
Abstract
Introduction
Abundant research documents Black-White disparities in the quality of patient-physician clinical communication during oncology interactions. Prior research shows that Black patients’ and non-Black physicians’ race-related attitudes and perceptions influence clinical communication and patient and physician perceptions of one another. The aim of this cross-sectional study was to determine the effects of such attitudes and perceptions on another important but understudied aspect of interpersonal communication—nonverbal synchrony. The attitudes and perceptions included non-Black physician implicit racial bias; and Black patients’ suspicion of medical care Black patients receive, trust in healthcare systems, and previous experience with discrimination. We predicted that patient and physician race-related attitudes and perceptions would be associated with various nonverbal synchrony measures during oncology interactions between Black patients and non-Black physicians.
Methods
This was a secondary analysis of video-recorded cancer treatment discussions between Black patients and their non-Black physicians collected as part of a larger study. Participants included 66 Black patients and 13 non-Black physicians. Physician implicit racial bias and demographic characteristics and Black patient race-related attitudes, perceptions, and demographic characteristics were assessed prior to the interactions. Using automated motion energy analysis software, we evaluated three measures to examine nonverbal synchrony: (1) global nonverbal synchrony, (2) patient-led nonverbal synchrony, and (3) physician-led nonverbal synchrony.
Results
We found positive relationships between physicians’ implicit racial bias and all measures of nonverbal synchrony. We found a positive relationship between one patient attitude (trust in healthcare systems) and one nonverbal synchrony measure (patient-led nonverbal synchrony).
Conclusions
Findings provide evidence of a link between Black patient and non-Black physician race-related attitudes and perceptions and their jointly determined nonverbal synchrony during clinical interactions. Further work is needed to understand the nuances and clinical implications of this complicated relationship, and to inform potential interventions to improve communication quality and related patient outcomes.
Keywords
Introduction
Decades of research across many medical contexts, including oncology, demonstrate that Black people generally experience poorer quality communication with their physicians than White people.1-5 Communication disparities likely contribute to similarly well-documented racial treatment disparities, and, in turn, poorer health and greater mortality rates among Black relative to White patients.6-8
Race-related attitudes and perceptions held by non-Black physicians and Black patients have been shown to contribute to communication disparities and related short- and longer-term outcomes.9-11 As detailed in a previous paper describing the conceptual model and methods used in this current study, 12 much of this research has focused on a few influential attitudes and perceptions: non-Black physicians’ implicit racial bias; and Black patients’ suspicion of medical care Black patients receive, trust in healthcare systems, and previous experience with discrimination.
Implicit biases are feelings and beliefs that are automatically and spontaneously activated and are more difficult to control 13 than explicit biases.14-17 Higher levels of oncologist implicit racial bias preferring White people over Black people are associated with lower quality communication with Black people with cancer, including shorter treatment discussions and less patient-centered communication, which, in turn, negatively influence other important patient outcomes (eg, reduced confidence is recommended treatment).18-21
Black patients with higher levels of suspicion about the care Black people are likely to receive are less optimistic about outcomes of recommended treatments and are perceived by their physicians as less educated. This perception is, in turn, associated with lower physician expectations about the extent to which their Black patients will adhere to or tolerate a recommended treatment. 22 Black patients with higher levels of previously experienced discrimination tend to be more verbally active while communicating with non-Black physicians, which has been interpreted as an attempt to verbally control the interaction and prevent further discrimination. 22 Research has also identified positive relationships between Black patients’ trust in their physician and the healthcare system and patient-provider communication quality, highlighting the importance trust plays for Black patients when they communicate with their providers and interact with a healthcare system.23,24
Clinical communication disparities research has typically focused on verbal communication (eg, physicians’ patient-centered communication) with a few exceptions.25-27 This is despite the critical role that nonverbal communication plays in creating, defining, and managing patient-physician relationships.28-32 The little research that has investigated nonverbal clinical communication mainly examines discrete patient and physician nonverbal behaviors (eg, eye gaze, smiling). However, researchers have yet to examine nonverbal behaviors that are part of the dynamic interplay between patients and physicians when they interact.27,33
An important nonverbal aspect of interpersonal communication is nonverbal synchrony, or the nonconscious coordination of behavior between individuals during an interaction, which is a dynamic and jointly determined phenomenon.12,34 Nonverbal synchrony is distinct from mimicry in that it involves meaningful temporal association between similar kinds of motion.35-37 Some examples are when a patient leans toward their physician, the physician walks closer to the patient; and when a patient lowers and shakes their head, the physician shifts their posture in the direction of the patient. 35
Although nonverbal synchrony is largely nonconscious, unintentional, and effortless, it plays a role in several critical aspects of interpersonal relationships.37-42 Research outside of clinical settings has identified positive relationships with nonverbal synchrony that are likely important for the clinical context including cooperation, 43 adherence, 40 and recollection of what transpired during an interaction.42,44 In a clinical context, however, findings are mixed regarding whether nonverbal synchrony has an exclusively positive role.45-47 In psychotherapy sessions between White patients and White therapists, high levels of nonverbal synchrony occur when a patient displays more aggressive and confrontational behavior and a therapist displays higher levels of attention. 48 A recent meta-analysis of 11 studies which assessed nonverbal synchrony in psychotherapy found that nonverbal synchrony was positively associated with patients’ perceived alliance with the psychotherapist, but not associated with therapeutic outcomes. 49 There is also evidence that nonverbal synchrony can help repair strained relationships, but that process is not well-understood. 38 Thus, it is unclear whether nonverbal synchrony has a consistent function in clinical communication and related outcomes or if its function(s) differ based on the racial composition or other characteristics of the patient-physician dyad or context.
To further explore nonverbal synchrony in a clinical context, Hamel and colleagues 34 compared video-recorded clinical interactions between White or Black patients with cancer and their non-Black oncologists. 37 Interestingly, the study found higher levels of nonverbal synchrony between Black patients and non-Black physicians than between White patients and non-Black physicians. They then examined whether this pattern persisted when patients’ nonverbal behaviors led or followed physicians’ nonverbal behaviors. They found that levels of nonverbal synchrony were highest in interactions with Black patients and their physicians when the patient led and the physician followed, but no associations with leading/following behavior were found for White patients. 34 These findings again indicate that nonverbal synchrony is a complex interpersonal process. Hamel and colleagues speculated that these differences may indicate that non-Black physicians are nonconsciously adapting their behavior to their Black patients’ behavior to interpersonally bridge a perceived racial divide. The current study extends this earlier research on nonverbal synchrony by analyzing some of the same data to examine the extent to which nonverbal synchrony is influenced by patient and physician race-related attitudes and perceptions during clinical interactions between Black patients and non-Black physicians.
The following is hypothesized regarding the associations for physicians’ implicit racial bias:
During clinical interactions, non-Black physicians’ levels of implicit racial bias will be: (a) negatively associated with global nonverbal synchrony levels and (b) patient-led nonverbal synchrony levels and, (c) positively associated with physician-led nonverbal synchrony levels. Given what is known regarding the influence of Black patients’ race-related attitudes and perceptions on clinical communication with non-Black physicians, their perceptions of non-Black physicians, their non-Black physicians’ perceptions, and our previous nonverbal synchrony research, the following associations for patients’ race-related attitudes and perceptions are predicted:
During clinical interactions, Black patients’ levels of suspicion of medical care Black patients receive will be: negatively associated with (a) global nonverbal synchrony levels, (b) positively associated with patient-led nonverbal synchrony levels, and negatively associated with (c) physician-led nonverbal synchrony levels.
During clinical interactions, Black patients’ experience with previous racial discrimination will be: negatively associated with (a) global nonverbal synchrony levels, (b) positively associated with patient-led nonverbal synchrony levels, and negatively associated with (c) physician-led nonverbal synchrony levels.
During clinical interactions, Black patients’ levels of trust in healthcare systems will be: positively associated with (a) global nonverbal synchrony levels, (b) patient-led nonverbal synchrony levels, and (c) physician-led nonverbal synchrony levels.
Methods
Reporting of this study conforms to STROBE guidelines. 50
Participants and Procedures of the Parent Studies
Data included video-recorded interactions and associated self-report data from a parent study conducted between April 2012 and December 2014 at a National Cancer Institute-designated comprehensive cancer center and another large cancer center located in an urban Midwestern city with a majority Black population. The parent study investigated associations between communication and outcomes during initial oncology treatment discussions between Black patients and their non-Black physicians. 51 All patients were newly diagnosed and were meeting their medical oncologist for the first time.
Physicians were eligible to participate if they provided medical oncology treatment for patients with breast, colon, or lung cancer at a participating cancer center. Patients were eligible if they (1) self-identified as Black, African American, or Afro-Caribbean; (2) were between the ages of 30 and 85 years of age; (3) had a diagnosis of breast, colon, or lung cancer; (4) could read and understand English well enough to provide informed consent and complete questionnaires; and (5) had an appointment within 2 weeks to see a participating physician for an initial discussion of medical treatment. Patients and physicians who provided consent to allow their data, including video recordings, to be used in secondary analyses were included in the current study. All study procedures for the current study were approved by IRBs at both cancer centers and the affiliated university.
For the parent study, 51 upon consent, patients provided sociodemographic information and completed several measures, including suspicion of medical care Black patients receive, 52 trust in healthcare systems, 53 and experiences of previous racial discrimination. 54 Physician participants provided sociodemographic and professional information and completed several measures including an assessment of their racial implicit bias at enrollment. 47 Interactions between patients and physicians occurred within two weeks of the patients’ consent and were video recorded. Details regarding procedures for the parent study are provided elsewhere.27,51
Participant Demographics a
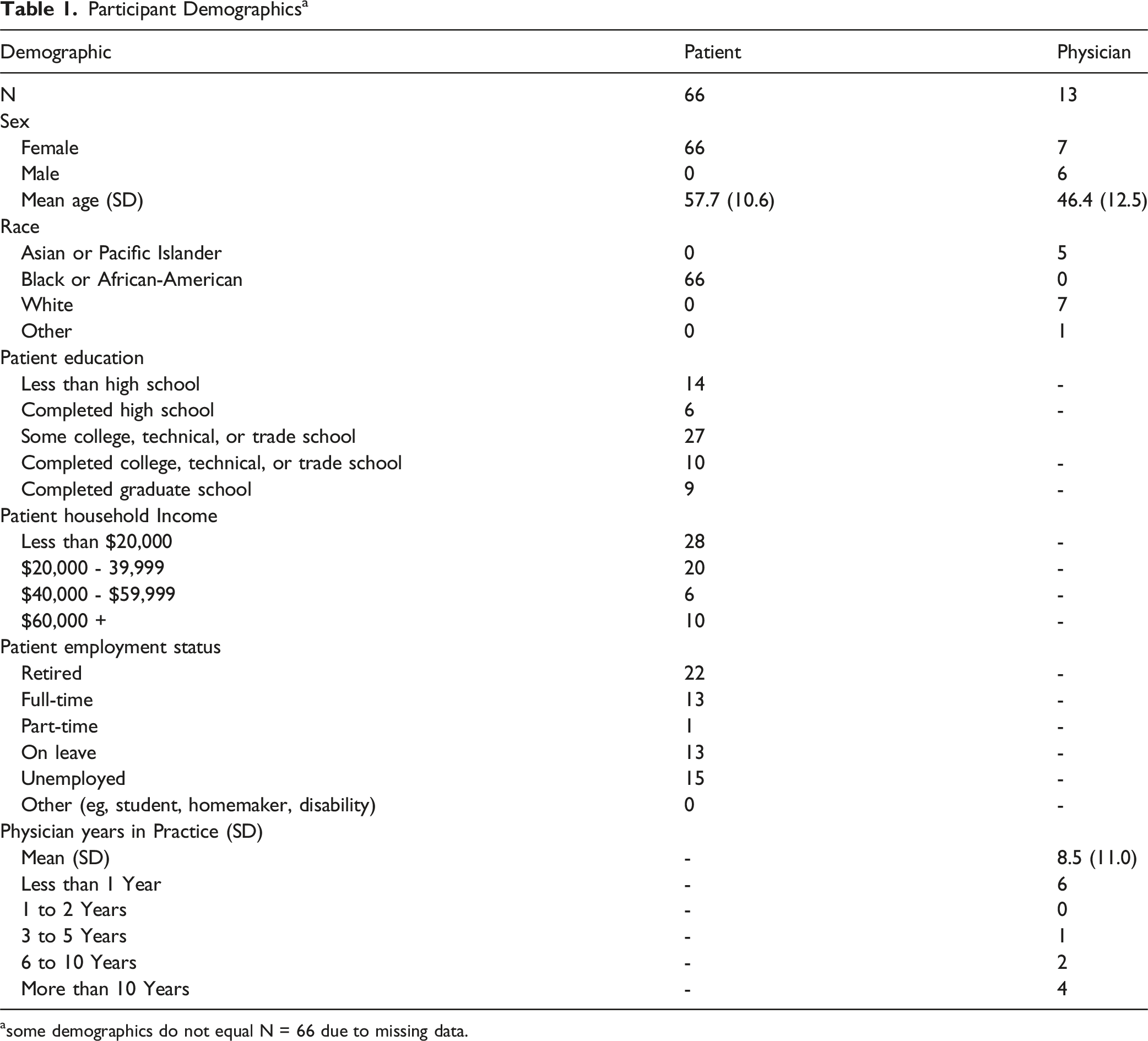
asome demographics do not equal N = 66 due to missing data.
Study Procedures
Data for this analysis included patient and physician self-reported demographic characteristics, their race-related attitudes and perceptions and video-recordings of patient-physician cancer treatment discussions. The software (described below) used to assess nonverbal synchrony requires the individuals being tracked to remain in pre-defined areas in the video. As these were naturally occurring interactions, patients and physicians sometimes moved about the exam room, potentially affecting nonverbal synchrony analyses. To address this, we edited the full interactions into smaller, five-minute segments to allow us to reposition the pre-defined areas of assessment in the video in the cases when a physician or patient moved outside the pre-defined areas of assessment. 48 To illustrate, an interaction that was 23 min long was edited to have four five-minute segments and one three-minute segment, and the software was repositioned at the start of each new segment. For privacy, in selecting the segments, portions that included patient physical exams during the interactions were excluded. 27
Assessing Nonverbal Synchrony
We assessed nonverbal synchrony using Motion Energy Analysis (MEA) software,
55
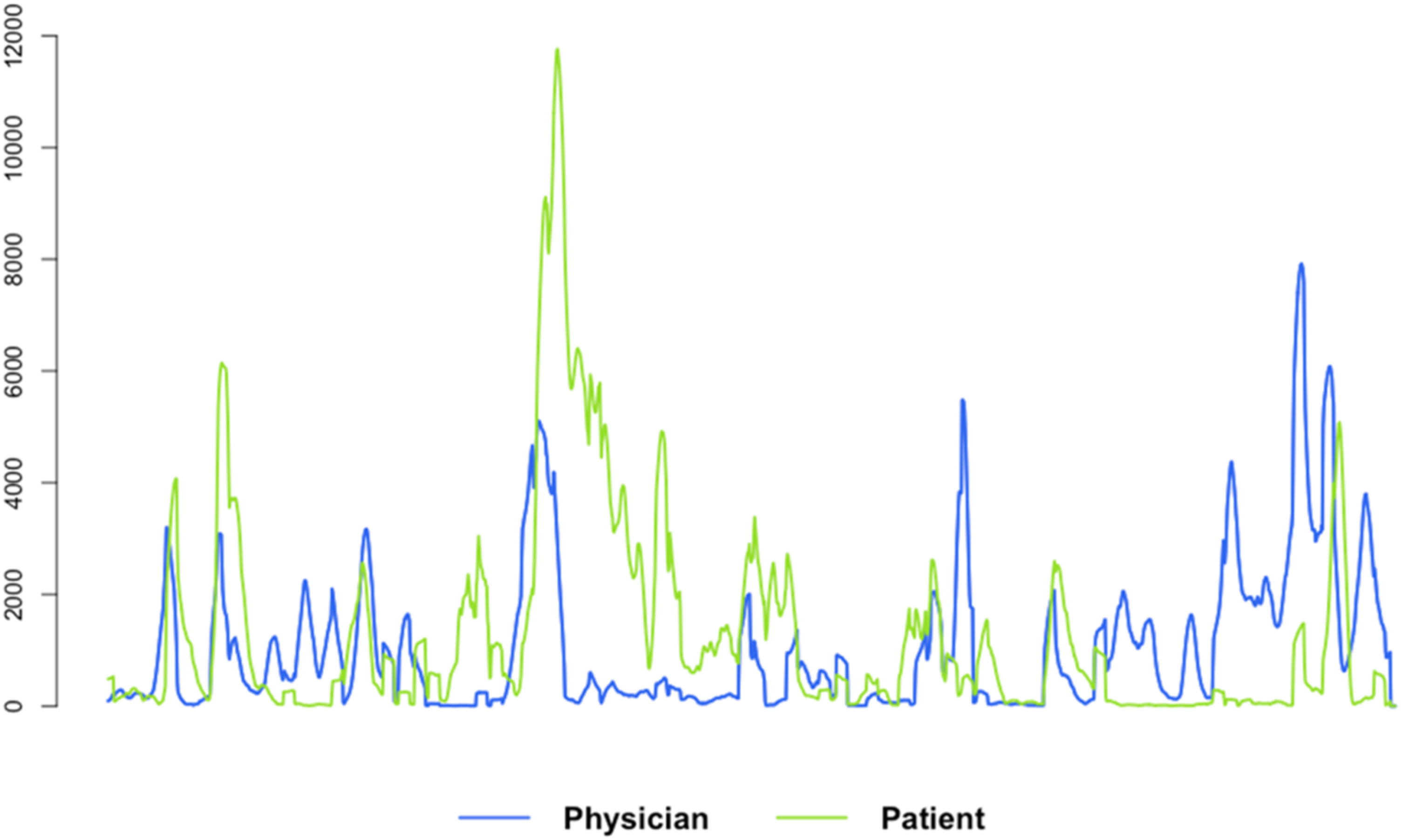
which provided time series data representing the amount of motion observed in the clinical video recordings. MEA measures the extent to which pixels in a video recording change over time. It is an automated method that continuously monitors the amount of change in pre-defined regions of interest (eg, the patient and physician), thus quantifying movement occurrence. Nonverbal synchrony scores represent the amount and direction of influence of synchronous movement within interactions. We considered each individual (ie, patient or physician) in the interactions as one region of interest to capture full body movement. As nonverbal synchrony levels tend to ebb and flow during conversations, we used windowed cross-correlation to measure the changing synchrony levels that occurred in the interactions by comparing small sections of time at different time lags.56,57 By identifying multiple smaller sections at different time lags, windowed cross-correlation provides an estimate of synchronization between systems that do not have a constant lag, as occurs in this study with two people having a discussion. Figure 1 provides an example of MEA time series data. Example Motion Energy Analysis Time Series of Movement
1
Nonverbal Synchrony Outcomes

Data Analysis
We used linear mixed-effects models to analyze the influence of individual attitudes and perceptions on nonverbal synchrony outcomes using R analytic software. 58 Patient and physician nonverbal synchrony outcomes from each video-recorded segment were nested within the interaction with an additional random effect by physician to account for variation between interactions and individual physicians. MEA output was used to obtain bivariate time series of motion (one time series for the patient and one for the physician; see Figure 1). Flat lines indicate no movement; spikes and peaks represent movement. We assessed nonverbal synchrony occurring within a 4-second time frame (ie, patient leading/following up to two seconds or physician leading/following up to 2 s) in windows of 4 s duration.35,59
Individuals often repeat behaviors within conversations. For example, throughout a conversation individuals may shift their posture many times or smile and nod frequently, but not in a coordinated way. Given this, time series data from human behavior may show spurious (not coordinated) nonverbal synchrony values even when nonverbal synchrony is not present. This “pseudo-synchrony” is problematic and can lead to false conclusions because hypothesis-testing of synchrony between any two-time series assumes the time series are in synch with one another. To avoid this, a surrogate analysis was first conducted to obtain a reliable measure for detecting “real synchrony” vs “pseudo-synchrony.” In a surrogate analysis framework, a large number of pseudo-pairs are generated by randomly matching patients’ data from one interaction with physicians’ data from a different interaction (ie, an interaction between a patient and physician who did not actually interact).35,57
Results
Nonverbal synchrony outcomes were first assessed for pseudo pairs and the results were compared to the results of the nonverbal synchrony outcomes obtained from our actual pairs. A significant difference indicates that observed nonverbal synchrony outcomes in actual pairs are higher than expected by chance. The surrogate analysis showed observed nonverbal synchrony outcomes were more significantly different than the chance distribution; Δ|zCCF| = .08, z = 3.43, P < .001.
Before testing the hypotheses, the correlation between physician-led nonverbal synchrony and patient-led nonverbal synchrony was examined, which was positive and significant as expected (r(64) = 0.64, 95% CI [.58-.70]). These models account for dyad-level differences and, thus, cannot produce separate models for patients and physicians. A post-hoc power analysis could not be computed because this is a secondary analysis.
Hypothesis One
Linear Mixed-Effects Models of the Influence of Attitudes and Perceptions on Nonverbal Synchrony Outcomes

Bold denotes significance.
CI, confidence interval.
Summary of Relationships Among Attitudes and Perception and Nonverbal Synchrony Outcomes

Hypothesis Two
We predicted that during clinical interactions, Black patients’ levels of suspicion of medical care Black patients receive would be: negatively associated with (a) global nonverbal synchrony levels, (b) positively associated with patient-led nonverbal synchrony levels, and negatively associated with (c) physician-led nonverbal synchrony levels. Results were not consistent with H2 a, b, or c as we found no significant associations between patient suspicion and the nonverbal synchrony outcomes (Tables 3 and 4).
Hypothesis Three
We predicted that during clinical interactions, Black patients’ previous experience with racial discrimination would be: negatively associated with (a) global nonverbal synchrony levels, (b) positively associated with patient-led nonverbal synchrony levels, and negatively associated with (c) physician-led nonverbal synchrony levels. Results were not consistent with H3 a, b, or c as we found no significant associations between patient previous experience with racial discrimination and the nonverbal synchrony outcomes (Tables 3 and 4).
Hypothesis Four
We predicted that during clinical interactions, Black patients’ levels of trust in healthcare systems will be: positively associated with (a) global nonverbal synchrony levels, (b) patient-led nonverbal synchrony levels, and with (c) physician-led nonverbal synchrony levels. We found a positive relationship between patient-led nonverbal synchrony and patient trust but no relationship between patient trust and global nonverbal synchrony or physician-led nonverbal synchrony (Tables 3 and 4). Thus, results were not consistent with H4a or c but were consistent with H4b.
Supplementary materials provide the within subject correlation matrix (Table S1) and the between subject correlation matrix (Table S2).
Discussion
Findings from this study demonstrate potentially important ways that race-related attitudes and perceptions of Black patients and non-Black physicians can influence patient-physician clinical communication—through nonverbal synchrony, an understudied aspect of nonverbal communication. Patient-physician communication is how healthcare, information, and treatment decisions are transacted. These findings provide new insights into how race-related attitudes and perceptions may affect clinical communication and contribute, in turn, to better or poorer treatment and treatment-related outcomes.
A major finding of this study builds upon prior research documenting the numerous effects of non-Black physician implicit bias on interactions with Black patients.18-20 Findings show that this powerful race-related attitude influences even subtle, jointly-determined, nonverbal, dynamic aspects of patient-physician communication. Contrary to our predictions, we found that levels of non-Black physicians’ implicit racial bias were positively related to all three outcomes representing aspects of nonverbal synchrony (global nonverbal synchrony, patient-led nonverbal synchrony, and physician-led nonverbal synchrony). In other words, non-Black physicians with higher levels of implicit racial bias had more, not less, synchrony with Black patients. This surprising finding adds to a mixed literature on whether higher levels of nonverbal synchrony are exclusively a positive relationship indicator in a clinical setting.45,46,48 To summarize this literature, higher levels of nonverbal synchrony in clinical relationships may: indicate attempts to manage perceived or anticipated tension in relationships, can occur when a patient displays more aggressive and confrontational behavior and a therapist displays higher levels of attention, 48 and be positively associated with a patients’ perceived alliance with their psychotherapist. 49 These findings could potentially be due to the complex nature of high-stakes clinical relationships.
In contrast, Black patient attitudes and perceptions had little effect on nonverbal synchrony. Although we examined several race-related attitudes and perceptions among Black patients in this sample, the only significant association we found was a positive relationship between patient trust and one aspect of nonverbal synchrony (patient-led). We contextualize this finding by considering a series of studies conducted by Bergsieker and colleagues 60 comparing same-race and inter-racial interactions using self-report and observational behavior. They found that people from different racial groups often have divergent goals in the impressions they aim to make in interactions. They concluded that people of color tend to seek to be respected and seen as competent in inter-racial interactions, whereas White people tend to seek to be liked and viewed as moral in inter-racial interactions. They also observed divergent behavioral strategies undertaken by people of different racial groups to achieve the desired impression. Black people displayed more self-promotion behaviors (eg, show confidence, mention accomplishments) whereas White people displayed more ingratiation behaviors (eg, smiles, eye contact, flattery) in inter-racial interactions. Our own previous research on verbal clinical communication showed that Black patients with higher levels of previous experiences with discrimination were more verbally active while communicating with their non-Black physicians compared to Black patients with lower levels of previous discrimination. Perhaps the patterns observed here and in our previous research with Black patients are evidence of Black patients’ strategies to manage their desired impression in their interactions with non-Black physicians. 22
Clinical Implications and Potential Interventions
Investigations of clinical communication disparities and what leads to those disparities can inform the development of interventions to improve the quality of clinical communication and, in turn, treatment- and mortality-related outcomes for Black patients.51,61,62 Although our findings help to understand the link between patient and physician race-based attitudes and perceptions and their influence on clinical communication, further work is needed to clearly understand the clinical implications of patterns of nonverbal synchrony. Overall, the challenge is to mitigate the influence of negative attitudes and perceptions that patients and physician may not even be aware that they hold. Making patients and physician aware that their attitudes may influence communication and outcomes can only move the needle on disparity mitigation so far and, in some cases, may make things worse. 63 Rather, intervention efforts may need to focus on modifiable features that have been shown to reduce the influence of nonconscious attitudes and perceptions. Greenwald’s recent review of implicit bias-focused research provide evidence-based suggestions for change. These include interventions based around the contact hypothesis, which predicts that positive or favorable contact between members of different groups (including racial groups) will lead to improved relationships, including communication, and potentially lower implicit bias. 64 Importantly, the contact hypothesis interventions rely on the critical role of diversity in recruitment in all levels of a clinic and hospital hierarchy/organization.4,65
Greenwald’s review also offers support for interventions that link bias-recognition curricula to interventions that modify the clinical context in ways that prevent or reduce the negative influence of implicit biases and other race-based attitudes and perceptions on clinical communication and related outcomes. 64 This includes reducing distractions (eg, cell phones, pagers, interruptions, etc.) in the exam room, providing adequate time for patients to express themselves and physicians to follow-up on ambiguous or unanswered questions, and physicians giving themselves time to question any assumptions they may be making about patients and whether those are based on evidence. More generally, interventions that prompt high-quality clinical communication between patients and their physicians will likely help mitigate the negative influence of race-related attitudes and perceptions on clinical communication, perceptions, and potentially, patient outcomes.51,66-68
Our current findings add to a growing body of work demonstrating the need for more nuanced investigations of nonverbal synchrony and interaction outcomes in various contexts while also considering individual and relationship variables. In response to this need, Gordon and colleagues (2024) recently presented a Theory of Flexible Multimodal Synchrony. 69 This theory accounts for the dynamical nature of nonverbal synchrony over time, offers an alternative to the assumption that nonverbal synchrony is inherently a positive state, and integrates context and individual and relationship-level variables as critical factors in predicting nonverbal synchrony. 69
Limitations
Findings from this study must be considered within its limitations. First, we analyzed initial visits of patients and their medical oncologists, suggesting that patients and physicians were only beginning to build a relationship. Although this provides a unique context for nonverbal synchrony in naturally occurring interactions, it is possible that patterns of nonverbal synchrony change over time as the clinical relationship develops. Future research should examine this and related questions including nonverbal synchrony’s influence on patient outcomes.36,45 This does not, however, diminish the importance of examining nonverbal synchrony in the early stages of potentially difficult clinical interactions, as they may well set the tone for subsequent interactions. Second, because this was a secondary analysis, we had little control over the selection of participants; this study’s participants were all Black women and their non-Black physicians, and there was an imbalance in the number of patients each physician saw. These characteristics suggest that we have a unique and rich data set, but also limit the generalizability of the study’s findings. Third, similarly, the primary study did not collect data related to the physicians’ background characteristics. Fourth, the primary study was conducted more than 10 years ago, and therefore do not consider recent social changes or changes related to medical training or context. However, this study does provide an important proof of concept test, allowing future investigators to utilize this method with newer data. Last, our study did not focus on the outcomes of interactions such as treatment decisions or treatment adherence. However, our findings offer a foundation of knowledge on which to build a greater understanding of the dynamic, jointly-determined behavioral channels through which race-related attitudes and perceptions may be expressed.
Conclusion
Findings confirm and extend research demonstrating that Black patient and non-Black physician race-related attitudes and perceptions influence their clinical communication. This has important implications as we continue to work to mitigate clinical communication disparities and move toward health equity in cancer care. We emphasize especially the role physicians and their attitudes play with regard to nonverbal synchrony and how these may help or hinder their relationship with their Black patients and the immediate and longer-term outcomes of their clinical interactions. While we work toward interventions that address verbal and nonverbal communication, this new evidence provides suggestions for theory-based interventions (eg, interventions designed around contact hypothesis).
Supplemental Material
Supplemental Material - The Influence of Patient and Physician Race-Related Attitudes and Perceptions on Nonverbal Synchrony in Oncology Treatment Interactions Between Black Patients and Non-Black Physicians
Supplemental Material for The Influence of Patient and Physician Race-Related Attitudes and Perceptions on Nonverbal Synchrony in Oncology Treatment Interactions Between Black Patients and Non-Black Physicians by Lauren M. Hamel, Robert Moulder, Felicity W. K. Harper, Milisa Manojlovich, Fabian T. Ramseyer, Louis A. Penner, Terrance L. Albrecht, Steven Boker, Diliara Bagautdinova, and Susan Eggly in Cancer Control.
Footnotes
Ethical Consideration
The Institutional Review Board (IRB) at Wayne State University approved our secondary analysis (approval: 044716B3E) on June 17, 2016.
Informed Consent
Respondents gave written consent for review and signature before starting questionnaires and being video recorded. They provided permission for their data to be used in secondary analyses.
Author Contributions
Lauren M. Hamel: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft. Robert Moulder: Formal analysis, Writing – review & editing. Felicity K.W. Harper: Writing – review & editing. Milisa Manojlovich: Writing – review & editing. Fabian T. Ramseyer: Writing – review & editing. Louis A. Penner: Writing – review & editing. Terrance L. Albrecht: Writing – review & editing. Steven Boker: Writing – review & editing. Diliara Bagautdinova: Writing – review & editing. Susan Eggly: Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Institute of Minority Health and Health Disparities grant R21MD011766-01 (LMH) and National Cancer Institute grant U54CA153606 (TLA).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.