the transcription.
Statistical Analysis
Survey responses were summarized using descriptive statistics. Audio recordings from V-CES were transcribed verbatim in the original language. Rapid analysis procedures were used to identify actionable feedback from transcripts. 24 Two coders independently analyzed transcripts, highlighting exemplary quotes and key themes and identifying actionable feedback. After independently coding the transcripts, they compared their findings to achieve consensus. English and Spanish transcripts were analyzed in the original language. The coders and principal investigators then collaboratively organized the actionable feedback into themes.
Results
Community Expert Stakeholders
Twelve stakeholders (aged 26-70 years; 75% female, and 58% Hispanic) agreed to participate. Stakeholders self-identified as a cancer survivor (n = 2), family caregiver of someone with cancer (n = 3), healthcare provider (n = 3), or community health worker (n = 4). Of the 12 recruited stakeholders, nine participated in the V-CES sessions (five in English; four in Spanish). Three stakeholders did not participate due to scheduling conflicts.
Stakeholder Feedback
Overall, the feedback was positive for an SMS intervention and the specific SMS content. Stakeholders stated that SMS would be accessible and low cost to implement. Technological literacy and access were not concerns for stakeholders, as many believed individuals with various backgrounds would have the skills and ability to engage in an SMS intervention and that healthcare providers would be able to integrate. It was stated that SMS may be preferrable, as many patients and caregivers, especially older adults, struggle to access email or websites. SMS content was considered culturally sensitive and appropriate for individuals with cancer and caregivers. Stakeholders recommended that participants receive between one and three SMS per day, and that a frequency of two messages per day for each behavior was considered adequate and enough to maintain engagement without imposing excessive burden. They recommended to schedule delivery for both the survivor and caregiver to receive the same SMS at relevant times for the behavior to maximize engagement. It was suggested that when appropriate, starting with more SMS at the beginning of the intervention and then decreasing frequency may reduce participation fatigue and should be considered.
Exemplar Quotes and Actionable Feedback
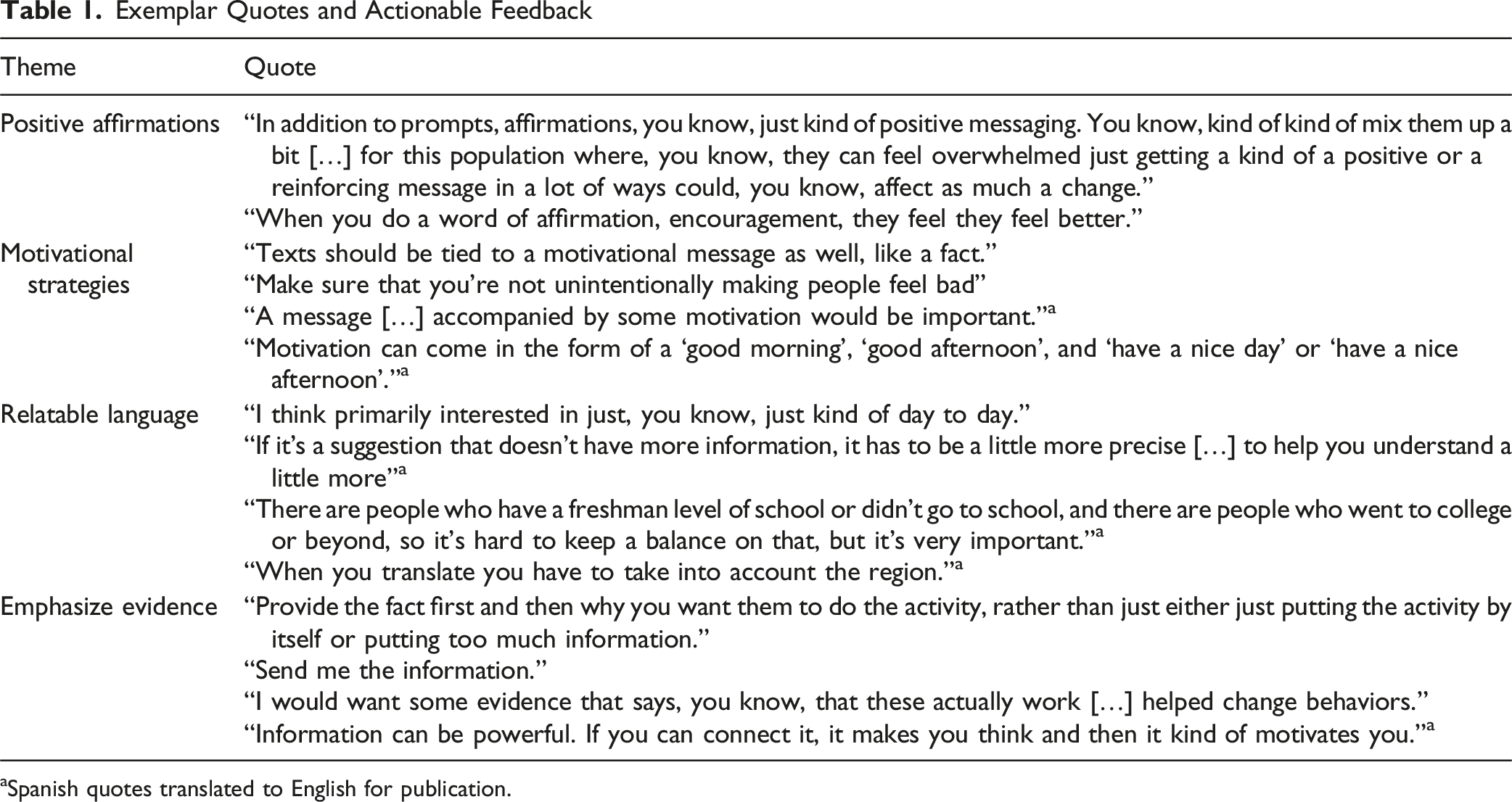
aSpanish quotes translated to English for publication.
Integrating Stakeholder Feedback into SMS Revisions
Changes to SMS included simplifying sentence structure, focusing on actionable suggestions, ensuring shame-free messaging, and highlighting relevance to daily activities. The Spanish SMS required more extensive revisions to make language less formal and to integrate more common terminology and Spanish colloquialisms. SMS content was revised to incorporate more regional foods and activities. The final SMS libraries included the following themes for each health behavior: Dietary Quality - food groups (example: “Choose whole fruits over fruit juices to increase fiber and help stabilize blood sugar. Try eating an orange instead of drinking a glass of orange juice. You may notice a difference!”), beverages, food preparation, mindful eating, grocery shopping, macronutrients, vitamins & minerals, and other phytochemicals; Physical Activity - increasing activity strategies (example: “Break up your day with activities like walking/stretching for 5 min. This is especially helpful on days with a lot of sitting or lying down.”), exercise benefits, exercise tips, types of exercise, play activities, and rest & recovery; and Sleep Hygiene - sleep schedule (example: “Prioritize your well-being with a good night’s sleep! Set a regular bedtime that allows for 7-9 h of rest.”), screen time, sleep-wake cycles, bedroom environment, wind-down practices, health-related, food-related, and activity-related. We coded all revised SMS to COM-B domains per stakeholder recommendations (Figure 1). Across behaviors, all COM-B domains were represented. Approximately one third of the final SMS targeted motivation (31%), 43% targeted capability, and 21% targeted opportunity. The greatest source of behavior change was physical (58%). When considering intervention function, the largest portion of SMS were educational (38%). Coding behavior change strategies in SMS following capability (C), opportunity (O), and motivation (M) for behavior (B) change (COM-B) domains
Discussion
We developed and refined a library of health education SMS to promote dietary quality, physical activity, and sleep hygiene behaviors among English and Spanish speaking individuals with cancer and their caregivers using a V-CES model. Actionable stakeholder feedback and recommendations ensured that SMS in both languages included positive affirmations, motivational strategies, relatable language, and emphasized evidence. Stakeholders also recommended that SMS frequency be twice daily at relevant times. For example, dietary quality and physical activity SMS may be scheduled for delivery at 7:00 am (to set intention for the day) and 3:00 pm (‘midday dip’) while sleep hygiene SMS may be scheduled for delivery and at 7:00 am (wake up) and 7:45 pm (end of day reflection). This formative research was consistent with ORBIT Phase I, providing key information to establish intervention content, protocols, and procedures. 16 As the next step (ORBIT Phase II), SMS will be tested for feasibility and acceptability in a pilot dyadic intervention for English- or Spanish-speaking individuals with any cancer and their caregivers.
This study contributes to the literature on development of SMS interventions for health behavior change in cancer survivorship. SMS have been extensively used as a strategy for health promotion trials in cancer survivorship. 11 We engaged stakeholders early in intervention development using a V-CES model to systematically collect stakeholder feedback and recommendations on expert-drafted SMS for diet, physical activity, and sleep. Our approach was similar to that used by Singleton et al, who co-designed a SMS strategy to increase health self-efficacy among individuals with breast cancer. 25 Their SMS intervention was later tested and was found to be feasible, acceptable, and low-cost to deliver. 26
Our SMS were coded to COM-B18,19 in alignment with stakeholder recommendations. Doing so will highlight which behavior change strategies (eg, motivation) may be most acceptable and influence intended behavior change. SMS may be limited in effects on health behavior change and relevant clinical outcomes without additional support. However, when paired with health coaching and/or activity trackers, SMS interventions have demonstrated significant improvement in dietary change, physical activity, sleep quality, and quality of life. 11 SMS may be an ideal strategy to implement health behavior education as a supportive service to survivors and caregivers in alignment with current survivorship care standards 9 as stakeholders suggested that SMS were easy to access and able to be integrated and delivered by healthcare providers. Interventions may integrate multiple modalities of behavior change support, including coaching combined with SMS as part of a comprehensive survivorship care plan. Future research should consider distal effects of SMS health behavior change interventions on relevant clinical outcomes for survivors and caregivers like mental health, symptoms (ie, pain, fatigue), and quality of life, as these were highlighted by stakeholders.
Limitations
Our findings may be limited by sampling bias in the selection of expert community stakeholders through existing research networks and community partnerships. While our cohort of stakeholders was representative of the cancer community in Southern Arizona, including diversity in age, gender, background, and experiences, our findings may not be generalizable to other regions or all cancer types.
Conclusion
Stakeholder feedback utilizing a V-CES model provided key recommendations to inform the refinement of SMS content and delivery within a multiple health behavior intervention for individuals with cancer and their caregivers. V-CES may be beneficial for the development of adaptation of other supportive care interventions intended for diverse cancer survivorship and caregiving populations with various needs.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of the community expert stakeholders. We would also like to thank Bianca SantaMaria, Aleyia Gabriel, and Anastasia McCleary for their support in this research. This research was funded by the University of Arizona Cancer Center Cancer Prevention and Control Program Pilot Grant (MPI: Skiba/Fox). RSF was funded by the National Cancer Institute (K08247973; PI: Fox).
Ethical Considerations
This research did not meet the criteria for human subjects research as determined by the Institutional Review Board at the University of Arizona (#0003817). All participating community stakeholders provided their agreement to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Division of Cancer Prevention, National Cancer Institute (K08247973), University of Arizona Cancer Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study, including the SMS libraries developed from this study are not publicly available but are available from the corresponding author on reasonable request.