
Abstract

Approximately 1 in 5 men or women develop cancer in a lifetime, whereas around 1 in 9 men and 1 in 12 women died from it in 2022. 1 The number of new cases of cancer is predicted to rise dramatically reaching 35 million by 2050, representing a 77% increase from 2022. 1 By 2050, up to 70% of cancer deaths are expected to be in low-and-middle-income countries (LMICs); a disproportionate impact in countries with severe resource constraints.
Meanwhile, cancer screening, early detection, diagnosis and treatment availability remain grossly inadequate in the majority of LMICs. For example, in the 2023 WHO country capacity assessment survey for prevention and control of noncommunicable diseases, organized population -based cervical cancer screening and radiotherapy were reported as available in less than a third of low-income countries. 2 Most LMICs are unable to afford many cancer medicines sustainably, especially newer targeted therapies and immunotherapies. Targeted therapies may cost $50,000–$200,000 per patient per year in high-income countries. 3 The median annual government health expenditure per person in low-income countries is often less than $100 — a fraction of the cost of one cancer treatment course. Notably, in 2021 the share of the world’s population living in countries with health spending per capita less than US$100 was around 39%. 4 This share has changed little over the last decade. Multifaceted challenges impede cancer control in LMICs- shortages in oncology workforce, screening services, diagnostic infrastructure, access to treatment, high out-of-pocket costs and social inequities. 5 These are unlikely to be adequately addressed to significantly improve cancer outcomes in the foreseeable future.
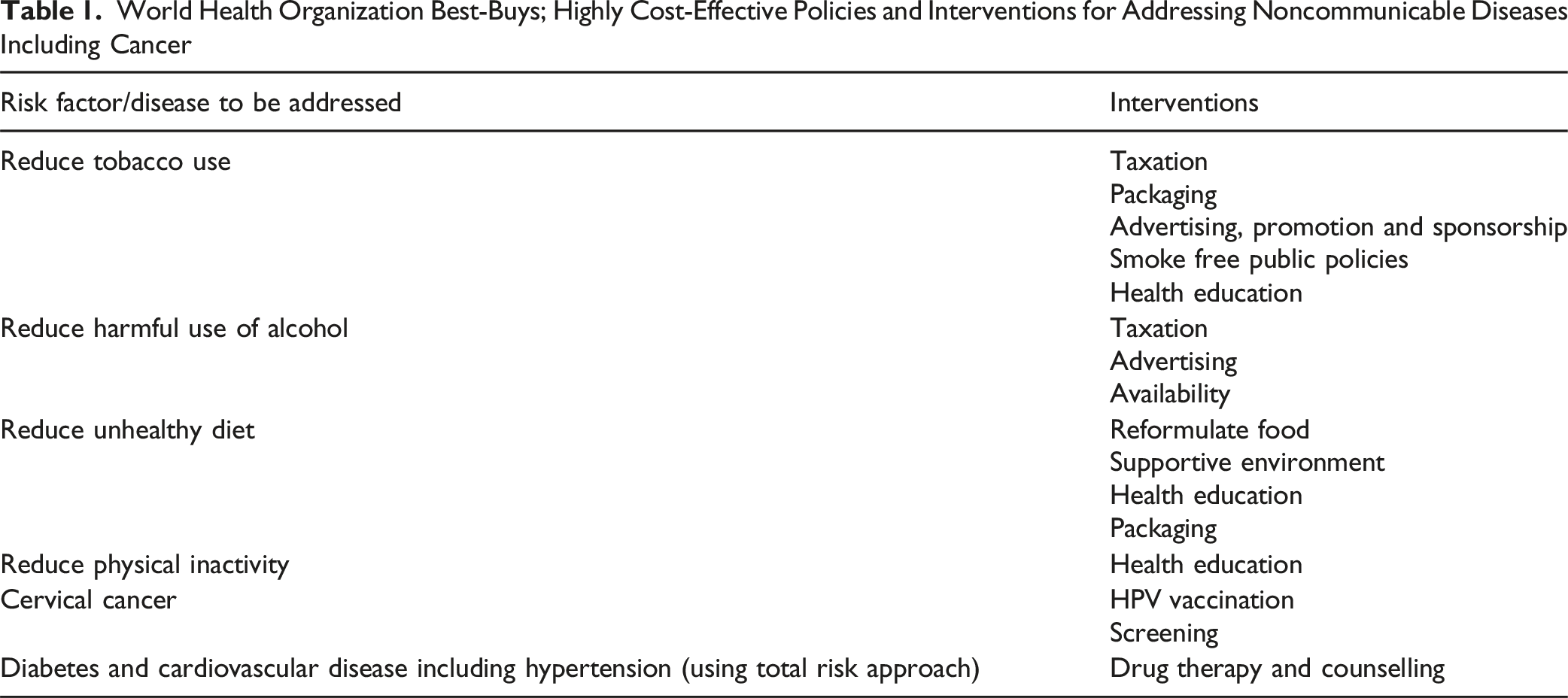
World Health Organization Best-Buys; Highly Cost-Effective Policies and Interventions for Addressing Noncommunicable Diseases Including Cancer
In addition, the WHO Framework to Implement a Life Course Approach in Practice 6 provides a valuable guide to operationalizing these prevention efforts. It calls for person-centred, equity-driven and systems-integrated actions that connect health promotion, environmental protection and social policy from early development to older age. Applying these principles to cancer prevention means ensuring that children grow up in environments free from carcinogenic exposures, adolescents are equipped with health-promoting skills, and adults have sustained opportunities to reduce risks and build resilience, including maternal and paternal health that not only impacts the health of their children, but shapes ageing as older adults.
Policy choices can address in appropriate disposal of hazardous waste as this adds carcinogens to air, water and soil. In 2022 global hazardous waste generation was estimated at 300-500 million metric tons annually. Hazardous waste characterized by toxicity is produced in manufacturing, household, healthcare, agriculture, industry, construction, mining and nuclear sectors. Yet, on a global scale effective recycling of waste remains minimal. Moreover, greater solidarity is needed: in 2022 high-income countries sent some 3.3 billion kilograms of e-waste and used electronics to LMICs through uncontrolled transboundary movements. 13 Dumping, open incineration and informal recycling of waste are emitting hazardous heavy metals and other carcinogens such as dioxins, into the environment increasing the risk of cancer.
Policies and interventions (Figure 1) that have the potential to prevent cancer across the life course as well as other noncommunicable diseases that share the same risk factors are also underutilized by many LMIC governments. Consequently, prevalence of obesity as well as other noncommunicable diseases including cancer are rising.
14
Obesity increases the risk of several types of cancer. Hepatitis B virus (HBV) and Human Papilloma Virus (HPV) vaccines reduce the risk of cancer by strengthening the body’s immune system and providing protection. HPV Vaccination of adolescent girls is the most effective long-term intervention for reducing the risk of developing cervical cancer.
15
Yet, only an estimated 13% of adolescent girls globally are fully vaccinated at present.
16
Although more than 85% of cervical cancers worldwide are detected in LMICs, only 40% of them have introduced HPV vaccination.
15
High vaccine prices coupled with health system challenges have significantly constrained the ability of many LMICs to introduce HPV vaccine into national immunization programmes (Table 2).17,18 Implementing a life course approach for primordial prevention of cancer: Policies and interventions (They also contribute to primordial prevention of cardiovascular disease) Key Barriers to Achieving the Necessary Uptake of HPV Vaccination in LMICs and Strategic Actions to Overcome Them

In order to operationalize a life course approach for primordial prevention of cancer, policymakers need to implement the following: (1) Health promotion interventions to address risk factors of cancer (eg, tobacco, alcohol, physical inactivity, unhealthy diet, obesity) embedding them within maternal and child health services, schools, workplaces, primary health care and community programs minimizing barriers to access for underprivileged groups and giving due attention to social determinants (Figure 1). (2) Public policies, taxes and regulations to support the implementation of population-based interventions to control the drivers and determinants of cancer risk (eg, tobacco, alcohol, physical inactivity and unhealthy diet) across the life span (Table 1). (3) Incorporation of HPV and HBV vaccination and health promotion interventions within national Universal Health Coverage (UHC) benefit packages and strategic actions to overcome barriers to HPV vaccination (Table 2). (4) Policies for effective management of air pollution and hazardous waste through surveillance and regulatory frameworks, public awareness, and global cooperation giving priority to waste reduction
Monitoring and evaluation are crucial for success and LMICs need to reinforce appropriate information systems for tracking alcohol and tobacco consumption, obesity, physical inactivity, HPV and HBV vaccination, occupational and environmental carcinogens as well as cancer incidence. In recent years, several low-income countries eg, Bangladesh, Bhutan, Ethiopia, Ruwanda, Tanzania and others have achieved high HPV vaccination coverage through strategic planning, community-tailored approaches, and high-level political commitment. Effective HPV vaccine roll-out was facilitated in these countries through partnership with GAVI (ensured affordability and financing), UNICEF (handled procurement and delivery) and World Health Organization (provided global leadership and technical guidance).
LMICs are on different points in the level of financing of health systems, health-workforce capacities and organization of primary health care services. However, all ministries of health have opportunities to start operationalizing a life course approach for primordial prevention of cancer through existing services and collaboration with other Ministries and international organizations. Investments in primordial prevention, by tackling key risk factors for cancer (including tobacco, alcohol, unhealthy diet, physical inactivity, HPV and HBV infections, air and environmental pollutants), could avert millions of new cancer cases, make cancer control sustainable and equitable while saving many lives and bringing economic as well as societal dividends to LMICs.
Footnotes
Author Contributions
SM drafted the manuscript. All authors revised the draft manuscript critically for important intellectual content. The views expressed in the paper are solely the responsibility of the authors and they do not necessarily reflect the views, decisions, or policies of the institutions with which they are affiliated.
AI statement
Artificial Intelligence was not used.