
Abstract
Background
Colorectal cancer screening reduces colorectal cancer morbidity and mortality. Identifying the factors associated with screening participation is needed to overcome barriers to screening. While several of those factors have been identified, the impact of mental and physical health on screening behaviour is not well understood.
Methods
This retrospective cohort study compared the self-reported mental and physical health of those who did screen for colorectal cancer and those who did not. Participants of the Australasian Colorectal Cancer Family Registry Cohort that were aged 45-75 years and had never been diagnosed with colorectal cancer were asked to complete a questionnaire detailing their colorectal cancer screening participation in the preceding 5 years, and a validated questionnaire of mental and physical health. Multivariable logistic regression was used to adjust for measured potential confounders.
Results
Of the 1130 eligible participants, 781 had a family history of colorectal cancer (69.5%), and 819 reported colorectal cancer screening in the past 5 years (72%). After adjusting for potential confounders, there was no evidence that overall mental or physical health was associated with colorectal cancer screening. However, those reporting higher levels of general health were more likely to participate in colorectal cancer screening (OR = 1.02 (100 point scale), 95% CI 1.004, 1.037, P = .014).
Conclusion
We found limited evidence that mental and physical health were associated with colorectal cancer screening. The high proportion of participants with a family history of colorectal cancer limits the generaliseability of the findings to the general population, although we observed no differences in findings by strength of family history.
Keywords
Introduction
Colorectal cancer was the fourth most diagnosed cancer and the second most common cause of cancer-related deaths in Australia in 2021 1 with 15,540 diagnoses and 5295 deaths. Screening for colorectal cancer can prevent the disease, and detect it at an early stage, resulting in reduced morbidity and mortality from the disease. National screening guidelines recommend fecal immunochemical test (FIT) screening for those with no family history of colorectal cancer, FIT every 2 years (from age 40 to age 49) and colonoscopy every 5 years (from age 50 to age 74) for those with moderate family history, and five-yearly colonoscopy for those with a strong family history since 2006. 2 The Australian government funds the National Bowel Cancer Screening Program (NBCSP), which provides biennial FIT for all Australians from age 50-74 years. Participation in the NBCSP is currently at 40% 3 with additional opportunistic screening (of unknown prevalence) provided via general practice, referral to gastroenterology, or private purchase of FIT kits from pharmacies. 4 People with a family history of the disease are also inadequately screening, with only 6% of Australians at moderate or high risk reporting a level of screening that meets or exceeds that recommended by the guidelines. 5
Identifying the reasons for not screening is essential to develop strategies to increase screening. Several factors have been identified as being associated with a lack of participation in the NBCSP. For example, men, those living in remote areas of Australia, those at the younger age of the eligibility range, and first-time invitees are less likely to screen. 6 Recent studies have found that the existing barriers to the FIT include: inconvenience of the testing process, aversion to collecting faeces, lack of knowledge of the benefit of screening, fear of a cancer diagnosis, and cultural beliefs and attitudes. 5
We hypothesise, that mental health and physical health might also be associated with CRC screening participation by impacting motivation to screen and capability to complete the screening tests. In the Australian context, we are not aware of any studies that have examined the relationship between physical health and CRC screening and only 2 studies of the relationship between mental health and CRC screening. Internationally, lower levels of CRC screening have been associated with antipsychotic, anxiolytic, antidepressant and hypnotic medication use 5 and severe mental illness but less so for common mental illness. 7 A limitation of these studies is they did not assess the potential role of the physical health of the same study participants, which can have an important interplay with mental health. For example, chronic disease has been associated with lower participation in colorectal cancer screening programs,5,7-9 and chronic disease can impact mental health.
Similar associations have been observed between mental health and screening for other breast cancer and cervical cancer.10,11 Women with mental health problems were less likely to attend national breast cancer or cervical cancer screening programs,10-12 possibly because of barriers due to a range of complex possible factors including low socioeconomic status, poor functioning or cognitive difficulties, stigma, and on-going psychological stress. 12 However, results are inconsistent with 1 study reporting no differences in mammography rates between women with or without any medically diagnosed mental illness in the United States. 11 A possible explanation for this is women with mental health problems tend to access primary health care more often and therefore have increased access to General Practitioner (GP) recommendations for cancer screening. 12
In summary, some severe levels of mental are negatively associated with colorectal cancer screening (see above). However, there is a dearth of published research on assessing the role of both physical and mental health in the same subjects on colorectal cancer screening, particularly in Australia. The aims of this study are to measure the association between mental and physical health and screening for colorectal cancer in a large population-based sample.
Methods
Data Source
The data for this analysis were sourced from the Australasian Colon Cancer Family Registry Cohort, a family cohort resource for research on colorectal cancer prevention, aetiology and prognosis that forms part of the international Colon Cancer Family Registry Cohort (CCFRC). 13 Participants in the CCFRC included colorectal cancer cases recruited from population-based cancer registries and family cancer clinics in Australia, New Zealand, the USA and Canada and their relatives and spouses. 13 At recruitment, all participants gave written consent to complete a baseline questionnaire on their risk factors for colorectal cancer and their relatives’ cancer history. 5 years after recruitment, attempts were made to follow up with all participants (including those with and without colorectal cancer) by questionnaire to update their risk factor data and family history of cancer. Follow-up was repeated every 5 years. Questionnaires were administered through face-to-face interview, telephone interview, or by mail. The baseline questionnaire included demography questions such as age, sex, family history of cancer, cancer history, marital status, level of education, diet and medication use, alcohol and smoking, weight and height and cancer screening history. The follow-up questionnaires included the age of the completed follow-up survey, first and last colorectal cancer detection tests in the previous 5 years (fecal occult blood test (FOBT), sigmoidoscopy, colonoscopy), the reason for the test, and the short form 12 health survey items (see Supplement for the questionnaires).
For this study we included all the relatives and spouses recruited between 1998 and 2008 in Australia who completed a baseline questionnaire at recruitment and a follow-up questionnaire 5 years later between 2003-2013. We excluded any participant with a previous diagnosis of colorectal cancer.
Definition of Screening
Given the recruitment strategy, a high proportion of participants had a family history of colorectal cancer. Therefore, we included all screening modalities in our definition of screening. Colorectal cancer screening was defined as at least 1 FIT, sigmoidoscopy or colonoscopy in the past 5 years reported by the participant in the first follow-up questionnaire (ie, tests undergone between the time of completing the baseline questionnaire and the first follow-up questionnaire) with the reported reason for the most recent test as “routine/yearly exam or check-up” or “family history.”
Definition of Physical and Mental Health
The 8 Domains of Mental and Physical Health Based and the Items of the SF-12 on Which They are Based.

Scores for overall mental and physical health care are based on weighted combinations of the answers to all 12 questions. Scores are calibrated so that a higher score indicates a better health state. 14 Item responses from the SF-12 questions are converted into summary scores by aggregating the standardized scales for each of the 8 domains (weighted by Australian general population means and standard deviations), and then transforming these summary scores into t-scores (See Supplement for detailed statistical method). Each score has a possible range from 0 to 100 and is calibrated so each score indicates a level of health equivalent to the average Australian, and a score above or below 50 indicates better or poorer health, respectively.
Analysis
The data were analysed as a retrospective cohort study, measuring the relationship between self-reported mental and physical health and self-reported screening for colorectal cancer. Inclusion criteria for participants were as follows: participated in the first follow-up of the Australian Colorectal Cancer Family Study; nationality is Australian; living in Australia at the time of the first follow-up; aged between 45-75 at the time of the first follow-up; and have completed the SF-12 questionnaire items in the first follow-up. Exclusion criteria were diagnosis of colorectal cancer at any time up to and including the date of the first follow-up questionnaire.
The main analysis was a logistic regression to estimate the odds ratio of screening for overall mental and physical health. Secondary analyses were conducted for each of the 8 domains. Adjustment was made for these potential confounders: family history of cancer, age at completion of first follow-up, gender, education level, marital status and any previous cancer diagnosis (apart from colorectal cancer). Non-independence of any participants who were relatives was taken into account using the VCE(cluster) option by family ID in Stata. This specifies that the standard errors allow for intragroup correlation. Mental and physical health were fitted as a continuous measure and as quintiles. The analysis of physical and mental health as quintiles was conducted by a visual examination of the quintile coefficients for patterns or trends by quintile. We also measured the association between physical and mental health and colorectal cancer stratified by family history of colorectal cancer (no first-degree relatives with colorectal cancer, one first-degree relative with colorectal cancer, and two or more first-degree relatives with colorectal cancer). To account for potential intragroup correlation within the data, we used cluster-robust standard errors in our logistic regression analysis, clustering at the level of the family identifier.
Given the recruitment criteria for any participants was having a relative with colorectal cancer, we conducted a sub-analysis by assessing the strength of the association between mental or physical health and colorectal cancer screening stratified by the number of first-degree relatives with colorectal cancer.
A binominal test for differences in proportions and Students t-test were used to compare means. All statistical analyses were performed using Stata statistical software version 16 (Stata Corporation, College Station, Texas 2019). 17
Ethical Approval
This research was approved by the Health Research Ethics Committee of the University of Melbourne, Victoria, Australia (approval number: 13094; approval date: 25/9/2019). An amendment was also approved by the Office of Research Ethics and Integrity Committee of the University of Melbourne, Victoria, Australia on 11/2/2020 (reference number: 2021-13094-17415-4).
Results
The First Follow-Up Participant Characteristics. a
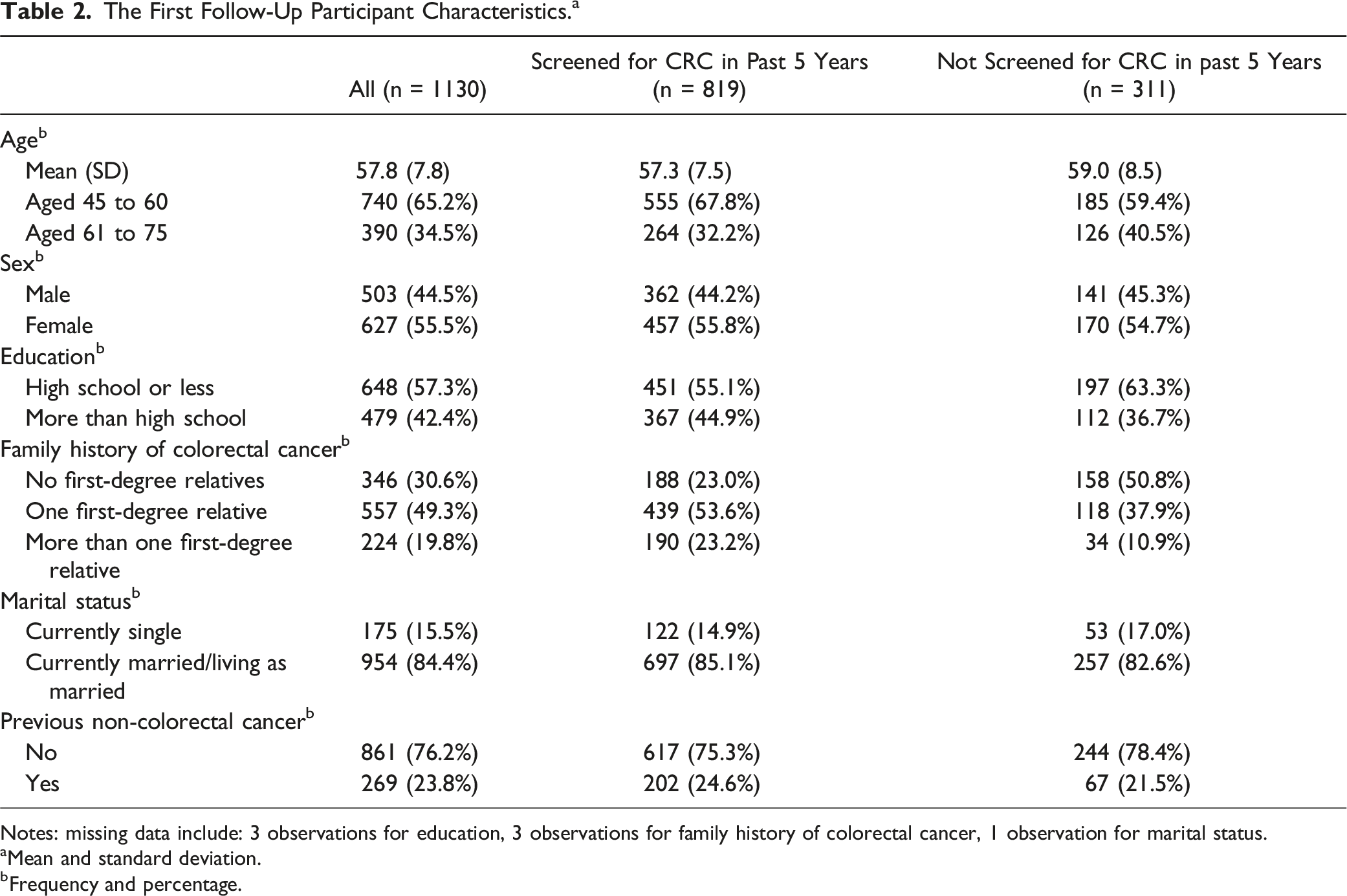
Notes: missing data include: 3 observations for education, 3 observations for family history of colorectal cancer, 1 observation for marital status.
aMean and standard deviation.
bFrequency and percentage.
Participants’ Scores for 8 Domains of Mental and Physical Health in the SF-12 Score.

Notes. PF: physical functioning; RP: role-physical; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: Role-emotional; MH: mental health; PHYS: total physical health score; MENT: total mental health score.
Median and Interquartile Range of the Mental and Physical Health Scores of Participants by Colorectal Cancer Screening Status.

aMedian and interquartile range (IQR).
Odds Ratios, 95% Confidence Intervals and P-Values for Association Between Mental and Physical Health (Fitted as a Continuous Measure and as Quintiles) and Colorectal Cancer Screening, Adjusted for Age, Sex, Education, Family History of Colorectal Cancer, Marital Status, and Previous Non-Colorectal Cancer.

Odds Ratios, 95% Confidence Intervals and P-Values for Association Between Mental and Physical Health (Fitted as a Continuous Measure and as Quintiles) and Colorectal Cancer Screening, Adjusted for Age, Sex, Education, Marital Status, and Previous Non-Colorectal Cancer. Participants With No First-Degree Relatives With Colorectal Cancer.

Odds Ratios, 95% Confidence Intervals and P-Values for Association Between Mental and Physical Health (Fitted as a Continuous Measure and as Quintiles) and Colorectal Cancer Screening, Adjusted for Age, Sex, Education, Family History of Colorectal Cancer, Marital Status, and Previous Non-Colorectal Cancer. Participants With One First-Degree Relative With Colorectal Cancer.

Odds Ratios, 95% Confidence Intervals and P-Values for Association Between Mental and Physical Health (Fitted as a Continuous Measure and as Quintiles) and Colorectal Cancer Screening, Adjusted for Age, Sex, Education, Family History of Colorectal Cancer, Marital Status, and Previous Non-Colorectal Cancer. Participants With Two or More First-Degree Relatives With Colorectal Cancer.

Odds Ratios (100 Pint Scale), and 95% Confidence Intervals and P-Values for Association Between Each of the Scales of Physical and Mental Health Adjusted for Age, Sex, Education, Previous Cancer Diagnosis Other Than Colorectal Cancer, Family History of Colorectal Cancer, Marital Status.

Discussion
We investigated whether there was any association between mental and physical health and colorectal cancer screening by analysing questionnaire data from 1130 Australians aged between 45 and 75. We found no overall evidence of an association between mental or physical health and colorectal cancer screening either before or after controlling for age, sex, education, other cancer, family history, and marital status.
This null finding is in contrast with previous Australian studies. One study reported a complex non-linear relationship between CRC screening and psychological distress, with people at the low end and high end having lower levels of participation, but those with moderate levels having a higher level of participation. 5 The other Australian study reporting severe mental illness had lower levels of screening. 18 Our findings add to the mixed findings of previous large international studies that found people with anxiety or depression were either: less likely to screen for colorectal cancer (UK study of men and women finding long-term depression associated with not screening for colorectal cancer before adjusting for other factors, but null association after adjustment) 19 ; equally likely to screen (US study of post-menopausal women finding no association of depressive signs at baseline associated with colorectal cancer screening) 20 ; or more likely to screen (European study finding greater use of colorectal screening in depressed people). 21 This inconsistency may be due to the heterogeneous measures of mental health across studies, different definitions of CRC screening participation, and differences in any barriers or enablers for screening participation that exists between countries.
We did observe that general health (1 of the 8 domains of mental and physical health that we assessed) was positively associated with colorectal cancer screening, ie, greater general health appeared to increase screening likelihood. This association can also be interpreted as people with poor general health are less likely to screen. One possible explanation for this association is that people with poor perceived health may be less interested in focusing on other potential health problems. Poor general health may be a legitimate reason not to screen as there may be a natural life limitation in these people, which would mitigate any benefits of screening. Some studies have shown that people with existing chronic diseases may have functional limitations that may impact their capacity to participate in cancer screening. In addition, people with chronic disease are over-represented in lower socioeconomic status groups, and this has been linked to lower screening participation. 11 GPs may discourage participation if general health concerns (and co-morbidities) make colonoscopy inadvisable. People with poorer general health may have doubts about health insurance rebates for the test fee. In this case, GPs could recommend people with poor general health to participate in NBCSP using non-invasive testing (eg, FIT). In sum, this finding does suggest a potential strategy to increase participation is to provide additional support to some people with poor general health to help them screen.
Strengths
The study has a large sample size and therefore, is able to provide more precise estimates of association than previous studies. We have used the SF-12 for the questionnaire items on mental and physical health, which is a standardized, validated and widely used health survey that can be coded for multiple measures of participants’ mental and physical health. The SF-12 can examine both mental health and physical health and is an accurate reproduction of average scores for the longer SF-36 questionnaire, and therefore completed more quickly and easily by participants. 14 SF-12 has a 90% validated rate in the US population and is also valid and reliable for the Australian population.8,15 There was a high level of questionnaire completion by participants (approximately 90% of items were complete), which gives confidence that the estimates of association are unlikely to be biased because of non-completion. We were also able to adjust for factors associated with mental and physical health and cancer screening to reduce the risk of confounding. Previous studies were more focused on the specific, rather than general, mental or physical illness impact on cancer screening. In contrast, our study filled a knowledge gap by examining the impact of both mental and physical health on colorectal cancer screening participation among the general population unselected for health conditions.
Limitations
This analysis was performed on data that focused on the screening period in the 5 years between baseline and follow-up. As screening outside this period, eg, after completing the follow-up was not considered, some infrequent screeners would have been defined as non-screeners. If delay in screening was associated with mental or physical health, this could bias the associations. Non-completion of the questionnaires, either due to death or ill health, might limit the generalisability of the findings to relatively healthy people. Even though the data for this analysis came from a cohort study, we were not able to determine the temporal relationship between mental and physical health and screening, so could not be certain that the mental and physical health status predated their screening behaviour. This study used SF-12, which is based on the participants’ self-report. Therefore, participants may over-report or exaggerate their health issues, increasing the risk of false positive findings. Participation in colorectal cancer screening in this study was relatively high compared with the general population participation in the National Bowel Cancer Screening Program. This is likely due to the high prevalence of family history becasue of the recruitment strategy to enrol relatives of colorectal cancer cases. Thus, participants had an overall higher level of colorectal cancer risk and therefore, were more motivated to screen. However, we showed that the associations we observed were consistent at varying levels of family history. Finally, we were unable to accurately determine, based on the questions asked of the participants in the follow-up survey, whether or not they were up to date with their screening according to the national guidelines, and therefore we could not assess whether physical and mental health were associated with recommended screening. Future studies should attempt to overcome these limitations by recruiting Australians across a wider risk spectrum, by seeking dates of all screening procedures, and by using an extended range of mental and physical health beyond the SF-12.
Conclusion
While other studies have observed that specific mental health conditions could impact colorectal cancer screening participation; this study found no evidence that general measures of perceived mental and physical health influenced colorectal cancer screening participation in Australia. We did find some evidence that a specific sub-category of health, general health, may be associated with screening participation. This provides some support for a possible avenue to increase screening participation by focusing encouragement or support on those with low levels of general health.
Supplemental Material
Supplemental Material - The Association Between Screening for Colorectal Cancer and Mental and Physical Health
Supplemental Material for The Association Between Screening for Colorectal Cancer and Mental and Physical Health by Yiting Gong, Louisa B. Flander, Finlay Macrae, Carlene Wilson and Mark A. Jenkins in Journal of Cancer Control.
Footnotes
Acknowledgments
The content of this manuscript is solely the responsibility of the authors and does not necessarily reflect the views or policies of the NIH or any of the collaborating centers in the CCFR, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government, any cancer registry, or the CCFR. The authors gratefully acknowledge the contribution of Caroline Gao for their assistance preparing the paper.
Author Contributions
YTG: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data Curation, Writing - Original Draft, Writing - Review & Editing, Software. MJ: Supervision, Conceptualization, Methodology, Validation, Formal analysis, Writing - Review & Editing. CW&LF&FM: Supervision, Conceptualization, Writing-Review, Validation, & Editing.
Declaration of Conflicting Interests
The authors have no conflict of interest to declare with respect to this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Australiasian Colorectal Cancer Family Registry is supported by funding from the National Cancer Institute (NCI), National Institutes of Health (NIH) (award U01 CA167551). This research was funded in whole or part by the National Health and Medical Research Council [1195099]. For the purposes of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Ethical Statement
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.