
Abstract
Introduction
This study aimed to assess whether the Access to Breast Care for West Texas (ABC4WT) program impacted regional breast cancer detection and mortality in the Texas Council of Governments (COG)1 region.
Methods
Interrupted time series analyses were utilized to evaluate the impact of the intervention. Spearman’s rank correlation and cross-orrelation analyses were performed to assess the relationship between the total number of screenings and (i) the total number of breast cancer detected and (ii) the proportion of early-stage cancer detected and the (pre-whitened) residuals. A three-way interaction model compared pre-and post-intervention mortality in COG 1 with the COG 9 region (control).
Results
Increased screening rate was associated with increased breast and early-stage cancer incidences (P = .001 and P = .002, respectively). There were significant positive cross-correlations between the total number of screenings and the total number of breast cancer detected (r = .996) and the proportion of early-stage cancer detected (r = .709) without a lag even after pre-whitening. Univariate analysis showed that regional mortality decreased with time (P < .001) and after intervention (P = .001). Multivariate analysis did not show any significant difference in time (P = .594), intervention (P = .453), and time and intervention interaction (P = .273). The three-way interaction model showed no difference in the baseline mortality and pre-intervention trend difference in COG 1 and COG 9 regions. However, there was a significant pre-post intervention trend difference in mortality COG 1 compared to the COG 9 region (P = .041).
Conclusion
Implementing the ABC4WT program was associated with the early detection of breast cancer and reducing regional mortality in the COG 1 region.
Keywords
Introduction
Breast cancer is 1 of the commonest cancers, predominantly affecting the female population in the United States (US) and Texas. 1 The age-adjusted mortality rate in Texas in 2018 was around 20.1 per 100,000, and the incidence was 115.5 per 100,000. 2 Even though breast cancer-related mortality has declined over the years and the incidence of breast cancer has remained stable, there are notable differences between rural and urban settings. 1 In rural settings, more people are uninsured, have high unemployment rates, and have low levels of education. 3 Furthermore, they have difficulty in reaching out to healthcare facilities to obtain routine care and screening. 4 Therefore, many patients present when symptomatic or are lost for follow-up after an abnormal mammogram screening. For instance, from 2014 to 2018, the incidence of breast cancer in rural areas was 104.5, compared to 115.4 per 100,000 in urban areas. 5 This noteworthy difference in incidence could be due to variability in healthcare access, including screening and early detection. Furthermore, a smaller proportion of cases were diagnosed at a localized stage in rural counties (58%) than urban areas (61%), indicating room for improvement by local outreach programs. 5
While screening mammograms are recommended for all women older than 50 according to US Preventive Services Task Force 6 or for those older than 40 according to the American Cancer Society, 7 many women in underserved communities do not undergo routine mammography screening. Leung et al 8 reported that women residing in rural areas were less likely than those in urban regions to have ever had a mammogram (odds ratio (OR) [95% confidence interval] = .74, [.62-.89]) or to have an up-to-date mammogram (OR = .59, [.49-.70]). 8 One particular reason is that many rural people lack early access to health care due to a lack of insurance coverage. Evidence suggests that disenrollment from insurance plans like Medicare or having no insurance contributes to late detection of cancers and treatment delay, which heavily burden the cancer outcome, especially in the case of breast cancer in rural communities. 9 Several outreach programs have been functioning nationwide to increase access to breast cancer screening services and reduce cancer-related health care burden.10,11 However, the national screening program serves only 10.6% of the underserved population. Furthermore, the impact of the federal screening program on the mortality rate has been questioned. 12
Similarly, Texas Medicaid Breast and Cervical Cancer Services (BCCS) is a statewide preventive program. Unfortunately, BCCS serves only a limited number of counties in Texas, which does not provide adequate coverage, especially in rural areas. For instance, in 2010, only one-third of the counties in Texas had a BCCS provider. 13 Therefore, the importance of local outreach programs has been emphasized.13,14
The Cancer Prevention & Research Institute of Texas (CPRIT) is the most significant statewide cancer research and prevention investment in the history of the US. Several cancer-related outreach programs have been implemented via CPRIT funding, and it has been serving Texas for 20 years. Access to Breast Care for West Texas (ABC4WT) program continues to serve in the Texas panhandle area - Council of Governments (COG) 1 since 2010. In this study, we evaluated the outcome of our outreach program. We compared regional breast cancer mortality data and our quantitative assessments of the program to assess whether it impacts the regional mortality rate, the total number of breast cancer detected, and the proportion of early-stage cancer detected. Furthermore, we have compared mortality rates in the COG 1 region with a similar area in West Texas, which has not been served by the ABC4WT program (COG 9) (Figure 1). Regional differences in breast cancer mortality in the 2000-2009 period vs 2010-2019 period in council of governments 1- panhandle regional planning commission (COG 1) and council of governments 9- permian basin regional planning commission region 9 (COG 9) regions.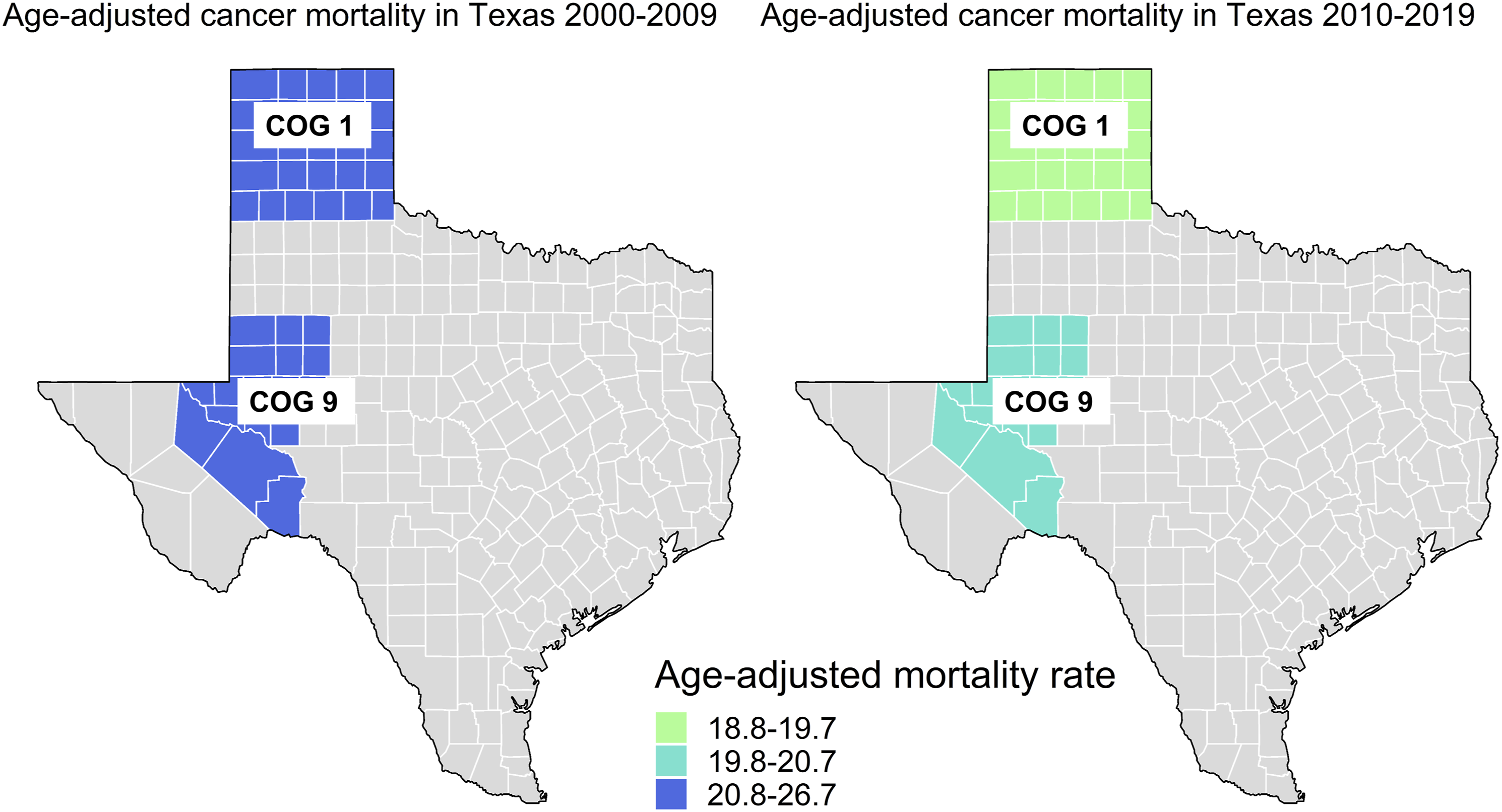
Methods
Intervention
ABC4WT is involved in outreach, awareness campaign, education, and service programs. The program has particularly focused on rural West Texas communities, in addition to metropolitan areas. The main objectives of the ABC4WT program were: (i) to build a West Texas breast cancer community network, (ii) to increase breast cancer screening rates through education and outreach, (iii) to enhance comprehensive counseling for high-risk women and offer chemoprevention, and (iv) to prevent advanced breast cancer in targeted underserved West Texas populations.
Data Sources and Study Population
As the study involved secondary analysis of the information retrieved from publicly available anonymized datasets, ethical review and approval were waived. Details regarding services provided by the ABC4WT program, including the number of screenings, were obtained by ABC4WT prospective data from outreach. 15 The number of cancer patients and their stages at diagnosis in the Texas panhandle area were obtained from Cancer Registry. 16 Stages 0, 1, and 2 were considered early-stage breast cancer, and stages 3 and 4 were considered late. COG 9 (Permian Basin Regional Planning Commission Region 9) was selected as the control region. It is geographically located in the West Texas region and demographically similar to COG 1 region in terms of the proportion of rural countries, population at risk, and area17,18 (Figure 1). Age-adjusted breast cancer mortality rates for COG 1 and COG 9 regions and the number of breast cancer detected were obtained by Texas Cancer Registry. 19
Statistical Methods
First, interrupted time series with linear regression models20,21 were used to assess the impact of the intervention (ABC4WT program) on the age-adjusted mortality rate in the COG 1 region. Models were constructed after checking for autocorrelation. The Durbin-Watson test was used to check autocorrelation in fitted models. As the breast cancer incidence and mortality time series were stationary, the analyses were conducted using interaction models by checking time and intervention and time and intervention interaction. We used a multivariate linear regression that modeled the interaction between time and intervention to predict mortality.
Second, multivariate regression models with interaction were constructed to examine the association between (i) breast cancer incidence and (ii) early-stage breast cancer incidence and the screening rate. We used a multivariate linear regression that modeled the interaction between time and screening rate to predict the incidences. Spearman’s rank correlation coefficient was calculated to assess the relationship between the total number of patients screened and (i) the total number of breast cancer detected, and (ii) the proportion of early-stage cancer detected. The total number of screening time series and (i) the total number of breast cancer detected over the years, and (ii) the proportion of early-stage cancers detected over the years were assessed for cross-correlation. Each pair of time series were compared and explored the temporal relationship through the cross-correlation function. 22
Finally, a three-way interaction model was constructed to assess the changes in mortality in the COG 1 region compared to the COG 9 region, which is considered a control region where the intervention (ie, the ABC4WT program) was not implemented. In this model, the pre-intervention trend difference (ie, the change in mortality over time in COG 1 before executing the intervention compared to the change in mortality over time in COG 9 region) was compared to the post-intervention trend difference (ie, the change in mortality over time in COG 1 before implementing the intervention comparing to change in mortality over time in COG 9 region). This linear regression model independent variables were time, region, and pre-or post-implementation of the intervention. Statistical analyses were performed using R statistical software (version 4.0.2).
Results
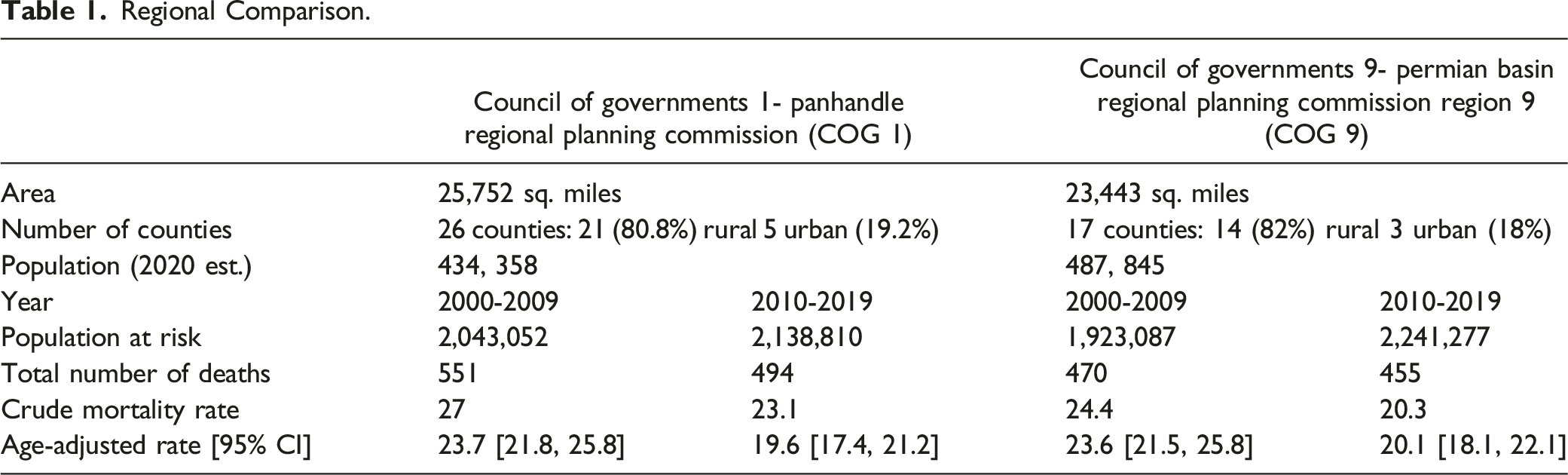
Regional Comparison.
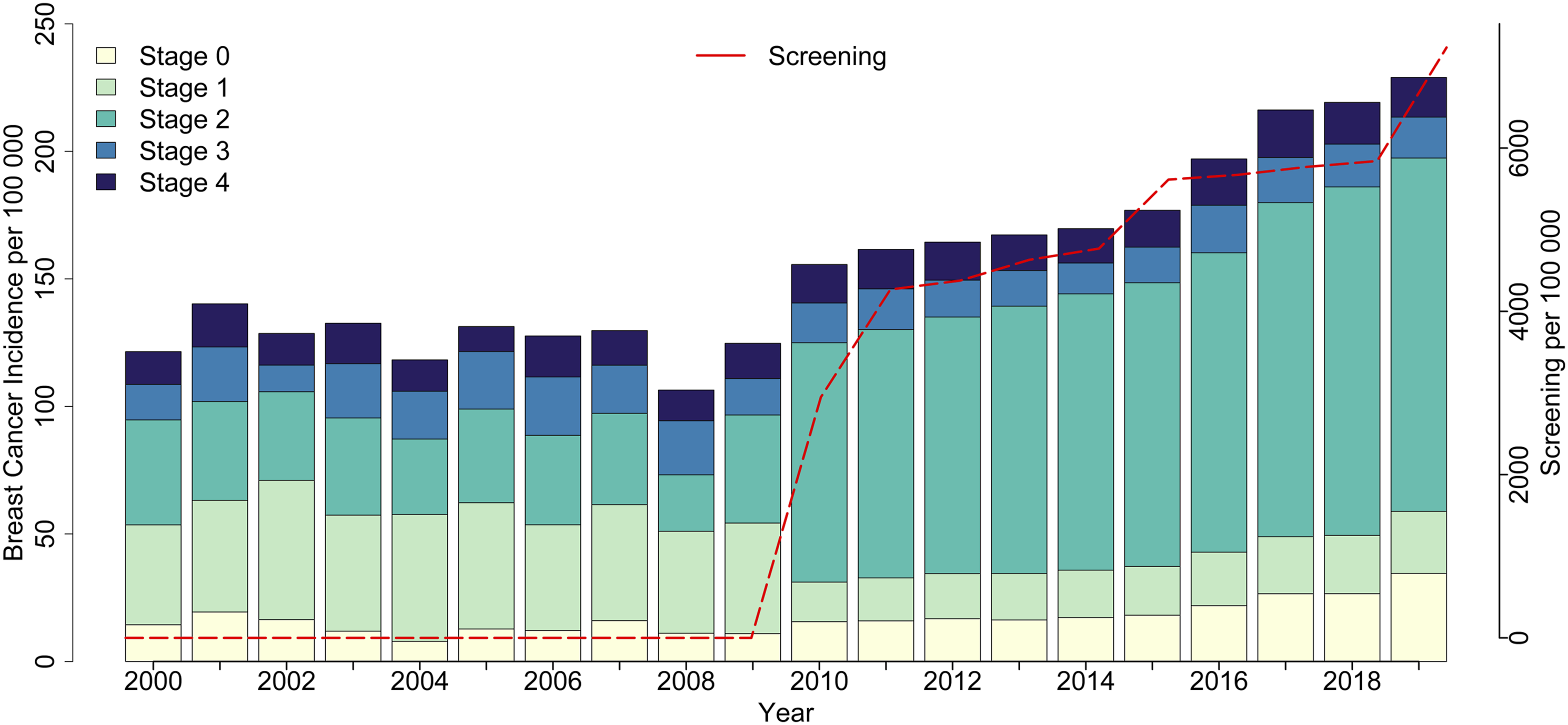
Screening rates and incidence for each stage of breast cancer in COG 1 region during 2000-2019.
Multivariate Regression Models Were Constructed to Predict the Breast Cancer Incidence in COG 1 and the Incidence of Early-Stage Breast Cancer.
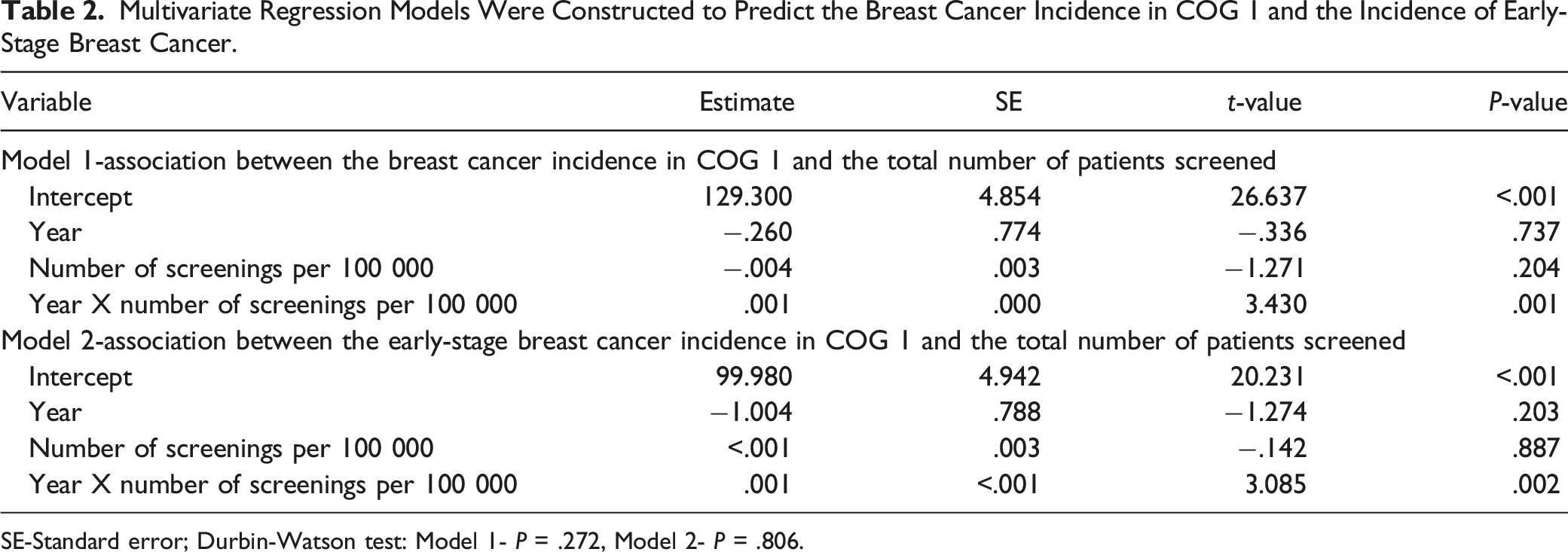
SE-Standard error; Durbin-Watson test: Model 1- P = .272, Model 2- P = .806.
When multivariate linear regression was constructed to examine the early-stage breast cancer incidence over the years and the rate of screenings, a significant positive effect was seen in the time and rate of screening interaction, indicating that screening increased the detection of early-stage breast cancer (P = .002) (Table 2). Furthermore, the proportion of early-stage cancer detected over the years was positively correlated with the total number of screening time series without lagging between the 2 series. Spearman’s rank correlation showed a positive correlation (r = .709, P = .028, Figure S1 in Supplement).
Interaction Model Comparing Pre-and Post-Intervention Age-Adjusted Death Rate in COG 1 Region.

Intervention- ABC4WTprogram; SE-Standard error; Durbin-Watson test: Univariate model 1- P = .592, Univariate model 1- P = .864, Multivariate Interaction model-P = .632.

The mortality rate in COG 1 region. In solid black line shows how the slope of mortality changed after implementing the ABC4WT program. Values predicted by a model in the absence of the intervention (counterfactual) are shown in gray.
Interaction Model Comparing Mortality Rate Between COG 1 Region vs Control (COG 9) Before and After Implementing the ABC4WT Outreach Program.
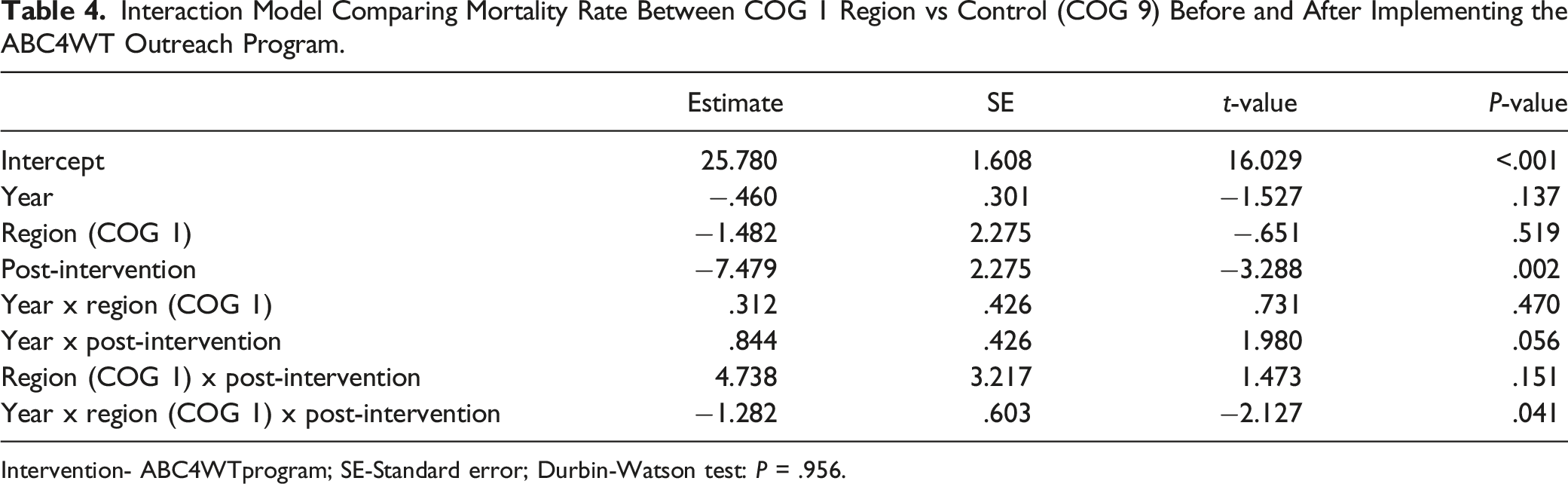
Intervention- ABC4WTprogram; SE-Standard error; Durbin-Watson test: P = .956.

Scatter plot with fitted regression lines presenting the interaction effect of time and regional differences on the age-adjusted mortality rate of breast cancer patients before and after implementing the intervention (ie, ABC4WT program). The intervention group is COG 1 region, and the control group is COG 9 region. Before implementing the ABC4WT program, the mortality rates in COG 1 and COG 9 regions were not different. Following the ABC4WT program, there was a significant pre-post trend difference indicating the age-adjusted mortality rate was decreased compared to control (P = .041).
Discussion
In this study, we have tried to assess the impact of the ABC4WT program that has served the Texas Panhandle, which primarily comprises rural communities, for over a decade. ABC4WT program includes outreach, education, and service programs where we mainly focus on increasing awareness and participation in screening. We found that with increased screening by the ABC4WT program, the detection of breast cancer, specifically the incidence of early-stage cancer, has increased markedly. Furthermore, we found that the age-adjusted mortality rate in COG 1 region is low compared to COG 9 region, where the ABC4WT program has not been implemented.
The majority of Texas counties are rural. There are 172 rural counties, and about 11% of Texans live in these counties. COG 1 comprises mainly rural counties and a few urban counties, rendering COG 1 region vulnerable to rural and urban challenges. ABC4WT project was funded by CPRIT in 2010 with a crucial intent to improve early breast cancer detection in this region. Therefore, we focused on increasing the breast cancer screening rate in the target population group in Texas Panhandle for secondary prevention via early detection. According to our study, we successfully increased breast cancer detection, specifically at an early stage.
Mammography rates remain lower among uninsured, low-income, and low-education groups even though overall mammography rates have increased over 30 years. 23 Therefore, age and racial and social disparities have been identified as factors governing the differences in cancer incidence rates.2,24,25 It was found that rural counties have a lower per-capita income and a lower percentage of adults below the poverty level, and a higher unemployment rate. These variations between rural vs urban have differing impacts on cancer diagnosis. Many studies revealed differences in adherence to breast cancer screening among women living in rural vs urban communities.26,27 Leung et al 8 showed that the stage at which breast cancer is diagnosed differs between women living in urban vs rural areas. Here, women in rural settings present at late stages of breast cancer more than in urban settings. For instance, this very notion is evident in West Texas. 28 Several studies have shown that rural communities in West Texas are reluctant to obtain breast cancer screening, leading to later presentation and poor outcomes.29,30 Interestingly, we found a strong positive correlation between screening rates and the incidence of breast cancer in the COG 1 region, specifically early-stage breast cancer. Hence, it is apparent that the ABC4WT program also successfully reached this difficult-to-reach underserved population. The difference in breast cancer screening participation in rural and urban communities could be linked to a lack of proper screening facilities or unequal distribution. 31 By implementing a successful outreach program, we hope to have subdued that challenge to a certain extent.
Although studies showed a reduction in later-stage breast cancer,32-36 some studies pointed out that early detection did not decrease late-stage breast cancer and showed substantial overdiagnosis occurred by screening.37-39 Reason for this controversy may be that screening benefits are not straightforward and are subject to several factors, including differences in patient population (age, racial/ethnic, and socioeconomic disparities) and study design. 35 For instance, Broeders et al 40 suggest methodological differences, such as the length of the follow-up period, the definition of advanced BC, and the definition of the age groups, which limit the interpretability of results coming from observational studies on this notion. According to our study, we have seen an increase in total breast and early-stage cancer but no reduction in late-stage cancer incidence. As shown in previous studies, 41 lack of adequate follow-up period could be the underlying cause for not seeing a reduction.
Before implementing the ABC4WT outreach program, breast cancer mortality for 1990-1999 and 2000-2010 was 27.3 per 100,000 and 23.1 per 100,000, respectively. From 2010 to 2018 mortality rate was 19.1 per 100,000. 19 So, it is apparent that there has been a decline in the mortality rate over time, probably due to the overall improvement of healthcare facilities and patient awareness. Increased detection and quick diagnosis of early-stage tumors that otherwise would have metastasis may have contributed to improving motility. Early diagnosis can lead to early access to treatment as well. Our study supports the temporal relationship between the decline in mortality and the comprehensive ABC4WT program. We explored if the ABC4WT program has altered the trajectory of the decline, which means a decrease in mortality rate furthered over time once the outreach program was implemented. Despite the difference in the overall mortality rate between 2000-2009 vs 2010-2019, there was no significant impact on the mortality rate reduction in the COG 1 region compared to pre-vs post-intervention. Failure to show a difference in the slope could be due to the inadequacy of time points since we have only had the ABC4WT program for nearly a decade, and to see an actual benefit, we might have to follow up on this for a longer duration. Since breast cancer has a lag time, we cannot expect a reduction in breast cancer mortality as soon as detection is improved. One study showed that it takes at least 2 years from the intervention for any difference to emerge in mortality rates by screening and early detection. 42 Hence, a longer time is required to get a meaningful difference in mortality rate at a population level. Nonetheless, we saw a significant impact on mortality when we compared the mortality rate in COG 1 with a mortality rate of a similar region that did not have the ABC4WT program, which provides evidence to suggest that the ABC4WT program was effective.
There is a disparity regarding treatment adherence between rural and urban populations. Rural residents face limited access to health services, fewer providers, higher costs, longer distances to travel to reach healthcare services with limited transportation options, and inadequate or under-utilized infrastructure.43,44 Therefore, due to the issue of accessibility, rural residents are less likely to receive treatment consistently, which leads to poor disease outcomes. 4 For instance, Thomas et al 45 revealed that older age, increased poverty, and rural geographical location are barriers to chemotherapy in West Texas. Similarly, Robertson et al 46 showed that the distance to cancer centers is positively associated with poorer outcomes. Therefore, 1 possible explanation for decreasing mortality following the ABC4WT program is increased outreach, leading to increased treatment adherence.
The importance of local outreach programs has been emphasized because, despite the availability of appropriate services and access mechanisms placed by nationwide or statewide programs, the reach of these services is compromised without awareness and targeted change in local cultures and beliefs toward screening.12,13 Evidence suggests that effective patient navigation improves cancer screening, reduces breast care delays, helps patients overcome barriers to accessing care, and provides psychosocial support and care coordination. 47 In the ABC4WT program, we had local community activists sensitive to local cultures trained to approach their communities, effective patient navigation services, and an organizational structure focused on public-private-community partnerships. These mechanisms introduced systems change where timely communication and flow of information were tremendously helpful. For instance, women could get screening at their local facilities, with suspicious screening results being evaluated by university-based experts. These women were then navigated through the system via diagnostic work-up and referral to appropriate treatment including financial counseling and support.
Partnerships with community-based organizations, health care systems, and insurers are encouraged to set up a successful outreach program. 47 In the ABC4WT program, we have tried to educate the community via reaching the public through community-based events (health fairs, faith-based events), multimedia, and social media. We conducted both group education sessions and one-on-one education sessions. We have achieved network building with partners in the Panhandle region. Several barriers were resolved through repeated negotiations, emphasizing community service and networking with neutral agencies in the Panhandle site. Border et al 29 showed that the Hispanic community is an underserved population in breast cancer screening in West Texas. However, we have been very successful in reaching the Hispanic community. We experienced some hindrance in some smaller pockets of refugees and other African cultures. To overcome that barrier, we used peer trainers, Women Inspiring, Serving and Educating (WISE) Women who reside in communities to educate women about the importance of breast health made inroads in communities, especially African American and Hispanic populations.
Furthermore, innovative means of reaching potential groups of individuals have been encouraged. For instance, McElfish et al 14 showed that a mobile mammovan recruited the rural underserved population better, which was an innovative intervention. Similarly, we used a different tactic to overcome a reduced follow-up rate after initial contact for scheduling mammogram appointments. Here, we negotiated blocks of time with mammogram providers that allowed us to do “on the spot” scheduling at the first encounter with women either through phone, one-on-one or out in the field at group events.
The study had several strengths and limitations. Regarding strengths, we used an interrupted time series design, a robust study design for studying the impact of health interventions.20,48,49 Then, a control group was used to compare the effects of our outreach program. Next, we used cancer incidence to explore the outcomes of the ABC4WT program, explicitly focusing on early-stage breast cancer. Regarding limitations, we had only a limited number of data points in our time series. Therefore, we could not avoid sample size limitations, which is necessary to generate sufficient power to estimate the regression coefficients.50,51 Finally, we can only show an association between mortality rates and the implementation of the ABC4WT program. We cannot prove causation as cancer mortality has various contributory factors.
In conclusion, the ABC4WT program successfully served the West Texas population. We believe that our program significantly impacts the detection of early-stage breast cancer and reduces overall mortality. The intervention, screening strategies, and results would have critical implications for future public health policymaking, and the findings of this study can be generalized to the population with geographic and race-specific similarities.
Supplemental Material
Supplemental Material - Impact of Access to Breast Care For West Texas Program on Early Detection and Regional Breast Cancer Mortality
Supplemental Material for Impact of Access to Breast Care For West Texas Program on Early Detection and Regional Breast Cancer Mortality by Chathurika S Dhanasekara, MD, PhD, Hafiz Khan, PhD, and Rakhshanda L Rahman, MD, FRCS, FACS in Cancer Control
Footnotes
Acknowledgments
The study group would like to thank the Cancer Prevention & Research Institute of Texas (CPRIT) for funding the Access to Breast Care for West Texas (ABC4WT) program.
Author Contributions
Conceptualization, RLR, and CSD; Methodology, CSD; Software, CSD; Validation, CSD, HK, and RLR.; Formal Analysis, CSD; Investigation, CSD; Resources, RLR; Data Curation, CSD; Writing – Original Draft Preparation, CSD; Writing – Review & Editing, CSD, HK, and RLR; Visualization, CSD; Supervision, RLR; Project Administration, RLR All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical review and approval were waived for this study as the study involved secondary analysis of the information retrieved from publicly available anonymized datasets.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.