
Abstract
Background
Women with breast cancer usually face multiple short-term and long-term problems in dealing with their acute and chronic symptoms during and after cancer treatment. However, serious gaps remain in addressing these issues in clinical and public health practice.
Methods
According to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, we conducted a systematic literature search from 2000-2021 in electronic databases, including Medline, PubMed, Embase, Scopus, Web of Knowledge, and Google Scholar databases using predefined keywords.
Results
The review identified several significant and interconnected problems in breast cancer patient’s treatment and supportive care. The results revealed that these issues are very common among breast cancer patients, and specific attention and serious measures are needed to address these problems. Despite implementing different protocols and programs for covering and addressing these problems, serious gaps still exist in supporting breast cancer patients during clinical and follow-up care.
Conclusion
Developing innovative and holistic approaches and programs based on the multifactorial assessment of symptoms are suggested for addressing and covering the multidimensional requirements of this population. Consequently, thorough evaluation, education, treatment, and referrals should be provided for the most common sequelae of these patients by including appropriate medication, exercise, counselling, occupational therapy, and complementary therapies. The present study provides a more comprehensive source of information about breast cancer patient’s medical and supportive needs in comparison with individual studies on symptom experiences.
Introduction
As the second most common cancer among the women population, breast cancer (BC) imposes a significant health and economic burden on this population and the countries they live in. According to the World Health Organization (WHO), BC annually impacts 2.3 million women and results in the highest number of cancer-related deaths in women. WHO reported that 685 000 women died from BC in 2020, about 15% of cancer deaths among women. 1 On the other hand, the World Cancer Research Fund (WCRF) reported over 2.26 million new cases worldwide, contributing 15.5% of the new cases diagnosed in 2020. 2 It is estimated that about 268600 and 2670 new cases of invasive BC will be diagnosed in 2022 among women and men, respectively. In addition, about 41760 women and 500 men are expected to die from BC in 2022.3,4 Unless this trend is slowed, it is estimated that BC incidence and its burden will continue to rise steadily in developed and especially in less developed countries, requiring special efforts in providing proper treatment and follow-up healthcare services. 5
Despite some remarkable achievements in improving BC treatment and follow-up support, the available evidence from various research revealed significant barriers to these patient’s clinical and post-clinical care. 6 Inadequate attention to BC patient’s supportive care and survivorship issues, such as physical, biological, psychosocial, and long-term health problems, has been repeatedly reported in previous studies. These problems ultimately make it difficult for women who are fortunate enough to remain disease-free to rebuild their physical, social, professional, and personal well-being. 7 The reasons for these inadequacies in addressing the particular issues of this population are multifold. In short, financial and budgetary constraints, inadequate and inappropriate medical infrastructures, lack of standard protocol and guidelines, lack of well-trained healthcare providers, patient’s personal characteristics, and other social barriers, among others, are reported as the most frequent and challenging obstacles in addressing the particular issues of this population.8,9
The current BC early detection strategies mainly rely on BC education and awareness (patient, community, and health professional education), breast health awareness, breast self-detection, and clinical breast exams (CBE).10,11 Treatment of BC often involves a combination of surgical resection, radiotherapy, and medications (hormonal therapy, chemotherapy, and/or targeted biological therapy) to treat the microscopic cancerous cells that have spread from the breast tumor through the blood.12-15 The timely diagnosis and well-developed treatment protocols and procedures are highly crucial for achieving the desired clinical outcome in BC treatment. However, women in various countries face different impediments to early diagnosis, such as socioeconomic, personal, and other interrelated barriers that could restrict their timely access to efficacious breast healthcare services. For example, a careful analysis of the current situation based on development indicators in the diagnosis and treatment of BC revealed significant disparities among many settings and a perverse relationship worth emphasizing.
16
In fact, the budgetary constraints in Low-to-Middle-Income Countries (LMICs) resulted in fragile and ill-prepared healthcare systems with significant differences in resource provision, appropriate infrastructure, and organization. This has led to limited access to general and particular healthcare services in these settings. Therefore, a significant proportion of BC women are diagnosed with later-stage disease, leading to worse clinical outcomes.
16
In this regard, LMICs are usually associated with lower (but increasing) BC prevalence and elevated mortality rates than High-Income Countries (HICs) (Figure 1). On the other hand, the lack of suitable and appropriate follow-up or palliative care in these countries resulted in impaired physical, psychological, and social aspects of BC patients. (A) Incidence and (B) mortality rates of BC per 100000 women in HICs and LMICs, respectively, obtained by country-summary from the literature (Data were collected in 2022).
Although enormous studies have addressed the various clinical and post-clinical problems of BC patients, only a few have been focused on comprehensively addressing the general and interconnected issues of this population. On the other hand, most of these studies have only focused on one aspect of this population’s health concerns (physical, mental, etc.) at a time, and studies on the comprehensive assessment of their short-term and long-term problems are usually scarce. Likewise, little is known about the coping strategies employed by women to manage the difficulties arising from their experiences after receiving a BC diagnosis. Therefore, following our previous study, 17 we aim to highlight and address the various problems of BC patients, especially Young Women with Breast Cancer (YWBC), and explore existing and possible strategies to overcome barriers and provide comprehensive and appropriate care and support to this unique population.
Methods
The present systematic study was designed, conducted, and reported in adherence to the PRISMA guidelines to evaluate and investigate the main short- and long-term problems affecting the QOL of patients with active BC and cancer-free women (after treatment) and present contingency options proposed to relieve these problems.
18
The main objective of the present study was to provide adequate answers to the following questions: (1) What are the main short- and long-term problems that affect the QOL of BC patients?” (2) What are the possible strategies implemented worldwide to overcome these problems and enhance patient’s QOL?
Information Sources
A preliminary search showed that a lot of journals contain published articles evaluating BC patients and survivor’s various and different problems. Therefore, a comprehensive search was undertaken in multiple electronic databases, including Medline, PubMed, Embase, Scopus, Web of Knowledge, and Google Scholar databases.
Search Strategy
Following the PRISMA guidelines, 18 a systematic literature search was conducted from 2000 to 2021 using the following predefined keywords or their combinations: breast cancer, women with breast cancer, young women with breast cancer, breast cancer problems, breast cancer short-term and long-term problems. The search was carried out to identify studies reporting BC patient’s different problems in dealing with diseases and specify current solutions for addressing these issues.
Eligibility Criteria
The review included all studies published in peer-reviewed journals; written in English; focused on BC patient’s various problems, including general, physical, psychological, social, and spiritual issues; and focused on treatment and coping methods for those problems were included in the present study. For establishing comprehensive inclusion criteria, the websites on BC issues and support programs have also been reviewed and included. The exclusion criteria of the present study were as follows: non-peer-reviewed journal articles, Books, book abstracts, or dissertations; studies reporting on views of nurses, caregivers, doctors, and complementary and alternative medicine practitioners; and theoretical articles. Overall, about 1247 papers were found useful to incorporate into the research. After carefully reviewing the abstracts of the selected studies, ultimately, 190 studies meet the eligibility requirements and the scope of the review (Figure 2). Flow diagram for identification and selection of studies based on PRISMA guidelines.
Study Selection
The eligibility of the studies was assessed independently by 3 authors by reviewing their titles and abstracts. The non-relevant or redundant studies that did not meet the inclusion criteria were eliminated through this approach. When there was disagreement, a discussion would fix the issue. Other authors reviewed the entire texts following the first screening.
Data Collection and Extraction
The information of the selected studies was carefully extracted by 4 authors. When there was disagreement, the problem was fixed by discussion between them.
Risk of Bias Assessment
The Cochrane Collaboration and ROBINS-I tools were used to assess the risk of bias in the randomized and non-randomized clinical trials used in the study, respectively.19,20 In this context, the Cochrane Collaboration’s tool was assessed according to the following criteria: Creating a random sequence, hiding allocations, blinding participants and researchers, blinding outcome evaluation, incomplete outcome data, selective reporting, and other biases. The risk of bias in the research was classified by the review authors as low, unclear, or high. Bias resulting from confounding, bias in participant selection for the study, bias in intervention classification, bias resulting from deviations from intended interventions, bias resulting from missing data, bias in outcome measurement, bias resulting from choosing the reported result, and overall bias are assessed for ROBINS-I bias assessment tool.
Results and Discussion
Study Selection and Methodological Quality Evaluation
We identified 1247 eligible papers, of which 190 studies were found suitable for full-text assessment (Figure 2). Of these, five studies were randomized clinical trials and 15 articles were non-randomized studies of interventions. These studies were generally conducted to identify and evaluate BC patients’ various problems during or after the treatment course, as well as their various coping strategies. The remaining articles were review articles or other surveys mainly focused on developing or establishing coping strategies for multiple issues of BC patients. Figure 3 classifies the included articles according to their types and nature. Classification of the included articles according to their types and nature.
The Risk of Bias Assessment Results of Randomized Clinical Trials Using the Cochrane Collaboration Tool.
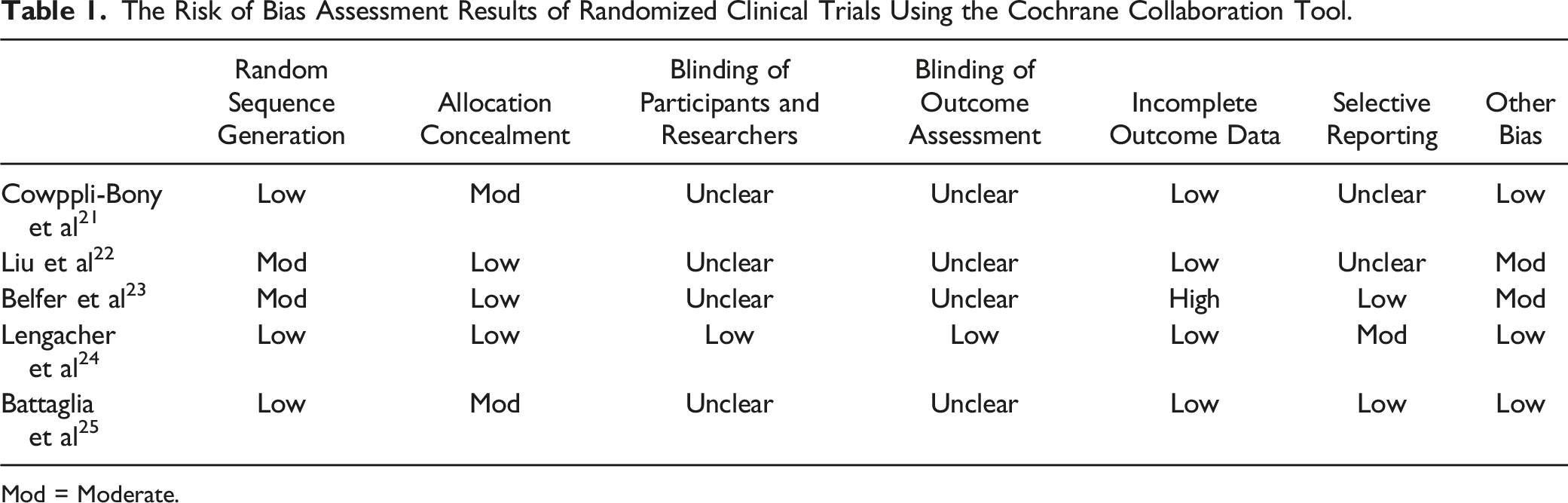
Mod = Moderate.
The Risk of Bias Assessment Results of Non-randomized Studies of Interventions Using the ROBINS-I Tool.
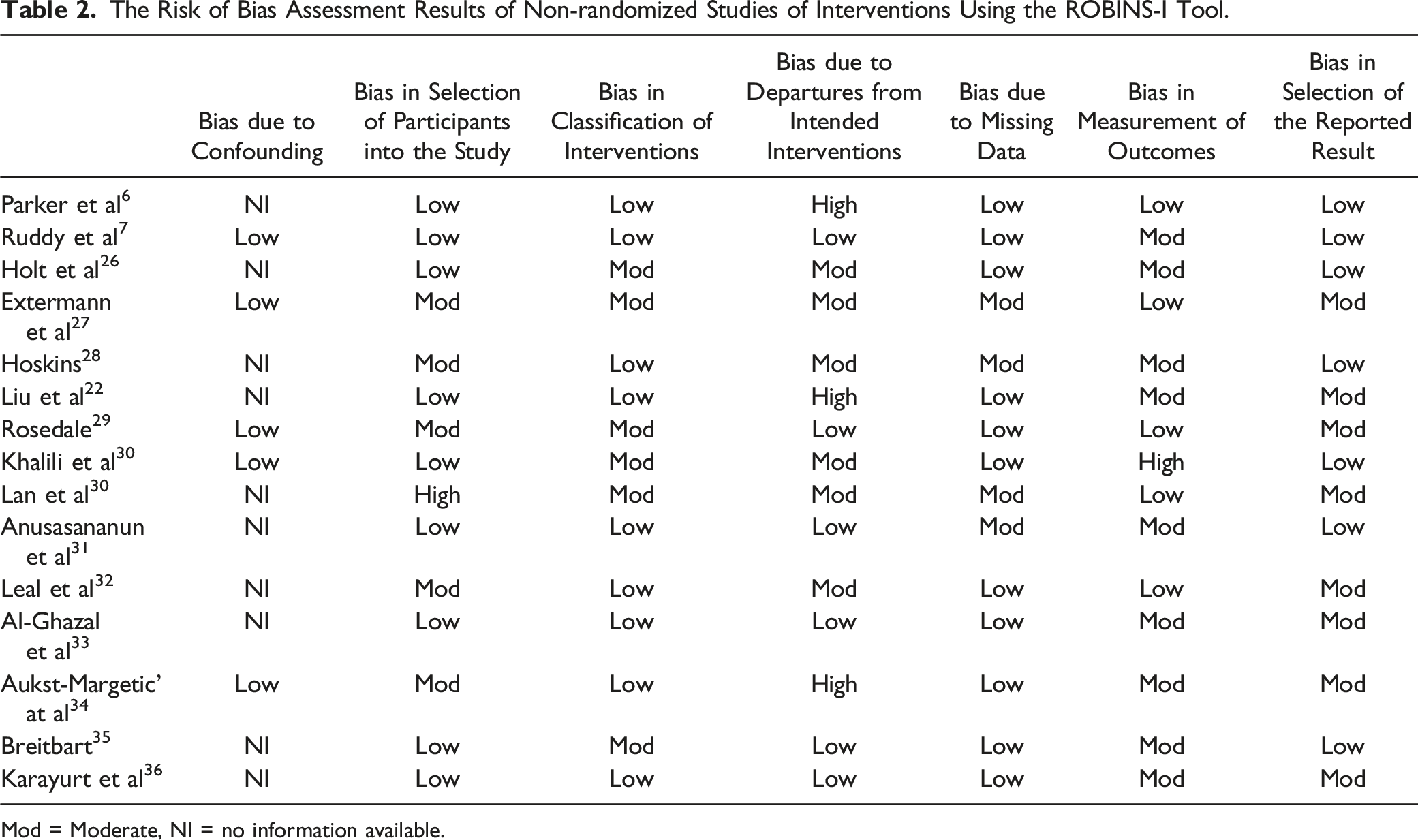
Mod = Moderate, NI = no information available.
Study Outcomes
Various BC-related challenges in the short term, including general, physical, psychological, spiritual, educational, social, and long-term problems, have been identified for BC patients in the clinical and post-clinical sectors (Figure 4). These problems are summarized and discussed separately in more detail below. Various BC-related problems were identified for BC and YWBC patients. The common BC-related issues include short-term problems (Psychological, general, educational, social, spiritual, physical, and functional problems) and long-term problems, which may consist any of the highlighted short-term problems that persist and linger in the long term.
Short-Term Problems
Epidemiological Data Scarcity
As a first impediment, the comprehensive data on the prevalence and mortality of BC, especially from LMICs, are sparse or underreported, which somewhat hampers the data interpretation. This problem also applies to other epidemiological aspects of BC patients, including risk factors, early detection methods, and treatment.4,37 Therefore, evaluating the current situation and patient’s serious challenges relies mainly on available data that might not represent worldwide.38,39 On the other hand, the information on various issues relating to BC patient’s care and support varies widely based on different country’s geographical, ethnic, and socio-economical diversities. 40 The only valid data about the majority of this population are available from the population-based cancer registries. However, because these registries mainly rely on data provided by pathology laboratories for case ascertainment, it is believed that their statistics may underestimate the true impact of diseases. Another major obstacle in collecting information from different registries is the lack of universal methods for collecting and storing the information. Consistently, this leads to significant disparities in the interpretation of worldwide-published data on the treatment and support of BC patients, and any attempts in this area are often viewed with suspicion.41-43 Significant difficulties were also found in collecting precise incidence rates in poor nations, according to a study by Fregene et al. Not many have cancer registries that can give incidence rates at intervals of 15 years or more. Many of the most established registers have limited population coverage. The calculation of incidence and death rates is further complicated by challenges in estimating population denominators. 44 The scarcity of comprehensive and accurate data about different BC epidemiological aspects may hamper effective decision-making policies to prevent, detect, and control BC on a large scale.
As a result, data from the SEER program on the BC burden have presented contradictory incidence and mortality rates in countries with different levels of resources (Figure 1). The world's most developed regions have the highest incidence rates in this instance, with 74.1 new cases per 100000 women, compared to 31.3 new cases per 100000 in less developed regions. However, in 2012, the developing nations with the greatest incidence rates of BC (above 80 per 100000 women) and the highest fatality rates (above 20 per 100000 women) also happened to have higher mortality rates. In other words, the reported incidence rate of BC in well-developed countries and urban areas is higher than in less-developed countries and rural regions, respectively.45-47 This is mainly related to the notably better screening and treatment infrastructures in high-income countries. 48 However, based on the abovementioned problems, these results seem also to be related to the lack of accurate epidemiological data and statistics, population-based cancer registries, different proportions of the women in a specific population or even different age distribution, and finally, lack of adequate screening programs of BC in these countries, rather than biological differences.5,49,50 This may explain the higher cancer-related mortality in low-income countries, among other shortcomings.48,51,52 Nevertheless, other reasons have also been suggested for the lower incidence of BC in some regions, including different dietary habits, socioeconomic status, parity, competing illnesses, and ethnic ancestry. On the other hand, lower survival rates in LMICs are mainly attributed to late-stage detection by screening, delayed and ineffective treatment, restricted resources for diagnosis and treatment, etc.53,54
Infrastructure and Financial Problems
While there has been much discussion about the benefits of early diagnosis in terms of results, little is known about the structural and financial ramifications. In many countries, public hospitals besides dealing with advanced diseases and lower chances of survival, also face limited budgets and high treatment costs.55,56 Financial and cost-related problems are major catastrophic medical constraints for both healthcare initiatives and BC patients in providing and seeking adequate treatment and supportive care. Budgetary constraints and lack of governmental or non-governmental support have limited the options available in this area, leading to a significant deterrent for screening, diagnosis, proper treatment, and timely advice and treatment.57,58 A survey by Bellanger et al. revealed that despite the higher incidence of BC in Upper-Middle-Income Countries (UMIC), women in the poorest nations carry a comparatively more significant burden of BC mortality, especially women under the age of 5046. Consequently, most studies in this field have focused on assessing the cancer situations in LMICs.
Financial resource deficiency also meant that there were insufficient resources for skilled workers, large-population healthcare facilities, appropriate BC diagnostic tools, screening programs, etc. Therefore, only a few centers are well equipped to provide multimodality protocol-based treatment with all its components, and even these centers sometimes are out of reach for most patients.38,51,59 Financial problems also dictate the existence of new and advanced treatment protocols (such as second-line and third-line therapies) and drugs in a healthcare institution.60-62 In countries with major rural hinterlands and remote areas, substantial expenditures on transportation and professional fees also are challenging. In such countries, substantial regional disparities accompany socioeconomic disparities leading to insufficient financial resources, inappropriate infrastructure, and limited healthcare staff.42,63
The availability and timely delivery of proper diagnosis and treatment methods for BC is highly dictated by the patient’s socioeconomic background and varies extensively depending on the patient's treatment facility. 64 In fact, most BC patients belong to a poorer socioeconomic background and cannot afford medical bills. These patients typically receive a late diagnosis and therapy that is ineffective, unsuitable, and delayed.64,65 For example, the findings of a nationwide multicenter study in China highlighted that more women belonging to higher socioeconomic groups presented with stage I and II disease than disadvantaged women, who presented with stage III or IV disease. 66 In most countries, a large number of patients have to pay for their systemic treatment and medicine costs without any governmental or insurance support. So, cheaper and unappropriated treatments are still preferred as the first line of treatment for the vast majority of poor and elderly patients. 67 A previous study revealed that patients treated in public facilities had progressive BC at diagnosis, and their overall survival was lower than women treated in private institutions. 68 The patient’s affordability also affects their compliance with treatment and follow-up care. For example, low acceptance of Breast-Conserving Surgery (BCS) and significantly poor compliance with treatment and follow-up among cancer patients outside major institutions were reported in previous studies.21,69 This can cause a higher rate of loco-regional recurrences and impoverish families and overall survival.
Age-specific Problems
Recently, age-specific problems have also emerged as new and significant healthcare challenges in the treatment and aftercare of BC patients. Almost 50% of cancers have been recorded in people 70 years of age and beyond. 70 Elderly patients have a number of issues that can make cancer treatment more complex, such as depression, comorbidity, functional reliance, poor access to care, and cognitive decline. 27 Despite the lack of any significant effect of patient age on cancer treatment, young patients usually face certain problems. Larger tumors, more metastatic lymph nodes, lower tumor grades, low rates of hormone receptor-positive status, earlier and more frequent loco-regional recurrences, and worse overall survival are generally linked to these patients’ biological features.71-73 Findings from previous studies revealed that despite the relatively uncommon prevalence and rarity of BC in young women, survival rates in this unique population are inferior than for their older counterparts, and it is the major reason of higher cancer-related deaths despite receipt of generally most effective and efficient treatments. The relative rarity and low priority of BC in young women, among the other public health problems, resulted in insufficient attention to the special requirements of this unique population in cancer-related training programs and consequently led to inappropriate addressing of those needs. Untimely diagnosis and insignificant clinical outcomes have been reported for women younger than 50 years due to a lack of effective prevention protocols and approaches, inadequate age-specific information, more flawed awareness about cancer screening, lack of early detection and timely treatment, and inadequate infrastructures.74-76 On the other hand, the benefits of some preventive and screening programs, such as mammography screening, population-based breast screening, diagnostic and opportunistic screening, and other preventive measures, felt that might not be cost-effective in these patients because of the lower incidence of BC in this population.77-79 This situation, in turn, results in delays in diagnosis and ultimately impact clinical outcomes.
Young patients usually lose a great number of life years as a result of their age-specific issues, late diagnosis, and a greater extent of systemic recurrence at different stages of BC treatment and follow-up care. On the other hand, younger women face unique age-related issues such as fertility, body image, appearance, and attractiveness compared to older women, which significantly affect their quality and longevity of life. In addition, these patients might be diagnosed at a point in their life where they play a variety of roles that may not easily be filled by others. Finally, compared to older women, YWBCs often feel lonely and unaware and they may be anxious about survival and other cancer-related issues. These diverse concerns may contribute to further and more emotional distress and psychosocial problems at both diagnoses and in follow-up. Therefore, YWBCs usually require special and complex supportive care than their older counterparts.73,80,81
Physical Problems
Diseases and Treatment-Related Side Effects of BC.

Psychological Problems
BC patients also face psychological and emotional problems during treatment and after the treatment course. A cancer diagnosis is accompanied with psychological effects, and at least one-third of cancer patients suffer from psychological issues.30,97 Psychological challenges and mood disorders of BC patients like fear, anxiety, depression, and disturbances in social roles are mostly affected by different factors such as personal, social, and illness-related factors and may continue into treatment and recovery phases and even into the possible reoccurrence phases.98,99 These factors generally include self-esteem, social stress, emotional problems, stage of illness, type of operation, disease symptoms, physical fitness, perceptions of illness, coping methods, and relationships with health staff.23,100 Many studies have reported that the experience of psychological problems is more likely among YWBCs than compared to their older counterparts.101-103 This unique population usually shows heightened vulnerability to the abovementioned challenges due to their younger age and age-specific problems. Financial loss, changes in body image, feelings of alienation from healthy peers, infertility, premature treatment-induced menopause, marital strain, fear of beginning a new relationship, childcare challenges, and finally, the ongoing threat of recurrence and death are among the most common concerns of YWBC. These concerns typically stem from a variety of sources.31,32,104 Even years after treatment is finished, YWBC are very concerned about the possibility of cancer returning and other long-term consequences. Fear of the future and shortened life are repeatedly reported in all phases of the BC experience.105,106 Based on Cordova et al., 107 this natural response is usually experienced by 64% of BC patients due to physical symptoms like pain, invasive treatments, possible reoccurrence of cancer, and the possibility of death. Another psychological manifestation of cancer and its therapies is anxiety in the patient, which is directly linked to fear and both actual and erroneous ideas and expectations. Distress and depression are other psychological symptoms reported in high numbers (33%) of BC patients. These psychological health challenges also influence the other aspects of BC patient’s treatment care and post-treatment support. Depression, in certain situations, might even result in suicide due to the patient’s perception of being a psychological burden to the family. Psychological issues and the way the patients choose to adjust to their situations verify the value of QOL in these patients.108,109
Recently, new and advanced treatment options such as breast, fertility, and sexuality-conserving treatments, targeted therapy, and other less-aggressive treatments have been introduced to BC therapy to overcome treatment-related physical and psychological problems. However, these options are only offered to a minuscule proportion of BC patients because of the patient’s financial constraints or lack of adequate infrastructure. In fact, adjuvant therapy during the patient’s reproductive years, information about the ability to become pregnant, and the effect of BC on pregnancy loss have been limited.33,110 On the other hand, poor satisfaction among patients, especially younger ones with conservative and non-aggressive treatments (such as mastectomy vs BCS) issues has been reported repeatedly in previous studies.111-114
Spirituality Problems
Spirituality is the inner strength of a person to deal and cope with significant adversities such as cancer. This personal characteristic usually stems from the religious background, meaning component, and existential coping aspects.115,116 In the study conducted by Aukst-Maretic, the relationship between the religiosity of patients and their major symptoms like depression and pain, was assessed in patients with BC. 34 The results revealed that higher spirituality and adequate social and mental support could alleviate the patient’s strength in confronting BC and associated symptoms. However, this essential element is usually neglected and underestimated by healthcare providers due to a lack of practical guidelines. The study conducted by Breitbart 35 among almost 300 BC patients revealed that 42% and 40% of patients require assistance to find hope and meaning in their lives, respectively. Another survey conducted among BC patients from the USA about their spiritual/existential needs showed that the majority of these patients wanted help to overcome spirituality issues. 91 The main “existential sufferings” that these patients typically deal with are reliance, meaninglessness, hopelessness, burdensomeness, loss of social role, and feeling unimportant. Inappropriate dealing with emotional and mental health concerns and the spousal relationship of women patients with BC by healthcare professionals were also reported in previous studies.117,118 Patient’s unmet spirituality/religiosity problems negatively impact the QOL and may continue for years after their treatment is finished. Social pressures, religious misperceptions, and false beliefs all play a part in the delaying of help-seeking attitudes and inadequate BC screening efforts. 48
Educational Problems
Informational needs and new methods of accessing information about patients with BC in scientific literature and clinical practice are insufficiently investigated. However, it is generally accepted that similar to insignificant overall health awareness, awareness of BC is inferior among the public, and patients with BC do not receive sufficient information about cancer disease’s signs and symptoms, where to look for treatment, and find BC professionals, or how to do some preventive behaviors.36,119,120 In most cases, adequate information and support were either lacking or inappropriate or did not “fit” or match the BC patients’ age or life stage. These problems, along with other socioeconomic barriers such as financial affordability, social and religious stigma, lack of pervasive screening programs, etc., result in delayed diagnosis. On the other hand, differences in public awareness with significant delays in diagnosis could lead to stage progression, disease exacerbation, and several prognostic elements like large tumors, metastases from lymph nodes, elevated pathological grade, and inadequate hormone receptor status.42,121 Cancer patients’ lack of knowledge about the disease causes a tiny percentage of women to choose mammography, Self-Breast Examination (SBE), or periodic examination by medical professionals for BC screening, which results in an advanced stage presentation.122,123
Another important and common scenario is typically imagined when a patient with BC symptoms comes to the cancer center for the first time in order to receive both primary and cancer-related therapies. In most cases, they have no preview of the courses and treatment activities, so they are generally frightened and anxious at their first visit.48,124 On the other hand, an increasing number of cancer patients are receiving treatment as outpatients, putting them at risk for a variety of unfavorable outcomes that they must manage for themselves. Therefore, patients require to know how to recognize, assess, interpret, monitor, and manage their symptoms. However, previous studies revealed that many BC patients do not receive appropriate education about treatment options and lose the opportunity to receive proper training at the right time. 125 It is worth mentioning that providing information alone is not enough to support patient symptom self-management. In this way, there is a concern among the nurses that they were perhaps not providing adequate information and support, both practical and emotional, for patients in their unit who are undergoing BC treatment. 126 The lack of information on treatment protocols leads to significant difficulty in the selection and interpretation of the appropriate treatment for patients and such patients generally referred following an inappropriate operation that poses a challenge in terms of the evaluation of the need/extent of re-operation and modified procedures or even for planning adjuvant treatment. Therefore, these patients may have worse outcomes than those initially managed in a suitable protocol-based manner. 40 On the other hand, patients are usually diagnosed by low-skilled physicians due to the scarcity of specialists with adequate training and appropriate skills in the management of BC. This, in turn, leads to non-optimal treatments and high mortality among these patients. 127
Social Problems
Although social challenges of BC patients due to the long-term physical, psychological, and other cancer-related health problems were reported in the previous studies, they are not sufficiently addressed.128,129 Social issues may alter all cancer patient’s social roles and activities, not just those with BC. Despite its important effect on the overall well-being of BC patients, unfortunately, social support services are still underdeveloped in many countries, especially in LMICs. 130 In the study conducted by Sidra et al., feminine sensitivity, stigmatization, and aversion to male doctors were reported as the main socio-cultural barriers in Pakistan. This study highlighted that BC patients suffer from a lack of social and emotional support from family and other relationships. Consequently, women with BC prefer social isolation over available social support and spend more time in isolation to avoid negative body image evaluation of their bodies. 48 Other studies in this area confirmed that reductions in social function often last for many years after treatment is completed.24,131 This, along with social stigma and frequent strong taboos against discussion of BC and social refusal to admit these patients in some cultures, leads to improper compliance of patients to treatment and follow-up and poor QOL for patients and their families.132,133 Other factors, such as personal, environmental, financial, and cultural issues, and relationships with healthcare providers and family members, may alter BC patient’s social status. BC patients also often feel isolated because of potential barriers to adjusting to their social statuses, such as employment, changes in relationships, role adjustment, and leisure activities.134-136 In the survey performed by Cimprich et al. 137 based on the patient’s age, it is revealed that younger patients have poorer outcomes in social aspects, whereas older patients manifest the lower QOL regarding their physical well-being. This lower social well-being among YWBC is attributed to insufficient family and social support. Social problems also negatively affect patient’s other personal aspects, such as psychological and spiritual well-being. Because of the inter-related nature of the social and mental aspects, the “Psychosocial” concept is frequently used in oncology texts to describe the QOL of BC patients.137,138 On the other hand, social concerns issues interference with activities at home and employment and result in a major financial burden. Therefore, the psychosocial well-being of BC patients must be considered within the context of women’s daily lives and routines.
Long-Term Problems
Despite the increasing number of BC survivors, up to 90% of this population suffers from unexpected long-term sequelae. 139 Once BC treatment finishes, most side effects disappear. However, some long-lasting side effects may arise and linger months or even years after treatment. Therefore, the long-term problems of BC patients could be defined as any problems (including those discussed in the short-term problems sections above) that sustain and linger for an extended period. However, most of these problems directly result from cancer treatment.140,141 The type and duration of each treatment mainly rely on the type and stage of the illness. Similarly, the results and outcomes of BC treatment vary considerably depend on the type and duration of the treatment and could result in different lingering and chronic physical, emotional, psychological, and spiritual problems. Acute and chronic pains are the most prevalence and universal symptoms reported for almost all women with BC. 23 The main risk factors for pain syndrome usually include younger age, BMI, acute or chronic anxiety and depression, any surgical procedure including axillary lymph node dissection and radiation therapy.142,143 Other treatment-related long-term effects, such as anatomic changes, headaches, fatigue, axillary web syndrome, dental issues, phantom breast pain, musculoskeletal symptoms, lymphedema, etc., have been reported for BC patients.144,145 Late effects also vary widely from person to person, and in most cases, various descriptions are assigned for a specific symptom. For example, different terminologies have been assigned in the literature for the chronic pain of BC patients and survivors. These nomenclatures vary widely and may include chronic neuropathic pain after breast surgery, chronic postsurgical pain, persistent post-mastectomy pain, post-mastectomy pain syndrome, persistent pain after BC treatment, and chronic pain syndrome. 89 Anyway, these long-term effects usually change or alter the patient’s and survivor’s lives after treatment. In the study by Hidding et al., almost half of the women receiving treatment for BC were in preretirement age. For younger or working-age women, 43% to 52% have employment concerns, potentially requiring reduced work hours or stopping employment entirely.83,131,146
Almost all BC patients experience fertility and pregnancy concerns in their clinical and post-clinical stages that would result in chronic symptoms over a long period. In women with mastectomy, musculoskeletal changes such as scapular incoordination, shoulder impingement, rotator cuff disease, asymmetric gait, and loss of strength may occur on both the affected and non-affected sides depending on unilateral or bilateral mastectomy. 147 Radiation therapy, by damaging tissue and releasing inflammatory factors, usually increases long-term dysfunction and local and regional pain syndromes. On the other hand, abnormal sensations on the chest wall, axilla, upper arm, and sometimes upper back and side may result from nerve damage in radiation therapy. 148
Despite the abovementioned physical outcomes, long-term functional changes also occur in this population. As a few examples, fatigue, decreased strength, mobility, aerobic capacity, and cognitive dysfunction are common disorders in these population.146,149 Depending on treatment regimens, other long-standing issues may include psychological alterations, cognitive dysfunction, cardiotoxicity, nephrotoxicity, and neurotoxicity. 89 Previous studies reported that over 50% of women experience some degree of upper extremity impairment, and 24% of them continue to have clinically considerable impairments more than one year after completion of treatment. Moreover, 70% of women who underwent mastectomy with axillary lymph node dissection had clinically meaningful impairment in at least one aspect of upper body function on follow-up 7 years later, as well as 41% of women who had sentinel node biopsy. Loss of grip strength was a most noticeable issue in patients who underwent chemotherapy.150,151
BC patients and survivors also suffer from multiple QOL issues for a long time after BC treatments end. 152 With recent advancements in BC patient’s supportive care, most survivors report a good QOL after completing BC treatment. However, serious gaps still remain in addressing these patient’s psychological, mental, personal, and financial concerns. 153 As discussed above, financial constraints not only limited the treatment options and QOL of these patients but also led to long-term social and livelihood problems due to the exorbitant costs of cancer treatment. Moreover, the timely delivery of medical and rehabilitation services has been suggested through some care delivery models (including the prospective surveillance model, procedure-linked referrals, survivorship care plans, risk stratification, etc.) but has been limitedly implemented. On the other hand, long-term psychological, mental, and spiritual issues like depression, anxiety, body image concerns, and sexuality issues may occur in these patients in the absence of effective and adequate medical and social support. Previous literature have shown that YWBCs are more likely to develop these problems than their older counterparts. 154 Therefore, the development and implementation of age-specific supportive care and social support are essential to improving these patient’s QOL and overall well-being.
Coping and Adjustment Strategies
Addressing the above-mentioned problems in BC patient’s treatment and care and coping with the gruel and debilitating sequelae of these patients require the focus of very particular attention. The sections below describe the existing strategies currently used for improving the clinical outcomes and supportive care of these patients.
Establishment, Dissemination and Implementation of Effective Guidelines in Managing BC
As discussed above, BC patients in general and YWBCs in particular face multiple problems through their initial disease diagnosis, clinical treatment, and survivorship. Evaluating and addressing these problems may eventually result in better patient satisfaction with decision-making procedures and QOL.155,156 In this regard, several recommendations and guidelines have been disseminated and implemented on the national and international scale to address and cope with these issues. For example, the National Comprehensive Cancer Network (NCCN) provided guidelines for addressing the most prevalent symptoms of BC patients during and after the treatment course. 157 On the other hand, BHGI cosponsored by other collaborating organizations such as the Centers for Disease Control and Prevention (CDC), National Cancer Institute (NCI), and Susan G. Komen, held two Global Summits in Seattle (2002) and Bethesda (2005). At the Bethesda meeting, universal systematic approaches (including basic, limited, enhanced, and maximal levels) have been developed and defined for improving global healthcare resources. Each level is referred to specific regions with different levels of financial and infrastructural resources.158,159 Similarly and consistent with previous guidelines, the European School of Oncology (ESO) and the European Society for Medical Oncology (ESMO) disseminated comprehensive recommendations in the fourth International Consensus Conference for BC in Young Women (BCY4). These recommendations are suggested to cover various activities, such as management (general guidelines), assessment, and treatment (screening, diagnosis, and imaging for staging and follow-up, genetic counseling and testing, early BC loco-regional treatment, and adjuvant systemic treatments) of early, advanced, and inflammatory BC in YWBC, and are proposed to implement for standard care outside of clinical trials. Regarding this, it is proposed that the diagnostic and treatment suggestions be taken into account in relation to national regulatory approval, accessibility, and payment. During the clinical care phase, the panelists reaffirmed earlier recommendations that emphasized the value of multidisciplinary care, acknowledging that in settings with fewer resources, this may not always be feasible. Accordingly, in order to improve clinical and supportive treatment in LMICs, nine necessary resources were identified, and resource-stratified suggestions (akin to the Bethesda meeting) were proposed.160,161 In individual treatment planning, further advice is given for customized psychosocial support, genetic predisposition counseling, fertility consultations and preservation, sexual health, and economic consequences. 161
Establishment of Comprehensive BC Supportive Programs and Initiatives
Besides the abovementioned guidelines, different supportive programs and initiatives have established a multidisciplinary BC team, composed of various expertise in medical oncology, nursing, psychology, pathology, consulting, data management, research coordination, survivorship, etc., to address the BC patient’s specific requirements and support them through BC treatment.
162
The four primary sectors of these programs are education, improvement of clinical care, supportive activities, and research. The educational sector enhances patient, professional, and community awareness and streamlines practical guidelines for efficacious prevention. The clinical care sector establishes general and advanced medical care for patients and enforces existing protocols for prevention and treatment. Supportive activities encourage patients to connect with each other and the community by breaking their isolation from family and community. In the meantime, the research sector investigates the other aspects of BC patient’s care to improve their clinical outcome and QOL (Figure 5). Different activities of current BC programs in education, clinical care improvement, supportive care, and research sectors (17).
In these programs, primary BC prevention has been developed to improve the early detection and timely treatment of BC by implementing different cancer control and screening programs like door-to-door and mobile cancer screening programs. A primary assessment of each patient’s needs and conditions is conducted and continually monitored by timely referrals to other healthcare and supportive services. 17 Financial and budgetary assistance of needy patients and families by governmental and non-governmental agencies, volunteer-based charities, and charity care programs enhanced BC patient’s opportunity to complete treatment courses and prevent disease progression and unwanted outcomes. 163 Patient navigation as a patient-centric healthcare service delivery model is provided for patients from their first referral by introducing the available resources and how to access them. Comprehensive and well-coordinated medical care with standard protocols is provided to enhance BC prevention and clinical outcomes. Conservative and less-aggressive treatments were introduced broadly to clinical care to minimize the treatment-oriented physical impairments and other possible issues such as fertility and menopausal concerns. In this respect, the American Society of Clinical Oncology (ASCO) established recommendations for maintaining fertility in BC patients and focuses on guidance to oncologists to prevent sexual problems and other related issues in people undergoing cancer treatment. These essential and significant steps in providing appropriate clinical and supportive care for BC patients have greatly facilitated the treatment course for these patients and prevented anxiety feelings.25,164
BC Supportive Care
Although the abovementioned advancements have improved BC patient’s clinical and post-clinical outcomes, effective strategies and long-term support are required to enhance their QOL and better adaptation to the disease. Therefore, holistic approaches based on the multifactorial assessment of patient’s symptoms are proposed to address and cover BC patient’s multidimensional requirements (Figure 6). These treatment approaches generally include medication, exercise, counseling, physical and occupational therapy, and alternative and complementary therapies. Primary care, gynecologic clinicians, and midwives are considered the well-positioned staff to provide a thorough evaluation, education, treatment, and referral for the most common sequelae of mastectomy and BC treatments.157,165 One-to-one peer support and patient and family counseling are suggested as valuable strategies for coping with psychological issues. Adequate support (emotional, informational, and financial), especially from family, friends, cancer survivors, and healthcare professionals, is expected to encourage patients to cope with their cancer-related challenges.
166
Besides BC patients, their families and close relatives also have higher supportive care needs, and some psychological and educational sessions seem to be helpful for them. Proper streamlining and augmenting services are also needed to address BC patient’s most critical needs, such as genetic counseling, rapid fertility consultations, etc.167,168 Many previous studies revealed the significant benefits of early home-based physiotherapy interventions on functional and emotional well-being and life quality on completion of the service at two months post-diagnosis.169-171 However, the results showed minimal change in the abovementioned factors for women who received group-based exercise and psychosocial intervention on completion approximately four months after the diagnosis.
172
In another study, an evaluation of the exercise effect on the BC treatment side effects showed that compared to sufficiently active women, sedentary women reported higher rates of weight gain, shoulder limitations, breathlessness, and muscular chest wall pain.
88
In addition, sexual health programs and behavioral sexual therapies may diminish the fertility issue concerns, produce substantive improvements in sexuality, and improve the overall QOL of BC patients. A Holistic approach was proposed for addressing and covering the multidimensional requirements of BC patients in the different stages of their treatment and follow-up care.
Psychological Support
For coping with emotional and psychological problems, effective strategies are needed for both BC patients and survivors to adjust to the inevitable impacts of cancer, such as cancer-induced emotional senses and psychological reactions that are commonly referred to as “Emotional turmoil”.
Spirituality, an integral dimension of human beings, is correlated with various short-term and long-term outcomes during and after BC treatment, such as spiritual, physical, and psychosocial well-being. Many factors are involved in increasing the patient’s spiritual well-being, including the patient’s self-esteem, social background, religious beliefs, family support, doctor-patient relationships, etc. 173 Previous studies highlighted that the psychological problems of BC patients and coping mechanisms are influenced mainly by the patient’s social and contextual status.174,175 Moreover, patients personal characteristics have correlated with several positive effects on their physical and emotional health, reduced chronic pain, enhanced coping skills, and elevated QOL. 166 In this regard, BC patients showed to adopt different coping strategies in dealing with BC and associated symptoms, such as avoidance, problem-focused strategies, logical efforts, fatalistic viewpoint, etc. 91 Coping is acknowledged as one of the fundamental ideas in the context of QOL, and it affects the treatment results and survival rates of women with BC. Among different personal characteristics, religious beliefs have an essential effect on dealing with cancer-related symptoms and soothing long-term complications. Religious beliefs are considered a source of resilience and a means of overcoming severe illnesses. On the other hand, it is shown that emotional support from patients’ families (including spouses, mothers, sisters, brothers, and children) also could enable BC patients to cope with cancer-related complications and adjust to their new situations. 153 In this respect, family counseling helps patients and their attendants cope and reconcile to the disease symptoms, treatment course, and clinical outcomes.
Spiritual well-being also plays a vital role in soothing the physical and psychological symptoms and cultivating meaning, purpose, and comfort in patients’ lives. Spiritual characteristics could be a valuable resource for managing and adjusting the patient’s symptoms. An enhanced spiritual and moral well-being could result in desired patient adherence to treatment, reduce anxiety and hopelessness, shorten hospitalization duration, and improve treatment outcomes. One study found that higher spirituality usually enhances and improves mental and physical health, coping with illness, patients’ compliance to treatment, and medical outcomes. This state is increasingly considered an essential element of health and well-being. Currently, patient’s psychosocial and spiritual characteristics have been utilized as a useful tool for assessing the chronic and long-term effects of BC on patient’s satisfaction and QOL.176,177 Therefore, adequate attention to BC patient’s spiritual and moral issues could improve their treatment outcomes and overall well-being.
Due to the important effect of spirituality on the patient’s QOL, different supportive programs have provided Body-Mind-Social-Spiritual group therapies to promote meaning in life and enhance opportunities for the patient’s personal growth, decrease stressful conditions, and maintain a stable lifestyle. Cordova et al. 107 suggested providing an environment and a facilitator to support BC patients in reevaluating priorities, life goals, and sources of meaning. In this regard, some supportive programs, like the PYNK Program, provided a “Waiting room model” for patients in which YWBC spends the most treatment course time in that room. This model provided an additional benefit to the clinic by elevating patient’s experience, encouraging informal peer support, and often creating new friendships. 178 Other BC programs have started to involve BC patients and survivors in their own treatment and program activities to enhance their spiritual well-being, knowledge, and confidence. It is expected that these activities finally encourage and empower patients not only to face their own issues and problems from a more strong and powerful standpoint but also to break their isolation and inspire newly diagnosed BC patients to cope quickly with current illness conditions and become part of this strong and hopeful entity.179,180
Recently, integrative oncology in the form of various programs and strategies has been introduced to clinical and post-clinical segments to alleviate the BC patient’s various physical, psychological, and spiritual challenges. These approaches were developed to combine and implement evidence-based complementary therapies with mainstream supportive care to improve physical, psychological, and spiritual well-being and QOL of YWBCs. For example, several studies have used Psycho-Spiritual Integrative Therapy (PSIT) as a combined resource of spiritual and psychological aspects to evaluate and promote the BC patient’s physical, psychological, and spiritual well-being. 181 As another example, Complementary and Alternative Medicine (CAM) interventions have been used for this purpose, and a growing number of cancer patients and survivors followed these interventions to fulfill their spiritual needs.182,183 In these interventions, higher levels of spirituality and faith positively correlated to elevated psychological and physical well-being and QOL. PSIT is another integrated psychotherapeutic approach that is frequently used for targeting the treatment of physical, psychological, existential, and spiritual symptoms. This integrated multicomponent approach has shown considerable promise in improving health and well-being among BC patients. Participants in this intervention were involved in multidimensional spirituality assessments to identify and understand their highest life meaning or aspiration. On the other hand, cancer patients and survivors have valuable opportunities to evoke and cultivate their personal sense of religious/spirituality aspects by responding to their bodily sensations, emotions, thoughts, images, and motivations in this program.
In these interventions, the BC participants report about a specific factor that is usually validated and quantified by matching their score on a measurement system like the Functional Assessment of Cancer Therapy (FACT). The FACT measurement system generally includes different scales, such as the general scale and disease-, symptom-, and treatment-oriented subscales. These measurement scales and subscales evaluate the patients and survivor’s various cancer-related factors, such as physical, emotional, social, and functional well-being and their relationship with the doctor. Similar measurement systems were also developed for evaluating the physical symptoms of BC patients and survivors. These systems generally include the Multidimensional Fatigue Inventory (MFI), which is designed to measure general, physical, and mental fatigue; the Functional Assessment of Cancer Therapy-Breast Cancer Symptom Index (FBSI); and Patient-Reported Outcomes Measurement Information System (PROMIS) Function Short Form 10b for measuring the important and relevant concepts of interest related to disease symptoms, treatment side effects, and physical functioning impacts in this patient population, etc. In this manner, three cancer-specific instruments, QLACS, QLI-CV, and QOL-CS, have been developed to evaluate all four domains of QOL (physical, psychological, social, and spiritual) and include questions specifically relevant to BCS.184,185 Other BC-related instruments for the assessment of BC patient’s different treatment and QOL aspects have been summarized elsewhere. 186
Educational Support
Increasing awareness and providing appropriate information to young women about BC early diagnosis, risk reduction, and prevention is another crucial component of their health. This may ultimately impact this population's early BC diagnosis. It has been shown that proper education of BC patients can increase their knowledge and reduce the risk of unwanted clinical outcomes.187-189 In one study, the need for information from cancer patients was assessed based on their employment status. The results showed that most participants were homemakers (67%) and were in dire need of information about cancer. 190 Therefore, it is essential that BC patients receive ongoing medical education as well as therapy information throughout their course of treatment and follow-up care. Until today, significant efforts have been made to promote the patients, their families, and the public awareness about BC.187-190 However, providing timely and appropriate information to needy patients is always challenging because of the vast social, cultural, racial, and religious diversity in the targeted population and different countries. Despite these challenges, various national and international programs embarked to timely promote BC patient’s awareness of cancer symptoms, diagnoses, and clinical treatment. In this regard, evidence-based policies that are suitable from an economic and cultural standpoint for developing nations have been created and put into practice.191-194
The early patient education program can decrease the disease progress and enhance the early and timely diagnosis of BC by promoting awareness among patients, healthcare staff, and society. On the other hand, the provision of pre-treatment information and counseling about BC patient’s specific problems and clinical concerns have been highly recommended by previous studies, especially for YWBC.192-194 Oncology nurses are considered well-situated healthcare staff to help patients through their communicating needs, values, and preferences during medical treatment and support them with symptom self-management. Therefore, the nurses concluded that it would be beneficial to better understand patients personal and medical issues and the way they could assist them in resolving these issues. To this end, well-educated nursing and healthcare providers are needed to improve BC treatment and address their various personal and communication needs. 126
As discussed above, an increasing ratio of patients are undergoing outpatient cancer therapy and require additional information and educational interventions about self-management to actively recognize, assess, comprehend, monitor, and control their symptoms. The main components of self-management educational interventions are thought to be promoting appropriate problem-solving and decision-making skills, enhancing patient self-efficacy to communicate with healthcare providers effectively, customizing recommendations to specific conditions, and establishing goals with action plans. 195 For this purpose, establishing self-management supports to ensure effectiveness and sustainability, providing detailed explanations of interventions to facilitate behavior change, and employing advanced educating methods to promote successful execution have been suggested in previous studies.195-198 Moreover, evidence-based reports have emphasized the significance of offering symptom self-management strategies within a multidisciplinary healthcare team. 195 Despite increasing evidence emphasizing the value of symptom self-management support for needy patients, nurse-directed interventions are scarcely conducted in standard clinical settings. For example, it is reported that patients in Switzerland require additional information and support for self-managing their problems during cancer treatment. 199 Accordingly, in 2011, Swiss oncology nurses began working on the Symptom Navi©Programme (SN©P). The SN©P comprises a training manual for nurses to conduct semi-structured nurse-led consultations as well as sixteen evidence-based written information leaflets (Symptom Navi© Flyers, SN©Flyers). SN©Flyers offers patients organized information on methods for managing their own psychological and physical symptoms to help with common symptoms. At the beginning of treatment, semi-structured nurse-led discussions with SN©Flyers are initiated. Nurses assist patients in managing their own symptoms by customizing consultations to the recommended therapy. At least two consultations should be provided to each patient. 200
Supportive programs are also required to provide sexuality and breast reconstruction, nutrition evaluation, survivorship augments, and encompassing supportive care for these patients and their families. In this regard, patient navigation is proposed as the most efficient strategy to effectively decrease anxiety and promote patient satisfaction in recently diagnosed BC patients. As a result, education programs or the education component of current programs are primely implemented for healthcare providers, patients, their families, and society to address the BC patient’s particular needs. 201 Recently, some BC supportive programs have embarked on increasing BC patient’s information by delivering lectures, printing, publishing, distributing, or selling books, newspapers, magazines, or any other literature in the oncology field.38,117 Other programs establish and maintain libraries and reading rooms and provide a platform for discussing oncology issues nationally. These programs mainly focused on providing age-appropriate information to patients and their families about the condition, different treatment and post-treatment procedures, and emotional support to enable them to reconnect and return to their family, social, and economic life as soon as possible. 202 In addition, scientific-based psychological and educational programs implemented by behavior change principles should be provided. In this regard, workshops with different subjects should be created for BC patients having treatment-related intimacy and sexuality problems. The long-term adverse effects of anti-cancer treatments must be considered by national and international agencies. Likewise, robust strategies should be implemented to address the psychosocial challenges of BC patients, and promote their health and wellness.
Besides providing appropriate treatment-based and survivorship information to BC patients and the public, extensive research programs and activities are needed to focus on the clinical, social, communicational, and behavioral issues of these patients in order to furnish a practical and scientific-based health policy and decision-making criteria and assist existing programs and initiatives. Clinical and post-clinical research will increase our knowledge about patient’s most important problems and requirements and enable us to design effectual and practical solutions and develop specific measurements to directly improve this vulnerable group’s overall medical and clinical outcomes. Clinical studies tailored to different economic and social conditions of each country would be valuable benchmarks to assess the unique issues of BC patients and recognize their medical, biological, psychosocial needs, and survivorship concerns, and evaluate whether these needs are being addressed. As a result, different national and international programs created comprehensive research sectors for performing clinical trials, analyzing the biological characteristics of BC, comparing them to other cancer types in various age groups and racial backgrounds, evaluating the effectiveness and results of treatment, and exploring activities related to physical, psychological, and emotional support. 203 However, additional research with dedicated clinical researchers and scientists is needed to clarify the influential parameters that affect BC prevalence and their effect on the detection, treatment, and follow up care of patients with emphasizing age-specific problems of BC patients such as pregnancy-associated BC. The results of these studies may help clinicians, professionals, and policymakers best address the essential needs of these populations worldwide.
Social Support
Adequate social support for BC patients may enhance and improve their physical and psychological health by providing the basic social requirements of patients. Previous studies have found that a reliable social background and family support have statistically significant protective effects on cancer overall morbidity and mortality. On the other hand, the effectiveness of social support on patient’s symptoms positively correlated with physical, psychological, and long-term variables. 204 Facilitating and improving the patient’s personal and social lives and properly educating the public regarding cancer and its early diagnosis effectively enhance their clinical outcomes and QOL. Therefore, the supportive arm of healthcare systems should facilitate the connection of patients with together and community through breaking the patient’s isolation.
Study Limitations
Although the current comprehensive review's results are encouraging, some limitations are mentioned. For example, some randomized and non-randomized studies were excluded because they lacked a control group, limiting our analysis to within-group changes (pre- and post-treatment). The exclusion of these studies from the systematic review was based on the need to answer the questions posed by the study. Moreover, a significant risk of bias was identified for randomized and non-randomized clinical studies in terms of “blindness of participants and researches”, “blinding assessment of the outcomes”, “Selective reporting”, “Bias due to confounding”, and “bias due to departures from intended interventions” categories. This imposes a significant uncertainty on the results derived and extracted from these studies. In addition, the large diversity of BC patient’s problems and their origins complicated the analysis and resulted in misclassification and underestimation of the contribution of individual problems to patients’ overall health and QOL. Therefore, the findings of the present study should be considered carefully, mainly because of the disparity of BC patient’s problems and also the methods used to identify them among patients with variable medical, personal, and socioeconomical conditions.
Conclusion
BC represents a significant global challenge that require the focus of very particular attention. This systematic review has identified BC patient’s various short-term and long-term issues through their disease diagnoses to follow-up care and highlighted the existing strategies for coping with them. In this respect, significant and persistent health concerns and QOL-related issues such as general, physical, psychological, spiritual, educational, and social problems have been identified for this population. Despite many advancements in addressing these problems and disseminating numerous protocols and strategies on national and international scales, there is no gold standard for managing and supporting these patients in clinical and post-clinical sectors. Therefore, effective measures and guidelines should be implemented through political and strategic agendas to provide essential resources for BC prevention, detection, and control. Medical practitioners and decision-makers should diligently monitor each patient and survivor’s different personal, medical, and QOL-based needs. These complex and interconnected short-term and long-term issues of BC patients should be evaluated in the clinical and post-clinical sectors to encourage and instruct adequate follow-up care after BC treatment completion. Besides knowledgeable practitioners, there is a vital need to develop innovative and holistic approaches and programs for assessment, treatment, and referral of these patient’s most serious problems and enhancing their QOL during and after treatment. In addition to presenting current strategies for coping with the various problems of BC patients, the present review also provides valuable insight into the useful tools for evaluating the QOL changes of BC patients. Using validated methods and instruments will provide valid data and enable researchers and clinicians to choose the most proper protocols to promote health outcomes and QOL of their patients in the short and long term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.