
Abstract
Introduction
Classical Philadelphia-negative myeloproliferative neoplasm (MPN) includes Essential Thrombocythemia (ET), Polycythemia Vera (PV) and Primary Myelofibrosis (PMF). The JAK2V617F mutation is part of the major criteria for diagnosis of MPN. WT1 is reported to be highly overexpressed in most hematological malignancy. Our aim was to explore the combination value of JAK2V617F allele burden and WT1 expression in distinguishing the subtype of MPN patients.
Methods
Allele specific real-time quantitative fluorescence PCR (AS-qPCR) was conducted to detect JAK2V617F allele burden. WT1 expression was assessed by RQ-PCR. Our study is a retrospective study.
Results
JAK2V617F allele burden and WT1 expression were different in MPN subgroups. The expression of WT1 in PMF and PV is higher than in ET. JAK2V617F allele burden in PMF and PV is also higher than in ET. ROC analysis indicated that combination of JAK2V617F allele burden and WT1 expression to discriminate ET and PV, ET and PMF, PV and PMF is 0.956, 0.871, 0.737 respectively. Furthermore, their ability to distinguish ET patients with high Hb levels from PV patients with high platelet counts is 0.891.
Conclusions
Our data revealed that combination of JAK2V617F allele burden and WT1 expression is useful in distinguishing the subtype of MPN patients.
Introduction
Myeloproliferative neoplasm (MPN) is a group of clonal hematopoietic stem cell disorders characterized by clonal proliferation of one or more hematopoietic progenitors in the bone marrow, and may progress to acute leukemia. 1 Classical Philadelphia-negative (Ph-negative) MPN can be divided into three main sets: essential thrombocythemia (ET), Polycythemia vera (PV) and primary myelofibrosis (PMF). 2 Currently, bone marrow (BM) histology, including megakaryocyte morphology and degree of myeloproliferation, is essential in the distinguish of ET from PV and PMF. 3 However, when BM fibrosis was absent and the morphology changes of megakaryocyte are atypical, it is difficult to distinguish ET and Pre-primary myelofibrosis (Pre-PMF). 4 In a large multicenter study, that included 1104 patients with ET and pre-PMF, significant differences in the occurrence of bleeding, rate of death, progression to overt myelofibrosis and transformation to leukemia were found. 5 Since the different prognosis and treatment for MPN patients, it is urgently needed to find new tools to correctly distinguish the specific type of MPNs.
Human Janus kinase 2 (JAK2) gene is mapped to chromosome region 9p24.1. 6 In normal hematopoietic cells, JAK2 consists two homologous kinases: one is an enzymatically active kinase domain and the other is a catalytically inactive pseudokinase domain (JH2). 7 The most common mutation of JAK2 is the substitution of valine with phenylalanine at position 617 (JAK2-V617F). JAK2V617F mutations mainly occurred in MPN patients and a small part of AML patients. 8 The mutation frequency of JAK2V617F in PV patients was more than 95.0% and 55.0-60.0% in ET and PMF patients. 9 The finding that JAK2V617F was mutated in patients with myeloproliferative disorders has changed the diagnostic landscape of MPNs greatly. 10 JAK2V617F mutation is essential in the screening of MPN. However, For JAK2V617F-positive patients, the patient can only be diagnosed as MPN, we could not distinguish their specific subtypes.
Wilms’ tumor 1 gene (WT1) is known for its function in organ development and cell differentiation. 11 It is a transcription factor that guides the development of several organs and tissues. 12 WT1 is essential in the maintenance of tissue homeostasis and can act as either a tumor suppressor or an oncogene in several solid tumors and leukemia. 13 In a normal human bone marrow, WT1 is expressed in a small percentage and confined to CD34+ cells. 14 However, existing studies suggested that WT1 tend to be highly overexpressed in most de novo acute myeloid leukemias (AML),15,16 myelodysplastic syndromes17,18 and chronic myelogenous leukemia (CML). 19 Recent years, increasing number of studies have focused on evaluating the correlation between WT1 and MPNs. Guglielmelli et al. 20 using an approach of transcriptomic micro array showed that WT1 level was higher in PMF-derived CD34+ cells than in PV and patients who had higher WT1 expression levels tend to be disease active. In 2016, Gallo et al. 21 reported a positive correlation between WT1 transcript levels and IPSS score at diagnosis in PMF patients and they also found that WT1 expression can be a marker of response to therapy. Recently, Cottin and his colleagues 22 validated WT1 expression was significantly increased during the myelofibrotic transformation of ET or PV. In their study, they also reported that WT1 transcription levels was related to age over 65, splenomegaly and thrombocytopenia. Based on the above findings, we assume that the combination of WT1 expression and JAK2V617F allele burden may be helpful in distinguishing the subtype of MPN patients.
Materials and Methods
Sample and Collection
A total of 90 (38 men and 52 women, median age 62,22–85) bone marrow from new diagnosed MPN patients with JAK2V617F mutation positive were collected from January 2019 and October 2021 at Zhongnan Hospital of Wuhan University. Of all the 90 patients, 45 patients were ET, 26 patients were PV, and 19 patients were PMF. All patient details are de-identified in our study. The diagnosis was made according to the 2016 revision to WHO myeloid neoplasms and acute leukemia. 23 All patients included in our study had no any other hematological malignancy. All MPN patients were analyzed at diagnosis before any treatment, and informed consent was obtained from all individuals involved in this study. Our study is a retrospective study.
DNA and RNA Extraction
Total genomic DNA was extracted from EDTA-anticoagulated bone marrow samples by using DNA Isolation Kit (Tiangen Biotech, Beijing, China) following the manufacturer’s instructions. Total RNA was extracted using Trizol reagent (Invitrogen, Carlsbad, CA, USA) as described by the manufacturer. After extraction, DNA and RNA concentration was measured using Nanodrop 2000 spectrophotometer (Thermo Scientific Inc., Waltham, MA, USA).
JAK2V617F Allele Burden Detection and WT1 Expression Detection
Allele specific real-time quantitative fluorescence PCR (AS-qPCR) was conducted to detect JAK2V617F allele burden by using a quantitative fluorescent DNA detection kit (Yuanqi, Shanghai, China). JAK2 wild-type and mutation type were both amplified with respective primers, and JAK2V617F mutant allele burden was relatively quantified (JAK2V617F%) by determining the percentage of JAK2 mutation type quantity in the total JAK2 quantity. WT1 expression was assessed by RQ-PCR using WT1 ProfileQuant Kit (Yuanqi, Shanghai, China). Calibration curves with plasmids containing ABL1 and WT1 target sequences were used. The WT1 transcript values measured by RQ-PCR were normalized with respect to the number of ABL1 transcript and expressed per 104 ABL1 copies. The WT1 expression was transformed into a logarithm to ensure that values follow a normal distribution for statistical analysis. All PCR analyses were performed in duplicate. RQ-PCR was performed on ABI Prism 7500 system (Applied Biosystems).
Statistical Analysis
Patients’ characteristics were summarized as numbers (range) for qualitative variables. Shapiro-Wilk test was performed to check the normality of the distribution. For normally distributed data, student’s t test was used to compare 2 groups of continuous variables and one-way ANOVA was used for the comparison among multiple groups, while non-normally distributed data was analyzed by Kruskal-Wallis variance analysis. To evaluate the diagnostic value of JAK2 and WT1, receiver operating characteristic (ROC) curves were done, and the area under the ROC curves was determined. SPSS 17.0 software (SPSS, Chicago, IL, USA) and GraphPad Prism 5 software (GraphPad software, La Jolla, CA, USA) were used to analyze the data. All statistical tests were two-sided and P < .05 was considered statistically significant.
Results
Characteristics of the Studied Participants
Clinical and biologic characteristics of MPN patients.

Data are shown as Median and range. aChi-square test; bKruskal-Wallis. Abbreviation: LDH, lactate dehydrogenase.
JAK2V617F Allele Burden in MPN
Allele specific real-time quantitative fluorescence PCR (AS-qPCR) was conducted to detect JAK2V617F allele burden. Our results revealed that JAK2V617F allele burden in PMF (68.09 ± 6.60 vs 27.8 ± 2.98 P < 0.001) and PV(72.03 ± 2.89 vs 27.8 ± 2.98 P < 0.001) is higher than in ET. No significant difference was found between PV and PMF (72.03 ± 2.89 vs 68.09 ± 6.60 P = 0.551). We further explored the JAK2V617F allele burden distribution in the MPN subgroup. Patients were grouped by quantities of JAK2V617F allele burden. PV patients were more often distributed in the 50-75% or 75-100% groups, PMF patients were more often distributed in the 75-100% groups, whereas ET patients more often classified into 0%–25% and 25-50% groups (Figure 1). JAK2V617F allele burden in MPN and distribution in the subgroups. JAK2V617F allele burden were calculated by the following formula JAK2V617F Mutation/(Mutation + Wild Type). (A) JAK2V617F allele burden in ET, PV and PMF; (B) JAK2V617F allele burden distribution in ET; (C) JAK2V617F allele burden distribution in PV; (D) JAK2V617F allele burden in PMF. ET: essential thrombocythemia; PV: polycythemia vera; PMF: primary myelofibrosis, *P < .01, **P < .001.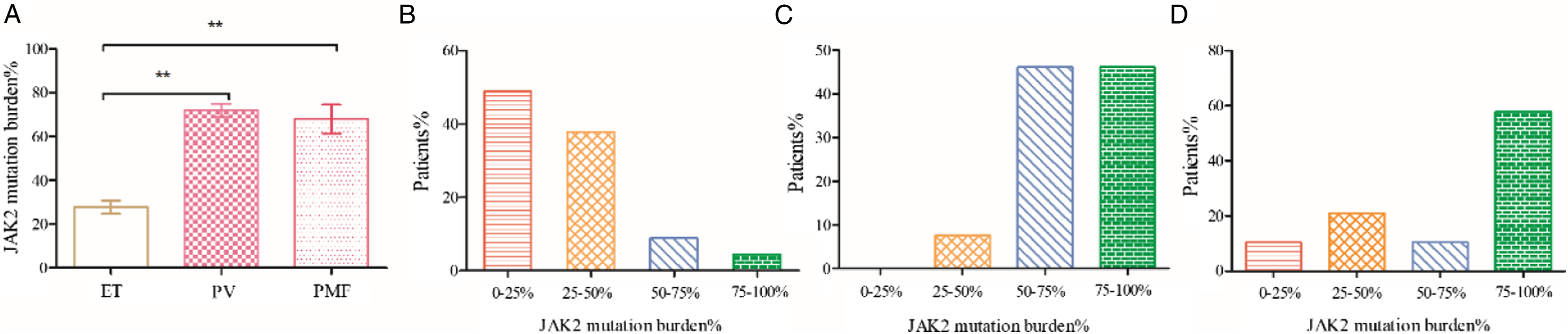
WT1 Expression in MPN
To investigate whether WT1 expression was different among ET, PV and PMF patients, one-way ANOVA test was performed. The results showed the expression of WT1 in PMF is higher than in ET (3.08 ± 1.59 vs 0.18 ± 0.029 P < .01). Besides, WT1 expression in PV is higher than in ET (0.55 ± 0.11 vs 0.18 ± 0.029 P < .001). When compared WT1 expression in PV and PMF, we found WT1 expression is higher in PMF than in PV, but the statics was not significant (3.08 ± 1.59 vs 0.55 ± 0.119 P = 0.069). To further investigate the relationship between WT1 expression and MPN patients, patients were grouped by quantities of WT1 expression. And we found that the patients were imbalanced distributed. All the ET and PV patients were populated in the 0-25%, as to the PMF patients, although most patients were classified into 0%–25%, there are a portion distributed in 25-50% groups (Figure 2). WT1 expression in MPN and distribution in the subgroups. WT1 levels were expressed as a ratio to ABL1 quantification. (A) WT1 expression in ET, PV and PMF; (B) WT1 expression distribution in ET; (C) WT1 expression distribution in PV; (D) WT1 expression distribution in PMF. ET: essential thrombocythemia; PV: polycythemia vera; PMF: primary myelofibrosis, *P < 0 .01, **P < 0 .001.
Diagnostic Value of JAK2V617F Allele Burden and WT1 Expression
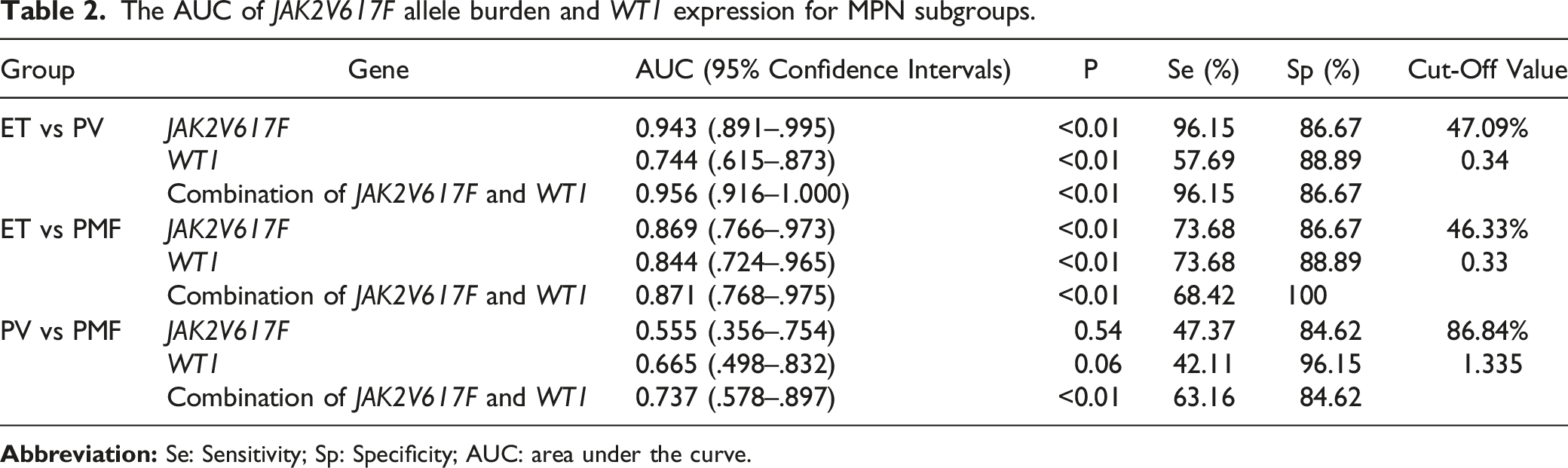
The AUC of JAK2V617F allele burden and WT1 expression for MPN subgroups.

Receiver operating characteristic (ROC) curves of JAK2V617F allele burden and WT1 expression for MPN subgroups. (A) ET vs PV; (B) ET vs PMF; (C) PV vs PMF.
Clinically, there are some ET patients with high Hb levels and PV patients with high platelet counts, for these patients, it is difficult to make a precise diagnosis. In our study, 6 ET patients with high Hb levels and 13 PV patients with high platelet counts were included, we conduct an ROC analysis, and found the combination of JAK2V617F allele burden and WT1 expression has a high ability to distinguish ET patients with high Hb levels from PV patients with high platelet counts with an AUC of 0.891 (Figure 4). Receiver operating characteristic (ROC) curves of Combination of JAK2V617F and WT1 for ET patients with high Hb levels and PV patients with high platelet counts.
Discussion
Studies have revealed that JAK2V617F mutation allele burden may be useful in evaluating the response to therapy. 24 Furthermore, researches have also reported JAK2V617F mutation allele burden can be used as a follow-up tool during the treatment of JAK2V617F positive patients. 25 Another perspective value of the allele burden is its predict value of both vascular events and fibrotic transformation. 26 However, the specific utility of the JAK2V617F allele burden for the differential diagnosis of MPN yet to be established. Our study for the first time explored the diagnostic value of JAK2V617F mutation allele burden to distinguish MPN subtypes.
In our study, we found an obvious differences between JAK2V617F mutations burden and WT1 expression within three subtypes of MPN. Both our studies and previous researches revealed that JAK2V617F allele burden27,28 and WT1 expression 29 will gradually increase with the progress of MPN. It is reported that JAK2V617F mutations mainly occurred in MPN patients and a small part of AML patients 8 and elevated expression of WT1 often imply patients to have malignant tumor. 30 In the present study, only new diagnosed MPN patients were included which will not be significantly affected factors other than subtypes.
Previous study has reported that WT1 transcript levels were higher in PMF than in ET and PV. 22 Our data showed the expression of WT1 in PMF and PV is higher than in ET. When comparing WT1 expression in PV and PMF, although no difference was found (P = 0.069), we think this is due to small size of this study. Gallo et al. found that hyperexpression of the WT1 gene in PMF is associated with the IPSS prognostic score and WT1 expression increased during leukemic transformation of MPN. 21 Our research focused on exploring combined value of WT1 expression and JAK2V617F allele burden in distinguishing the subtype of MPN patients. The combination of JAK2V617F allele burden and WT1 expression possessed a high ability to discriminate ET from PV and ET from PMF with area under the ROC curve of 0.9585 and 0.8713. And their combined value to discriminate PV from PMF is 0.7368. PV patients with thrombocytosis at disease presentation were frequently misclassified as JAK2V617F-positive ET patients.31,32 Our study found the combination of JAK2V617F allele burden and WT1 expression could distinguish ET patients with high Hb levels from PV patients with high platelet counts with an AUC of 0.891.
Limitations may exist in our study. First, in our retrospective study, although the diagnosis of MPN was made according to the WHO 2016 classification, but no pre-PMF patients were enrolled in our study, we were therefore unable to evaluated the value of WT1 expression and JAK2V617F allele burden to discriminate ET and pre-PMF that is difficult to differentiate by bone marrow biopsy; second although we only included patients that were firstly diagnosed before any treatment, there might be patients with initial diagnosis rather than initial onset; third the sample size selected for our study was not calculated and justified, and the statistical power of the study may be limited.
In conclusion, diagnosis of classical Ph-negative MPN should integrate several clinical, laboratory features, as well as morphology and immunophenotyping. When a patient is suspected to be MPN, JAK2 allele burden and WT1 expression can be a helpful additional diagnostic marker to distinguish the subtype of MPN patients. A prospective study with large sample is in need to confirm our findings. In our future study, we will explore whether the combination of JAK2V617F allele burden and WT1 expression in peripheral blood is helpful in distinguishing the subtype of MPN patients to overcome the obstacle due to the failure of the bone marrow aspirate in patients affected by myelofibrosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (81670125), Natural Science Foundation of Hubei Province (2018CFB243).
Ethics approval
The study protocol was approved by the Medical Ethical Committee of Zhongnan Hospital of Wuhan University (Ethical approval 2023022K, February 2023).